
Age and Training-Related Changes on Body Composition and Fitness in Male Amateur Cyclists

 ,
,  , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Experimental Design
2.4. Procedures
2.4.1. Anthropometric Assessment
2.4.2. Cardiorespiratory Fitness Assessment
2.4.3. Statistical Analyses
3. Results
3.1. Correlations between Skin Folds and Age and Training Kilometers
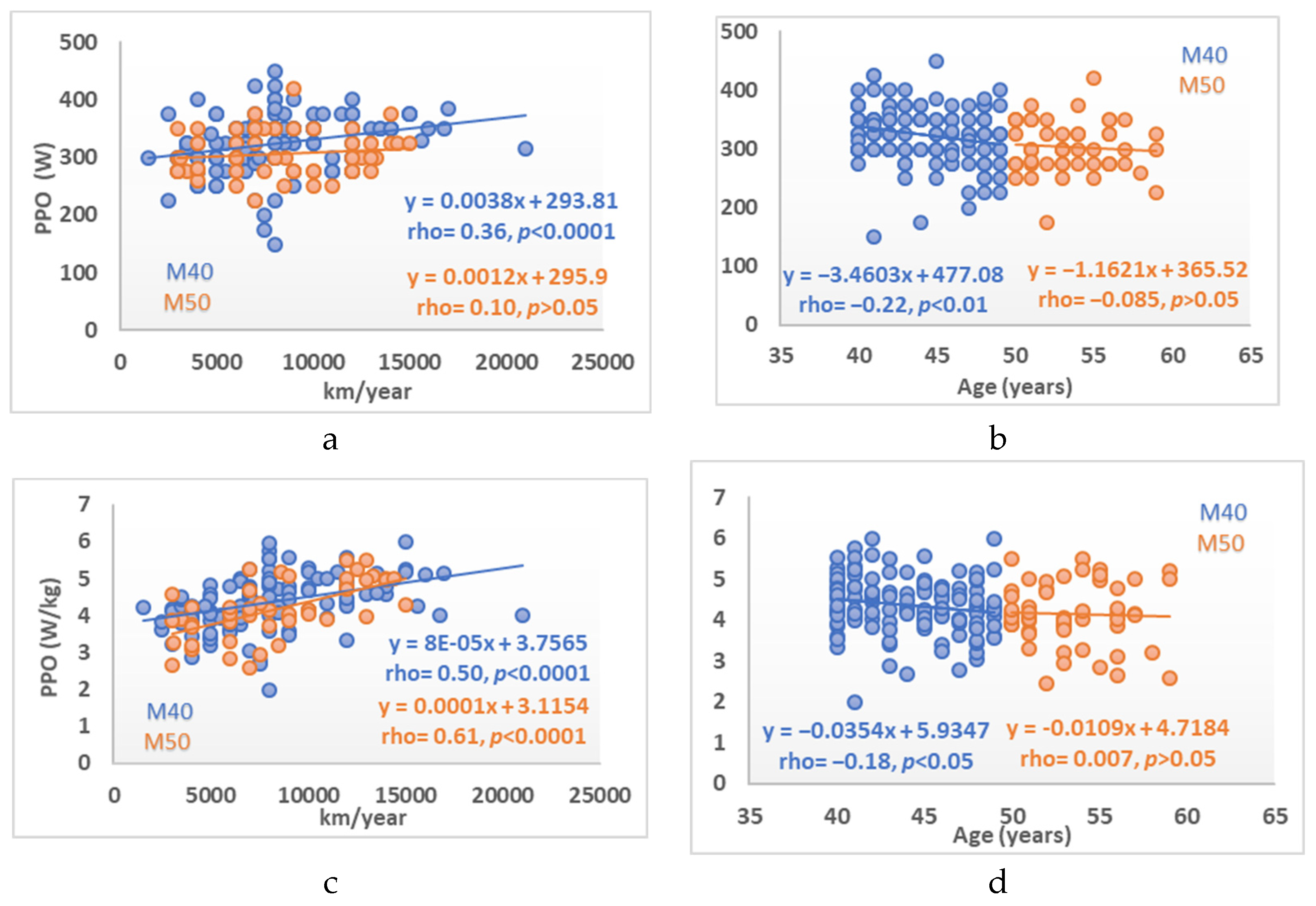
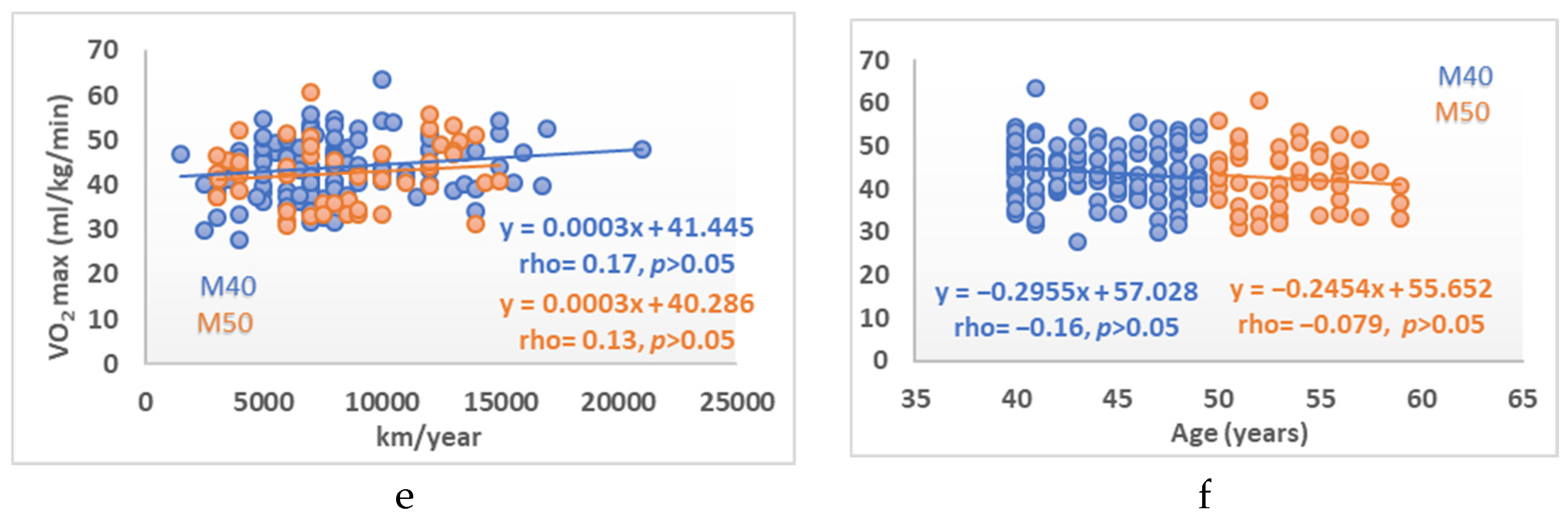
3.2. Correlations between Body Composition and Cardiovascular Fitness Variables with Age and km/year
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valenzuela, P.L.; Maffiuletti, N.A.; Joyner, M.J.; Lucia, A.; Lepers, R. Lifelong Endurance Exercise as a Countermeasure Against Age-Related V.O 2 max Decline: Physiological Overview and Insights from Masters Athletes. Sport. Med. 2020, 50, 703–716. [Google Scholar] [CrossRef]
- Ekblom-Bak, E.; Ekblom, B.; Söderling, J.; Börjesson, M.; Blom, V.; Kallings, L.V.; Hemmingsson, E.; Andersson, G.; Wallin, P.; Ekblom, Ö. Sex- and age-specific associations between cardiorespiratory fitness, CVD morbidity and all-cause mortality in in 266.109 adults. Prev. Med. 2019, 127, 105799. [Google Scholar] [CrossRef]
- Maharam, L.G.; Bauman, P.A.; Kalman, D.; Skolnik, H.; Perle, S.M. Masters athletes. Factors affecting performance. Sport. Med. 1999, 28, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, J.; Ruedl, G.; Posch, M.; Greier, K.; Burtscher, M. The upper limit of cardiorespiratory fitness associated with longevity: An update. AIMS Public Health 2019, 6, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Bagley, L.; McPhee, J.S.; Ganse, B.; Müller, K.; Korhonen, M.T.; Rittweger, J.; Degens, H. Similar