
Physical Restraint Events in Psychiatric Hospitals in Hong Kong: A Cohort Register Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
- What are the general characteristics of the physical-restraint incidents?
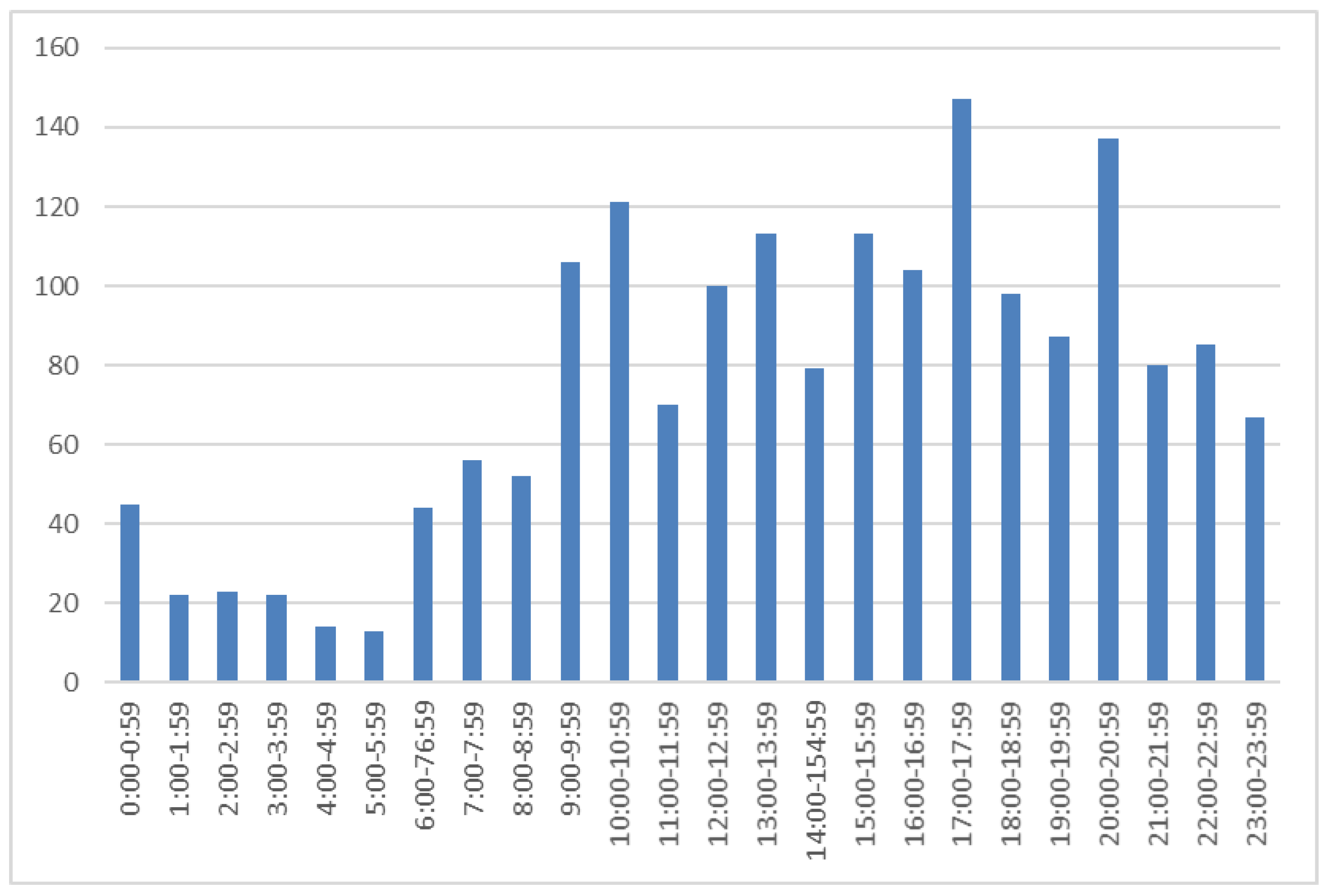
- When did the events of physical restraint occur?
