
Development and Validation of the Coping Capacity Measurement Scale of Public Health Emergencies in China





Abstract
1. Introduction
2. Methods
2.1. The Theoretical Structure of Public Health Emergency Response Capacity
- Global Constructive Thinking: High scorers are flexible and can adapt their way of thinking to the situation. When the condition is dangerous, they may be pessimistic, but if there is a possible or feasible way to control the problem, they will try to control it. They also accept conditions beyond their control; they accept others as well as themselves; they do not judge others, but they think about how to solve problems.
- Emotional Coping: High scorers deal with difficult situations in ways that do not create undue stress; they accept themselves and do not take things personally; they are not very sensitive to words such as disapproval, failure and rejection.
- Behavioral Coping: High scorers are optimistic, enthusiastic, energetic and responsible. Action is usually taken quickly and time is allocated to focus on solving practical problems.
- Categorical Thinking: High scorers are characterized by extreme thinking, intolerance and distrust of others.
- Superstitious Thinking: High scorers lack critical thinking and rely too much upon personal judgment.
- Negative Thinking: High scorers tend to be defensive against threats, and as a result, tend to be pessimistic, unhelpful, and depressed.
- Naive Optimism: Reasonable optimism is adaptable, energetic and well-liked; on the other hand, the negative side will be simple-minded, the wrong face of adversity.
2.2. Preparation of Public Coping Capacity for Public Health Emergencies
2.3. Statistical Analysis
3. Results
3.1. Development of the Initial Scale of Public Health Emergency Coping Capacity
3.1.1. Distribution and Recovery of Pre-Test Questionnaires
3.1.2. Descriptive Statistics
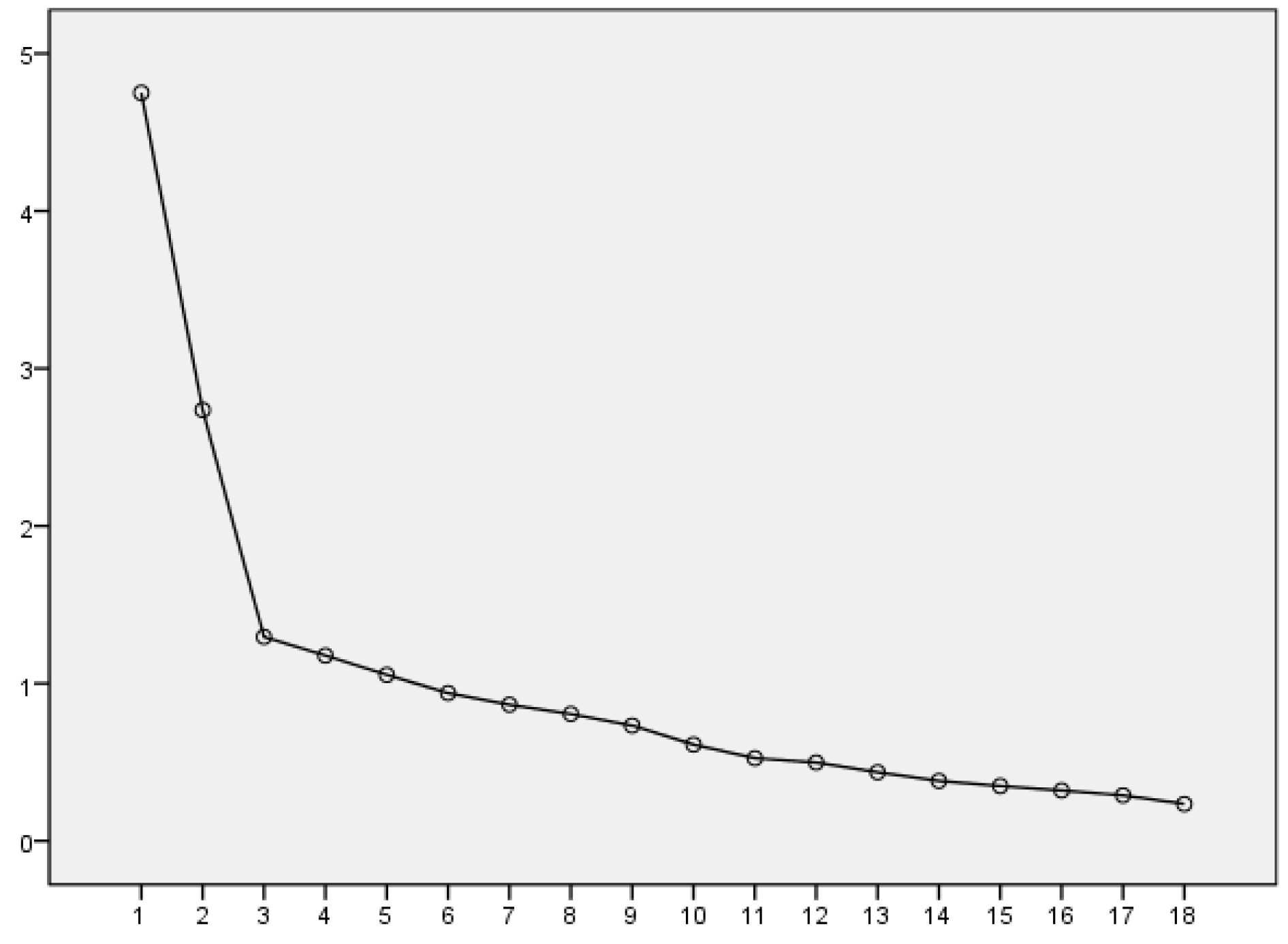
3.1.3. Exploratory Factor Analysis
3.1.4. Reliance Analysis
3.2. Verification of the Initial Scale Public of Coping Capacity to Public Health Emergencies
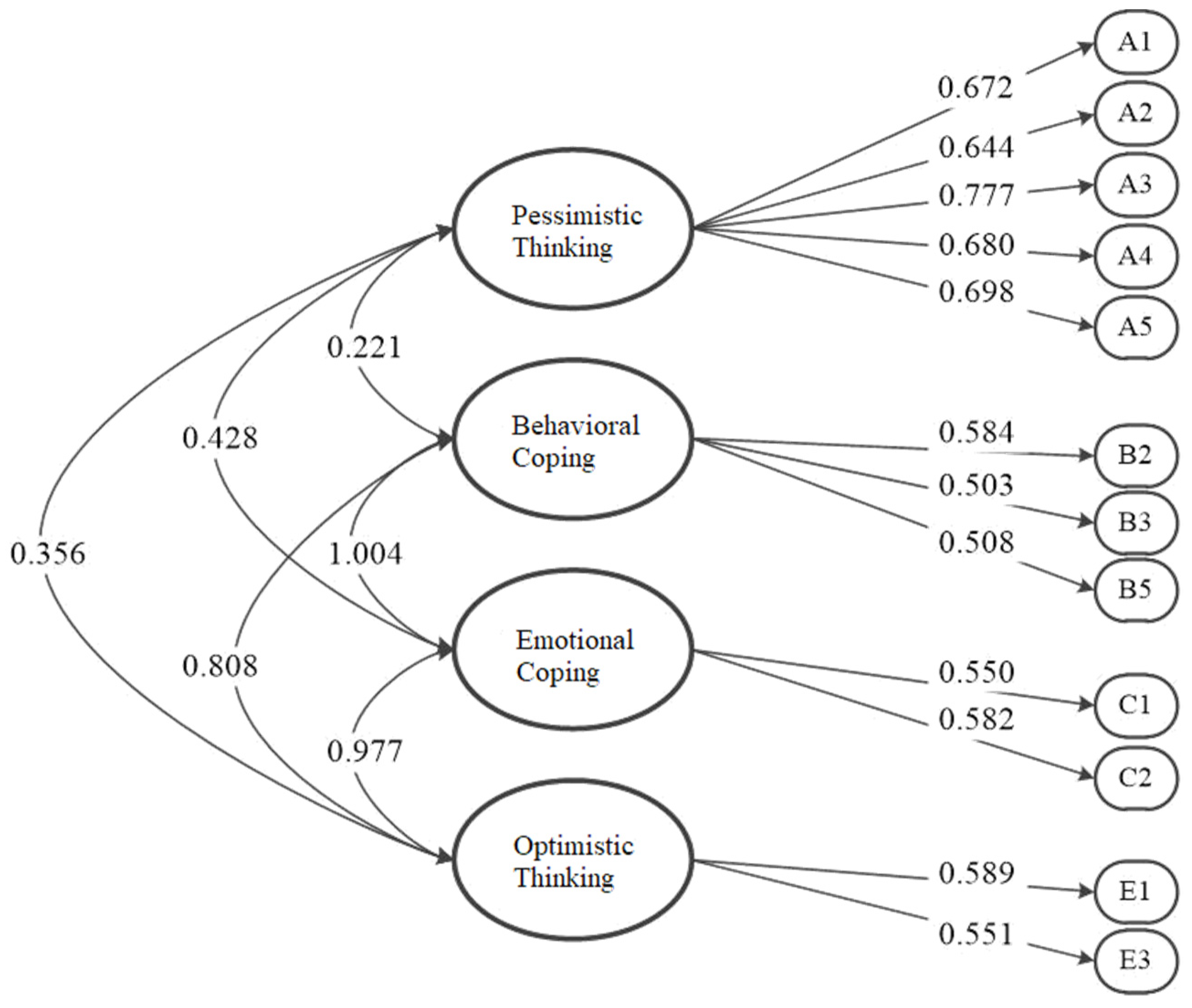
3.2.1. Confirmatory Factor Analysis
3.2.2. Reliability and Validity Analysis
4. Discussion
4.1. Overview of the Leading Research Results
4.2. Theoretical and Practical Significance
4.3. Limitations and Future Research Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Content | No. | Question Item | |
|---|---|---|---|
| Basic population information | Q1 | Gender | |
| Q2 | Age | ||
| Q3 | Academic Level (including ongoing studies) | ||
| Coping capacity measurement scale | Emotional Coping | Q4 | I do not let little things bother me. |
| Q5 | I tend to take things personally. | ||
| Behavioral Coping | Q6 | I am the kind of person who takes action rather than just thinks or complains about the situation. | |
| Q7 | I avoid challenges because it hurts too much when I fail. | ||
| Q8 | When faced with upcoming unpleasant events, I usually carefully think through how I will deal with them. | ||
| Categorical Thinking | Q9 | I think there are many wrong ways, but only one right way, to almost anything. | |