relative decline in aerobic and anaerobic power with age in endurance and power master athletes of both sexes. Scand. J. Med. Sci. Sport 2019, 29, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Ackland, T.R.; Lohman, T.G.; Sundgot-Borgen, J.; Maughan, R.J.; Meyer, N.L.; Stewart, A.D.; Mller, W. Current status of body composition assessment in sport: Review and position statement on behalf of the Ad Hoc research working group on body composition health and performance, under the auspices of the I.O.C. medical commission. Sport. Med. 2012, 42, 227–249. [Google Scholar] [CrossRef] [PubMed]
- Legaz, A. Changes in performance, skinfold thicknesses, and fat patterning after three years of intense athletic conditioning in high level runners. Br. J. Sports Med. 2005, 39, 851–856. [Google Scholar] [CrossRef]
- Knechtle, B.; Wirth, A.; Baumann, B.; Knechtle, P.; Rosemann, T.; Oliver, S. Differential Correlations Between Anthropometry, Training Volume, and Performance in Male and Female Ironman Triathletes. J. Strength Cond. Res. 2010, 24, 2785–2793. [Google Scholar] [CrossRef] [PubMed]
- Legaz Arrese, A.; González Badillo, J.J.; Serrano Ostáriz, E. Differences in skinfold thicknesses and fat distribution among top-class runners. J. Sports Med. Phys. Fit. 2005, 45, 512–517. [Google Scholar]
- Keating, S.E.; Machan, E.A.; O’Connor, H.T.; Gerofi, J.A.; Sainsbury, A.; Caterson, I.D.; Johnson, N.A. Continuous Exercise but Not High Intensity Interval Training Improves Fat Distribution in Overweight Adults. J. Obes. 2014, 2014, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bieuzen, F.; Hausswirth, C.; Louis, J.; Brisswalter, J. Age-related changes in neuromuscular function and performance