- What types of physical-restraint events occurred?
- What are the reasons for physical restraint and what factors are associated with these events?
2. Materials and Methods
2.1. Design and Setting
2.2. Procedures
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Characteristics
3.2. The Time of Physical Restraint Events
3.3. Types of Physical Restraint
3.4. Reasons for Physical Restraint and Alternative Methods
4. Discussion
4.1. What the Study Adds to the Existing Evidence
4.2. Strengths and Limitations
4.3. Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Szmukler, G. Compulsion and “Coercion” in Mental Health Care. World Psychiatry 2015, 14, 259–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drew, N.; Funk, M.; Tang, S.; Lamichhane, J.; Chávez, E.; Katontoka, S.; Pathare, S.; Lewis, O.; Gostin, L.; Saraceno, B. Human Rights Violations of People with Mental and Psychosocial Disabilities: An Unresolved Global Crisis. Lancet 2011, 378, 1664–1675. [Google Scholar] [CrossRef]
- Sugiura, K.; Mahomed, F.; Saxena, S.; Patel, V. An End to Coercion: Rights and Decision-Making in Mental Health Care. Bull. World Health Organ. 2020, 98, 52–58. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Report of the Special Rapporteur on the Rights of Persons with Disabilities (A/HRC/37/56). Available online: http://www.un.org/en/ga/search/view_doc.asp?symbol=A/HRC/37/56 (accessed on 25 March 2022).
- Kersting, X.A.K.; Hirsch, S.; Steinert, T. Physical Harm and Death in the Context of Coercive Measures in Psychiatric Patients: A Systematic Review. Front. Psychiatry 2019, 10, 400. [Google Scholar] [CrossRef]
- Steinert, T.; Birk, M.; Flammer, E.; Bergk, J. Subjective Distress after Seclusion or Mechanical Restraint: One-Year Follow-Up of a Randomized Controlled Study. Psychiatr. Serv. 2013, 64, 1012–1017. [Google Scholar] [CrossRef]
- Nelstrop, L.; Chandler-Oatts, J.; Bingley, W.; Bleetman, T.; Corr, F.; Cronin-Davis, J.; Fraher, D.-M.; Hardy, P.; Jones, S.; Gournay, K.; et al. A Systematic Review of the Safety and Effectiveness of Restraint and Seclusion as Interventions for the Short-Term Management of Violence in Adult Psychiatric Inpatient Settings and Emergency Departments. Worldviews Evid.—Based Nurs. 2006, 3, 8–18. [Google Scholar] [CrossRef]
- Lepping, P.; Masood, B.; Flammer, E.; Noorthoorn, E.O. Comparison of Restraint Data from Four Countries. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1301–1309. [Google Scholar] [CrossRef]
- Newton-Howes, G.; Savage, M.K.; Arnold, R.; Hasegawa, T.; Staggs, V.; Kisely, S. The Use of Mechanical Restraint in Pacific Rim Countries: An International Epidemiological Study. Epidemiol. Psychiatr. Sci. 2020, 29, e190. [Google Scholar] [CrossRef]
- Steinert, T.; Lepping, P.; Bernhardsgrütter, R.; Conca, A.; Hatling, T.; Janssen, W.; Keski-Valkama, A.; Mayoral, F.; Whittington, R. Incidence of Seclusion and Restraint in Psychiatric Hospitals: A Literature Review and Survey of International Trends. Soc. Psychiatr. Epidemiol. 2010, 45, 889–897. [Google Scholar] [CrossRef]
- The Joint Comission, Division of Healthcare Improvement. De-Escalation in Health Care. Quick Safety, Issue 47. Available online: https://www.jointcommission.org/-/media/tjc/documents/resources/workplace-violence/qs_deescalation_1_28_18_final.pdf?db=web&hash=DD556FD4E3E4FA13B64E9A4BF4B5458A (accessed on 25 March 2022).
