
Neighbourhood Socioeconomic Processes and Dynamics and Healthy Ageing: A Scoping Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Theoretical Background
1.1.1. Neighbourhood Socioeconomic Processes and Dynamics
1.1.2. Mechanisms Connecting Neighbourhood Structure and Dynamics and Healthy Ageing
- processes of influence by neighbours (social contagion) where people change their behaviours, aspirations, and attitudes based on contact with their peers;
- processes of adhering to local social norms (collective socialisation) through neighbourhood role models or social pressures;
- processes of transmission of information or resources (social networks) through neighbour networks;
- processes of influence in the behaviour of residents through a degree of social disorder (social cohesion and control) changing also psychological reactions;
- processes of competition due to limited resources in the neighbourhood;
- processes of relative deprivation where people tend to feel inferior to their neighbourhood peers that have reached a higher socioeconomic position;
- and finally, the process of parental mediation where the actions of parents are influenced by the environment of the neighbourhood and, therefore, affect the way they raise their children [38].
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Selection of Studies
2.5. Data Extraction
3. Results
3.1. General Characteristics of the Included Studies
3.2. Definition and Measurement of Neighbourhood Socioeconomic Processes and Dynamics
3.2.1. Geographical Unit of Analysis
3.2.2. Exposures
Gentrification
Segregation
Urban Renewal
Neighbourhood Socioeconomic Deprivation
3.2.3. Measurement of Healthy Ageing
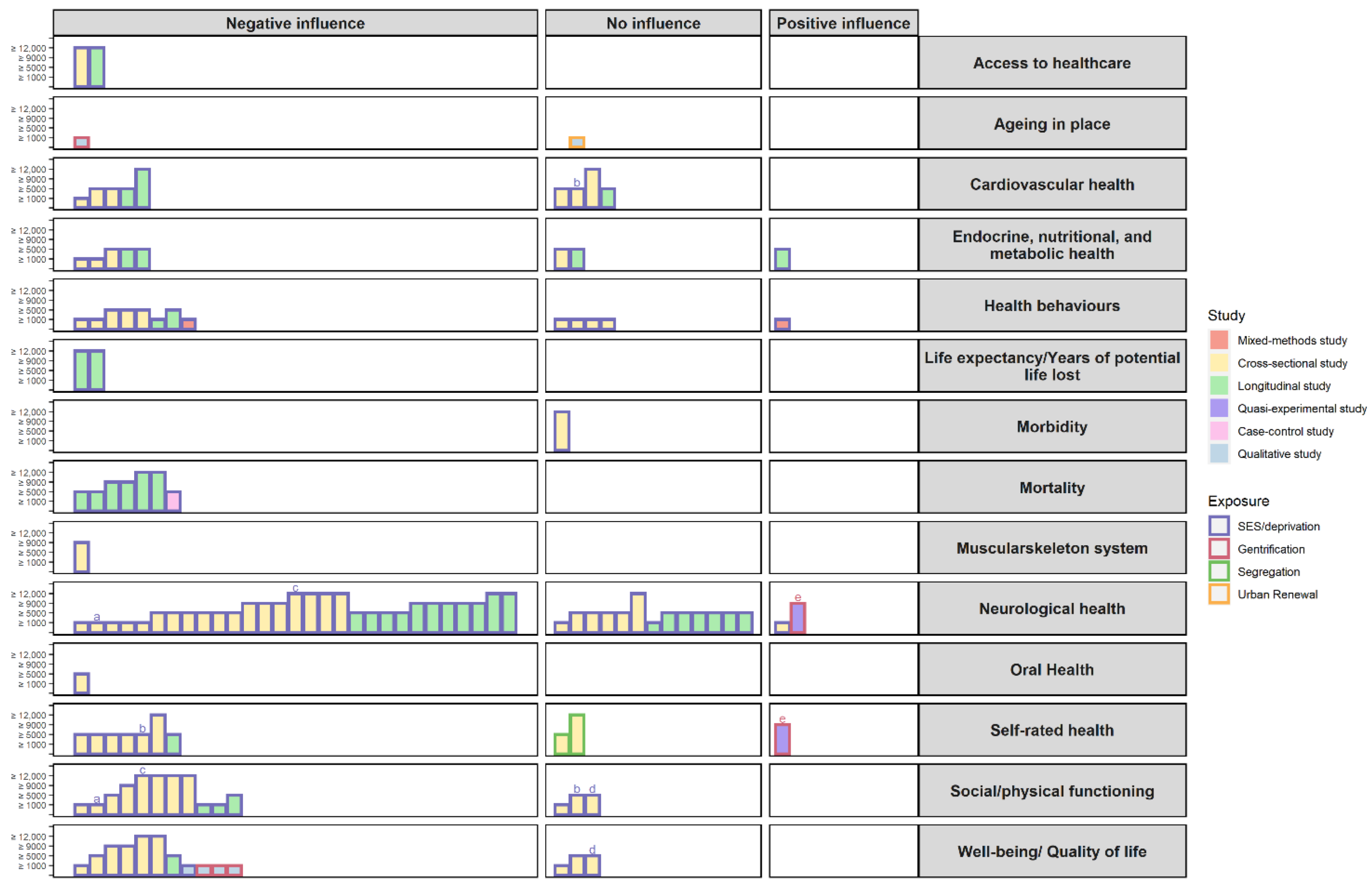
3.2.4. Associations
Gentrification
Segregation
Urban Renewal
Neighbourhood Socioeconomic Deprivation
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2020 Highlights: Living Arrangements of Older Persons; United Nations: New York, NY, USA, 2020. [Google Scholar]
- United Nations. World Population Ageing 2019; United Nations: New York, NY, USA, 2020. [Google Scholar]
- OECD. Healthy Life Expectancy at Birth and at Age 65. Available online: https://www.oecd-ilibrary.org/content/component/62efef1d-en (accessed on 7 June 2021).
- Zaninotto, P.; Head, J.; Steptoe, A. Behavioural risk factors and healthy life expectancy: Evidence from two longitudinal studies of ageing in England and the US. Sci. Rep. 2020, 10, 6955. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2021: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Eurostat. Mortality and Life Expectancy Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Mortality_and_life_expectancy_statistics (accessed on 7 June 2021).
- Eurostat. Healthy Life Years Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthy_life_years_statistics#Healthy_life_years_at_birth (accessed on 7 June 2021).