following a high-intensity intermittent task in endurance-trained men. Gerontology 2010, 56, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Seals, D.R. Endurance exercise performance in Masters athletes: Age-associated changes and underlying physiological mechanisms. J. Physiol. 2008, 586, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Lepers, R.; Stapley, P.J. Master athletes are extending the limits of human endurance. Front. Physiol. 2016, 12, 613. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Educación. Encuesta de Hábitos Deportivos 2015; Ministerio de Educación, Cultura y Deporte: Madrid, Spain, 2015; ISBN NIPO 030-15-402-9.
- JAMA Declaration of Helsinki World Medical Association Declaration of Helsinki. Bull. World Health Organ. 2013, 310, 2191–2194.
- Aird, T.P.; Davies, R.W.; Carson, B.P. Effects of fasted vs fed-state exercise on performance and post-exercise metabolism: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2018, 28, 1476–1493. [Google Scholar] [CrossRef]
- Ormsbee, M.J.; Bach, C.W.; Baur, D.A. Pre-exercise nutrition: The role of macronutrients, modified starches and supplements on metabolism and endurance performance. Nutrients 2014, 29, 1782–1808. [Google Scholar] [CrossRef] [PubMed]
- Marfell-Jones, M.; Olds, L. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2006. [Google Scholar]
- Peterson, M.J.; Czerwinski, S.A.; Siervogel, R.M. Development and validation of skinfold-thickness prediction equations with a 4-compartment model. Am. J. Clin. Nutr. 2003, 77, 1186–1191. [Google Scholar] [CrossRef]
- International Council of Sport Science and Physical Education|Science Education Policy. Available online: icsspe.org (accessed on 12 December 2021).
