
Tooth Loss Related with Prevalence of Metabolic Syndrome in a General Urban Japanese Population: The Suita Study

 ,
,  ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Research Subjects
2.2. Questionnaire Survey
2.3. Survey on the Components of Metabolic Syndrome
2.4. Definition of Metabolic Syndrome
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ritchie, C.S.; Joshipura, K.; Hung, H.-C.; Douglass, C.W. Nutrition as a mediator in the relation between oral and systemic disease: Associations between specific measures of adult oral health and nutrition outcomes. Crit. Rev. Oral Biol. Med. 2002, 13, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.; Hankey, C. Aging, nutritional status and health. Healthcare 2015, 3, 648–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zupo, R.; Castellana, F.; Bortone, I.; Griseta, C.; Sardone, R.; Lampignano, L.; Lozupone, M.; Solfrizzi, V.; Castellana, M.; Giannelli, G. Nutritional domains in frailty tools: Working towards an operational definition of nutritional frailty. Ageing Res. Rev. 2020, 64, 101148. [Google Scholar] [CrossRef] [PubMed]
- Fushida, S.; Kosaka, T.; Nakai, M.; Kida, M.; Nokubi, T.; Kokubo, Y.; Watanabe, M.; Miyamoto, Y.; Ono, T.; Ikebe, K. Lower Masticatory Performance Is a Risk for the Development of the Metabolic Syndrome: The Suita Study. Front. Cardiovasc. Med. 2021, 8, 752667. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Tominaga, K.; Ando, Y.; Toyama, Y.; Takeda, M.; Yamasaki, M.; Okuyama, K.; Hamano, T.; Isomura, M.; Nabika, T.; et al. Number of teeth and masticatory function are associated with sarcopenia and diabetes mellitus status among community-dwelling older adults: A Shimane CoHRE study. PLoS ONE 2021, 16, e0252625. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef]
- Miyatake, K. Japanese oral health care in the future. Dent. Jpn. 1991, 28, 217–221. [Google Scholar]
- Yamanaka, K.; Nakagaki, H.; Morita, I.; Suzaki, H.; Hashimoto, M.; Sakai, T. Comparison of the health condition between the 8020 achievers and the 8020 non-achievers. Int. Dent. J. 2008, 58, 146–150. [Google Scholar] [CrossRef]
- Yuan, J.Q.; Lv, Y.B.; Kraus, V.B.; Gao, X.; Yin, Z.X.; Chen, H.S.; Luo, J.S.; Zeng, Y.; Mao, C.; Shi, X.M. Number of natural teeth, denture use and mortality in Chinese elderly: A population-based prospective cohort study. BMC Oral Health 2020, 20, 100. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, S.; Konta, T.; Susa, S.; Ishizawa, K.; Togashi, H.; Ueno, Y.; Yamashita, H.; Kayama, T.; Iino, M. Association between presence of 20 or more natural teeth and all-cause, cancer-related, and cardiovascular disease-related mortality: Yamagata (Takahata) prospective observational study. BMC Oral Health 2020, 20, 353. [Google Scholar] [CrossRef]
