
Cardiovascular Disease Mortality Attributable to Low Whole-Grain Intake in CHINA: An Age-Period-Cohort and Joinpoint Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Data
2.2. Measurements
2.3. Statistical Analysis
3. Results
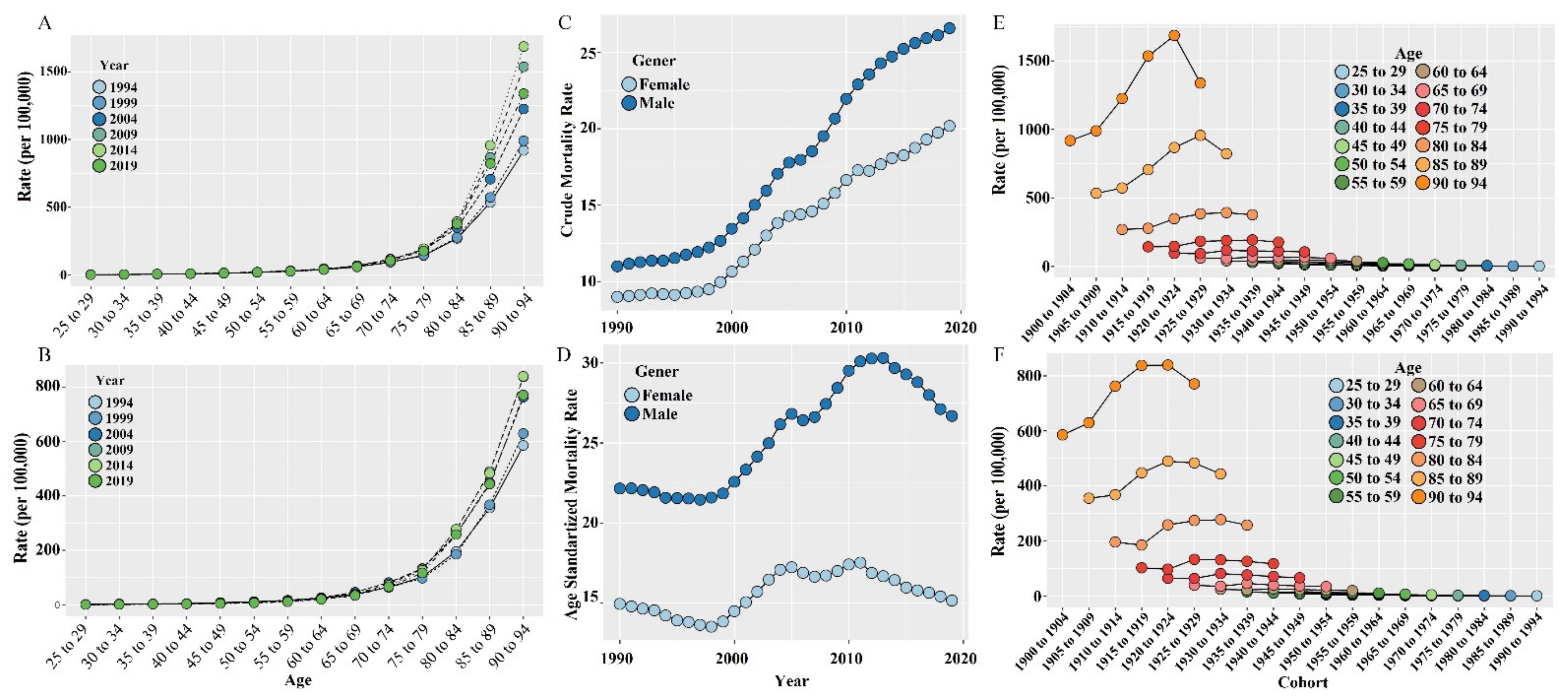
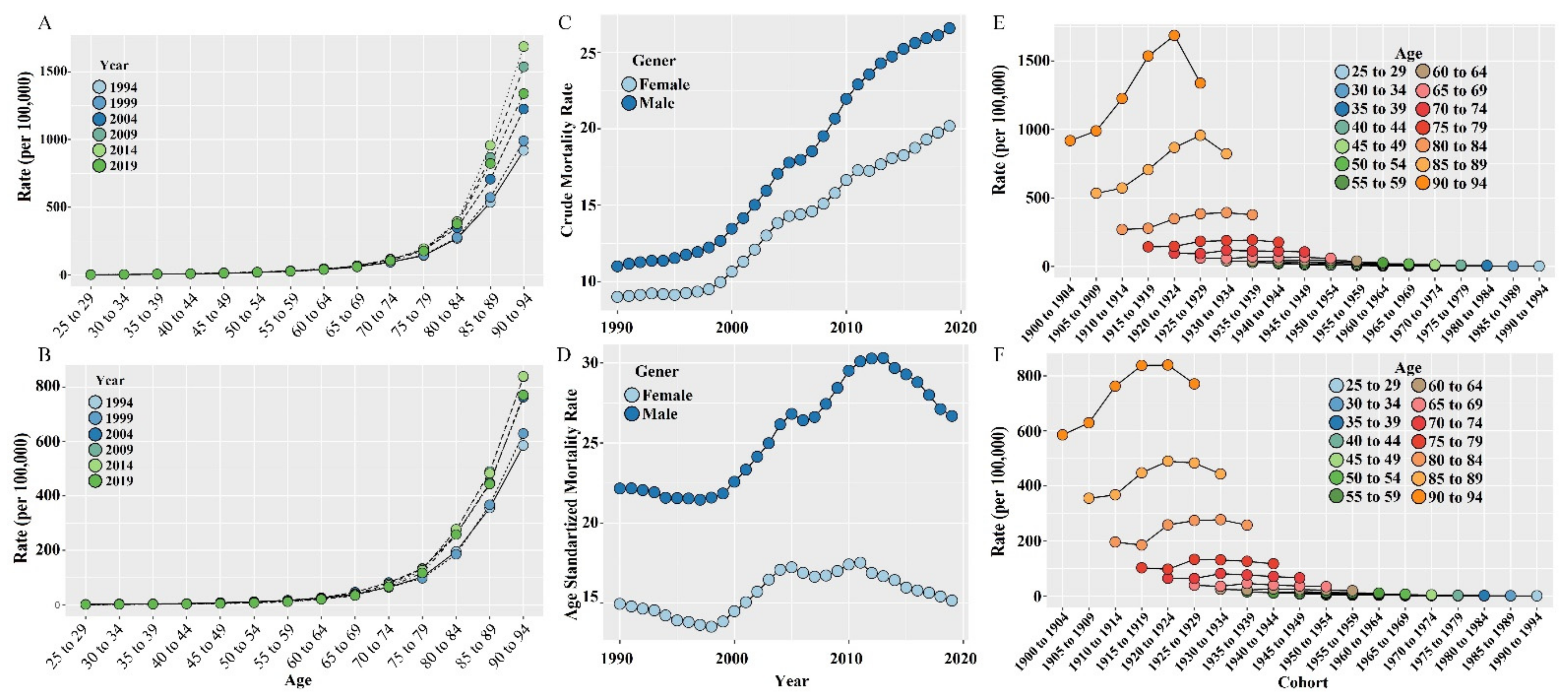
3.1. Long-Term Trend of CMR and ASMR
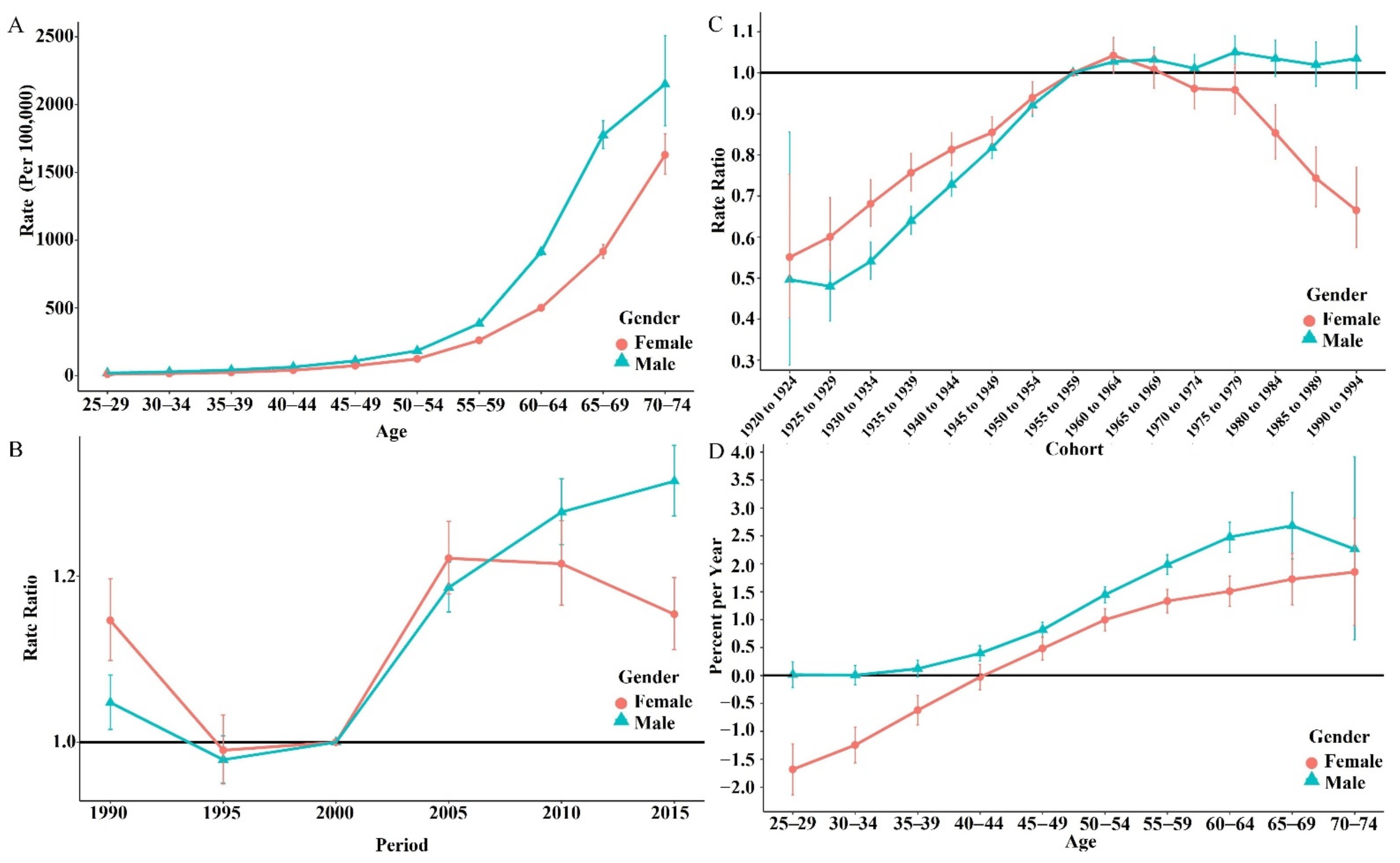
3.2. Age-Period-Cohort Analysis
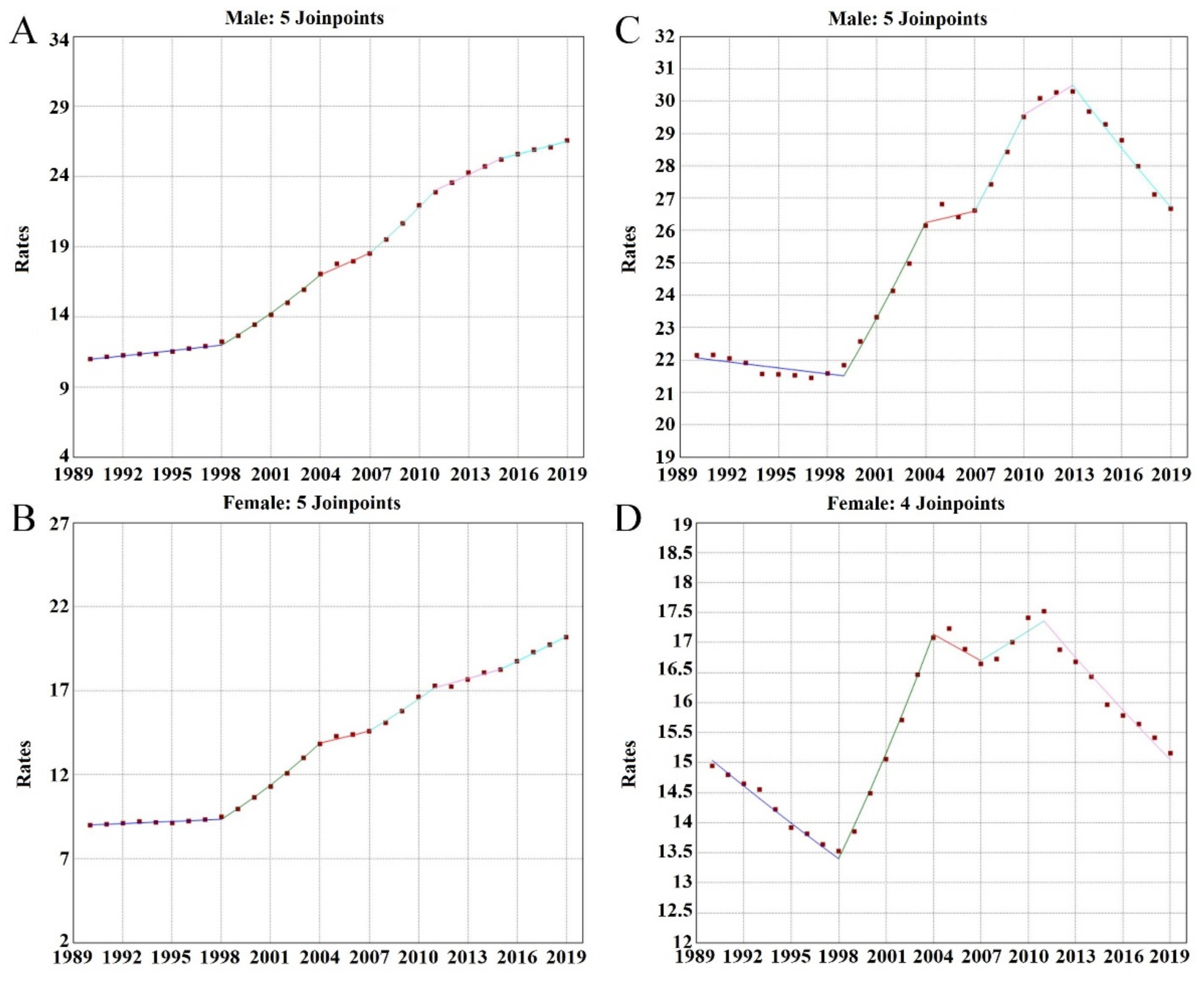
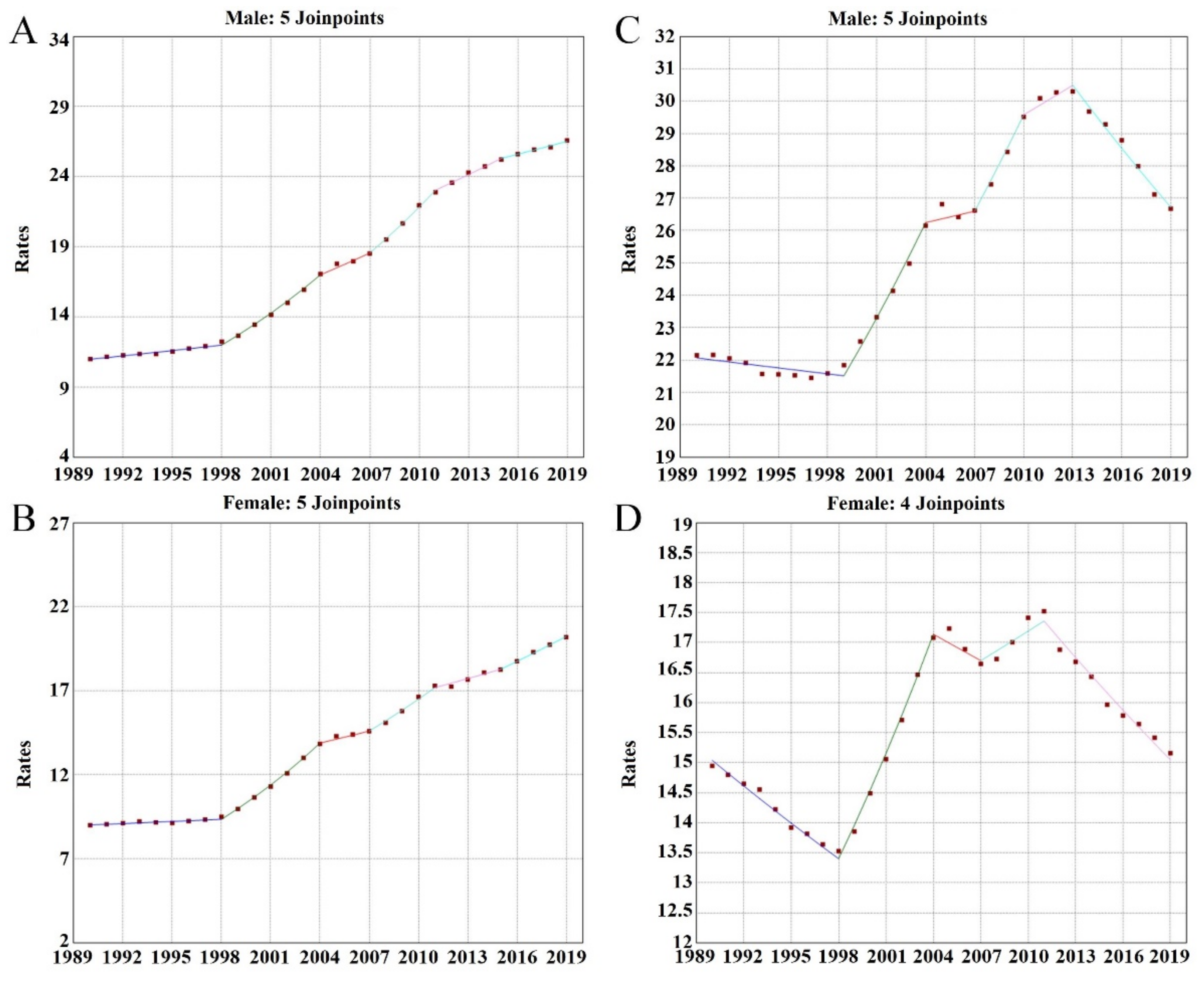
3.3. Joinpoint Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mensah, G.A.; Roth, G.A.; Fuste, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Alkatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Liu, J.; Wang, M.; Zhang, X.; Zhou, M. Epidemiology of cardiovascular disease in China: Current features and implications. Nat. Rev. Cardiol. 2019, 16, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Gu, D.; Zhao, D.; Coxson, P.; Wang, Y.C.; Chen, C.-S.; Liu, J.; Cheng, J.; Bibbins-Domingo, K.; Shen, Y.-M.; et al. Future Cardiovascular Disease in China Markov Model and Risk Factor Scenario Projections From the Coronary Heart Disease Policy Model-China. Circ.-Cardiovasc. Qual. Outcomes 2010, 3, 243–252. [Google Scholar] [CrossRef] [Green Version]