| Q10 | I tend to classify people as either for me or against me. | ||
| Superstitious Thinking | Q11 | I do not believe in any superstition. | |
| Q12 | When something happens to me, I believe it is likely to be balanced by something bad. | ||
| Negative Thinking | Q15 | When I am faced a new situation, I tend to think the worst possible outcome will happen. | |
| Q16 | I tend to dwell more on pleasant than unpleasant incidents from the past. | ||
| Q17 | I get so distressed when I notice that I am doing poorly in something that makes me do worse. | ||
| Naive Optimism | Q13 | If I do well on an important test, I feel like a total success. | |
| Q14 | I believe that people can accomplish anything they want to if they have enough willpower. | ||
| Disease Prevention | Q18 | I will often pay attention to the dynamics of public health emergencies, and if there are signs of an epidemic, I will take precautions. | |
| Q19 | I only believe in the information released by the official (government, relevant medical institutions). | ||
| Q20 | I would expect the possible consequences of a public health emergency. | ||
| Q21 | I will respond after the disaster news in the media. | ||
| Q22 | I have the habit of washing hands with soap or hand sanitizer. | ||
| Q23 | I have the habit of avoiding touching my eyes and nose as much as possible in public. | ||
| Q24 | I am in ill health, and I will choose to seek medical treatment as soon as possible. | ||
| Q25 | I am very concerned about the independent use of personal items like towels, toiletries, etc. | ||
| Q26 | I have the habit of deliberately avoiding crowded places. | ||
| Dimension | No. | Question Item |
|---|---|---|
| Pessimistic Thinking | Q10 | I tend to classify people as either for me or against me. |
| Q9 | I think there are many wrong ways, but only one right way, to almost anything. | |
| Q12 | When something happens to me, I believe it is likely to be balanced by something bad. | |
| Q7 | I avoid challenges because it hurts too much when I fail. | |
| Q15 | When I am faced a new situation, I tend to think the worst possible outcome will happen. | |
| Behavioral Coping | Q26 | I have the habit of deliberately avoiding crowded places. |
| Q18 | I will often pay attention to the dynamics of public health emergencies, and if there are signs of an epidemic, I will take precautions. | |
| Q19 | I only believe in the information released by the official (government, relevant medical institutions). | |
| Q22 | I have the habit of washing hands with soap or hand sanitizer. | |
| Q23 | I have the habit of avoiding touching my eyes and nose as much as possible in public. | |
| Emotional Coping | Q8 | When faced with upcoming unpleasant events, I usually carefully think through how I will deal with them. |
| Q20 | I would expect the possible consequences of a public health emergency. | |
| Q25 | I am very concerned about the independent use of personal items like towels, toiletries, etc. | |
| Superstition Thinking | Q11 | I do not believe in any superstition. |
| Q21 | I will respond after the disaster news in the media. | |