- Nowjack-Raymer, R.E.; Sheiham, A. Numbers of natural teeth, diet, and nutritional status in US adults. J. Dent. Res. 2007, 86, 1171–1175. [Google Scholar] [CrossRef] [PubMed]
- Aida, J.; Kondo, K.; Yamamoto, T.; Hirai, H.; Nakade, M.; Osaka, K.; Sheiham, A.; Tsakos, G.; Watt, R.G. Oral Health and Cancer, Cardiovascular, and Respiratory Mortality of Japanese. J. Dent. Res. 2011, 90, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Hung, H.C.; Rimm, E.B.; Willett, W.C.; Ascherio, A. Periodontal disease, tooth loss, and incidence of ischemic stroke. Stroke 2003, 34, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desvarieux, M.; Schwahn, C.; Volzke, H.; Demmer, R.T.; Ludemann, J.; Kessler, C.; Jacobs, D.R., Jr.; John, U.; Kocher, T. Gender differences in the relationship between periodontal disease, tooth loss, and atherosclerosis. Stroke 2004, 35, 2029–2035. [Google Scholar] [CrossRef] [Green Version]
- Taguchi, A.; Sanada, M.; Suei, Y.; Ohtsuka, M.; Lee, K.; Tanimoto, K.; Tsuda, M.; Ohama, K.; Yoshizumi, M.; Higashi, Y. Tooth loss is associated with an increased risk of hypertension in postmenopausal women. Hypertension 2004, 43, 1297–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, N.; Shimazaki, Y.; Shinagawa, T.; Yamashita, Y. Periodontal Status and Metabolic Syndrome in Middle-Aged Japanese. J. Periodontol. 2012, 83, 1363–1371. [Google Scholar] [CrossRef]
- Asai, K.; Yamori, M.; Yamazaki, T.; Yamaguchi, A.; Takahashi, K.; Sekine, A.; Kosugi, S.; Matsuda, F.; Nakayama, T.; Bessho, K. Tooth loss and atherosclerosis: The Nagahama Study. J. Dent. Res. 2015, 94, 52s–58s. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Hollis, J.H. Associations between the number of natural teeth and metabolic syndrome in adults. J. Clin. Periodontol. 2015, 42, 113–120. [Google Scholar] [CrossRef]
- Shin, H.S. The Number of Teeth Is Inversely Associated with Metabolic Syndrome: A Korean Nationwide Population-Based Study. J. Periodontol. 2017, 88, 830–838. [Google Scholar] [CrossRef]
- Lorenzo, C.; Williams, K.; Hunt, K.J.; Haffner, S.M. The National Cholesterol Education Program–Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care 2007, 30, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Okamura, T.; Kokubo, Y.; Watanabe, M.; Higashiyama, A.; Ono, Y.; Nishimura, K.; Okayama, A.; Miyamoto, Y. A revised definition of the metabolic syndrome predicts coronary artery disease and ischemic stroke after adjusting for low density lipoprotein cholesterol in a 13-year cohort study of Japanese: The Suita Study. Atherosclerosis 2011, 217, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Kosaka, T.; Ono, T.; Kida, M.; Kikui, M.; Yamamoto, M.; Yasui, S.