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; pp. 28–30. [Google Scholar]
- Alidoust, S.; Bosman, C. Planning for an ageing population: Links between social health, neighbourhood environment and the elderly. Aust. Plan. 2015, 52, 177–186. [Google Scholar] [CrossRef]
- Feng, J.; Tang, S.; Chuai, X. The impact of neighbourhood environments on quality of life of elderly people: Evidence from Nanjing, China. Urban Stud. 2017, 55, 2020–2039. [Google Scholar] [CrossRef]
- Rojo Perez, F.; Fernandez-Mayoralas Fernandez, G.; Pozo Rivera, E.; Manuel Rojo Abuin, J. Ageing in Place: Predictors of the Residential Satisfaction of Elderly. Soc. Indic. Res. 2001, 54, 173–208. [Google Scholar] [CrossRef]
- Diez-Roux, A.V. Bringing context back into epidemiology: Variables and fallacies in multilevel analysis. Am. J. Public Health 1998, 88, 216–222. [Google Scholar] [CrossRef]
- Mechanic, D. Social research in health and the American sociopolitical context: The changing fortunes of medical sociology. Soc. Sci. Med. 1993, 36, 95–102. [Google Scholar] [CrossRef]
- Macintyre, S.; Maciver, S.; Sooman, A. Area, Class and Health: Should we be Focusing on Places or People? J. Soc. Policy 1993, 22, 213–234. [Google Scholar] [CrossRef]
- Lynch, J.; Kaplan, G. Socioeconomic Position. In Social Epidemiology; Berkman, L.F., Kawachi, I., Eds.; Oxford University Press: New York, NY, USA, 2000; p. 13. [Google Scholar]
- Beyers, J.M.; Bates, J.E.; Pettit, G.S.; Dodge, K.A. Neighborhood structure, parenting processes, and the development of youths’ externalizing behaviors: A multilevel analysis. Am. J. Community Psychol. 2003, 31, 35–53. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Aikins, E.K. Environment, Diseases, and Health Interrelationships. In Elements of Health and Medical Geography; Kendall Hunt Publishing Company: Dubuque, IA, USA, 2019; p. 115. [Google Scholar]
- Frohlich, K.L. Area Effects on Behaviour and Lifestyle: The Spatiality of Injustice. In Neighbourhood Structure and Health Promotion; Stock, C., Ellaway, A., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Ribeiro, A.I.; Fraga, S.; Severo, M.; Kelly-Irving, M.; Delpierre, C.; Stringhini, S.; Kivimaki, M.; Joost, S.; Guessous, I.; Severi, G.; et al. Association of neighbourhood disadvantage and individual socioeconomic position with all-cause mortality: A longitudinal multicohort analysis. Lancet Public Health 2022, 7, e447–e457. [Google Scholar] [CrossRef]
- United Nations Department of Economic Social Affairs. World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Neighborhood Socioeconomic Status and Health: Context or Composition? City Community 2008, 7, 163–179. [Google Scholar] [CrossRef]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 2). J. Epidemiol. Community Health 2006, 60, 95–101. [Google Scholar] [CrossRef]
- Pornet, C.; Delpierre, C.; Dejardin, O.; Grosclaude, P.; Launay, L.; Guittet, L.; Lang, T.; Launoy, G. Construction of an adaptable European transnational ecological deprivation index: The French version. J. Epidemiol. Community Health 2012, 66, 982–989. [Google Scholar] [CrossRef]
- Lamnisos, D.; Lambrianidou, G.; Middleton, N. Small-area socioeconomic deprivation indices in Cyprus: Development and association with premature mortality. BMC Public Health 2019, 19, 627. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.I.; Mayer, A.; Miranda, A.; Pina, M.F. The Portuguese Version of the European Deprivation Index: An Instrument to Study Health Inequalities. Acta Med. Port. 2017, 30, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Zadnik, V.; Guillaume, E.; Lokar, K.; Žagar, T.; Primic Žakelj, M.; Launoy, G.; Launay, L. Slovenian Version of The European Deprivation Index at Municipal Level. Zdr. Varst. 2018, 57, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Schelling, T.C. Dynamic models of segregation. J. Math. Sociol. 1971, 1, 143–186. [Google Scholar] [CrossRef]
- Duncan, O.D.; Duncan, B. A Methodological Analysis of Segregation Indexes. Am. Sociol. Rev. 1955, 20, 210–217. [Google Scholar] [CrossRef]
- White, M.J.; Kim, A.H. Residential Segregation. In Encyclopedia of Social Measurement; Kempf-Leonard, K., Ed.; Elsevier: New York, NY, USA, 2005; pp. 403–409. [Google Scholar] [CrossRef]
- Schwirian, K.P. Models of Neighborhood Change. Annu. Rev. Sociol. 1983, 9, 83–102. [Google Scholar] [CrossRef]
- Scott, J.; Marshall, G. Invasion-Succession Model; Oxford University Press: Oxford, UK, 2009. [Google Scholar] [CrossRef]
- Urban Displacement Project. What Are Gentrification and Displacement. Available online: https://www.urbandisplacement.org/about/what-are-gentrification-and-displacement/ (accessed on 19 September 2021).
- United Nations Human Settlements Programme (Ed.) Leading Change: Delivering the New Urban Agenda through Urban and Territorial Planning; UN-Habitat: Kuala Lumpur, Malaysia, 2018. [Google Scholar]
- Raman, S. Gentrification. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 2509–2512. [Google Scholar] [CrossRef]
- Modai-Snir, T.; van Ham, M. Structural and Exchange Components in Processes of Neighbourhood Change: A Social Mobility Approach. Appl. Spat. Anal. Policy 2019, 12, 423–443. [Google Scholar] [CrossRef]
- Richards, R. Urban Renewal. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 6867–6868. [Google Scholar] [CrossRef]
- Mehdipanah, R.; Manzano, A.; Borrell, C.; Malmusi, D.; Rodriguez-Sanz, M.; Greenhalgh, J.; Muntaner, C.; Pawson, R. Exploring complex causal pathways between urban renewal, health and health inequality using a theory-driven realist approach. Soc. Sci. Med. 2015, 124, 266–274. [Google Scholar] [CrossRef]
- Galster, G.C. The Mechanism(s) of Neighbourhood Effects: Theory, Evidence, and Policy Implications. In Neighbourhood Effects Research: New Perspectives; van Ham, M., Manley, D., Bailey, N., Simpson, L., Maclennan, D., Eds.; Springer: Dordrecht, The Netherlands, 2012; pp. 23–56. [Google Scholar] [CrossRef]