- Requena, T.; Martínez-Cuesta, M.C.; Peláez, C. Diet and microbiota linked in health and disease. Food Funct. 2018, 9, 688–704. [Google Scholar] [CrossRef] [Green Version]
- Badimon, L.; Chagas, P.; Chiva-Blanch, G. Diet and Cardiovascular Disease: Effects of Foods and Nutrients in Classical and Emerging Cardiovascular Risk Factors. Curr. Med. Chem. 2019, 26, 3639–3651. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Guasch-Ferré, M.; Chung, W.; Ruiz-Canela, M.; Toledo, E.; Corella, D.; Bhupathiraju, S.N.; Tobias, D.K.; Tabung, F.K.; Hu, J.; et al. The Mediterranean diet, plasma metabolome, and cardiovascular disease risk. Eur. Heart J. 2020, 41, 2645–2656. [Google Scholar] [CrossRef]
- Joye, I.J. Dietary Fibre from Whole Grains and Their Benefits on Metabolic Health. Nutrients 2020, 12, 3045. [Google Scholar] [CrossRef]
- Kazemi, F.; Danaei, G.; Farzadfar, F.; Moradi, G.; Malik, V.; Parsaeian, M.; Pouraram, H.; Zamaninour, N.; Motlagh, A.R.D. Social awareness of whole grains and the feasibility of replacement with refined grains: A qualitative study. Int. J. Prev. Med. 2021, 12, 12–56. [Google Scholar] [CrossRef]
- Chinese Nutrition Society. The Chinese Dietary Guidelines; People’s Health Publishing House Co. Ltd.: Beijing, China, 2016; pp. 2–31. [Google Scholar]