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; et al. A multifactorial model of masticatory performance: The Suita study. J. Oral Rehabil. 2016, 43, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Niesten, D.; Bronkhorst, E.M.; Witter, D.J.; Creugers, N.H.J. Food avoidance is associated with reduced dentitions and edentulousness. Clin. Oral Investig. 2020, 24, 849–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakai, K.; Naito, M.; Naito, T.; Kojima, M.; Nakagaki, H.; Umemura, O.; Yokota, M.; Hanada, N.; Kawamura, T. Tooth loss and intakes of nutrients and foods: A nationwide survey of Japanese dentists. Community Dent. Oral Epidemiol. 2010, 38, 43–49. [Google Scholar] [CrossRef]
- Millen, B.E.; Pencina, M.J.; Kimokoti, R.W.; Zhu, L.; Meigs, J.B.; Ordovas, J.M.; D’Agostino, R.B. Nutritional risk and the metabolic syndrome in women: Opportunities for preventive intervention from the Framingham Nutrition Study. Am. J. Clin. Nutr. 2006, 84, 434–441. [Google Scholar] [CrossRef]
- Angeli, F.; Verdecchia, P.; Pellegrino, C.; Pellegrino, R.G.; Pellegrino, G.; Prosciutti, L.; Giannoni, C.; Cianetti, S.; Bentivoglio, M. Association between periodontal disease and left ventricle mass in essential hypertension. Hypertension 2003, 41, 488–492. [Google Scholar] [CrossRef] [Green Version]
- Beck, J.D.; Elter, J.R.; Heiss, G.; Couper, D.; Mauriello, S.M.; Offenbacher, S. Relationship of periodontal disease to carotid artery intima-media wall thickness: The atherosclerosis risk in communities (ARIC) study. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1816–1822. [Google Scholar] [CrossRef] [Green Version]
- Lalla, E.; Papapanou, P.N. Diabetes mellitus and periodontitis: A tale of two common interrelated diseases. Nat. Rev. Endocrinol. 2011, 7, 738–748. [Google Scholar] [CrossRef]
- Cutler, C.W.; Shinedling, E.A.; Nunn, M.; Jotwani, R.; Kim, B.O.; Nares, S.; Iacopino, A.M. Association between periodontitis and hyperlipidemia: Cause or effect? J. Periodontol. 1999, 70, 1429–1434. [Google Scholar] [CrossRef]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- D’Aiuto, F.; Sabbah, W.; Netuveli, G.; Donos, N.; Hingorani, A.D.; Deanfield, J.; Tsakos, G. Association of the metabolic syndrome with severe periodontitis in a large U.S. population-based survey. J. Clin. Endocrinol. Metab. 