
Association between Exposure to Ambient Air Pollution and the Risk of Rheumatoid Arthritis in Taiwan: A Population-Based Retrospective Cohort Study


 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
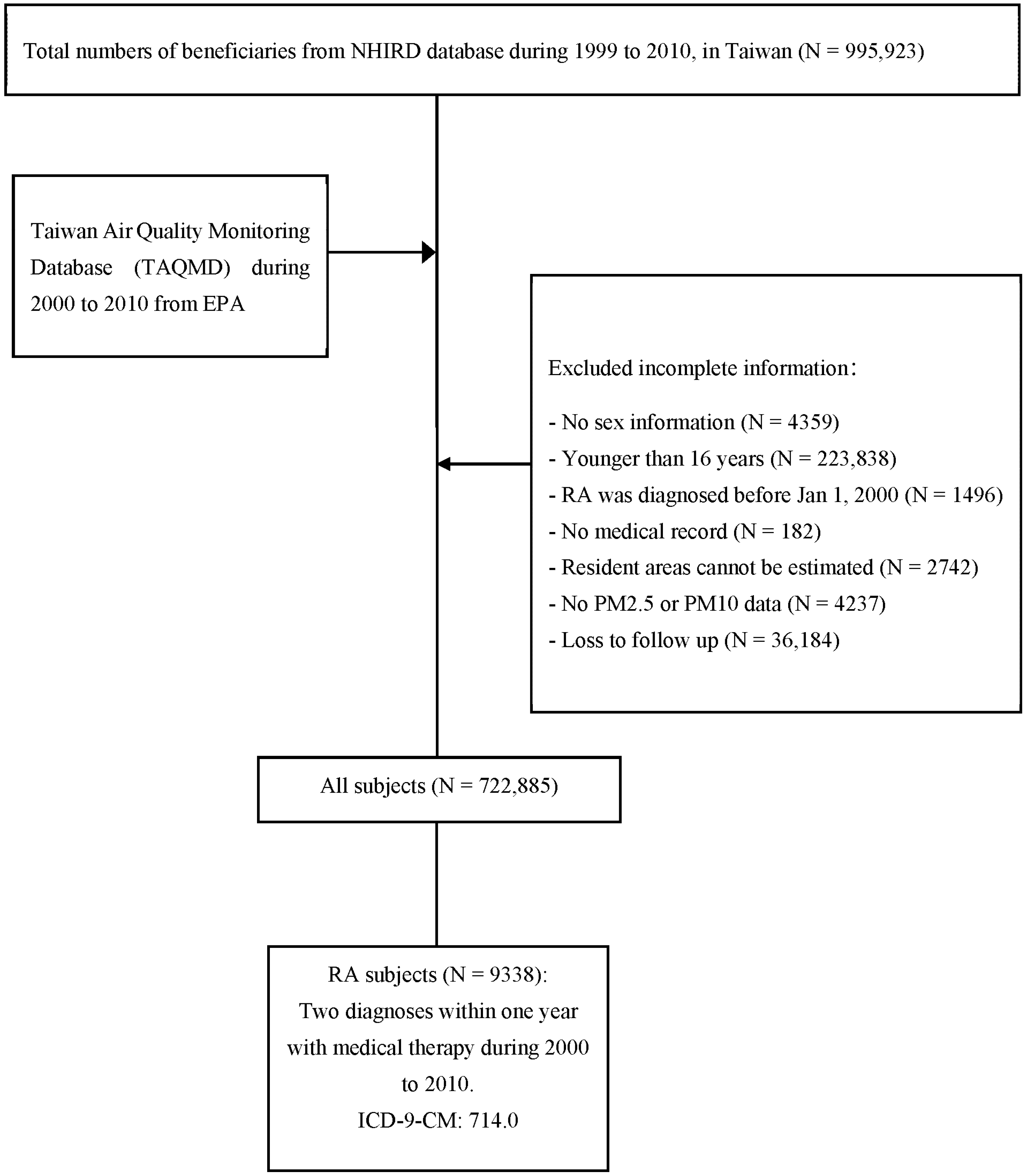
2.1. Data Source
2.2. Study Cohort
2.3. Outcome and Covariates
2.4. Statistical Analysis
3. Results
3.1. The Association between Exposure to PM2.5 and RA
3.2. The Association between Exposure to PM10 and RA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The global burden of rheumatoid arthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Almutairi, K.; Nossent, J.; Preen, D.; Keen, H.; Inderjeeth, C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatol. Int. 2021, 41, 863–877. [Google Scholar] [CrossRef] [PubMed]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Therneau, T.M.; Gabriel, S.E. Is the incidence of rheumatoid arthritis rising?: Results from Olmsted County, Minnesota, 1955–2007. Arthritis Rheumatol. 2010, 62, 1576–1582. [Google Scholar] [CrossRef]
- Hunter, T.M.; Boytsov, N.N.; Zhang, X.; Schroeder, K.; Michaud, K.; Araujo, A.B. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol. Int. 2017, 37, 1551–1557. [Google Scholar] [CrossRef]
- Lai, C.H.; Lai, M.S.; Lai, K.L.; Chen, H.H.; Chiu, Y.M. Nationwide population-based epidemiologic study of rheumatoid arthritis in Taiwan. Clin. Exp. Rheumatol. 2012, 30, 358–363. [Google Scholar]
- Arend, W.P.; Firestein, G.S. Pre-rheumatoid arthritis: Predisposition and transition to clinical synovitis. Nat. Rev. Rheumatol. 2012, 8, 573–586. [Google Scholar] [CrossRef]
- Linn-Rasker, S.P.; van der Helm-van Mil, A.H.; van Gaalen, F.A.; Kloppenburg, M.; de Vries, R.R.; le Cessie, S.; Breedveld, F.C.; Toes, R.E.; Huizinga, T.W. Smoking is a risk factor for anti-CCP antibodies only in rheumatoid arthritis patients who carry HLA-DRB1 shared epitope alleles. Ann. Rheum. Dis. 2006, 65, 366–371. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Payne, J.B.; Yu, F.; Thiele, G.M.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis and Porphyromonas gingivalis in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef]
- Demoruelle, M.K.; Weisman, M.H.; Simonian, P.L.; Lynch, D.A.; Sachs, P.B.; Pedraza, I.F.; Harrington, A.R.; Kolfenbach, J.R.; Striebich, C.C.; Pham, Q.N.; et al. Brief report: Airways abnormalities and rheumatoid arthritis-related autoantibodies in subjects without arthritis: Early injury or initiating site of autoimmunity? Arthritis Rheumatol. 2012, 64, 1756–1761. [Google Scholar] [CrossRef]
- Hutchinson, D.; Moots, R. Cigarette smoking and severity of rheumatoid arthritis. Rheumatology 2001, 40, 1426–1427. [Google Scholar] [CrossRef][Green Version]