| Optimistic Thinking | Q13 | If I do well on an important test, I feel like a total success. |
| Q16 | I tend to dwell more on pleasant than unpleasant incidents from the past. | |
| Q14 | I believe that people can accomplish anything they want to if they have enough willpower. |
| Dimension | No. | Question Item |
|---|---|---|
| Pessimistic Thinking | A1 | I tend to classify people as either for me or against me. |
| A2 | I think there are many wrong ways, but only one right way, to almost anything. | |
| A3 | When something happens to me, I believe it is likely to be balanced by something bad. | |
| A4 | I avoid challenges because it hurts too much when I fail. | |
| A5 | When I am faced a new situation, I tend to think the worst possible outcome will happen. | |
| Behavioral Coping | B1 | I will often pay attention to the dynamics of public health emergencies, and if there are signs of an epidemic, I will take precautions. |
| B2 | I only believe in the information released by the official (government, relevant medical institutions). | |
| B3 | I have the habit of avoiding touching my eyes and nose as much as possible in public. | |
| Emotional Coping | C1 | When faced with upcoming unpleasant events, I usually carefully think through how I will deal with them. |
| C2 | I would expect the possible consequences of a public health emergency. | |
| Optimistic Thinking | D1 | If I do well on an important test, I feel like a total success. |
| D2 | I believe that people can accomplish anything they want to if they have enough willpower. |
References
- Epstein, S.; Katz, L. Coping ability, stress, productive load, and symptoms. J. Personal. Soc. Psychol. 1992, 62, 813–825. [Google Scholar] [CrossRef]
- Myburgh, C.P.; Niehaus, L.; Poggenpoel, M. School and nursing service managers’ ability to hold their own amidst daily demands. Curationis 1999, 22, 36–45. [Google Scholar]
- Nicholls, A.R.; Levy, A.R.; Carson, F.; Thompson, M.A.; Perry, J.L. The applicability of self-regulation theories in sport: Goal adjustment capacities, stress appraisals, coping, and well-being among athletes. Psychol. Sport Exerc. 2016, 27, 47–55. [Google Scholar] [CrossRef]
- Ožura, A.; Šega, S. Profile of depression, experienced distress and capacity for coping with stress in multiple sclerosis patients—A different perspective. Clin. Neurol. Neurosurg. 2013, 115 (Suppl. 1), S12–S16. [Google Scholar] [CrossRef]
- Bode, C.; De Ridder, D.T.D.; Kuijer, R.G.; Bensing, J.M. Effects of an Intervention Promoting Proactive Coping Competencies in Middle and Late Adulthood. Gerontologist 2007, 47, 42–51. [Google Scholar] [CrossRef]
- Chisty, M.A.; Rahman, M. Coping capacity assessment of urban fire disaster: An exploratory study on ward no: 30 of Old Dhaka area. Int. J. Disaster Risk Reduct. 2020, 51, 101878. [Google Scholar] [CrossRef]
- Saldaña-Zorrilla, S.O. Stakeholders’ views in reducing rural vulnerability to natural disasters in Southern Mexico: Hazard exposure and coping and adaptive capacity. Glob. Environ. Chang. 2008, 18, 583–597. [Google Scholar] [CrossRef]
