
Digital Health Interventions by Clinical Pharmacists: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
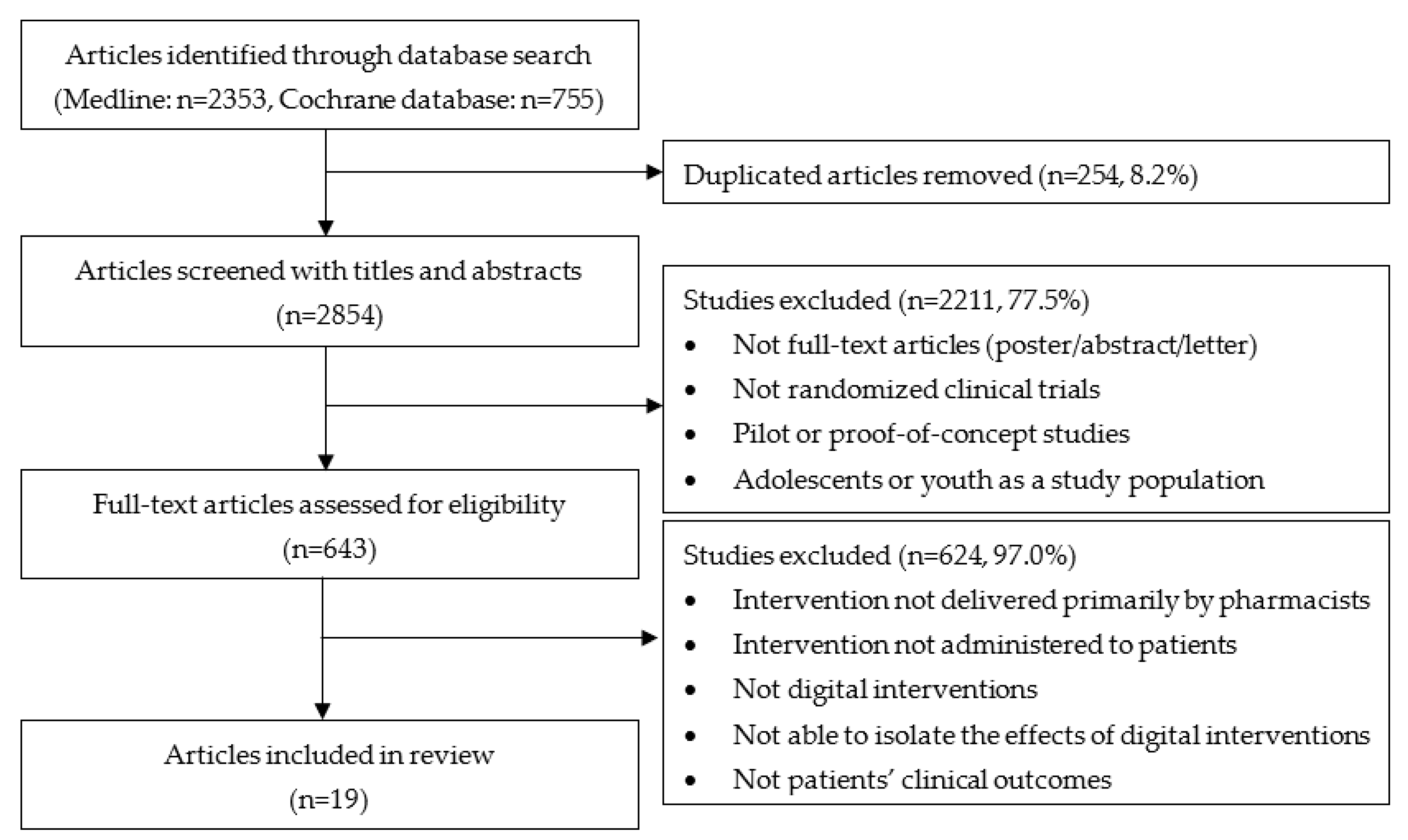
2.2. Selection Process and Inclusion/Exclusion Criteria
3. Results
3.1. Telephone-Based Intervention
3.2. Web-Based Intervention
3.3. Mobile-Based Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheth, N.; Kane, Y.I. Smart-phone makers call the doctor. Wall Str. J. 2009. Available online: https://www.wsj.com/articles/SB125487806705169673 (accessed on 6 September 2021).