- Soliman, G.A. Dietary Fiber, Atherosclerosis, and Cardiovascular Disease. Nutrients 2019, 11, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- China CDC. Eighty percent of adults in China have insufficient whole grain intake. Health Guide 2021, 27, 56–57. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- The World Health Data. Global Health Data Exchange. 2019. Available online: http://ghdx.healthdata.org/ (accessed on 10 January 2019).
- He, Y.; Zhao, W.; Zhang, J.; Zhao, L.; Yang, Z.; Huo, J.; Yang, L.; Wang, J.; He, L.; Sun, J.; et al. Data Resource Profile: China National Nutrition Surveys. Int. J. Epidemiol. 2019, 48, 368. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Wei, B.; Zhai, Z.; Zheng, Y.; Yao, J.; Wang, S.; Xiang, D.; Hu, J.; Ye, X.; Yang, S.; et al. Dietary Risk-Related Colorectal Cancer Burden: Estimates From 1990 to 2019. Front. Nutr. 2021, 8, 690663. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Rosenberg, S.; Check, P.; Anderson, W. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2296–2302. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Du, H.; Guo, Y.; Bian, Z.; Yu, C.; Chen, Y.; Yang, L.; Liu, J.; Han, X.; Chen, J.; et al. Coarse Grain Consumption and Risk of Cardiometabolic Diseases: A Prospective Cohort Study of Chinese Adults. J. Nutr. 2022, nxac041. [Google Scholar] [CrossRef]