- Ball, K.; Jeffery, R.W.; Abbott, G.; McNaughton, S.A.; Crawford, D. Is healthy behavior contagious: Associations of social norms with physical activity and healthy eating. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 86. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuis, J.; van Ham, M.; Yu, R.; Branje, S.; Meeus, W.; Hooimeijer, P. Being Poorer Than the Rest of the Neighborhood: Relative Deprivation and Problem Behavior of Youth. J. Youth Adolesc. 2017, 46, 1891–1904. [Google Scholar] [CrossRef] [PubMed]
- Kress, S.; Razum, O.; Zolitschka, K.A.; Breckenkamp, J.; Sauzet, O. Does social cohesion mediate neighbourhood effects on mental and physical health? Longitudinal analysis using German Socio-Economic Panel data. BMC Public Health 2020, 20, 1043. [Google Scholar] [CrossRef]
- Nishio, M.; Takagi, D.; Shinozaki, T.; Kondo, N. Community social networks, individual social participation and dietary behavior among older Japanese adults: Examining mediation using nonlinear structural equation models for three-wave longitudinal data. Prev. Med. 2021, 149, 106613. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S.; Jalaludin, B. Does rising crime lead to increasing distress? Longitudinal analysis of a natural experiment with dynamic objective neighbourhood measures. Soc. Sci. Med. 2015, 138, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Paciência, I.; Moreira, A.; Moreira, C.; Cavaleiro Rufo, J.; Sokhatska, O.; Rama, T.; Hoffimann, E.; Santos, A.C.; Barros, H.; Ribeiro, A.I. Neighbourhood green and blue spaces and allergic sensitization in children: A longitudinal study based on repeated measures from the Generation XXI cohort. Sci. Total Environ. 2021, 772, 145394. [Google Scholar] [CrossRef]
- Hamra, G.B.; Guha, N.; Cohen, A.; Laden, F.; Raaschou-Nielsen, O.; Samet, J.M.; Vineis, P.; Forastiere, F.; Saldiva, P.; Yorifuji, T.; et al. Outdoor particulate matter exposure and lung cancer: A systematic review and meta-analysis. Environ. Health Perspect. 2014, 122, 906–911. [Google Scholar] [CrossRef]
- Wilson-Genderson, M.; Pruchno, R. Effects of neighborhood violence and perceptions of neighborhood safety on depressive symptoms of older adults. Soc. Sci. Med. 2013, 85, 43–49. [Google Scholar] [CrossRef]
- Ailshire, J.A.; Clarke, P. Fine particulate matter air pollution and cognitive function among U.S. older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 322–328. [Google Scholar] [CrossRef]
- Lu, P.; Shelley, M.; Kong, D. Unmet Community Service Needs and Life Satisfaction Among Chinese Older Adults: A Longitudinal Study. Soc. Work Public Health 2021, 36, 665–676. [Google Scholar] [CrossRef]
- Tran, E.; Blankenship, K.; Whittaker, S.; Rosenberg, A.; Schlesinger, P.; Kershaw, T.; Keene, D. My neighborhood has a good reputation: Associations between spatial stigma and health. Health Place 2020, 64, 102392. [Google Scholar] [CrossRef] [PubMed]
- Shortt, N.K.; Tisch, C.; Pearce, J.; Mitchell, R.; Richardson, E.A.; Hill, S.; Collin, J. A cross-sectional analysis of the relationship between tobacco and alcohol outlet density and neighbourhood deprivation. BMC Public Health 2015, 15, 1014. [Google Scholar] [CrossRef]
- Rosso, A.L.; Grubesic, T.H.; Auchincloss, A.H.; Tabb, L.P.; Michael, Y.L. Neighborhood amenities and mobility in older adults. Am. J. Epidemiol. 2013, 178, 761–769. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Kuh, D.; Karunananthan, S.; Bergman, H.; Cooper, R. A life-course approach to healthy ageing: Maintaining physical capability. Proc. Nutr. Soc. 2014, 73, 237–248. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Ageing, Older Persons, and the 2030 Agenda for Sustainable Development; United Nations Development Programme: New York, NY, USA, 2017. [Google Scholar]
- Buffel, T.; Phillipson, C. Ageing in a Gentrifying Neighbourhood: Experiences of Community Change in Later Life. Sociol. J. Br. Sociol. Assoc. 2019, 53, 987–1004. [Google Scholar] [CrossRef]
- Burns, V.F.; Lavoie, J.P.; Rose, D. Revisiting the role of neighbourhood change in social exclusion and inclusion of older people. J. Aging Res. 2012, 2012, 148287. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.J.; Lehning, A.J.; Kim, K. Aging in Place in Gentrifying Neighborhoods: Implications for Physical and Mental Health. Gerontologist 2018, 58, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Weil, J. Relationship to Place for Older Adults in a New York City Neighborhood Undergoing Gentrification: A Discourse Analysis. City Community 2019, 18, 1267–1286. [Google Scholar] [CrossRef]
- Domínguez-Parraga, L. The effects of gentrification on the elderly: A case study in the city of Cáceres. Soc. Sci. 2020, 9, 154. [Google Scholar] [CrossRef]
- Robert, S.A.; Ruel, E. Racial segregation and health disparities between Black and White older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2006, 61, S203–S211. [Google Scholar] [CrossRef]
- Deng, G.; Mao, L. Spatially Explicit Age Segregation Index and Self-Rated Health of Older Adults in US Cities. ISPRS Int. J. Geo-Inf. 2018, 7, 351. [Google Scholar] [CrossRef]
- Lager, D.; Van Hoven, B.; Huigen, P.P.P. Dealing with change in old age: Negotiating working-class belonging in a neighbourhood in the process of urban renewal in the Netherlands. Geoforum 2013, 50, 54–61. [Google Scholar] [CrossRef]
- Behanova, M.; Katreniakova, Z.; Nagyova, I.; van Ameijden, E.J.; Dijkshoorn, H.; van Dijk, J.P.; Reijneveld, S.A. The effect of neighbourhood unemployment on health-risk behaviours in elderly differs between Slovak and Dutch cities. Eur. J. Public Health 2015, 25, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Behanova, M.; Katreniakova, Z.; Nagyova, I.; van Ameijden, E.J.C.; van Dijk, J.P.; Reijneveld, S.A. Elderly from lower socioeconomic groups are more vulnerable to mental health problems, but area deprivation does not contribute: A comparison between Slovak and Dutch cities. Eur. J. Public Health 2017, 27, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; Barnett, A.; Van Cauwenberg, J.; Zhang, C.J.P.; Sit, C.H.P.; Cerin, E. Main and interacting effects of physical activity and sedentary time on older adults’ BMI: The moderating roles of socio-demographic and environmental attributes. PLoS ONE 2020, 15, e0235833. [Google Scholar] [CrossRef]