- Page, D. Technology: Cell phones are quickly becoming cutting-edge medical devices. Hosp. Health Netw. 2008, 82, 13. [Google Scholar] [PubMed]
- Hardy, K. Physicians Network Uses Wireless IT to Improve Home-Based Care. Healthcare IT News. Available online: https://www.healthcareitnews.com/news/physicians-network-uses-wireless-it-improve-home-based-care (accessed on 10 September 2021).
- Putzer, G.J.; Park, Y. Are physicians likely to adopt emerging mobile technologies? Attitudes and innovation factors affecting smartphone use in the Southeastern United States. Perspect. Health Inf. Manag. 2012, 9, 1–22. [Google Scholar]
- Wallace, S.; Clark, M.; White, J. ‘It’s on my iPhone’: Attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open 2012, 2, e001099. [Google Scholar] [CrossRef] [Green Version]
- Bevilacqua, R.; Casaccia, S.; Cortellessa, G.; Astell, A.; Lattanzio, F.; Corsonello, A.; D’Ascoli, P.; Paolini, S.; Di Rosa, M.; Rossi, L.; et al. Coaching through technology: A systematic review into efficacy and effectiveness for the ageing population. Int. J. Environ. Res. Public Health 2020, 17, 5930. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Strano, S.; Di Rosa, M.; Giammarchi, C.; Cerna, K.K.; Mueller, C.; Maranesi, E. eHealth literacy: From theory to clinical application for digital health improvement. Results from the ACCESS training experience. Int. J. Environ. Res. Public Health 2021, 18, 11800. [Google Scholar] [CrossRef] [PubMed]
- Aungst, T.D. Medical applications for pharmacists using mobile devices. Ann. Pharmacother. 2013, 47, 1088–1095. [Google Scholar] [CrossRef]
- Dasgupta, A.; Sansgiry, S.S.; Sherer, J.T.; Wallace, D.; Sikri, S. Pharmacists’ utilization and interest in usage of personal digital assistants in their professional responsibilities. Health Info. Libr. J. 2010, 27, 37–45. [Google Scholar] [CrossRef]
- Dasgupta, A.; Sansgiry, S.S.; Sherer, J.T.; Wallace, D.; Sikri, S. Application of the extended technology acceptance model in predicting pharmacists’ intention to use personal digital assistants. J. Am. Pharm. Assoc. 2009, 49, 792–798a. [Google Scholar] [CrossRef]
- Fox, B.I.; Felkey, B.G.; Berger, B.A.; Krueger, K.P.; Rainer, R.K., Jr. Use of personal digital assistants for documentation of pharmacists’ interventions: A literature review. Am. J. Health Syst. Pharm. 2007, 64, 1516–1525. [Google Scholar] [CrossRef]
- Felkey, B.; Fox, B.I. Emerging technology at the point of care. J. Am. Pharm. Assoc. 2003, 43 (Suppl. S1), S50–S51. [Google Scholar]
- ScriptPro Telepharmacy Website. Available online: https://www.scriptpro.com (accessed on 1 October 2021).
- Crilly, P.; Kayyali, R. A systematic review of randomized controlled trials of telehealth and digital technology use by community pharmacists to improve public health. Pharmacy 2020, 8, 137. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldfien, R.; Pressman, A.; Jacobson, A.; Ng, M.; Avins, A. A pharmacist-staffed, virtual gout management clinic for achieving target serum uric acid levels: A randomized clinical trial. Perm. J. 2016, 20. [Google Scholar] [CrossRef] [Green Version]
- Huiskes, V.J.B.; van den Ende, C.H.M.; Kruijtbosch, M.; Ensing, H.T.; Meijs, M.; Meijs, V.M.M.; Burger, D.M.; van den Bemt, B.J.F. Effectiveness of medication review on the number of drug-related problems in patients visiting the outpatient cardiology clinic: A randomized controlled trial. Br. J. Clin. Pharmacol. 2020, 86, 50–61. [Google Scholar] [CrossRef]
- Wu, J.Y.; Leung, W.Y.; Chang, S.; Lee, B.; Zee, B.; Tong, P.C.; Chan, J.C. Effectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy: Randomised controlled trial. BMJ 2006, 333, 522. [Google Scholar] [CrossRef] [Green Version]