- Hogan, R.; Orr, F.; Fox, D.; Cummins, A.; Foureur, M. Developing nursing and midwifery students’ capacity for coping with bullying and aggression in clinical settings: Students’ evaluation of a learning resource. Nurse Educ. Pr. 2018, 29, 89–94. [Google Scholar] [CrossRef]
- McCarthy, K.M.; Tempia, S.; Kufa, T.; Kleynhans, J.; Wolter, N.; Jassat, W.; Ebonwu, J.; von Gottberg, A.; Erasmus, L.; Muchengeti, M.; et al. The importation and establishment of community transmission of SARS-CoV-2 during the first eight weeks of the South African COVID-19 epidemic. E. Clin. Med. 2021, 39, 101072. [Google Scholar]
- Rana, I.A.; Bhatti, S.S.; Aslam, A.B.; Jamshed, A.; Ahmad, J.; Shah, A.A. COVID-19 risk perception and coping mechanisms: Does gender make a difference? Int. J. Disaster Risk Reduct. 2021, 55, 102096. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Ni, Y. COVID-19 event strength, psychological safety, and avoidance coping behaviors for employees in the tourism industry. J. Hosp. Tour. Manag. 2021, 47, 431–442. [Google Scholar] [CrossRef]
- Chen, X.; Zou, Y.; Gao, H. Role of neighborhood social support in stress coping and psychological wellbeing during the COVID-19 pandemic: Evidence from Hubei, China. Heal. Place 2021, 69, 102532. [Google Scholar] [CrossRef] [PubMed]
- Her, M. Repurposing and reshaping of hospitals during the COVID-19 outbreak in South Korea. One Health 2020, 10, 100137. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Yin, P.; Xiao, L.D.; Wu, S.; Li, M.; Yang, X.; Zhang, D.; Liao, L.; Feng, H. Nursing home staff perceptions of challenges and coping strategies during COVID-19 pandemic in China. Geriatr. Nurs. 2021, 42, 887–893. [Google Scholar] [CrossRef]
- Porcher, S.; Renault, T. Social distancing beliefs and human mobility: Evidence from Twitter. PLoS ONE 2021, 16, e0246949. [Google Scholar] [CrossRef] [PubMed]
- Brodeur, A.; Clark, A.E.; Fleche, S.; Powdthavee, N. COVID-19, lockdowns and well-being: Evidence from Google Trends. J. Public Econ. 2021, 193, 104346. [Google Scholar] [CrossRef]
- Ito, M.; Seo, E.; Maeno, T.; Ogawa, R.; Maeno, T. Relationship Between Depression and Stress Coping Ability Among Residents in Japan: A Two-Year Longitudinal Study. J. Clin. Med. Res. 2018, 10, 715–721. [Google Scholar] [CrossRef]
- Chinaveh, M. The Examination of Reliability and Validity of Coping Responses Inventory Among Iranian Students. Procedia—Soc. Behav. Sci. 2013, 84, 607–614. [Google Scholar] [CrossRef][Green Version]
- Wang, T.; Yang, L.; Wu, S.; Gao, J.; Wei, B. Quantitative Assessment of Natural Disaster Coping Capacity: An Application for Typhoons. Sustainability 2020, 12, 5949. [Google Scholar] [CrossRef]
- Walkling, B.; Haworth, B.T. Flood risk perceptions and coping capacities among the retired population, with implications for risk communication: A study of residents in a north Wales coastal town, UK. Int. J. Disaster Risk Reduct. 2020, 51, 101793. [Google Scholar] [CrossRef]
- An, B.Y.; Tang, S.-Y. Lessons From COVID-19 Responses in East Asia: Institutional Infrastructure and Enduring Policy Instruments. Am. Rev. Public Adm. 2020, 50, 027507402094370. [Google Scholar] [CrossRef]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage: Newbury Park, CA, USA, 1991; p. 121. [Google Scholar]