- Pedersen, M.; Jacobsen, S.; Klarlund, M.; Pedersen, B.V.; Wiik, A.; Wohlfahrt, J.; Frisch, M. Environmental risk factors differ between rheumatoid arthritis with and without auto-antibodies against cyclic citrullinated peptides. Arthritis Res. Ther. 2006, 8, R133. [Google Scholar] [CrossRef] [PubMed]
- Makrygiannakis, D.; Hermansson, M.; Ulfgren, A.K.; Nicholas, A.P.; Zendman, A.J.; Eklund, A.; Grunewald, J.; Skold, C.M.; Klareskog, L.; Catrina, A.I. Smoking increases peptidylarginine deiminase 2 enzyme expression in human lungs and increases citrullination in BAL cells. Ann. Rheumatol. Dis. 2008, 67, 1488–1492. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K. Ambient air pollution and health. Br. Med. Bull. 2003, 68, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.N.; Xu, Z.; Wu, G.C.; Mao, Y.M.; Liu, L.N.; Qian, W.; Dan, Y.L.; Tao, S.S.; Zhang, Q.; Sam, N.B.; et al. Emerging role of air pollution in autoimmune diseases. Autoimmun. Rev. 2019, 18, 607–614. [Google Scholar] [CrossRef]
- Sigaux, J.; Biton, J.; André, E.; Semerano, L.; Boissier, M.C. Air pollution as a determinant of rheumatoid arthritis. Jt. Bone Spine 2019, 86, 37–42. [Google Scholar] [CrossRef]
- Perricone, C.; Versini, M.; Ben-Ami, D.; Gertel, S.; Watad, A.; Segel, M.J.; Ceccarelli, F.; Conti, F.; Cantarini, L.; Bogdanos, D.P.; et al. Smoke and autoimmunity: The fire behind the disease. Autoimmun. Rev. 2016, 15, 354–374. [Google Scholar] [CrossRef]
- Hart, J.E.; Laden, F.; Puett, R.C.; Costenbader, K.H.; Karlson, E.W. Exposure to traffic pollution and increased risk of rheumatoid arthritis. Environ. Health Perspect. 2009, 117, 1065–1069. [Google Scholar] [CrossRef]
- De Roos, A.J.; Koehoorn, M.; Tamburic, L.; Davies, H.W.; Brauer, M. Proximity to traffic, ambient air pollution, and community noise in relation to incident rheumatoid arthritis. Environ. Health Perspect. 2014, 122, 1075–1080. [Google Scholar] [CrossRef]
- Chen, C.-H.; Wu, C.-D.; Chiang, H.-C.; Chu, D.; Lee, K.-Y.; Lin, W.-Y.; Yeh, J.-I.; Tsai, K.-W.; Guo, Y.-L.L. The effects of fine and coarse particulate matter on lung function among the elderly. Sci. Rep. 2019, 9, 14790. [Google Scholar] [CrossRef]
- Genc, S.; Zadeoglulari, Z.; Fuss, S.H.; Genc, K. The adverse effects of air pollution on the nervous system. J. Toxicol. 2012, 2012, 782462. [Google Scholar] [CrossRef] [PubMed]
- Puett, R.C.; Hart, J.E.; Suh, H.; Mittleman, M.; Laden, F. Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environ. Health Perspect. 2011, 119, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Lin, Y.; Lin, Y.; Zhong, Y.; Yu, H.; Huang, Y.; Yang, J.; Cai, Y.; Liu, F.; Li, Y.; et al. PM2.5 induces pulmonary microvascular injury in COPD via METTL16-mediated m6A modification. Environ. Pollut. 2022, 303, 119115. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.E.; Källberg, H.; Laden, F.; Bellander, T.; Costenbader, K.H.; Holmqvist, M.; Klareskog, L.; Alfredsson, L.; Karlson, E.W. Ambient air pollution exposures and risk of rheumatoid arthritis: Results from the Swedish EIRA case-control study. Ann. Rheum. Dis. 2013, 72, 888–894. [Google Scholar] [CrossRef]