- Brown, S.C.; Perrino, T.; Lombard, J.; Wang, K.; Toro, M.; Rundek, T.; Gutierrez, C.M.; Dong, C.; Plater-Zyberk, E.; Nardi, M.I.; et al. Health Disparities in the Relationship of Neighborhood Greenness to Mental Health Outcomes in 249,405 US Medicare Beneficiaries. Int. J. Environ. Res. Public Health 2018, 15, 430. [Google Scholar] [CrossRef]
- Danielewicz, A.L.; Wagner, K.J.; d’Orsi, E.; Boing, A.F. Is cognitive decline in the elderly associated with contextual income? Results of a population-based study in southern Brazil. Cad. Saude Publica 2016, 32, e00112715. [Google Scholar] [CrossRef]
- Wörn, J.; Ellwardt, L.; Aartsen, M.; Huisman, M. Cognitive functioning among Dutch older adults: Do neighborhood socioeconomic status and urbanity matter? Soc. Sci. Med. 2017, 187, 29–38. [Google Scholar] [CrossRef]
- Vogt, S.; Mielck, A.; Berger, U.; Grill, E.; Peters, A.; Döring, A.; Holle, R.; Strobl, R.; Zimmermann, A.K.; Linkohr, B.; et al. Neighborhood and healthy aging in a German city: Distances to green space and senior service centers and their associations with physical constitution, disability, and health-related quality of life. Eur. J. Ageing 2015, 12, 273–283. [Google Scholar] [CrossRef]
- Wagner, K.J.; Boing, A.F.; Subramanian, S.V.; Höfelmann, D.A.; D’Orsi, E. Effects of neighborhood socioeconomic status on blood pressure in older adults. Rev. Saude Publica 2016, 50, 78. [Google Scholar] [CrossRef]
- Wight, R.G.; Aneshensel, C.S.; Miller-Martinez, D.; Botticello, A.L.; Cummings, J.R.; Karlamangla, A.S.; Seeman, T.E. Urban neighborhood context, educational attainment, and cognitive function among older adults. Am. J. Epidemiol. 2006, 163, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Cagney, K.A.; Browning, C.R.; Iveniuk, J.; English, N. The onset of depression during the great recession: Foreclosure and older adult mental health. Am. J. Public Health 2014, 104, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Chan, C.H.; Chang, Q.; Liu, T.; Yip, P.S.F. Neighborhood environment and cognitive function in older adults: A multilevel analysis in Hong Kong. Health Place 2019, 58, 102146. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Mooney, S.J.; Rundle, A.G.; Quinn, J.W.; Beard, J.R.; Cerdá, M. Pathways from neighborhood poverty to depression among older adults. Health Place 2017, 43, 138–143. [Google Scholar] [CrossRef]
- Yao, L.; Robert, S.A. Examining the Racial Crossover in Mortality between African American and White Older Adults: A Multilevel Survival Analysis of Race, Individual Socioeconomic Status, and Neighborhood Socioeconomic Context. J. Aging Res. 2011, 2011, 132073. [Google Scholar] [CrossRef]
- Huang, Y.; Meyer, P.; Jin, L. Neighborhood socioeconomic characteristics, healthcare spatial access, and emergency department visits for ambulatory care sensitive conditions for elderly. Prev. Med. Rep. 2018, 12, 101–105. [Google Scholar] [CrossRef]
- Auchincloss, A.H.; Van Nostrand, J.F.; Ronsaville, D. Access to health care for older persons in the United States: Personal, structural, and neighborhood characteristics. J. Aging Health 2001, 13, 329–354. [Google Scholar] [CrossRef]
- Buys, D.R.; Howard, V.J.; McClure, L.A.; Buys, K.C.; Sawyer, P.; Allman, R.M.; Levitan, E.B. Association between neighborhood disadvantage and hypertension prevalence, awareness, treatment, and control in older adults: Results from the University of Alabama at Birmingham Study of Aging. Am. J. Public Health 2015, 105, 1181–1188. [Google Scholar] [CrossRef]
- Nguyen, H.V. Keeping Up with the Joneses: Neighbourhood Wealth and Hypertension. J. Happiness Stud. 2016, 17, 1255–1271. [Google Scholar] [CrossRef]
- Brown, A.F.; Liang, L.J.; Vassar, S.D.; Stein-Merkin, S.; Longstreth, W.T., Jr.; Ovbiagele, B.; Yan, T.; Escarce, J.J. Neighborhood disadvantage and ischemic stroke: The Cardiovascular Health Study (CHS). Stroke 2011, 42, 3363–3368. [Google Scholar] [CrossRef]
- Nordstrom, C.K.; Diez Roux, A.V.; Jackson, S.A.; Gardin, J.M. The association of personal and neighborhood socioeconomic indicators with subclinical cardiovascular disease in an elderly cohort. The cardiovascular health study. Soc. Sci. Med. 2004, 59, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Wight, R.G.; Cummings, J.R.; Miller-Martinez, D.; Karlamangla, A.S.; Seeman, T.E.; Aneshensel, C.S. A multilevel analysis of urban neighborhood socioeconomic disadvantage and health in late life. Soc. Sci. Med. 2008, 66, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Lönn, S.L.; Melander, O.; Crump, C.; Sundquist, K. Accumulated neighbourhood deprivation and coronary heart disease: A nationwide cohort study from Sweden. BMJ Open 2019, 9, e029248. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Davey Smith, G.; Patel, R.; Ebrahim, S. Life-course socioeconomic position, area deprivation, and coronary heart disease: Findings from the British Women’s Heart and Health Study. Am. J. Public Health 2005, 95, 91–97. [Google Scholar] [CrossRef]
- Yan, T.; Escarce, J.J.; Liang, L.J.; Longstreth, W.T., Jr.; Merkin, S.S.; Ovbiagele, B.; Vassar, S.D.; Seeman, T.; Sarkisian, C.; Brown, A.F. Exploring psychosocial pathways between neighbourhood characteristics and stroke in older adults: The cardiovascular health study. Age Ageing 2013, 42, 391–397. [Google Scholar] [CrossRef][Green Version]
- Purser, J.L.; Kuchibhatla, M.N.; Miranda, M.L.; Blazer, D.G.; Cohen, H.J.; Fillenbaum, G.G. Geographical segregation and IL-6: A marker of chronic inflammation in older adults. Biomark. Med. 2008, 2, 335–348. [Google Scholar] [CrossRef]
- Corriere, M.D.; Yao, W.; Xue, Q.L.; Cappola, A.R.; Fried, L.P.; Thorpe, R.J., Jr.; Szanton, S.L.; Kalyani, R.R. The association of neighborhood characteristics with obesity and metabolic conditions in older women. J. Nutr. Health Aging 2014, 18, 792–798. [Google Scholar] [CrossRef]
- Araújo, C.A.H.; Giehl, M.W.C.; Danielewicz, A.L.; Araujo, P.G.; d’Orsi, E.; Boing, A.F. Built environment, contextual income, and obesity in older adults: Evidence from a population-based study. Cad. Saude Publica 2018, 34, e00060217. [Google Scholar] [CrossRef]
- Merkin, S.S.; Diez Roux, A.V.; Coresh, J.; Fried, L.F.; Jackson, S.A.; Powe, N.R. Individual and neighborhood socioeconomic status and progressive chronic kidney disease in an elderly population: The Cardiovascular Health Study. Soc. Sci. Med. 2007, 65, 809–821. [Google Scholar] [CrossRef]