2008, 93, 3989–3994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, T.; Ogawa, Y.; Takada, K.; Nishinoue, N.; Sasaki, Y.; Motohashi, M.; Maeno, M. Association between periodontal disease and metabolic syndrome. J. Public Health Dent. 2009, 69, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Kushiyama, M.; Shimazaki, Y.; Yamashita, Y. Relationship between metabolic syndrome and periodontal disease in Japanese adults. J. Periodontol. 2009, 80, 1610–1615. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.E.; Ha, J.E.; Paik, D.I.; Jin, B.H.; Bae, K.H. The relationship between periodontitis and metabolic syndrome among a Korean nationally representative sample of adults. J. Clin. Periodontol. 2011, 38, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Takeuchi, K.; Furuta, M.; Takeshita, T.; Suma, S.; Shinagawa, T.; Shimazaki, Y.; Yamashita, Y. Relationship of toothbrushing to metabolic syndrome in middle-aged adults. J. Clin. Periodontol. 2018, 45, 538–547. [Google Scholar] [CrossRef]
- Andriankaja, O.M.; Sreenivasa, S.; Dunford, R.; DeNardin, E. Association between metabolic syndrome and periodontal disease. Aust. Dent. J. 2010, 55, 252–259. [Google Scholar] [CrossRef]
- Furuta, M.; Shimazaki, Y.; Takeshita, T.; Shibata, Y.; Akifusa, S.; Eshima, N.; Kiyohara, Y.; Ninomiya, T.; Hirakawa, Y.; Mukai, N.; et al. Gender differences in the association between metabolic syndrome and periodontal disease: The Hisayama Study. J. Clin. Periodontol. 2013, 40, 743–752. [Google Scholar] [CrossRef]
- Kawashita, Y.; Kitamura, M.; Ando, Y.; Saito, T. Relationship between Metabolic Syndrome and Number of Teeth in Japan. JDR Clin. Transl. Res. 2017, 2, 87–92. [Google Scholar] [CrossRef]
- Pradhan, A.D. Sex Differences in the Metabolic Syndrome: Implications for Cardiovascular Health in Women. Clin. Chem. 2014, 60, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Unwin, N.; Shaw, J.; Zimmet, P.; Alberti, K.G. Impaired glucose tolerance and impaired fasting glycaemia: The current status on definition and intervention. Diabet. Med. A J. Br. Diabet. Assoc. 2002, 19, 708–723. [Google Scholar]
- Crook, D.; Seed, M. Endocrine control of plasma lipoprotein metabolism: Effects of gonadal steroids. Bailliere’s Clin. Endocrinol. Metab. 1990, 4, 851–875. [Google Scholar] [CrossRef]
- Chang, S.H.; Chang, Y.Y.; Wu, L.Y. Gender differences in lifestyle and risk factors of metabolic syndrome: Do women have better health habits than men? J. Clin. Nurs. 2019, 28, 2225–2234. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuki, M.; Hirayama, K.; Sato, M.; Han, T. Denture Wearing and Malnutrition Risk Among Community-Dwelling Older Adults. Nutrients 2020, 12, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, S.; Kosaka, T.; Nakai, M.; Kida, M.; Fushida, S.; Kokubo, Y.; Watanabe, M.; Higashiyama, A.; Ikebe, K.; Ono, T.; et al. A lower maximum bite force is a risk factor for developing cardiovascular disease: The Suita study. Sci. Rep. 2021, 11, 7671. [Google Scholar] [CrossRef] [PubMed]