- Hart, J.E.; Källberg, H.; Laden, F.; Costenbader, K.H.; Yanosky, J.D.; Klareskog, L.; Alfredsson, L.; Karlson, E.W. Ambient air pollution exposures and risk of rheumatoid arthritis. Arthritis Care Res. 2013, 65, 1190–1196. [Google Scholar] [CrossRef]
- Chang, K.; Yang, S.M.; Kim, S.H.; Han, K.H.; Park, S.J.; Shin, J.I. Smoking and rheumatoid arthritis. Int. J. Mol. Sci. 2014, 15, 22279–22295. [Google Scholar] [CrossRef]
- Heliövaara, M.; Aho, K.; Aromaa, A.; Knekt, P.; Reunanen, A. Smoking and risk of rheumatoid arthritis. J. Rheumatol. 1993, 20, 1830–1835. [Google Scholar]
- Barr, J.; Sharma, C.S.; Sarkar, S.; Wise, K.; Dong, L.; Periyakaruppan, A.; Ramesh, G.T. Nicotine induces oxidative stress and activates nuclear transcription factor kappa B in rat mesencephalic cells. Mol. Cell Biochem. 2007, 297, 93–99. [Google Scholar] [CrossRef]
- Bracke, K.; Cataldo, D.; Maes, T.; Gueders, M.; Noël, A.; Foidart, J.M.; Brusselle, G.; Pauwels, R.A. Matrix metalloproteinase-12 and cathepsin D expression in pulmonary macrophages and dendritic cells of cigarette smoke-exposed mice. Int. Arch. Allergy Immunol. 2005, 138, 169–179. [Google Scholar] [CrossRef]
- Chang, K.H.; Hsu, C.C.; Muo, C.H.; Hsu, C.Y.; Liu, H.C.; Kao, C.H.; Chen, C.Y.; Chang, M.Y.; Hsu, Y.C. Air pollution exposure increases the risk of rheumatoid arthritis: A longitudinal and nationwide study. Environ. Int. 2016, 94, 495–499. [Google Scholar] [CrossRef]
- Bernatsky, S.; Smargiassi, A.; Joseph, L.; Awadalla, P.; Colmegna, I.; Hudson, M.; Fritzler, M.J. Industrial air emissions, and proximity to major industrial emitters, are associated with anti-citrullinated protein antibodies. Environ. Res. 2017, 157, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Smargiassi, A.; Hatzopoulou, M.; Colmegna, I.; Hudson, M.; Fritzler, M.J.; Awadalla, P.; Bernatsky, S. Long-term exposure to a mixture of industrial SO2, NO2, and PM2.5 and anti-citrullinated protein antibody positivity. Environ. Health 2020, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Choi, S.; Kim, K.; Chang, J.; Kim, S.M.; Kim, S.R.; Lee, G.; Son, J.S.; Kim, K.H.; Lee, E.Y.; et al. Association of particulate matter with autoimmune rheumatic diseases among adults in South Korea. Rheumatology 2021, 60, 5117–5126. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Joo, H.S.; Lee, K.; Jang, M.; Kim, S.D.; Kim, I.; Borlaza, L.J.S.; Lim, H.; Shin, H.; Chung, K.H.; et al. Differential toxicities of fine particulate matters from various sources. Sci. Rep. 2018, 8, 17007. [Google Scholar] [CrossRef]