- Garcia, L.; Lee, A.; Zeki Al Hazzouri, A.; Neuhaus, J.; Epstein, M.; Haan, M. The Impact of Neighborhood Socioeconomic Position on Prevalence of Diabetes and Prediabetes in Older Latinos: The Sacramento Area Latino Study on Aging. Hisp. Health Care Int. Off. J. Natl. Assoc. Hisp. Nurses 2015, 13, 77–85. [Google Scholar] [CrossRef][Green Version]
- Garcia, L.; Lee, A.; Zeki Al Hazzouri, A.; Neuhaus, J.M.; Moyce, S.; Aiello, A.; Elfassy, T.; Haan, M.N. Influence of neighbourhood socioeconomic position on the transition to type II diabetes in older Mexican Americans: The Sacramento Area Longitudinal Study on Aging. BMJ Open 2016, 6, e010905. [Google Scholar] [CrossRef] [PubMed]
- Michael, Y.L.; Nagel, C.L.; Gold, R.; Hillier, T.A. Does change in the neighborhood environment prevent obesity in older women? Soc. Sci. Med. 2014, 102, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Nicklett, E.J.; Szanton, S.; Sun, K.; Ferrucci, L.; Fried, L.P.; Guralnik, J.M.; Semba, R.D. Neighborhood socioeconomic status is associated with serum carotenoid concentrations in older, community-dwelling women. J. Nutr. 2011, 141, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Amuzu, A.; Carson, C.; Watt, H.C.; Lawlor, D.A.; Ebrahim, S. Influence of area and individual lifecourse deprivation on health behaviours: Findings from the British Women’s Heart and Health Study. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 169–173. [Google Scholar] [CrossRef]
- Stroope, S.; Martinez, B.C.; Eschbach, K.; Peek, M.K.; Markides, K.S. Neighborhood Ethnic Composition and Problem Drinking Among Older Mexican American Men: Results from the Hispanic Established Populations for the Epidemiologic Study of the Elderly. J. Immigr. Minority Health 2015, 17, 1055–1060. [Google Scholar] [CrossRef]
- Cerin, E.; Mellecker, R.; Macfarlane, D.J.; Barnett, A.; Cheung, M.C.; Sit, C.H.; Chan, W.M. Socioeconomic status, neighborhood characteristics, and walking within the neighborhood among older Hong Kong Chinese. J. Aging Health 2013, 25, 1425–1444. [Google Scholar] [CrossRef]
- Hawkesworth, S.; Silverwood, R.J.; Armstrong, B.; Pliakas, T.; Nanchalal, K.; Jefferis, B.J.; Sartini, C.; Amuzu, A.A.; Wannamethee, S.G.; Ramsay, S.E.; et al. Investigating associations between the built environment and physical activity among older people in 20 UK towns. J. Epidemiol. Community Health 2018, 72, 121–131. [Google Scholar] [CrossRef]
- Mooney, S.J.; Joshi, S.; Cerdá, M.; Kennedy, G.J.; Beard, J.R.; Rundle, A.G. Contextual Correlates of Physical Activity among Older Adults: A Neighborhood Environment-Wide Association Study (NE-WAS). Cancer Epidemiol. Biomark. Prev. 2017, 26, 495–504. [Google Scholar] [CrossRef]
- Annear, M.J.; Cushman, G.; Gidlow, B. Leisure time physical activity differences among older adults from diverse socioeconomic neighborhoods. Health Place 2009, 15, 482–490. [Google Scholar] [CrossRef]
- Annear, M.J.; Gidlow, B.; Cushman, G. Neighbourhood deprivation and older adults’ preferences for and perceptions of active leisure participation. Ann. Leis. Res. 2009, 12, 96–128. [Google Scholar] [CrossRef]
- Giehl, M.C.G.; Hallal, P.C.; Weber Corseuil, C.; Schneider, I.J.; d’Orsi, E. Built Environment and Walking Behavior Among Brazilian Older Adults: A Population-Based Study. J. Phys. Act. Health 2016, 13, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Hannon, L., 3rd; Sawyer, P.; Allman, R.M. Housing, the Neighborhood Environment, and Physical Activity among Older African Americans. J. Health Disparities Res. Pract. 2012, 5, 27–41. [Google Scholar]
- Fox, K.R.; Hillsdon, M.; Sharp, D.; Cooper, A.R.; Coulson, J.C.; Davis, M.; Harris, R.; McKenna, J.; Narici, M.; Stathi, A.; et al. Neighbourhood deprivation and physical activity in UK older adults. Health Place 2011, 17, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.I.; Pires, A.; Carvalho, M.S.; Pina, M.F. Distance to parks and non-residential destinations influences physical activity of older people, but crime doesn’t: A cross-sectional study in a southern European city. BMC Public Health 2015, 15, 593. [Google Scholar] [CrossRef] [PubMed]
- Moser, A.; Panczak, R.; Zwahlen, M.; Clough-Gorr, K.M.; Spoerri, A.; Stuck, A.E.; Egger, M. What does your neighbourhood say about you? A study of life expectancy in 1.3 million Swiss neighbourhoods. J. Epidemiol. Community Health 2014, 68, 1125–1132. [Google Scholar] [CrossRef]
- Bhardwaj, R.; Amiri, S.; Buchwald, D.; Amram, O. Environmental Correlates of Reaching a Centenarian Age: Analysis of 144,665 Deaths in Washington State for 2011–2015. Int. J. Environ. Res. Public Health 2020, 17, 2828. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; Finney Rutten, L.J.; Wilson, P.M.; Fan, C.; Boyd, C.M.; Jacobson, D.J.; Rocca, W.A.; St Sauver, J.L. Neighborhood socioeconomic disadvantage is associated with multimorbidity in a geographically-defined community. BMC Public Health 2020, 20, 13. [Google Scholar] [CrossRef]
- Wight, R.G.; Cummings, J.R.; Karlamangla, A.S.; Aneshensel, C.S. Urban neighborhood context and mortality in late life. J. Aging Health 2010, 22, 197–218. [Google Scholar] [CrossRef]
- Balamurugan, A.; Delongchamp, R.; Bates, J.H.; Mehta, J.L. The neighborhood where you live is a risk factor for stroke. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 668–673. [Google Scholar] [CrossRef]
- Diez Roux, A.V.; Borrell, L.N.; Haan, M.; Jackson, S.A.; Schultz, R. Neighbourhood environments and mortality in an elderly cohort: Results from the cardiovascular health study. J. Epidemiol. Community Health 2004, 58, 917–923. [Google Scholar] [CrossRef]