- Margolis, K.L.; Asche, S.E.; Bergdall, A.R.; Dehmer, S.P.; Groen, S.E.; Kadrmas, H.M.; Kerby, T.J.; Klotzle, K.J.; Maciosek, M.V.; Michels, R.D.; et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control: A cluster randomized clinical trial. JAMA 2013, 310, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Sudas Na Ayutthaya, N.; Sakunrak, I.; Dhippayom, T. Clinical outcomes of telemonitoring for patients on warfarin after discharge from hospital. Int. J. Telemed. Appl. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.; Cymbala, A.A.; Delate, T.; Kurz, D.; Olson, K.L.; Youngblood, M.; Zadvorny, E. Cluster-randomized trial of clinical pharmacist tobacco cessation counseling among patients with cardiovascular disease. Popul. Health Manag. 2015, 18, 300–306. [Google Scholar] [CrossRef]
- Eldeib, H.K.; Abbassi, M.M.; Hussein, M.M.; Salem, S.E.; Sabry, N.A. The Effect of telephone-based follow-up on adherence, efficacy, and toxicity of oral capecitabine-based chemotherapy. Telemed. E-Health 2019, 25, 462–470. [Google Scholar] [CrossRef]
- Lauffenburger, J.C.; Ghazinouri, R.; Jan, S.; Makanji, S.; Ferro, C.A.; Lewey, J.; Wittbrodt, E.; Lee, J.; Haff, N.; Fontanet, C.P.; et al. Impact of a novel pharmacist-delivered behavioral intervention for patients with poorly-controlled diabetes: The ENhancing outcomes through Goal Assessment and Generating Engagement in Diabetes Mellitus (ENGAGE-DM) pragmatic randomized trial. PLoS ONE 2019, 14, e0214754. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Ockene, I.S.; Rosal, M.C.; Merriam, P.A.; Ockene, J.K.; Gandhi, P.J. Randomized trial of a pharmacist-delivered intervention for improving lipid-lowering medication adherence among patients with coronary heart disease. Cholesterol 2010, 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmany, S.S.; Ratrout, L.; Amireh, A.; Agha, R.; Nassar, N.; Mahmoud, N.; Rimawi, D.; Nazer, L. The impact of pharmacist telephone calls after discharge on satisfaction of oncology patients: A randomized controlled study. J. Oncol. Pharm. Pract. 2018, 24, 359–364. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Olsen, M.K.; McCant, F.; Stechuchak, K.M.; Danus, S.; Crowley, M.J.; Goldstein, K.M.; Zullig, L.L.; Oddone, E.Z. Telemedicine cardiovascular risk reduction in veterans: The CITIES trial. Am. Heart J. 2018, 199, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.L.; Levy, B.; Gryzlak, B.; Xu, Y.; Chrischilles, E.; Dawson, J.; Weg, M.V.; Christensen, A.; James, P.; Polgreen, L. Cluster-randomized trial to evaluate a centralized clinical pharmacy service in private family medicine offices. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004188. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Isaac, T.; Lauffenburger, J.C.; Gopalakrishnan, C.; Lee, M.; Vachon, A.; Iliadis, T.L.; Hollands, W.; Elman, S.; Kraft, J.M.; et al. Effect of a remotely delivered tailored multicomponent approach to enhance medication taking for patients with hyperlipidemia, hypertension, and diabetes: The STIC2IT cluster randomized clinical trial. JAMA Intern. Med. 2018, 178, 1182–1189. [Google Scholar] [CrossRef] [Green Version]
- Gernant, S.A.; Snyder, M.E.; Jaynes, H.; Sutherland, J.M.; Zillich, A.J. The effectiveness of pharmacist-provided telephonic medication therapy management on emergency department utilization in home health patients. J. Pharm. Technol. 2016, 32, 179–184. [Google Scholar] [CrossRef]
- Zillich, A.J.; Snyder, M.E.; Frail, C.K.; Lewis, J.L.; Deshotels, D.; Dunham, P.; Jaynes, H.A.; Sutherland, J.M. A randomized, controlled pragmatic trial of telephonic medication therapy management to reduce hospitalization in home health patients. Health Serv. Res. 2014, 49, 1537–1554. [Google Scholar] [CrossRef]
- Green, B.B.; Cook, A.J.; Ralston, J.D.; Fishman, P.A.; Catz, S.L.; Carlson, J.; Carrell, D.; Tyll, L.; Larson, E.B.; Thompson, R.S. Effectiveness of home blood pressure monitoring, Web communication, and pharmacist care on hypertension control: A randomized controlled trial. JAMA 2008, 299, 2857–2867. [Google Scholar] [CrossRef] [Green Version]