- Ushula, T.W.; Mamun, A.; Darssan, D.; Wang, W.Y.; Williams, G.M.; Whiting, S.J.; Najman, J.M. Dietary patterns and the risk of abnormal blood lipids among young adults: A prospective cohort study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1165–1174. [Google Scholar] [CrossRef]
- Brown, M.C.; Marciniak, C.M.; Garrett, A.M.; Gaebler-Spira, D.J. Diet quality in adults with cerebral palsy: A modifiable risk factor for cardiovascular disease prevention. Dev. Med. Child. Neurol. 2021, 63, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Busnatu, S.-S.; Salmen, T.; Pana, M.-A.; Rizzo, M.; Stallone, T.; Papanas, N.; Popovic, D.; Tanasescu, D.; Serban, D.; Stoian, A.P. The Role of Fructose as a Cardiovascular Risk Factor: An Update. Metabolites 2022, 12, 67. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Cao, W.; Chi, H.; Wang, J.; Zhang, H.; Liu, J.; Sun, B. Whole cereal grains and potential health effects: Involvement of the gut microbiota. Food Res. Int. 2018, 103, 84–102. [Google Scholar] [CrossRef] [PubMed]
- Vasanrs, D. Age as a risk factor. Med. Clin. N. Am. 2012, 96, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Barber, R.M.; Foreman, K.J.; Ozgoren, A.A.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Abraham, J.P.; Abubakar, I.; Abu-Raddad, L.J.; et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015, 386, 2145–2191. [Google Scholar] [CrossRef] [Green Version]