- Ramsay, S.E.; Morris, R.W.; Whincup, P.H.; Subramanian, S.V.; Papacosta, A.O.; Lennon, L.T.; Wannamethee, S.G. The influence of neighbourhood-level socioeconomic deprivation on cardiovascular disease mortality in older age: Longitudinal multilevel analyses from a cohort of older British men. J. Epidemiol. Community Health 2015, 69, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Chaix, B.; Rosvall, M.; Merlo, J. Assessment of the magnitude of geographical variations and socioeconomic contextual effects on ischaemic heart disease mortality: A multilevel survival analysis of a large Swedish cohort. J. Epidemiol. Community Health 2007, 61, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Meijer, M.; Kejs, A.M.; Stock, C.; Bloomfield, K.; Ejstrud, B.; Schlattmann, P. Population density, socioeconomic environment and all-cause mortality: A multilevel survival analysis of 2.7 million individuals in Denmark. Health Place 2012, 18, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Reimers, A.; Laflamme, L. Hip fractures among the elderly: Personal and contextual social factors that matter. J. Trauma 2007, 62, 365–369. [Google Scholar] [CrossRef]
- Powell, W.R.; Buckingham, W.R.; Larson, J.L.; Vilen, L.; Yu, M.; Salamat, M.S.; Bendlin, B.B.; Rissman, R.A.; Kind, A.J.H. Association of Neighborhood-Level Disadvantage with Alzheimer Disease Neuropathology. JAMA Netw. Open 2020, 3, e207559. [Google Scholar] [CrossRef]
- Walters, K.; Breeze, E.; Wilkinson, P.; Price, G.M.; Bulpitt, C.J.; Fletcher, A. Local area deprivation and urban-rural differences in anxiety and depression among people older than 75 years in Britain. Am. J. Public Health 2004, 94, 1768–1774. [Google Scholar] [CrossRef]
- Everson-Rose, S.A.; Skarupski, K.A.; Barnes, L.L.; Beck, T.; Evans, D.A.; Mendes de Leon, C.F. Neighborhood socioeconomic conditions are associated with psychosocial functioning in older black and white adults. Health Place 2011, 17, 793–800. [Google Scholar] [CrossRef]
- Guo, Y.; Chang, S.S.; Chan, C.H.; Chang, Q.; Hsu, C.Y.; Yip, P.S.F. Association of neighbourhood social and physical attributes with depression in older adults in Hong Kong: A multilevel analysis. J. Epidemiol. Community Health 2019, 74, 120–129. [Google Scholar] [CrossRef]
- Lang, I.A.; Llewellyn, D.J.; Langa, K.M.; Wallace, R.B.; Huppert, F.A.; Melzer, D. Neighborhood deprivation, individual socioeconomic status, and cognitive function in older people: Analyses from the English Longitudinal Study of Ageing. J. Am. Geriatr. Soc. 2008, 56, 191–198. [Google Scholar] [CrossRef]
- Rosso, A.L.; Flatt, J.D.; Carlson, M.C.; Lovasi, G.S.; Rosano, C.; Brown, A.F.; Matthews, K.A.; Gianaros, P.J. Neighborhood Socioeconomic Status and Cognitive Function in Late Life. Am. J. Epidemiol. 2016, 183, 1088–1097. [Google Scholar] [CrossRef]
- Sheffield, K.M.; Peek, M.K. Neighborhood context and cognitive decline in older Mexican Americans: Results from the Hispanic Established Populations for Epidemiologic Studies of the Elderly. Am. J. Epidemiol. 2009, 169, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.T.; Prina, A.M.; Jones, A.P.; Barnes, L.E.; Matthews, F.E.; Brayne, C. Community environment, cognitive impairment and dementia in later life: Results from the Cognitive Function and Ageing Study. Age Ageing 2015, 44, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Sisco, S.M.; Marsiske, M. Neighborhood Influences on Late Life Cognition in the ACTIVE Study. J. Aging Res. 2012, 2012, 435826. [Google Scholar] [CrossRef]
- Wee, L.E.; Yeo, W.X.; Yang, G.R.; Hannan, N.; Lim, K.; Chua, C.; Tan, M.Y.; Fong, N.; Yeap, A.; Chen, L.; et al. Individual and Area Level Socioeconomic Status and Its Association with Cognitive Function and Cognitive Impairment (Low MMSE) among Community-Dwelling Elderly in Singapore. Dement. Geriatr. Cogn. Disord. Extra 2012, 2, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Espino, D.V.; Lichtenstein, M.J.; Palmer, R.F.; Hazuda, H.P. Ethnic differences in Mini-Mental State Examination (MMSE) scores: Where you live makes a difference. J. Am. Geriatr. Soc. 2001, 49, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Blázquez, M.A.; Noriega-Ruiz, B.; Ávila-Villanueva, M.; Valentí-Soler, M.; Frades-Payo, B.; Del Ser, T.; Gómez-Ramírez, J. Impact of individual and neighborhood dimensions of socioeconomic status on the prevalence of mild cognitive impairment over seven-year follow-up. Aging Ment. Health 2020, 25, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Basta, N.E.; Matthews, F.E.; Chatfield, M.D.; Brayne, C.; MRC-CFAS. Community-level socio-economic status and cognitive and functional impairment in the older population. Eur. J. Public Health 2007, 18, 48–54. [Google Scholar] [CrossRef]
- Casanova, R.; Saldana, S.; Lutz, M.W.; Plassman, B.L.; Kuchibhatla, M.; Hayden, K.M. Investigating predictors of cognitive decline using machine learning. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, 733–742. [Google Scholar] [CrossRef]
- Hazzouri, A.Z.A.; Haan, M.N.; Osypuk, T.; Abdou, C.; Hinton, L.; Aiello, A.E. Neighborhood socioeconomic context and cognitive decline among older Mexican Americans: Results from the Sacramento Area Latino Study on Aging. Am. J. Epidemiol. 2011, 174, 423–431. [Google Scholar] [CrossRef]
- Kim, G.H.; Lee, H.A.; Park, H.; Lee, D.Y.; Jo, I.; Choi, S.H.; Choi, K.G.; Jeong, J.H. Effect of Individual and District-level Socioeconomic Disparities on Cognitive Decline in Community-dwelling Elderly in Seoul. J. Korean Med. Sci. 2017, 32, 1508–1515. [Google Scholar] [CrossRef]
- Shih, R.A.; Ghosh-Dastidar, B.; Margolis, K.L.; Slaughter, M.E.; Jewell, A.; Bird, C.E.; Eibner, C.; Denburg, N.L.; Ockene, J.; Messina, C.R.; et al. Neighborhood socioeconomic status and cognitive function in women. Am. J. Public Health 2011, 101, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Letellier, N.; Gutierrez, L.A.; Carrière, I.; Gabelle, A.; Dartigues, J.F.; Dufouil, C.; Helmer, C.; Cadot, E.; Berr, C. Sex-specific association between neighborhood characteristics and dementia: The Three-City cohort. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2017, 14, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Letellier, N.; Carrière, I.; Gutierrez, L.A.; Gabelle, A.; Dartigues, J.F.; Dufouil, C.; Helmer, C.; Cadot, E.; Berr, C. Influence of activity space on the association between neighborhood characteristics and dementia risk: Results from the 3-City study cohort. BMC Geriatr. 2019, 19, 4. [Google Scholar] [CrossRef] [PubMed]
- Cadar, D.; Lassale, C.; Davies, H.; Llewellyn, D.J.; Batty, G.D.; Steptoe, A. Individual and Area-Based Socioeconomic Factors Associated with Dementia Incidence in England: Evidence From a 12-Year Follow-up in the English Longitudinal Study of Ageing. JAMA Psychiatry 2018, 75, 723–732. [Google Scholar] [CrossRef]