- Essouma, M.; Noubiap, J.J. Is air pollution a risk factor for rheumatoid arthritis? J. Inflamm. 2015, 12, 48. [Google Scholar] [CrossRef]
- van der Woude, D.; Catrina, A.I. HLA and anti-citrullinated protein antibodies: Building blocks in RA. Best Pract. Res. Clin. Rheumatol. 2015, 29, 692–705. [Google Scholar] [CrossRef]
- Wu, Q.; Xu, Z.; Dan, Y.L.; Cheng, J.; Zhao, C.N.; Mao, Y.M.; Xiang, K.; Hu, Y.Q.; He, Y.S.; Pan, H.F. Association between traffic-related air pollution and hospital readmissions for rheumatoid arthritis in Hefei, China: A time-series study. Environ. Pollut. 2021, 268, 115628. [Google Scholar] [CrossRef]
- Di, D.; Zhang, L.; Wu, X.; Leng, R. Long-term exposure to outdoor air pollution and the risk of development of rheumatoid arthritis: A systematic review and meta-analysis. Semin. Arthritis Rheumatol. 2020, 50, 266–275. [Google Scholar] [CrossRef]
- Adami, G.; Viapiana, O.; Rossini, M.; Orsolini, G.; Bertoldo, E.; Giollo, A.; Gatti, D.; Fassio, A. Association between environmental air pollution and rheumatoid arthritis flares. Rheumatology 2021, 60, 4591–4597. [Google Scholar] [CrossRef]
- Hwa-Lung, Y.; Chih-Hsin, W. Retrospective prediction of intraurban spatiotemporal distribution of PM2.5 in Taipei. Atmos. Environ. 2010, 44, 3053–3065. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | ALL (N = 722,885) | % | RA (N = 9338) | % | |
|---|---|---|---|---|---|
| Gender | Male | 366,593 | 49.29 | 2936 | 31.44 |
| Female | 356,292 | 50.71 | 6402 | 68.56 | |
| Age | Mean (SD) | 40.34 (16.79) | 54.61 (15.48) | ||
| 16–38 | 367,831 | 50.88 | 1357 | 14.53 | |
| 39–60 | 246,643 | 34.12 | 4560 | 48.83 | |
| >60 | 108,411 | 15.00 | 3421 | 36.64 | |
| PM2.5 | |||||
| Q1 | 276,272 | 38.22 | 3683 | 39.44 | |
| Q2 | 163,683 | 22.64 | 2111 | 22.61 | |
| Q3 | 115,099 | 15.92 | 1591 | 17.04 | |
| Q4 | 167,831 | 23.22 | 1953 | 20.91 | |
| PM10 | |||||
| Q1 | 282,802 | 39.11 | 3860 | 41.34 | |
| Q2 | 148,437 | 20.53 | 1825 | 19.54 | |
| Q3 | 166,714 | 23.06 | 2256 | 24.16 | |
| Q4 | 125.32 | 17.30 | 1397 | 14.96 | |
| Follow years | Mean | 10.27 | 4.7 | ||
| Pollutant Levels | Event | PY | IR | cHR | 95%CI | aHR | 95%CI |
|---|---|---|---|---|---|---|---|
| All | |||||||
| Q1 | 3683 | 2,844,052 | 12.95 | 0.928 | 0.921–0.935 | 0.974 | 0.967–0.981 |
| Q2 | 2111 | 1,668,022 | 12.66 | 0.949 | 0.934–0.964 | 0.963 | 0.948–0.978 |
| Q3 | 1591 | 1,168,749 | 13.61 | 0.979 | 0.966–0.993 | 0.946 | 0.934–0.968 |
| Q4 | 1953 | 1,721,764 | 11.34 | 1.010 | 1.001–1.019 | 1.053 | 1.043–1.063 |
| Male | |||||||
| Q1 | 1101 | 1,391,484 | 7.91 | 0.933 | 0.920–0.945 | 0.982 | 0.969–0.994 |
| Q2 | 681 | 866,044 | 7.86 | 0.962 | 0.937–0.987 | 0.976 | 0.953–1.000 |
| Q3 | 522 | 590,660 | 8.84 | 0.993 | 0.970–1.017 | 0.966 | 0.944–0.989 |
| Q4 | 632 | 866,440 | 7.29 | 1.019 | 1.002–1.035 | 1.052 | 1.033–1.070 |