- Uth, N.; Sørensen, H.; Overgaard, K.; Pedersen, P.K. Estimation of VO2max from the ratio between HRmax and HRrest—The heart rate ratio method. Eur. J. Appl. Physiol. 2004, 91, 111–115. [Google Scholar] [CrossRef]
- Bandyopadhyay, A. Prediction of maximum oxygen uptake by using the heart rate ratio method in Indian university students. J. Hum. Ergol. 2013, 42, 55–63. [Google Scholar]
- Peiffer, J.J.; Abbiss, C.R.; Chapman, D.; Laursen, P.B.; Parker, D.L. Physiological characteristics of masters-level cyclists. J. Strength Cond. Res. 2008, 22, 1434–1440. [Google Scholar] [CrossRef]
- Sousa, C.V.; Knechtle, B.; Nikolaidis, P.T. Longitudinal Performance Analysis in Ultra-Triathlon of the World’s 2 Best Master Triathletes. Int. J. Sports Physiol. Perform. 2020, 15, 1480–1484. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Craig, N.P.; Hawley, J.A. The bioenergetics of world class cycling. J. Sci. Med. Sport 2000, 3, 414–433. [Google Scholar] [CrossRef]
- Yarizadeh, H.; Eftekhar, R.; Anjom-Shoae, J.; Speakman, J.R.; Djafarian, K. The Effect of Aerobic and Resistance Training and Combined Exercise Modalities on Subcutaneous Abdominal Fat: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Adv. Nutr. 2020, 12, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ponti, F.; Santoro, A.; Mercatelli, D.; Gasperini, C.; Conte, M.; Martucci, M.; Sangiorgi, L.; Franceschi, C.; Bazzocchi, A. Aging and Imaging Assessment of Body Composition: From Fat to Facts. Front. Endocrinol. 2020, 10, 861. [Google Scholar] [CrossRef] [PubMed]
- Auyeung, T.W.; Lee, J.S.W.; Leung, J.; Kwok, T.; Leung, P.C.; Woo, J. Survival in older men may benefit from being slightly overweight and centrally obese-a 5-year follow-up study in 4000 older adults using DXA. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X. Changes in body composition and metabolic disease risk. Eur. J. Clin. Nutr. 2019, 73, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Distefano, G.; Goodpaster, B.H. Effects of exercise and aging on skeletal muscle. Cold Spring Harb. Perspect. Med. 2018, 8, a029785. [Google Scholar] [CrossRef]
- Wilson, T.M.; Tanaka, H. Meta-analysis of the age-associated decline in maximal aerobic capacity in men: Relation to training status. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H829–H834. [Google Scholar] [CrossRef]
- Johnson, P.J.; Winter, E.M.; Paterson, D.H.; Koval, J.J.; Nevill, A.M.; Cunningham, D.A. Modelling the influence of age, body size and sex on maximum oxygen uptake in older humans. Exp. Physiol. 2000, 85, 219–225. [Google Scholar] [CrossRef]
- Baker, A.B.; Tang, Y.Q. Aging performance for masters records in athletics, swimming, rowing, cycling, triathlon, and weightlifting. Exp. Aging Res. 2010, 36, 453–477. [Google Scholar] [CrossRef]
- Lepers, R.; Stapley, P.J.; Cattagni, T. Variation of age-related changes in endurance performance between modes of locomotion in men: An analysis of master world records. Int. J. Sports Physiol. Perform. 2018, 13, 394–397. [Google Scholar] [CrossRef]
- Mekari, S.; Dupuy, O.; Martins, R.; Evans, K.; Kimmerly, D.S.; Fraser, S.; Neyedli, H.F. The effects of cardiorespiratory fitness on executive function and prefrontal oxygenation in older adults. GeroScience 2019, 41, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Clausen, J.S.R.; Marott, J.L.; Holtermann, A.; Gyntelberg, F.; Jensen, M.T. Midlife Cardiorespiratory Fitness and the Long-Term Risk of Mortality: 46 Years of Follow-Up. J. Am. Coll. Cardiol. 2018, 72, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Mandsager, K.; Harb, S.; Cremer, P.; Phelan, D.; Nissen, S.E.; Jaber, W. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Netw. Open 2018, 1, e183605. [Google Scholar] [CrossRef] [PubMed]