- Miao, J.; Wu, X.; Sun, X. Neighborhood, social cohesion, and the Elderly’s depression in Shanghai. Soc. Sci. Med. 2019, 229, 134–143. [Google Scholar] [CrossRef]
- Bolstad, C.J.; Moak, R.; Brown, C.J.; Kennedy, R.E.; Buys, D.R. Neighborhood Disadvantage Is Associated with Depressive Symptoms but Not Depression Diagnosis in Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 5745. [Google Scholar] [CrossRef]
- Almeida, O.P.; Pirkis, J.; Kerse, N.; Sim, M.; Flicker, L.; Snowdon, J.; Draper, B.; Byrne, G.; Lautenschlager, N.T.; Stocks, N.; et al. Socioeconomic disadvantage increases risk of prevalent and persistent depression in later life. J. Affect. Disord. 2012, 138, 322–331. [Google Scholar] [CrossRef]
- Wee, L.E.; Yong, Y.Z.; Chng, M.W.; Chew, S.H.; Cheng, L.; Chua, Q.H.; Yek, J.J.; Lau, L.J.; Anand, P.; Hoe, J.T.; et al. Individual and area-level socioeconomic status and their association with depression amongst community-dwelling elderly in Singapore. Aging Ment. Health 2014, 18, 628–641. [Google Scholar] [CrossRef]
- Meyer, O.L.; Sisco, S.M.; Harvey, D.; Zahodne, L.B.; Glymour, M.M.; Manly, J.J.; Marsiske, M. Neighborhood Predictors of Cognitive Training Outcomes and Trajectories in ACTIVE. Res. Aging 2017, 39, 443–467. [Google Scholar] [CrossRef]
- Gale, C.R.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Neighbourhood environment and positive mental health in older people: The Hertfordshire Cohort Study. Health Place 2011, 17, 867–874. [Google Scholar] [CrossRef]
- Aneshensel, C.S.; Wight, R.G.; Miller-Martinez, D.; Botticello, A.L.; Karlamangla, A.S.; Seeman, T.E. Urban neighborhoods and depressive symptoms among older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, S52–S59. [Google Scholar] [CrossRef] [PubMed]
- Kubzansky, L.D.; Subramanian, S.V.; Kawachi, I.; Fay, M.E.; Soobader, M.J.; Berkman, L.F. Neighborhood contextual influences on depressive symptoms in the elderly. Am. J. Epidemiol. 2005, 162, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Ostir, G.V.; Eschbach, K.; Markides, K.S.; Goodwin, J.S. Neighbourhood composition and depressive symptoms among older Mexican Americans. J. Epidemiol. Community Health 2003, 57, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Hybels, C.F.; Blazer, D.G.; Pieper, C.F.; Burchett, B.M.; Hays, J.C.; Fillenbaum, G.G.; Kubzansky, L.D.; Berkman, L.F. Sociodemographic characteristics of the neighborhood and depressive symptoms in older adults: Using multilevel modeling in geriatric psychiatry. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2006, 14, 498–506. [Google Scholar] [CrossRef]
- Wight, R.G.; Cummings, J.R.; Karlamangla, A.S.; Aneshensel, C.S. Urban neighborhood context and change in depressive symptoms in late life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, 247–251. [Google Scholar] [CrossRef]
- Salvatore, M.A.; Grundy, E. Area deprivation, perceived neighbourhood cohesion and mental health at older ages: A cross lagged analysis of UK longitudinal data. Health Place 2021, 67, 102470. [Google Scholar] [CrossRef]
- Kelley-Moore, J.A.; Cagney, K.A.; Skarupski, K.A.; Everson-Rose, S.A.; Mendes de Leon, C.F. Do Local Social Hierarchies Matter for Mental Health? A Study of Neighborhood Social Status and Depressive Symptoms in Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 369–377. [Google Scholar] [CrossRef]
- Kwag, K.H.; Jang, Y.; Rhew, S.H.; Chiriboga, D.A. Neighborhood Effects on Physical and Mental Health: A Study of Korean American Older Adults. Asian Am. J. Psychol. 2011, 2, 91–100. [Google Scholar] [CrossRef]
- Pearce, J.; Cherrie, M.; Shortt, N.; Deary, I.; Thompson, C.W. Life course of place: A longitudinal study of mental health and place. Trans. Inst. Br. Geogr. 2018, 43, 555–572. [Google Scholar] [CrossRef]
- Lang, I.A.; Gibbs, S.J.; Steel, N.; Melzer, D. Neighbourhood deprivation and dental service use: A cross-sectional analysis of older people in England. J. Public Health 2008, 30, 472–478. [Google Scholar] [CrossRef][Green Version]
- Omariba, W.R. Neighbourhood characteristics, individual attributes and self-rated health among older Canadians. Health Place 2010, 16, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.E.; Jang, Y.; Park, N.S.; Rhew, S.H.; Chiriboga, D.A. Neighborhood effects on the self-rated health of older adults from four racial/ethnic groups. Soc. Work Public Health 2014, 29, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Stroope, S.; Cohen, I.F.A.; Tom, J.C.; Franzen, A.B.; Valasik, M.A.; Markides, K.S. Neighborhood perception and self-rated health among Mexican American older adults. Geriatr. Gerontol. Int. 2017, 17, 2559–2564. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Eschbach, K.; Rudkin, L.L.; Peek, M.K.; Markides, K.S. Neighborhood context and self-rated health in older Mexican Americans. Ann. Epidemiol. 2003, 13, 620–628. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Kubzansky, L.; Berkman, L.; Fay, M.; Kawachi, I. Neighborhood effects on the self-rated health of elders: Uncovering the relative importance of structural and service-related neighborhood environments. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2006, 61, S153–S160. [Google Scholar] [CrossRef]
- Yao, L.; Robert, S.A. The contributions of race, individual socioeconomic status, and Neighborhood socioeconomic context on the self-rated health trajectories and mortality of older adults. Res. Aging 2008, 30, 251–273. [Google Scholar] [CrossRef]
- Jung, D.; Kind, A.; Robert, S.; Buckingham, W.; DuGoff, E. Linking Neighborhood Context and Health in Community-Dwelling Older Adults in the Medicare Advantage Program. J. Am. Geriatr. Soc. 2018, 66, 1158–1164. [Google Scholar] [CrossRef]
- Lang, I.A.; Llewellyn, D.J.; Langa, K.M.; Wallace, R.B.; Melzer, D. Neighbourhood deprivation and incident mobility disability in older adults. Age Ageing 2008, 37, 403–410. [Google Scholar] [CrossRef]
- Nordstrom, C.K.; Diez Roux, A.V.; Schulz, R.; Haan, M.N.; Jackson, S.A.; Balfour, J.L. Socioeconomic position and incident mobility impairment in the Cardiovascular Health Study. BMC Geriatr. 2007, 7, 11. [Google Scholar] [CrossRef]