- Bleijlevens, M.H.C.; Wagner, L.M.; Capezuti, E.; Hamers, J.P.H.; the International Physical Restraint Workgroup. Physical Restraints: Consensus of a Research Definition Using a Modified Delphi Technique. J. Am. Geriatr. Soc. 2016, 64, 2307–2310. [Google Scholar] [CrossRef]
- American Psychiatric Nurses Association. APNA Seclusion & Restraint Standards of Practice. Available online: https://www.apna.org/resources/apna-seclusion-and-restraint-standards-of-practice/ (accessed on 25 March 2022).
- National Institute for Clinical Excellence (NICE). Violence and Aggression: Short-Term Management in Mental Health, Health and Community Settings. Available online: Nice.org.uk/guidance/ng10 (accessed on 25 March 2022).
- Restraint Reduction Network (RRN). Training Standards. 1st Edition Ridley J & Leitch. Version 1.3. Available online: https://restraintreductionnetwork.org/wp-content/uploads/2021/08/RRN_standards_phase_8_accessible.pdf (accessed on 3 January 2022).
- Fukasawa, M.; Miyake, M.; Suzuki, Y.; Fukuda, Y.; Yamanouchi, Y. Relationship between the Use of Seclusion and Mechanical Restraint and the Nurse-Bed Ratio in Psychiatric Wards in Japan. Int. J. Law Psychiatry 2018, 60, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Wang, C.; Xiao, A.; Xia, Z.; Yu, L.; Lin, J.; Liao, Y.; Xu, Y.; Zhang, Y. Physical Restraint in Mental Health Nursing: A Concept Analysis. Int. J. Nurs. Sci. 2019, 6, 343–348. [Google Scholar] [CrossRef] [PubMed]
- An, F.-R.; Sha, S.; Zhang, Q.-E.; Ungvari, G.S.; Ng, C.H.; Chiu, H.F.K.; Wu, P.-P.; Jin, X.; Zhou, J.-S.; Tang, Y.-L.; et al. Physical Restraint for Psychiatric Patients and Its Associations with Clinical Characteristics and the National Mental Health Law in China. Psychiatry Res. 2016, 241, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.-M.; Xiang, Y.-T.; Zhou, J.-S.; Gou, L.; Himelhoch, S.; Ungvari, G.S.; Chiu, H.F.K.; Lai, K.Y.C.; Wang, X.-P. Frequency of Physical Restraint and Its Associations with Demographic and Clinical Characteristics in a Chinese Psychiatric Institution: Frequency of Physical Restraint and Its Associations With Demographic and Clinical Characteristics in a Chinese Psychiatric Institution. Perspect. Psychiatr. Care 2014, 50, 251–256. [Google Scholar] [CrossRef]
- Wu, W.W.K. Psychosocial correlates of patients being physically restrained within the first 7 days in an acute psychiatric admission ward: Retrospective case record review. East Asian Arch. Psychiatry 2015, 25, 47–57. [Google Scholar]
- Hsu, C.-C.; Chan, H.-Y. Factors Associated with Prolonged Length of Stay in the Psychiatric Emergency Service. PLoS ONE 2018, 13, e0202569. [Google Scholar] [CrossRef] [Green Version]
- Ye, J.; Xiao, A.; Yu, L.; Guo, J.; Lei, H.; Wei, H.; Luo, W. Staff Training Reduces the Use of Physical Restraint in Mental Health Service, Evidence-Based Reflection for China. Arch. Psychiatr. Nurs. 2018, 32, 488–494. [Google Scholar] [CrossRef]