- Borges, N.R.; Reaburn, P.R.; Doering, T.M.; Argus, C.K.; Driller, M.W. Autonomic cardiovascular modulation in masters and young cyclists following high-intensity interval training. Clin. Auton. Res. 2017, 27, 83–90. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B.; Ahmaidi, S. Parasympathetic reactivation after repeated sprint exercise. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H133–H141. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.L.; Mengelkoch, L.J.; Graves, J.E.; Lowenthal, D.T.; Limacher, M.C.; Foster, C.; Wilmore, J.H. Twenty-year follow-up of aerobic power and body composition of older track athletes. J. Appl. Physiol. 1997, 82, 1508–1516. [Google Scholar] [CrossRef]
- Capelli, C.; Rittveger, J.; Bruseghini, P.; Calabria, E.; Tam, E. Maximal aerobic power and anaerobic capacity in cycling across the age spectrum in male master athletes. Eur. J. Appl. Physiol. 2016, 116, 1395–1410. [Google Scholar] [CrossRef][Green Version]
- Wiswell, R.A.; Hawkins, S.A.; Jaque, S.V.; Hyslop, D.; Constantino, N.; Tarpenning, K.; Marcell, T.; Schroeder, E.T. Relationship between physiological loss, performance decrement, and age in master athletes. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 566, M618–M625. [Google Scholar] [CrossRef]
- Coetzee, B.; Malan, D. Laboratory-based physical and physiological test results that serve as predictors of male, amateur road cyclists’ performance levels. J. Strength Cond. Res. 2018, 32, 2897–2906. [Google Scholar] [CrossRef]
- García-García, O.; Cuba-Dorado, A.; Fernández-Redondo, D.; López-Chicharro, J. Neuromuscular Parameters Predict the Performance in an Incremental Cycling Test. Int. J. Sports Med. 2018, 39, 909–915. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | M 40 (n= 123) | M 50 (n= 53) | p | Change (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | Median | 95% CI | Min. | Max. | Median | 95% CI | |||
| Age (years) | 40 | 49 | 44 | 43.000 to 45.000 | 50 | 59 | 53 | 52.000 to 54.000 | <0.0001 | |
| Weight (kg) | 55 | 98 | 73.3 | 72.800 to 74.970 | 55.4 | 104 | 75.3 | 70.077 to 78.605 | 0.93 | 2.73 |
| Height (cm) | 156.5 | 189 | 170.6 | 169.000 to 172.800 | 160.1 | 184.6 | 169 | 166.959 to 171.141 | 0.039 | |
| BMI (kg/m2) | 19.28 | 33.87 | 25.28 | 24.778 to 25.722 | 21.61 | 35.36 | 25.56 | 24.846 to 26.681 | 0.141 | 1.11 |
| Fat mass (%) | 12.748 | 33.283 | 22.695 | 21.753 to 23.840 | 18.651 | 34.696 | 26.254 | 24.951 to 27.510 | <0.001 | 15.68 |
| HRrest (bpm) | 43 | 88 | 61 | 60.000 to 64.000 | 42 | 88 | 59 | 56.000 to 60.000 | 0.114 | −3.28 |
| HRmax (bpm) | 150 | 206 | 178 | 176.000 to 182.000 | 142 | 187 | 165 | 162.898 to 170.102 | <0.001 | −7.30 |
| HRrec3 (bpm) | 60 | 148 | 112 | 110.000 to 114.000 | 60 | 131 | 100 | 96.000 to 108.000 | <0.001 | −10.71 |
| km/year | 1500 | 21000 | 7000 | 7000.000 to 8000.0 | 3000 | 15000 | 8000 | 7000.0 to 9965.880 | 0.581 | |
| PPO (W) | 150 | 450 | 325 | 325.000 to 350.000 | 175 | 420 | 300 | 275.000 to 325.000 | 0.008 | −7.69 |
| PPO (W/kg) | 2 | 5.99 | 4.36 | 4.237 to 4.567 | 2.465 | 5.49 | 4.072 | 3.977 to 4.241 | 0.048 | −6.61 |
| VO2max (mL/kg/min) | 27.614 | 63.488 | 44.048 | 42.403 to 45.192 | 31.023 | 60.714 | 42.458 | 40.646 to 45.296 | 0.183 | −3.61 |
| METs (mL/kg) | 7.89 | 18.14 | 12.59 | 12.118 to 12.916 | 8.86 | 17.35 | 12.13 | 11.611 to 12.946 | 0.195 | −3.65 |