- Epstein, S.; Meier, P. Constructive thinking: A broad coping variable with specific components. J. Personal. Soc. Psychol. 1989, 57, 332–350. [Google Scholar] [CrossRef]
- Tran, B.X.; Nguyen, H.T.; Pham, H.Q.; Le, H.T.; Vu, G.T.; Latkin, C.A.; Ho, C.S.; Ho, R.C. Capacity of local authority and community on epidemic response in Vietnam: Implication for COVID-19 preparedness. Saf. Sci. 2020, 130, 104867. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhong, Z.; Xie, J.; Ding, S.; Li, S.; Li, C. Development and psychometric assessment of the public health emergency risk perception scale: Under the outbreak of COVID-19. Int. J. Nurs. Sci. 2020, 8, 87–94. [Google Scholar] [CrossRef]
- Diamantopoulos, A.; Sarstedt, M.; Fuchs, C.; Wilczynski, P.; Kaiser, S. Guidelines for choosing between multi-item and single-item scales for construct measurement: A predictive validity perspective. J. Acad. Mark. Sci. 2012, 40, 434–449. [Google Scholar] [CrossRef]
- Byrne, D. The repression-sensitization scale: Rationale, reliability, and validity1. J. Pers. 1961, 29, 334–349. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. Reply to Shinn and Krantz. J. Heal. Soc. Behav. 1981, 22, 457. [Google Scholar] [CrossRef]
- Mirkovic, B.; Belloncle, V.; Pellerin, H.; Guilé, J.-M.; Gérardin, P. Gender Differences Related to Spirituality, Coping Skills and Risk Factors of Suicide Attempt: A Cross-Sectional Study of French Adolescent Inpatients. Front. Psychiatry 2021, 12, 1027. [Google Scholar] [CrossRef]
- Nicholls, A.R.; Polman, R.; Levy, A.; Taylor, J.; Cobley, S. Stressors, coping, and coping effectiveness: Gender, type of sport, and skill differences. J. Sports Sci. 2007, 25, 1521–1530. [Google Scholar] [CrossRef]


| Statistical Content | Sample Classification | Number | Percentage (%) | Accumulative Percentage (%) |
|---|---|---|---|---|
| Gender | Male | 71 | 43.83 | 43.83 |
| Female | 91 | 56.17 | 100.00 | |
| Age | Under 18 | 2 | 1.23 | 1.23 |
| 18~25 | 79 | 48.77 | 50.00 | |
| 26~30 | 29 | 17.90 | 67.90 | |
| 31~40 | 24 | 14.81 | 82.71 | |
| 41~50 | 16 | 9.88 | 92.59 | |
| 51~60 | 11 | 6.79 | 99.38 | |
| Over 60 | 1 | 0.62 | 100.00 | |
| Degree level | Junior high school or below | 6 | 3.70 | 3.70 |
| High school | 29 | 17.90 | 21.60 | |
| Undergraduate | 73 | 45.06 | 66.66 | |
| Master | 51 | 31.48 | 98.14 | |
| Dr | 3 | 1.85 | 100.00 |
| KMO | 0.779 | |
| Bartlett spherical test | Approximate chi-square | 956.916 |
| df | 153 | |
| Sig. | 0.000 | |
| Factor Number | Characteristic Root | Variance Explained Rate | Variance Explained Rate after Rotation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CR | VER (%) | VERAR (%) | CR | VER (%) | VERAR (%) | CR | VER (%) | VERAR (%) | |
| 1 | 4.750 | 26.391 | 26.391 | 4.750 | 26.391 | 26.391 | 2.856 | 15.868 | 15.868 |
| 2 | 2.736 | 15.202 | 41.593 | 2.736 | 15.202 | 41.593 | 2.763 | 15.348 | 31.216 |
| 3 | 1.295 | 7.197 | 48.789 | 1.295 | 7.197 | 48.789 | 1.945 | 10.804 | 42.019 |
| 4 | 1.177 | 6.539 | 55.328 | 1.177 | 6.539 | 55.328 | 1.772 | 9.845 | 51.864 |