- Wu, K.K.; Cheng, J.P.; Leung, J.; Chow, L.; Lee, C. Patients’ Reports of Traumatic Experience and Posttraumatic Stress in Psychiatric Settings. East Asian Arch. Psychiatry 2020, 30, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Weltens, I.; Bak, M.; Verhagen, S.; Vandenberk, E.; Domen, P.; van Amelsvoort, T.; Drukker, M. Aggression on the Psychiatric Ward: Prevalence and Risk Factors. A Systematic Review of the Literature. PLoS ONE 2021, 16, e0258346. [Google Scholar] [CrossRef]
- Luciano, M.; Sampogna, G.; Del Vecchio, V.; Pingani, L.; Palumbo, C.; De Rosa, C.; Catapano, F.; Fiorillo, A. Use of Coercive Measures in Mental Health Practice and Its Impact on Outcome: A Critical Review. Expert Rev. Neurother. 2014, 14, 131–141. [Google Scholar] [CrossRef]
- Gooding, P.; McSherry, B.; Roper, C. Preventing and Reducing ‘Coercion’ in Mental Health Services: An International Scoping Review of English-language Studies. Acta Psychiatr. Scand. 2020, 142, 27–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beghi, M.; Peroni, F.; Gabola, P.; Rossetti, A.; Cornaggia, C.M. Prevalence and risk factors for the use of restraint in psychiatry: A systematic review. Riv. Di Psichiatr. 2013, 48, 10–22. [Google Scholar]
- Hospital Authority. Guidelines on the Use of Physical Restraint for Patients in Psychiatric Settings; HAHO-COC-GL-Psy-007-V03. Version 3; Hospital Authority Head Office: Hong Kong SAR, China, 2021. [Google Scholar]
- World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Al-Maraira, O.A.; Hayajneh, F.A. Use of Restraint and Seclusion in Psychiatric Settings: A Literature Review. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 32–39. [Google Scholar] [CrossRef] [PubMed]
- McKenna, B.; McEvedy, S.; Maguire, T.; Ryan, J.; Furness, T. Prolonged Use of Seclusion and Mechanical Restraint in Mental Health Services: A Statewide Retrospective Cohort Study. Int. J. Ment. Health Nurs. 2017, 26, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Nawka, A.; Kalisova, L.; Raboch, J.; Giacco, D.; Cihal, L.; Onchev, G.; Karastergiou, A.; Solomon, Z.; Fiorillo, A.; Del Vecchio, V.; et al. Gender Differences in Coerced Patients with Schizophrenia. BMC Psychiatry 2013, 13, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howell, A.-M.; Burns, E.M.; Bouras, G.; Donaldson, L.J.; Athanasiou, T.; Darzi, A. Can Patient Safety Incident Reports Be Used to Compare Hospital Safety? Results from a Quantitative Analysis of the English National Reporting and Learning System Data. PLoS ONE 2015, 10, e0144107. [Google Scholar] [CrossRef] [PubMed]
- Iversen, V.C.; Aasen, O.H.; Cüneyt Güzey, I.; Helvik, A.S. Incidence of violent behavior among patients in Psychiatric Intensive Care Units. Eur. J. Psychiatry 2016, 30, 67–78. [Google Scholar]
- Noda, T.; Sugiyama, N.; Sato, M.; Ito, H.; Sailas, E.; Putkonen, H.; Kontio, R.; Joffe, G. Influence of Patient Characteristics on Duration of Seclusion/Restrain in Acute Psychiatric Settings in Japan: Duration of Seclusion/Restraint in Japan. Psychiatry Clin. Neurosci. 2013, 67, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Kuosmanen, A.; Tiihonen, J.; Repo-Tiihonen, E.; Turunen, H. Voluntary Patient Safety Incidents Reporting in Forensic Psychiatry—What Do the Reports Tell Us? Psychiatr. Ment. Health Nurs. 2022, 29, 36–47. [Google Scholar] [CrossRef]