- Montero, J.; Dib, A.; Guadilla, Y.; Blanco, L.; Flores, J.; Gómez-Polo, C. Responsiveness of the different methods for assessing the short-term within-subject change in masticatory function after conventional prosthetic treatments. J. Prosthet. Dent. 2020, 123, 602–610. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Men | Women | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ≧20 Teeth | ≦19 Teeth | ≧20 Teeth | ≦19 Teeth | ≧20 Teeth | ≦19 Teeth | ||||
| Characteristics | (n = 946) | (n = 744) | (n = 1336) | (n = 745) | (n = 2282) | (n = 1489) | |||
| Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | |
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | ||||
| Age | 64.6 ± 10.3 | 72.9 ± 9.6 | <0.001 * | 62.5 ± 10.2 | 72.5 ± 9.1 | <0.001 * | 63.4 ± 10.3 | 72.7 ± 9.4 | <0.001 * |
| (yrs) | 65.0 (57.0–72.0) | 74.0 (67.0–80.0) | 63.0 (55.0–70.0) | 73.0 (67.0–79.0) | 64.0 (55.0–71.0) | 74.0 (67.0–79.0) | |||
| Waist | 85.9 ± 8.0 | 84.9 ± 8.6 | 0.042 * | 81.5 ± 9.1 | 83.3 ± 9.9 | <0.001 * | 83.3 ± 8.9 | 84.1 ± 9.3 | <0.001 * |
| (cm) | 86.0 (80.5–91.2) | 85.4 (79.5–90.5) | 80.8 (75.0–87.0) | 83.3 (76.5–89.6) | 83.1 (77.2–89.1) | 84.5 (78.0–90.0) | |||
| Diastolic blood pressure | 78.4 ± 10.7 | 77.1 ± 10.7 | 0.012 * | 72.5 ± 10.6 | 74.3 ± 10.8 | <0.001 * | 74.9 ± 11.0 | 75.7 ± 10.8 | <0.040 * |
| (mmHg) | 78.0 (71.0–85.6) | 76.6 (69.5–84.5) | 71.5 (64.5–79.5) | 73.5 (67.0–81.5) | 74.5 (67.0–82.5) | 75.0 (68.2–82.7) | |||
| Systolic blood pressure | 124.5 ± 17.7 | 127.0 ± 18.7 | 0.003 * | 118.2 ± 17.7 | 126.6 ± 19.9 | <0.001 * | 120.8 ± 17.9 | 126.8 ± 19.3 | <0.001 * |
| (mmHg) | 122.8 (112.0–135.1) | 125.0 (113.0–139.0) | 115.5 (105.0–129.5) | 124.5 (111.5–139.5) | 119.0 (107.5–132.5) | 124.5 (112.5–139.0) | |||
| HDL cholesterol | 55.0 ± 14.4 | 53.3 ± 14.5 | 0.008 * | 65.2 ± 14.7 | 61.5 ± 14.4 | <0.001 * | 61.0 ± 15.4 | 57.4 ± 15.0 | <0.001 * |
| (mg/dL) | 53.0 (46.0–62.0) | 51.0 (43.0–61.0) | 64.0 (55.0–74.0) | 60.0 (51.0–70.0) | 59.0 (50.0–70.0) | 55.0 (46.0–67.0) | |||
| LDL cholesterol | 118.6 ± 28.2 | 116.8 ± 27.7 | 0.190 | 131.7 ± 29.5 | 127.4 ± 28.1 | 0.001 * | 126.2 ± 29.7 | 122.1 ± 28.4 | <0.001 * |
| (mg/dL) | 119.4 (99.6–136.4) | 116.6 (97.4–135.0) | 131.8 (110.6–150.4) | 124.8 (108.4–144.1) | 125.4 (106.2–145.2) | 121.0 (103.4–140.1) | |||
| Fasting plasma glucose | 105.0 ± 24.4 | 106.5 ± 23.2 | 0.069 | 96.2 ± 15.1 | 100.3 ± 18.4 | <0.001 * | 99.8 ± 20.0 | 103.4 ± 21.2 | <0.001 * |