| 5 | 1.055 | 5.860 | 61.188 | 1.055 | 5.860 | 61.188 | 1.678 | 9.324 | 61.188 |
| 6 | 0.939 | 5.215 | 66.403 | - | - | - | - | - | - |
| 7 | 0.865 | 4.805 | 71.208 | - | - | - | - | - | - |
| 8 | 0.806 | 4.477 | 75.685 | - | - | - | - | - | - |
| 9 | 0.733 | 4.069 | 79.755 | - | - | - | - | - | - |
| 10 | 0.612 | 3.398 | 83.153 | - | - | - | - | - | - |
| 11 | 0.525 | 2.917 | 86.070 | - | - | - | - | - | - |
| 12 | 0.498 | 2.766 | 88.836 | - | - | - | - | - | - |
| 13 | 0.436 | 2.422 | 91.258 | - | - | - | - | - | - |
| 14 | 0.381 | 2.115 | 93.373 | - | - | - | - | - | - |
| 15 | 0.349 | 1.937 | 95.311 | - | - | - | - | - | - |
| 16 | 0.320 | 1.778 | 97.089 | - | - | - | - | - | - |
| 17 | 0.289 | 1.608 | 98.697 | - | - | - | - | - | - |
| 18 | 0.235 | 1.303 | 100.000 | - | - | - | - | - | - |
| Item | Factor Load Coefficient | Common Degree | ||||
|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | ||
| Q10 | 0.791 | 0.674 | ||||
| Q9 | 0.728 | 0.590 | ||||
| Q12 | 0.702 | 0.675 | ||||
| Q7 | 0.692 | 0.571 | ||||
| Q15 | 0.689 | 0.637 | ||||
| Q26 | 0.749 | 0.683 | ||||
| Q18 | 0.718 | 0.691 | ||||
| Q19 | 0.703 | 0.557 | ||||
| Q22 | 0.579 | 0.554 | ||||
| Q23 | 0.538 | 0.572 | ||||
| Q8 | 0.727 | 0.602 | ||||
| Q20 | 0.581 | 0.659 | ||||
| Q25 | 0.533 | 0.562 | ||||
| Q11 | 0.779 | 0.640 | ||||
| Q21 | 0.620 | 0.655 | ||||
| Q13 | 0.729 | 0.600 | ||||
| Q16 | 0.687 | 0.660 | ||||
| Q14 | 0.542 | 0.432 | ||||
| Sample Size | Cronbach’α | Cronbach’α Based on the Standardization Project | Item Number |
|---|---|---|---|
| 162 | 0.817 | 0.821 | 18 |
| Statistical Content | Sample Classification | Number | Percentage (%) | Accumulative Percentage (%) |
|---|---|---|---|---|
| Gender | Male | 233 | 41.98 | 41.98 |
| Female | 322 | 58.02 | 100.00 | |
| Age | Under 18 | 7 | 1.26 | 1.26 |
| 18~25 | 167 | 30.09 | 31.35 | |
| 26~30 | 174 | 31.35 | 62.70 | |
| 31~40 | 152 | 27.39 | 90.09 | |
| 41~50 | 31 | 5.59 | 95.68 | |
| 51~60 | 20 | 3.60 | 99.28 | |
| Over 60 | 4 | 0.72 | 100.00 | |
| Degree level | Junior high school or below | 12 | 2.16 | 2.16 |
| High school | 57 | 10.27 | 12.43 | |
| Undergraduate | 388 | 69.91 | 82.34 | |
| Master | 88 | 15.86 | 98.20 | |
| Dr | 10 | 1.80 | 100.00 |
| Factor (Subvariable) | No. | Measurement Item (Dominant Variable) | Coef. | Std. Error | z | p | Std. Estimate |
|---|---|---|---|---|---|---|---|
| Pessimistic Thinking | A1 | I tend to classify people as either for me or against me. | 1.000 | - | - | - | 0.666 |
| A2 | I think there are many wrong ways, but only one right way, to almost anything. | 1.051 | 0.086 | 12.172 | 0.000 | 0.640 | |
| A3 | When something happens to me, I believe it is likely to be balanced by something bad. | 1.305 | 0.093 | 14.035 | 0.000 | 0.776 | |
| A4 | I avoid challenges because it hurts too much when I fail. | 1.092 | 0.085 | 12.910 | 0.000 | 0.689 | |
| A5 | When I am faced a new situation, I tend to think the worst possible outcome will happen. | 1.158 | 0.088 | 13.086 | 0.000 | 0.701 | |
| Behavioral Coping | B1 | I have the habit of deliberately avoiding crowded places. | 1.000 | - | - | - | 0.309 |