- Knutzen, M.; Bjørkly, S.; Eidhammer, G.; Lorentzen, S.; Helen Mjøsund, N.; Opjordsmoen, S.; Sandvik, L.; Friis, S. Mechanical and Pharmacological Restraints in Acute Psychiatric Wards—Why and How Are They Used? Psychiatry Res. 2013, 209, 91–97. [Google Scholar] [CrossRef]
- Knutzen, M.; Bjørkly, S.; Eidhammer, G.; Lorentzen, S.; Mjøsund, N.H.; Opjordsmoen, S.; Sandvik, L.; Friis, S. Corrigendum to “Characteristics of Patients Frequently Subjected to Pharmacological and Mechanical Restraint—A Register Study in Three Norwegian Acute Psychiatric Wards” [Psychiatry Res. 215 127–133]. Psychiatry Res. 2014, 219, 714. [Google Scholar] [CrossRef]
- Narita, Z.; Inagawa, T.; Yokoi, Y.; Stickley, A.; Maruo, K.; Yamada, Y.; Sugawara, N. Factors Associated with the Use and Longer Duration of Seclusion and Restraint in Psychiatric Inpatient Settings: A Retrospective Chart Review. Int. J. Psychiatry Clin. Pract. 2019, 23, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Miodownik, C.; Friger, M.D.; Orev, E.; Gansburg, Y.; Reis, N.; Lerner, V. Clinical and Demographic Characteristics of Secluded and Mechanically Restrained Mentally Ill Patients: A Retrospective Study. Isr. J. Health Policy Res. 2019, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Nieuwenhuis, J.G.; Noorthoorn, E.O.; Nijman, H.L.I.; Naarding, P.; Mulder, C.L. A Blind Spot? Screening for Mild Intellectual Disability and Borderline Intellectual Functioning in Admitted Psychiatric Patients: Prevalence and Associations with Coercive Measures. PLoS ONE 2017, 12, e0168847. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Revuelta, J.I.; Torrecilla-Olavarrieta, R.; García-Spínola, E.; López-Martín, Á.; Guerrero-Vida, R.; Mongil-San Juan, J.M.; Rodríguez-Gómez, C.; Pascual-Paño, J.M.; González-Sáiz, F.; Villagrán-Moreno, J.M. Factors Associated with the Use of Mechanical Restraint in a Mental Health Hospitalization Unit: 8-year Retrospective Analysis. J. Psychiatr. Ment. Health Nurs. 2021, 28, 1052–1064. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulou, C.; Doherty, C.; Tosey, P. How Effective Are Incident-Reporting Systems for Improving Patient Safety? A Systematic Literature Review: Incident-Reporting Systems for Improving Patients’ Safety. Milbank 2015, 93, 826–866. [Google Scholar] [CrossRef] [Green Version]
- Sashidharan, S.P.; Mezzina, R.; Puras, D. Reducing Coercion in Mental Healthcare. Epidemiol. Psychiatr. Sci. 2019, 28, 605–612. [Google Scholar] [CrossRef]
- Lantta, T.; Varpula, J.; Cheung, T.; Wong, W.K.; Cheng, P.Y.I.; Ng, T.; Ng, C.F.; Yam, C.P.; Ip, G.; Bressington, D.; et al. Prevention and Management of Aggressive Behaviour in Patients at Psychiatric Hospitals: A Document Analysis of Clinical Practice Guidelines in Hong Kong. Int. J. Ment. Health Nurs. 2020, 29, 1079–1091. [Google Scholar] [CrossRef]
- Mann, K.; Gröschel, S.; Singer, S.; Breitmaier, J.; Claus, S.; Fani, M.; Rambach, S.; Salize, H.-J.; Lieb, K. Evaluation of Coercive Measures in Different Psychiatric Hospitals: The Impact of Institutional Characteristics. BMC Psychiatry 2021, 21, 419. [Google Scholar] [CrossRef]