| (mg/dL) | 99.0 (93.0–108.0) | 100.0 (93.0–111.0) | 94.0 (89.0–99.0) | 96.0 (90.0–104.0) | 95.0 (90.0–103.0) | 98.0 (92.0–107.0) | |||
| Triglyceride | 116.0 ± 69.5 | 113.4 ± 67.9 | 0.595 | 92.8 ± 48.7 | 99.8 ± 47.9 | 0.002 * | 102.5 ± 59.3 | 106.6 ± 59.2 | 0.001 * |
| (mg/dL) | 97.0 (69.0–141.0) | 96.0 (68.3–137.0) | 82.0 (60.0–111.0) | 89.0 (68.0–119.0) | 87.5 (64.0–125.0) | 92.0 (68.0–129.0) | |||
| Components of Metabolic Syndrome (MetS) | Men | Women | Total | ||||
|---|---|---|---|---|---|---|---|
| ≧20 teeth | ≦19 Teeth | ≧20 Teeth | ≦19 Teeth | ≧20 Teeth | ≦19 Teeth | ||
| (n = 946) | (n = 744) | (n = 1336) | (n = 745) | (n = 2282) | (n = 1489) | ||
| No. of Participants (%) | No. of Participants (%) | No. of Participants (%) | |||||
| Metabolic Syndrome | Normal | 748 (79.1) | 587 (78.9) | 1135 (85.0) | 560 (75.2) | 1883 (82.5) | 1147 (77.0) |
| Abnormal | 198 (20.9) | 157 (21.1) | 201 (15.0) | 185 (24.8) | 399 (17.5) | 342 (23.0) | |
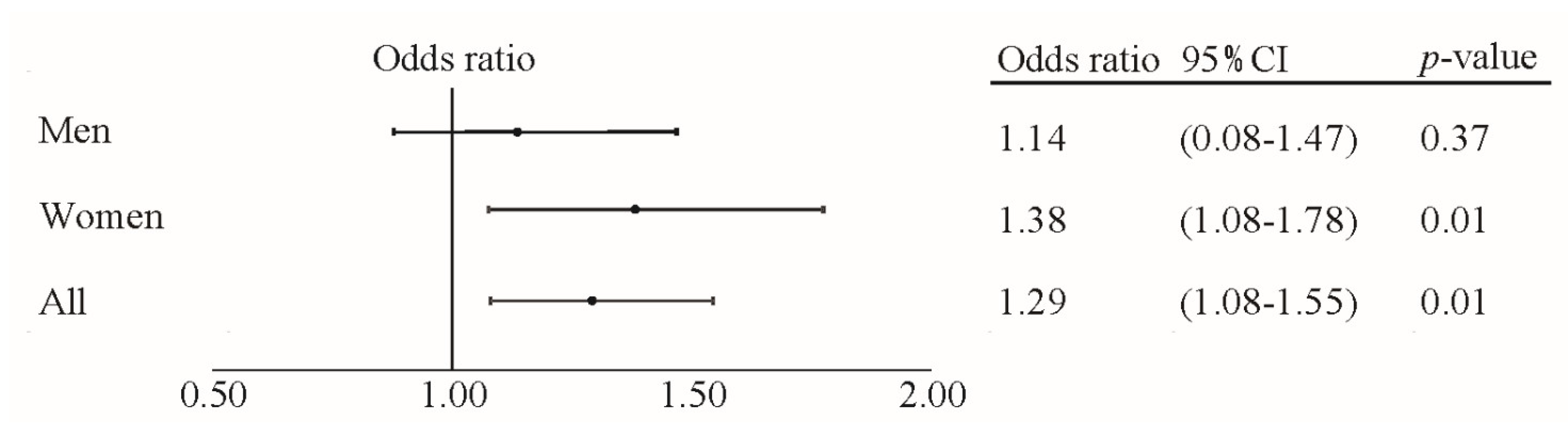
| Odds ratio (CI) | 1 | 1.14 (0.88–1.47) | 1 | 1.38 (1.08–1.78) | 1 | 1.29 (1.08–1.55) | |
| p value | - | 0.33 | - | 0.01 * | - | 0.01 * | |
| Blood pressure (mmHg) | Systolic < 130 and Diastolic < 85 | 560 (59.2) | 399 (53.6) | 970 (72.6) | 439 (58.9) | 1530 (67.0) | 838 (56.3) |
| Systolic ≧ 130 or Diastolic ≧ 85 | 386 (40.8) | 345 (46.4) | 366 (27.4) | 306 (41.1) | 752 (33.0) | 651 (43.7) | |
| Odds ratio (CI) | 1 | 1.04 (0.84–1.29) | 1 | 1.13 (0.92–1.40) | 1 | 1.12 (0.97–1.30) | |
| p value | - | 0.71 | - | 0.27 | - | 0.15 | |
| Fasting plasma glucose (mg/dL) | <100 | 502 (53.1) | 365 (49.1) | 1008 (75.4) | 472 (63.4) | 1510 (66.2) | 837 (56.2) |
| ≧100 | 444 (46.9) | 379 (50.9) | 328 (24.6) | 273 (36.6) | 772 (33.8) | 652 (43.8) | |
| Odds ratio (CI) | 1 | 1.21 (0.98–1.50) | 1 | 1.33 (1.07–1.65) | 1 | 1.32 (1.14–1.53) | |
| p value | - | 0.08 | - | 0.01 * | - | <0.01 * | |
| HDL cholesterol (mg/dL) | Men ≧ 40 Women ≧ 50 | 845 (89.3) | 637 (85.6) | 1161 (86.9) | 599 (80.4) | 2006 (87.9) | 1236 (83.0) |
| Men < 40 Women < 50 | 101 (10.7) | 107 (14.4) | 175 (13.1) | 146 (19.6) | 276 (12.1) | 253 (17.0) | |
| Odds ratio (CI) | 1 | 1.37 (1.00–0.64) | 1 | 1.41 (1.08–1.85) | 1 | 1.37 (1.12–1.69) | |
| p value | - | 0.05 * | - | 0.01 * | - | <0.01 * | |
| Triglyceride (mg/dL) | <150 | 742 (78.4) | 601 (80.8) | 1202 (90.0) | 645 (86.6) | 1944 (85.2) | 1246 (83.7) |
| ≧150 | 204 (21.6) | 143 (19.2) | 134 (10.0) | 100 (13.4) | 338 (14.8) | 243 (16.3) | |
| Odds ratio (CI) | 1 | 1.05 (0.81–1.36) | 1 | 1.48 (1.08–2.01) | 1 | 1.28 (1.05–1.56) | |
| p value | - | 0.72 | - | 0.02 * | - | 0.02 * | |
| Waist (cm) | Men < 90 Women < 80 | 654 (69.1) | 539 (72.4) | 613 (45.9) | 275 (36.9) | 1267 (55.5) | 814 (54.7) |