| B2 | I will often pay attention to the dynamics of public health emergencies, and if there are signs of an epidemic, I will take precautions. | 1.514 | 0.252 | 6.008 | 0.000 | 0.547 | |
| B3 | I only believe in the information released by the official (government, relevant medical institutions). | 1.387 | 0.234 | 5.936 | 0.000 | 0.524 | |
| B4 | I have the habit of washing hands with soap or hand sanitizer. | 1.413 | 0.245 | 5.761 | 0.000 | 0.477 | |
| B5 | I have the habit of avoiding touching my eyes and nose as much as possible in public. | 1.617 | 0.270 | 5.990 | 0.000 | 0.541 | |
| Emotional Coping | C1 | When faced with upcoming unpleasant events, I usually carefully think through how I will deal with them. | 1.000 | - | - | - | 0.568 |
| C2 | I would expect the possible consequences of a public health emergency. | 0.997 | 0.100 | 9.939 | 0.000 | 0.540 | |
| C3 | I am very concerned about the independent use of personal items like towels, toiletries, etc. | 0.828 | 0.090 | 9.198 | 0.000 | 0.488 | |
| Superstition Thinking | D1 | I do not believe in any superstition. | 1.000 | - | - | - | 0.473 |
| D2 | I will respond after the disaster news in the media. | 1.097 | 0.121 | 9.103 | 0.000 | 0.642 | |
| Optimistic Thinking | E1 | If I do well on an important test, I feel like a total success. | 1.000 | - | - | - | 0.569 |
| E2 | I tend to dwell more on pleasant than unpleasant incidents from the past. | 0.721 | 0.101 | 7.112 | 0.000 | 0.417 | |
| E3 | I believe that people can accomplish anything they want to if they have enough willpower. | 1.023 | 0.114 | 8.965 | 0.000 | 0.584 |
| Indicators of Fitting | χ2/df | GFI | NFI | CFI | TLI | RMSEA | |
|---|---|---|---|---|---|---|---|
| The fit value | 3.586 | 0.912 | 0.818 | 0.860 | 0.829 | 0.071 | |
| Standard value | Satisfied | <5 | >0.90 | >0.90 | >0.90 | >0.90 | <0.05 |
| Acceptable | 3~5 | 0.85~0.90 | 0.80~0.90 | 0.80~0.90 | 0.80~0.90 | 0.05~0.08 | |
| Insufficient | >5 | <0.85 | <0.80 | <0.80 | <0.80 | >0.10 | |
| Factor (Subvariable) | No. | Measurement Item (Dominant Variable) | Coef. | Std. Error | z | p | Std. Estimate |
|---|---|---|---|---|---|---|---|
| Pessimistic Thinking | A1 | I tend to classify people as either for me or against me. | 1.000 | - | - | - | 0.672 |
| A2 | I think there are many wrong ways, but only one right way, to almost anything. | 1.048 | 0.085 | 12.322 | 0.000 | 0.644 | |
| A3 | When something happens to me, I believe it is likely to be balanced by something bad. | 1.295 | 0.091 | 14.178 | 0.000 | 0.777 | |
| A4 | I avoid challenges because it hurts too much when I fail. | 1.067 | 0.083 | 12.877 | 0.000 | 0.680 | |
| A5 | When I am faced a new situation, I tend to think the worst possible outcome will happen. | 1.142 | 0.087 | 13.148 | 0.000 | 0.698 | |
| Behavioral Coping | B2 | I will often pay attention to the dynamics of public health emergencies, and if there are signs of an epidemic, I will take precautions. | 1.000 | - | - | - | 0.584 |
| B3 | I only believe in the information released by the official (government, relevant medical institutions). | 0.824 | 0.102 | 8.090 | 0.000 | 0.503 | |