| Female | |||||||
| Q1 | 2582 | 1,452,568 | 17.78 | 0.926 | 0.918–0.935 | 0.970 | 0.962–0.978 |
| Q2 | 1430 | 801,978 | 17.83 | 0.941 | 0.922–0.961 | 0.955 | 0.936–0.973 |
| Q3 | 1069 | 578,088 | 18.49 | 0.972 | 0.956–0.989 | 0.953 | 0.922–0.969 |
| Q4 | 1321 | 855,324 | 15.44 | 1.004 | 0.993–1.016 | 1.053 | 1.040–1.065 |
| Pollutant Levels | Event | PY | IR | cHR | 95%CI | aHR | 95%CI |
|---|---|---|---|---|---|---|---|
| All | |||||||
| Q1 | 3860 | 2,907,882 | 13.27 | 0.946 | 0.942–0.951 | 0.984 | 0.980–0.988 |
| Q2 | 1825 | 1,513,200 | 12.06 | 0.950 | 0.941–0.958 | 0.982 | 0.973–0.991 |
| Q3 | 2256 | 1,696,087 | 13.30 | 1.019 | 1.013–1.026 | 0.998 | 0.994–1.003 |
| Q4 | 1397 | 1,285,417 | 10.87 | 0.998 | 0.991–1.005 | 1.048 | 1.039–1.058 |
| Male | |||||||
| Q1 | 1160 | 1,424,055 | 8.15 | 0.952 | 0.944–0.959 | 0.992 | 0.985–0.998 |
| Q2 | 584 | 788,026 | 7.41 | 0.959 | 0.944–0.973 | 1.001 | 0.987–1.015 |
| Q3 | 767 | 857,465 | 8.95 | 1.020 | 1.009–1.031 | 0.999 | 0.990–1.006 |
| Q4 | 425 | 645,083 | 6.59 | 1.009 | 0.995–1.022 | 1.053 | 1.036–1.070 |
| Female | |||||||
| Q1 | 2700 | 1483,828 | 18.20 | 0.943 | 0.938–0.949 | 0.981 | 0.976–0.986 |
| Q2 | 1241 | 725,174 | 17.11 | 0.944 | 0.933–0.955 | 0.971 | 0.960–0.983 |
| Q3 | 1489 | 838,622 | 17.76 | 1.019 | 1.011–1.027 | 0.998 | 0.992–1.004 |
| Q4 | 972 | 640,334 | 15.18 | 0.993 | 0.984–1.001 | 1.046 | 1.035–1.057 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, W.-C.; Chou, L.-W.; Wang, R.-Y.; Doan, T.-N.; Yu, H.-L.; Chou, T.-H.; Liu, K.-Y.; Wu, P.-C.; Shieh, S.-H. Association between Exposure to Ambient Air Pollution and the Risk of Rheumatoid Arthritis in Taiwan: A Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 7006. https://doi.org/10.3390/ijerph19127006
Ho W-C, Chou L-W, Wang R-Y, Doan T-N, Yu H-L, Chou T-H, Liu K-Y, Wu P-C, Shieh S-H. Association between Exposure to Ambient Air Pollution and the Risk of Rheumatoid Arthritis in Taiwan: A Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7006. https://doi.org/10.3390/ijerph19127006
Chicago/Turabian StyleHo, Wen-Chao, Li-Wei Chou, Ruey-Yun Wang, Thanh-Nhan Doan, Hwa-Lung Yu, Ting-Hsuan Chou, Kang-Yung Liu, Po-Chang Wu, and Shwn-Huey Shieh. 2022. "Association between Exposure to Ambient Air Pollution and the Risk of Rheumatoid Arthritis in Taiwan: A Population-Based Retrospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 12: 7006. https://doi.org/10.3390/ijerph19127006
APA StyleHo, W.-C., Chou, L.-W., Wang, R.-Y., Doan, T.-N., Yu, H.-L., Chou, T.-H., Liu, K.-Y., Wu, P.-C., & Shieh, S.-H. (2022). Association between Exposure to Ambient Air Pollution and the Risk of Rheumatoid Arthritis in Taiwan: A Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 19(12), 7006. https://doi.org/10.3390/ijerph19127006