| Men ≧ 90 Women ≧ 80 | 292 (30.9) | 205 (27.6) | 723 (54.1) | 470 (63.1) | 1015 (44.5) | 675 (45.3) | |
| Odds ratio (CI) | 1 | 0.90 (0.72–1.13) | 1 | 1.12 (0.91–1.38) | 1 | 0.97 (0.84–1.12) | |
| p value | - | 0.4 | - | 0.31 | - | 0.68 | |
| Components of Metabolic Syndrome (MetS) | Men | Women | Total | ||||
|---|---|---|---|---|---|---|---|
| Adjusted Odds Ratio (95% CI) | p Value | Adjusted Odds Ratio (95% CI) | p Value | Adjusted Odds Ratio (95% CI) | p Value | ||
| Blood pressure (mmHg) | ≧20 teeth | 1 | 1 | 1 | |||
| ≦19 teeth | 1.11 (0.90–1.38) | 0.33 | 1.15 (0.92–1.43) | 0.23 | 1.15(0.98–1.34) | 0.08 | |
| Fasting plasma glucose (mg/dL) | ≧20 teeth | 1 | 1 | 1 | |||
| ≦19 teeth | 1.22 (0.98–1.51) | 0.08 | 1.37 (1.09–1.70) | 0.01 * | 1.32 (1.13–1.53) | <0.01 * | |
| HDL cholesterol (mg/dL) | ≧20 teeth | 1 | 1 | 1 | |||
| ≦19 teeth | 1.23 (0.89–1.70) | 0.21 | 1.40 (1.06–1.83) | 0.02 * | 1.32 (1.07–1.63) | 0.01 * | |
| Triglyceride (mg/dL) | ≧20 teeth | 1 | 1 | 1 | |||
| ≦19 teeth | 1.06 (0.82–1.39) | 0.65 | 1.47 (1.07–2.02) | 0.02 * | 1.25 (1.02–1.52) | 0.03 * | |
| Waist (cm) | ≧20 teeth | 1 | 1 | 1 | |||
| ≦19 teeth | 0.91 (0.72–1.15) | 0.42 | 1.12 (0.91–1.37) | 0.31 | 0.99 (0.85–1.15) | 0.89 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ono, T.; Kato, S.; Kokubo, Y.; Hasegawa, Y.; Kosaka, T.; Maeda, Y.; Okamura, T.; Miyamoto, Y.; Ikebe, K. Tooth Loss Related with Prevalence of Metabolic Syndrome in a General Urban Japanese Population: The Suita Study. Int. J. Environ. Res. Public Health 2022, 19, 6441. https://doi.org/10.3390/ijerph19116441
Ono T, Kato S, Kokubo Y, Hasegawa Y, Kosaka T, Maeda Y, Okamura T, Miyamoto Y, Ikebe K. Tooth Loss Related with Prevalence of Metabolic Syndrome in a General Urban Japanese Population: The Suita Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6441. https://doi.org/10.3390/ijerph19116441
Chicago/Turabian StyleOno, Takahiro, Satoshi Kato, Yoshihiro Kokubo, Yoko Hasegawa, Takayuki Kosaka, Yoshinobu Maeda, Tomonori Okamura, Yoshihiro Miyamoto, and Kazunori Ikebe. 2022. "Tooth Loss Related with Prevalence of Metabolic Syndrome in a General Urban Japanese Population: The Suita Study" International Journal of Environmental Research and Public Health 19, no. 11: 6441. https://doi.org/10.3390/ijerph19116441
APA StyleOno, T., Kato, S., Kokubo, Y., Hasegawa, Y., Kosaka, T., Maeda, Y., Okamura, T., Miyamoto, Y., & Ikebe, K. (2022). Tooth Loss Related with Prevalence of Metabolic Syndrome in a General Urban Japanese Population: The Suita Study. International Journal of Environmental Research and Public Health, 19(11), 6441. https://doi.org/10.3390/ijerph19116441