| B5 | I have the habit of avoiding touching my eyes and nose as much as possible in public. | 0.938 | 0.115 | 8.136 | 0.000 | 0.508 | |
| Emotional Coping | C1 | When faced with upcoming unpleasant events, I usually carefully think through how I will deal with them. | 1.000 | - | - | - | 0.550 |
| C2 | I would expect the possible consequences of a public health emergency. | 1.111 | 0.116 | 9.606 | 0.000 | 0.582 | |
| Optimistic Thinking | E1 | If I do well on an important test, I feel like a total success. | 1.000 | - | - | - | 0.589 |
| E3 | I believe that people can accomplish anything they want to if they have enough willpower. | 0.931 | 0.112 | 8.343 | 0.000 | 0.551 |
| Indicators of Fitting | χ2/df | GFI | NFI | CFI | TLI | RMSEA | |
|---|---|---|---|---|---|---|---|
| The fit value | 3.978 | 0.940 | 0.880 | 0.907 | 0.871 | 0.076 | |
| Standard value | Satisfied | <5 | >0.90 | >0.90 | >0.90 | >0.90 | <0.05 |
| Acceptable | 3~5 | 0.85~0.90 | 0.80~0.90 | 0.80~0.90 | 0.80~0.90 | 0.05~0.08 | |
| Insufficient | >5 | <0.85 | <0.80 | <0.80 | <0.80 | >0.10 | |
| Factor | Factor | Coef. | Std.Error | z | p | Std.Estimate |
|---|---|---|---|---|---|---|
| Behavioral Coping | Pessimistic Thinking | 0.163 | 0.030 | 5.418 | 0.000 | 0.428 |
| Behavioral Coping | Emotional Coping | 0.150 | 0.032 | 4.710 | 0.000 | 0.356 |
| Behavioral Coping | Optimistic Thinking | 0.093 | 0.029 | 3.235 | 0.001 | 0.221 |
| Emotional Coping | Pessimistic Thinking | 0.278 | 0.035 | 7.931 | 0.000 | 1.004 |
| Emotional Coping | Optimistic Thinking | 0.247 | 0.034 | 7.169 | 0.000 | 0.808 |
| Optimistic Thinking | Pessimistic Thinking | 0.269 | 0.035 | 7.768 | 0.000 | 0.977 |
| Pessimistic Thinking | Behavioral Coping | Emotional Coping | Optimistic Thinking | |
|---|---|---|---|---|
| Pessimistic Thinking | 0.698 | |||
| Behavioral Coping | 0.163 | 0.532 | ||
| Emotional Coping | 0.269 | 0.520 | 0.567 | |
| Optimistic Thinking | 0.234 | 0.428 | 0.476 | 0.570 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, A.; Yang, H.; Wu, X.; Luo, X.; Gao, J. Development and Validation of the Coping Capacity Measurement Scale of Public Health Emergencies in China. Int. J. Environ. Res. Public Health 2022, 19, 94. https://doi.org/10.3390/ijerph19010094
Zhang A, Yang H, Wu X, Luo X, Gao J. Development and Validation of the Coping Capacity Measurement Scale of Public Health Emergencies in China. International Journal of Environmental Research and Public Health. 2022; 19(1):94. https://doi.org/10.3390/ijerph19010094
Chicago/Turabian StyleZhang, Ao, Hao Yang, Xiang Wu, Xiaowei Luo, and Jingqi Gao. 2022. "Development and Validation of the Coping Capacity Measurement Scale of Public Health Emergencies in China" International Journal of Environmental Research and Public Health 19, no. 1: 94. https://doi.org/10.3390/ijerph19010094
APA StyleZhang, A., Yang, H., Wu, X., Luo, X., & Gao, J. (2022). Development and Validation of the Coping Capacity Measurement Scale of Public Health Emergencies in China. International Journal of Environmental Research and Public Health, 19(1), 94. https://doi.org/10.3390/ijerph19010094