- Beard, J.R.; Blaney, S.; Cerda, M.; Frye, V.; Lovasi, G.S.; Ompad, D.; Rundle, A.; Vlahov, D. Neighborhood characteristics and disability in older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, 252–257. [Google Scholar] [CrossRef]
- Bowling, A.; Stafford, M. How do objective and subjective assessments of neighbourhood influence social and physical functioning in older age? Findings from a British survey of ageing. Soc. Sci. Med. 2007, 64, 2533–2549. [Google Scholar] [CrossRef] [PubMed]
- Franse, C.B.; van Grieken, A.; Qin, L.; Melis, R.J.F.; Rietjens, J.A.C.; Raat, H. Socioeconomic inequalities in frailty and frailty components among community-dwelling older citizens. PLoS ONE 2017, 12, e0187946. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.A.; Hubbard, R.E.; Andrew, M.K.; Llewellyn, D.J.; Melzer, D.; Rockwood, K. Neighborhood deprivation, individual socioeconomic status, and frailty in older adults. J. Am. Geriatr. Soc. 2009, 57, 1776–1780. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, S.E.; Hazuda, H.P. Frailty prevalence and neighborhood residence in older Mexican Americans: The San Antonio longitudinal study of aging. J. Am. Geriatr. Soc. 2015, 63, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Procter-Gray, E.; Lipsitz, L.A.; Leveille, S.G.; Hackman, H.; Biondolillo, M.; Hannan, M.T. Utilitarian walking, neighborhood environment, and risk of outdoor falls among older adults. Am. J. Public Health 2014, 104, e30–e37. [Google Scholar] [CrossRef]
- Lo, A.X.; Rundle, A.G.; Buys, D.; Kennedy, R.E.; Sawyer, P.; Allman, R.M.; Brown, C.J. Neighborhood Disadvantage and Life-Space Mobility Are Associated with Incident Falls in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2016, 64, 2218–2225. [Google Scholar] [CrossRef]
- Schieman, S.; Pearlin, L.I.; Meersman, S.C. Neighborhood disadvantage and anger among older adults: Social comparisons as effect modifiers. J. Health Soc. Behav. 2006, 47, 156–172. [Google Scholar] [CrossRef]
- Brenner, A.B.; Clarke, P.J. Difficulty and independence in shopping among older Americans: More than just leaving the house. Disabil. Rehabil. 2019, 41, 191–200. [Google Scholar] [CrossRef]
- Menec, V.H.; Shooshtari, S.; Nowicki, S.; Fournier, S. Does the relationship between neighborhood socioeconomic status and health outcomes persist into very old age? A population-based study. J. Aging Health 2010, 22, 27–47. [Google Scholar] [CrossRef]
- Beere, P.; Keeling, S.; Jamieson, H. Ageing, loneliness, and the geographic distribution of New Zealand’s interRAI-HC cohort. Soc. Sci. Med. 2019, 227, 84–92. [Google Scholar] [CrossRef]
- Timmermans, E.; Motoc, I.; Noordzij, J.M.; Beenackers, M.A.; Wissa, R.; Sarr, A.; Gurer, A.; Fabre, G.; Ruiz, M.; Doiron, D.; et al. Social and physical neighbourhood characteristics and loneliness among older adults: Results from the MINDMAP project. J. Epidemiol. Community Health 2020, 75, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, C.; Gallacher, J.; Webster, C. Urban built environment configuration and psychological distress in older men: Results from the Caerphilly study. BMC Public Health 2013, 13, 695. [Google Scholar] [CrossRef] [PubMed]
- Alaazi, D.A.; Menon, D.; Stafinski, T.; Hodgins, S.; Jhangri, G. Quality of life of older adults in two contrasting neighbourhoods in Accra, Ghana. Soc. Sci. Med. 2021, 270, 113659. [Google Scholar] [CrossRef] [PubMed]
- Mõttus, R.; Gale, C.R.; Starr, J.M.; Deary, I.J. ‘On the street where you live’: Neighbourhood deprivation and quality of life among community-dwelling older people in Edinburgh, Scotland. Soc. Sci. Med. 2012, 74, 1368–1374. [Google Scholar] [CrossRef] [PubMed]
- Breeze, E.; Jones, D.A.; Wilkinson, P.; Bulpitt, C.J.; Grundy, C.; Latif, A.M.; Fletcher, A.E. Area deprivation, social class, and quality of life among people aged 75 years and over in Britain. Int. J. Epidemiol. 2005, 34, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Buffel, T.; Phillipson, C.; Scharf, T. Experiences of neighbourhood exclusion and inclusion among older people living in deprived inner-city areas in Belgium and England. Ageing Soc. 2013, 33, 89–109. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Krainski, E.T.; Carvalho, M.S.; Launoy, G.; Pornet, C.; de Pina, M.F. Does community deprivation determine longevity after the age of 75? A cross-national analysis. Int. J. Public Health 2018, 63, 469–479. [Google Scholar] [CrossRef]
- Pickett, K.E.; Pearl, M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: A critical review. J. Epidemiol. Community Health 2001, 55, 111–122. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Moudon, A.V.; Smith, N.L.; Lumley, T.; Larson, E.B.; Sohn, D.W.; Siscovick, D.S.; Psaty, B.M. Evaluating options for measurement of neighborhood socioeconomic context: Evidence from a myocardial infarction case-control study. Health Place 2008, 14, 453–467. [Google Scholar] [CrossRef]
- Collyer, T.A.; Smith, K.E. An atlas of health inequalities and health disparities research: “How is this all getting done in silos, and why?”. Soc. Sci. Med. 2020, 264, 113330. [Google Scholar] [CrossRef]
- Ribeiro, A.I. Public health: Why study neighborhoods? Porto Biomed J. 2018, 3, e16. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, C.J.; Paciência, I.; Ribeiro, A.I. Neighbourhood Socioeconomic Processes and Dynamics and Healthy Ageing: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 6745. https://doi.org/10.3390/ijerph19116745
Santos CJ, Paciência I, Ribeiro AI. Neighbourhood Socioeconomic Processes and Dynamics and Healthy Ageing: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(11):6745. https://doi.org/10.3390/ijerph19116745
Chicago/Turabian StyleSantos, Cláudia Jardim, Inês Paciência, and Ana Isabel Ribeiro. 2022. "Neighbourhood Socioeconomic Processes and Dynamics and Healthy Ageing: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 11: 6745. https://doi.org/10.3390/ijerph19116745
APA StyleSantos, C. J., Paciência, I., & Ribeiro, A. I. (2022). Neighbourhood Socioeconomic Processes and Dynamics and Healthy Ageing: A Scoping Review. International Journal of Environmental Research and Public Health, 19(11), 6745. https://doi.org/10.3390/ijerph19116745