- Välimäki, M.; Yang, M.; Vahlberg, T.; Lantta, T.; Pekurinen, V.; Anttila, M.; Normand, S.-L. Trends in the Use of Coercive Measures in Finnish Psychiatric Hospitals: A Register Analysis of the Past Two Decades. BMC Psychiatry 2019, 19, 230. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.K.; Välimäki, M.; Lantta, T. The knowledge, practice and attitudes of nurses regarding physical restraint: Survey results from psychiatric inpatient settings. Int. J. Environ. Res. Public Health 2021, 18, 6747. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.T.; Chan, C.W.; Lam, L.W.; Kam, C.W. Psychiatric inpatients’ perceptions of positive and negative aspects of physical restraint. Patient Educ. Couns. 2015, 59, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Sethi, F.; Parkes, J.; Baskind, E.; Paterson, B.; O’Brien, A. Restraint in mental health settings: Is it time to declare a position? Br. J. Psychiatry 2018, 212, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Reymann, S.; Schoretsanitis, G.; Egger, S.T.; Mohonko, A.; Kirschner, M.; Vetter, S.; Homan, P.; Selfritz, E.; Burrer, A. Use of Long-Acting Injectable Antipsychotics in Inpatients with Schizophrenia Spectrum Disorder in an Academic Psychiatric Hospital in Switzerland. J. Pers. Med. 2022, 12, 441. [Google Scholar] [CrossRef]
- Olayinka, O.; Oyelakin, A.; Cherukupally, K.; Virk, I.; Ojimba, C.; Khadka, S.; Maksymenko, A.; Fouron, P.; Khandaker, T.; Olupona, T.; et al. Use of long-acting injectable antipsychotic in an inpatient unit of a community teaching hospital. Psychiatry J. 2019, 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, S.; Steinert, T. Measures to Avoid Coercion in Psychiatry and Their Efficacy. Dtsch. Ärzteblatt Int. 2019, 116, 336–343. [Google Scholar] [CrossRef]

{kind=link}
| Hospital A | Hospital B | |
|---|---|---|
| Number of study wards | 6 | 8 |
| Specialty of the wards | 4 acute admission wards 2 rehabilitation wards | Intensive care wards for acute care |
| Gender type of the wards | 3 female wards 3 male wards | 4 female wards 4 male wards |
| A range of a number of beds in each study ward | 40–48 beds | 50–65 beds |
| Number of staff working on the study wards | Around 20 nurses per ward | About 25 nurses per ward |
| Typical age distribution of patients | 18–65 years | 16–64 years |
| Two most typical diagnoses | Schizophrenia Mood disorder | Schizophrenia Mood disorder |
| Number of patients treated on the study wards during the data collection | 913 | 3257 |
| f | % | Mean (SD) | |
|---|---|---|---|
| Physical restraints (f = 1798) | |||
| Hospital A | 616 | 34 | |
| Hospital B | 1182 | 66 | |
| Patient age in each incident (f = 1790) | 39.96 (15.73) | ||
| Range 13–95 years | |||
| Patient gender in each incident (f = 1798) | |||
| Male | 899 | 50 | |
| Female | 899 | 50 | |
| Patient legal status in each event (f = 1593) | |||
| Voluntary | 1251 | 70 | |
| Non-voluntary | 342 | 30 | |
| * Diagnosis, ICD-10 1 (f = 1106) | |||
| Neurodevelopmental disorder | 199 | 18 | |