| Group | Variable | Triceps | Subscapular | Biceps | Iliac Crest | Ileospinale | Abdominal | Front Thigh | Medial Calf |
|---|---|---|---|---|---|---|---|---|---|
| All | Age | 0.16 * | 0.23 ** | 0.24 ** | 0.06 | 0.12 | 0.11 | 0.05 | 0.12 |
| km/year | −0.23 ** | −0.15 * | −0.19 * | −0.32 *** | −0.31 *** | −0.39 *** | −0.13 | −0.2 * | |
| M40 | Age | −0.004 | 0.06 | 0.09 | −0.03 | 0.01 | 0.05 | −0.09 | 0.01 |
| km /year | −0.24 * | −0.16 | −0.17 | −0.32 *** | −0.34 *** | 0.38 *** | −0.16 | −0.18 * | |
| M50 | Age | 0.12 | −0.07 | 0.10 | −0.02 | 0.11 | 0.17 | 0.11 | 0.11 |
| km /year | −0.30 * | −0.24 | −0.38 ** | −0.35 * | −0.27 | −0.48 *** | −0.11 | −0.26 |
| Group | Variable | Weight (kg) | BMI (kg/m2) | Fat mass (%) | HRrest (bpm) | HRmax (bpm) | HRrec3 (bpm) | PPO (W) | PPO (W/kg) | VO2max (mL·min−1·kg−1) |
|---|---|---|---|---|---|---|---|---|---|---|
| All | Age | −0.02 | .069 | 0.31 *** | −0.08 | −0.55 *** | −0.34 *** | −0.30 *** | −0.20 ** | −0.16 * |
| km/year | −0.35 *** | −0.39 *** | −0.20 ** | −0.24 ** | −0.20 ** | −0.36 *** | 0.26 ** | 0.52 *** | 0.15 | |
| M40 | Age | −0.06 | 0.01 | 0.11 | 0.03 | −0.29 ** | −0.215 ** | −0.22 ** | −0.18 * | −0.16 |
| km/year | −0.20 * | −0.35 *** | −0.28 ** | −0.25 ** | −0.17 | −0.26 ** | 0.36 *** | 0.50 *** | 0.17 | |
| M50 | Age | 0.09 | 0.03 | 0.13 | −0.04 | −0.38 ** | −0.175 | −0.085 | 0.01 | −0.08 |
| km/year | −0.62 *** | −0.54 *** | −0.14 | −0.24 | −0.32 * | −0.58 *** | 0.102 | 0.61 *** | 0.13 |
| Independent Variables | Coefficient | Std. Error | t | p | rpartial | rsemipartial | VIF |
|---|---|---|---|---|---|---|---|
| (Constant) | −4.560.375 | ||||||
| Fat mass (%) | −23.234 | 0.7978 | −2.912 | 0.0041 | −0.2198 | 0.156 | 1.627 |
| Height (cm) | 31.358 | 0.4123 | 7.605 | <0.0001 | 0.5072 | 0.4075 | 1.222 |
| km/year | 0.003771 | 0.0007846 | 4.806 | <0.0001 | 0.3486 | 0.2575 | 1.239 |
| HRmax (bpm) | 0.706 | 0.2122 | 3.327 | 0.0011 | 0.2493 | 0.1783 | 1.23 |
| BMI (kg/m2) | 27.619 | 12.546 | 2.201 | 0.0291 | 0.1679 | 0.118 | 1.473 |
| VO2max (mL kg−1 min−1) | 16.182 | 0.427 | 3.79 | 0.0002 | 0.2814 | 0.2031 | 1.198 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvero-Cruz, J.R.; García Romero, J.C.; Ordonez, F.J.; Mongin, D.; Correas-Gómez, L.; Nikolaidis, P.T.; Knechtle, B. Age and Training-Related Changes on Body Composition and Fitness in Male Amateur Cyclists. Int. J. Environ. Res. Public Health 2022, 19, 93. https://doi.org/10.3390/ijerph19010093
Alvero-Cruz JR, García Romero JC, Ordonez FJ, Mongin D, Correas-Gómez L, Nikolaidis PT, Knechtle B. Age and Training-Related Changes on Body Composition and Fitness in Male Amateur Cyclists. International Journal of Environmental Research and Public Health. 2022; 19(1):93. https://doi.org/10.3390/ijerph19010093
Chicago/Turabian StyleAlvero-Cruz, José Ramón, Jerónimo C. García Romero, Francisco Javier Ordonez, Denis Mongin, Lorena Correas-Gómez, Pantelis T. Nikolaidis, and Beat Knechtle. 2022. "Age and Training-Related Changes on Body Composition and Fitness in Male Amateur Cyclists" International Journal of Environmental Research and Public Health 19, no. 1: 93. https://doi.org/10.3390/ijerph19010093
APA StyleAlvero-Cruz, J. R., García Romero, J. C., Ordonez, F. J., Mongin, D., Correas-Gómez, L., Nikolaidis, P. T., & Knechtle, B. (2022). Age and Training-Related Changes on Body Composition and Fitness in Male Amateur Cyclists. International Journal of Environmental Research and Public Health, 19(1), 93. https://doi.org/10.3390/ijerph19010093