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Walker, M.; Talley, N. Functional Dyspepsia in the Elderly. Curr. Gastroenterol. Rep. 2019, 21, 54. [Google Scholar] [CrossRef]
- Mai, Q. Status of Wholegrains Consumption and Industrial Development. Agric. Econ. 2021, 6, 75–79. [Google Scholar] [CrossRef]
- Keyes, K.; Li, G. Age–Period–Cohort Modeling. In Injury Research; Springer Press: Boston, MA, USA, 2012; pp. 409–426. [Google Scholar]
- Bell, A. Age period cohort analysis: A review of what we should and shouldn’t do. Ann. Hum. Biol. 2020, 47, 208–217. [Google Scholar] [CrossRef]
- Wang, X. Gender Difference of the Risk Factors for Patients with Coronary Heart Disease. Master’s Thesis, Hebei Medical University, Shijiazhuang, China, 2021. [Google Scholar]
- Hyun, K.; Negrone, A.; Redfern, J.; Atkins, E.; Chow, C.; Kilian, J.; Rajaratnam, R.; Brieger, D. Gender Difference in Secondary Prevention of Cardiovascular Disease and Outcomes Following the Survival of Acute Coronary Syndrome. Heart Lung Circ. 2021, 30, 121–127. [Google Scholar] [CrossRef]