| Schizophrenia spectrum and other psychotic disorder | 672 | 61 | |
| Affective/mood disorder | 151 | 13 | |
| Substance-related addictive disorder | 32 | 3 | |
| Other | 52 | 5 |
| Safety West | Waist Belt | Limb Holder | Magnetic Traps | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| f | % | f | % | f | % | f | % | f | % | |
| Minutes | ||||||||||
| −60 | 0 | 0 | 8 | 8 | 95 | 91 | 1 | 1 | 104 | 5.24 |
| 61–120 | 4 | 0.4 | 163 | 15.1 | 906 | 84.1 | 4 | 0.4 | 1077 | 52.23 |
| 121–180 | 0 | 0 | 24 | 12 | 175 | 88 | 0 | 0 | 199 | 10.02 |
| 181–240 | 0 | 0 | 86 | 14 | 512 | 85 | 6 | 1 | 604 | 30.41 |
| 241- | 0 | 0 | 0 | 0 | 2 | 100 | 0 | 0 | 2 | 0.1 |
| Totally | 4 | 281 | 1690 | 11 | 1986 | |||||
| Total | <120 * | 120 *≤ | |||||
|---|---|---|---|---|---|---|---|
| f | f | % | f | % | Chi Square (df) | p | |
| Variables | |||||||
| Age | 9.11 (3) | 0.028 | |||||
| 30 or below | 642 | 373 | 58.1% | 269 | 41.9% | ||
| 31–40 | 295 | 165 | 55.9% | 130 | 44.1% | ||
| 41–50 | 349 | 215 | 61.6% | 134 | 38.4% | ||
| 51 or above | 504 | 329 | 65.3% | 175 | 34.7% | ||
| Gender | 111.47 (1) | <0.001 | |||||
| Male | 899 | 433 | 48.2% | 456 | 50.7% | ||
| Female | 899 | 652 | 72.5% | 247 | 27.5% | ||
| Legal status | 10.61 (1) | 0.001 | |||||
| Voluntary | 1251 | 786 | 62.8% | 465 | 37.2% | ||
| Other | 547 | 299 | 54.7% | 248 | 45.3% | ||
| Diagnosis | 30.04 (4) | <0.001 | |||||
| Neurodevelopmental disorder | 199 | 79 | 39.7% | 120 | 60.3% | ||
| Schizophrenia spectrum and other | 672 | 404 | 60.1% | 268 | 39.9% | ||
| Affective/mood disorder | 151 | 90 | 59.6% | 61 | 40.4% | ||
| Substance-related addictive disorder | 32 | 16 | 50.0% | 16 | 50.0% | ||
| Other | 52 | 35 | 67.3% | 17 | 32.7% | ||
| * Minutes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Välimäki, M.; Lam, Y.T.J.; Hipp, K.; Cheng, P.Y.I.; Ng, T.; Ip, G.; Lee, P.; Cheung, T.; Bressington, D.; Lantta, T. Physical Restraint Events in Psychiatric Hospitals in Hong Kong: A Cohort Register Study. Int. J. Environ. Res. Public Health 2022, 19, 6032. https://doi.org/10.3390/ijerph19106032
Välimäki M, Lam YTJ, Hipp K, Cheng PYI, Ng T, Ip G, Lee P, Cheung T, Bressington D, Lantta T. Physical Restraint Events in Psychiatric Hospitals in Hong Kong: A Cohort Register Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6032. https://doi.org/10.3390/ijerph19106032
Chicago/Turabian StyleVälimäki, Maritta, Yuen Ting Joyce Lam, Kirsi Hipp, Po Yee Ivy Cheng, Tony Ng, Glendy Ip, Paul Lee, Teris Cheung, Daniel Bressington, and Tella Lantta. 2022. "Physical Restraint Events in Psychiatric Hospitals in Hong Kong: A Cohort Register Study" International Journal of Environmental Research and Public Health 19, no. 10: 6032. https://doi.org/10.3390/ijerph19106032
APA StyleVälimäki, M., Lam, Y. T. J., Hipp, K., Cheng, P. Y. I., Ng, T., Ip, G., Lee, P., Cheung, T., Bressington, D., & Lantta, T. (2022). Physical Restraint Events in Psychiatric Hospitals in Hong Kong: A Cohort Register Study. International Journal of Environmental Research and Public Health, 19(10), 6032. https://doi.org/10.3390/ijerph19106032