- Mumme, K.; Conlon, C.; Von Hurst, P.; Jones, B.; Stonehouse, W.; Heath, A.-L.; Coad, J.; Haskell-Ramsay, C.; De Seymour, J.; Beck, K. Dietary Patterns, Their Nutrients, and Associations with Socio-Demographic and Lifestyle Factors in Older New Zealand Adults. Nutrients 2020, 12, 3425. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, V.A.; Allès, B.; Feron, G.; Gonzalez, R.; Sulmont-Rossé, C.; Galan, P.; Hercberg, S.; Méjean, C. Sex-Specific Sociodemographic Correlates of Dietary Patterns in a Large Sample of French Elderly Individuals. Nutrients 2016, 8, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reamy, B.; Williams, P.; Kuckel, D. Prevention of Cardiovascular Disease. Prim. Care 2017, 13, 13185–13192. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Segment | No. of Death # | Year | APC (95% CI) | t (p) | |
|---|---|---|---|---|---|
| Male | Trend 1 | 661,850 | 1990~1998 | 1.1 (0.9, 1.3) | 11.7 (<0.001) |
| Trend 2 | 596,401 | 1998~2004 | 6.0 (5.6, 6.3) | 38.6 (<0.001) | |
| Trend 3 | 373,521 | 2004~2007 | 3.0 (1.8, 4.1) | 5.5 (<0.001) | |
| Trend 4 | 592,942 | 2007~2011 | 5.6 (5.0, 6.1) | 23.4 (<0.001) | |
| Trend 5 | 692,046 | 2011~2015 | 2.4 (1.9, 2.8) | 11.9 (<0.001) | |
| Trend 6 | 751,059 | 2015~2019 | 1.2 (0.9, 1.4) | 9.5 (<0.001) | |
| AAPC | - | - | 3.1 (2.9, 3.3) | - (<0.05) * | |
| Female | Trend 1 | 494,414 | 1990~1998 | 0.5 (0.3, 0.6) | 5.6 (<0.001) |
| Trend 2 | 451,587 | 1998~2004 | 6.8 (6.7, 7.1) | 49.1 (<0.001) | |
| Trend 3 | 282,907 | 2004~2007 | 1.7 (0.6, 2.7) | 3.5 (0.004) | |
| Trend 4 | 430,779 | 2007~2011 | 4.2 (3.7, 4.6) | 18.9 (<0.001) | |
| Trend 5 | 482,611 | 2011~2015 | 1.6 (1.1, 2.0) | 7.9 (<0.001) | |
| Trend 6 | 399,331 | 2015~2019 | 2.6 (2.3, 2.8) | 21.4 (<0.001) | |
| AAPC | - | - | 3.0 (2.7, 3.2) | - (<0.05) * | |
| Segment | No. of Death # | Year | APC (95% CI) | t (p) | |
|---|---|---|---|---|---|
| Male | Trend 1 | 746,208 | 1990~1999 | −0.3 (−0.5, −0.1) | −3.4 (0.005) |
| Trend 2 | 512,043 | 1999~2004 | 4.1 (3.5, 4.6) | 15.4 (<0.001) | |
| Trend 3 | 373,521 | 2004~2007 | 0.4 (−1.1, 2.0) | 0.6 (0.549) | |
| Trend 4 | 432,525 | 2007~2010 | 3.6 (2.0, 5.2) | 5.1 (<0.001) | |
| Trend 5 | 497,638 | 2010~2013 | 1.0 (−0.4, 2.4) | 1.6 (0.135) | |
| Trend 6 | 1,105,884 | 2013~2019 | −2.2 (−2.2, −1.9) | −18.1 (<0.001) | |
| AAPC | - | - | 0.7 (0.4, 0.9) | - (<0.05) * | |
| Female | Trend 1 | 494,414 | 1990~1998 | −1.4 (−1.6, −1.3) | −19.0 (<0.001) |
| Trend 2 | 451,587 | 1998~2004 | 4.2 (3.9, 4.5) | 28.2 (<0.001) | |
| Trend 3 | 282,907 | 2004~2007 | −0.9 (−2.1, 0.44) | −1.5 (0.157) | |
| Trend 4 | 430,779 | 2007~2011 | 1.0 (0.4, 1.6) | 3.4 (0.004) | |
| Trend 5 | 881,943 | 2011~2019 | −1.8 (−1.9, 1.6) | −25.1 (<0.001) | |
| AAPC | - | - | 0.0 (−0.2, 0.2) | - (>0.05) * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, F.; Zhang, Y.; Chen, S.; Si, A.; Hu, W. Cardiovascular Disease Mortality Attributable to Low Whole-Grain Intake in CHINA: An Age-Period-Cohort and Joinpoint Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7096. https://doi.org/10.3390/ijerph19127096
Chen F, Zhang Y, Chen S, Si A, Hu W. Cardiovascular Disease Mortality Attributable to Low Whole-Grain Intake in CHINA: An Age-Period-Cohort and Joinpoint Analysis. International Journal of Environmental Research and Public Health. 2022; 19(12):7096. https://doi.org/10.3390/ijerph19127096
Chicago/Turabian StyleChen, Fangyao, Yuxiang Zhang, Shiyu Chen, Aima Si, and Weiwei Hu. 2022. "Cardiovascular Disease Mortality Attributable to Low Whole-Grain Intake in CHINA: An Age-Period-Cohort and Joinpoint Analysis" International Journal of Environmental Research and Public Health 19, no. 12: 7096. https://doi.org/10.3390/ijerph19127096
APA StyleChen, F., Zhang, Y., Chen, S., Si, A., & Hu, W. (2022). Cardiovascular Disease Mortality Attributable to Low Whole-Grain Intake in CHINA: An Age-Period-Cohort and Joinpoint Analysis. International Journal of Environmental Research and Public Health, 19(12), 7096. https://doi.org/10.3390/ijerph19127096