- Magid, D.J.; Olson, K.L.; Billups, S.J.; Wagner, N.M.; Lyons, E.E.; Kroner, B.A. A pharmacist-led, American Heart Association Heart360 Web-enabled home blood pressure monitoring program. Circ. Cardiovasc. 2013, 6, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Gonzales, H.M.; Fleming, J.N.; Gebregziabher, M.; Posadas-Salas, M.A.; Su, Z.; McGillicuddy, J.W.; Taber, D.J. Pharmacist-led mobile health intervention and transplant medication safety: A randomized controlled clinical trial. Clin. J. Am. Soc. Nephrol. 2021, 16, 776–784. [Google Scholar] [CrossRef]
- Fleming, J.N.; Gebregziabher, M.; Posadas, A.; Su, Z.; McGillicuddy, J.W.; Taber, D.J. Impact of a pharmacist-led, mHealth-based intervention on tacrolimus trough variability in kidney transplant recipients: A report from the TRANSAFE Rx randomized controlled trial. Am. J. Health Syst. Pharm. 2021. [Google Scholar] [CrossRef]
- Kosse, R.C.; Bouvy, M.L.; de Vries, T.W.; Koster, E.S. Effect of a mHealth intervention on adherence in adolescents with asthma: A randomized controlled trial. Respir. Med. 2019, 149, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Crilly, P.; Jair, S.; Mahmood, Z.; Moin Khan, A.; Munir, A.; Osei-Bediako, I.; Samir, M.; Kayyali, R. Public views of different sources of health advice: Pharmacists, social media and mobile health applications. Int. J. Pharm. Pract. 2019, 27, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyne, J.M.; Fortney, J.C.; Tripathi, S.P.; Maciejewski, M.L.; Edlund, M.J.; Williams, D.K. Cost-effectiveness analysis of a rural telemedicine collaborative care intervention for depression. Arch. Gen. Psychiatry 2010, 67, 812–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Painter, J.T.; Fortney, J.C.; Austen, M.A.; Pyne, J.M. Cost-effectiveness of telemedicine-based collaborative care for posttraumatic stress disorder. Psychiatr. Serv. 2017, 68, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Avery, A.J.; Rodgers, S.; Cantrill, J.A.; Armstrong, S.; Cresswell, K.; Eden, M.; Elliott, R.A.; Howard, R.; Kendrick, D.; Morris, C.J.; et al. A pharmacist-led information technology intervention for medication errors (PINCER): A multicentre, cluster randomised, controlled trial and cost-effectiveness analysis. Lancet 2012, 379, 1310–1319. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author (Year) | Setting (Duration and Location) | Subject | Intervention (n, Mean Age, %Female) | Control (n, Mean Age, %Female) | Outcomes | Result | Risk of Bias Using the Jaded/PEDro Scales |
|---|---|---|---|---|---|---|---|
| Telephone-based intervention | |||||||
| Adams et al. (2015) [22] | Three months, privately insured population in the U.S. | Tobacco users who were enrolled in Clinical Pharmacy Cardiac Risk Service (CPCRS) | Telephone-based counseling (n = 64, 66.6, 43.8%) | Usual care (n = 56, 64.6, 28.6%) | Primary: Proportion of individuals who reported a tobacco cessation attempt during follow-up Secondary: Proportion of individuals who had (1) at least one contact with a phone counseling service; (2) purchased at least one tobacco cessation medication aid; and (3) attended at least one tobacco cessation program or webinar | Primary: No significant difference in tobacco cessation attempt between the treatment and the control groups (38.6% vs. 36.2%, p = 0.804) Secondary: No significant difference between the two groups in the proportion of individuals who had (1) at least one contact with a phone counseling service (0.0% vs. 5.4%, p = 0.099); (2) purchased at least one tobacco cessation medication aid (10.9% vs. 19.6%, p = 0.183); and (3) attended at least one tobacco cessation program or webinar (1.6% vs. 0.0%, p = 0.348) | Low/Low |
| Bosworth et al. (2018) [27] | 12 months, a veterans’ medical center in the U.S. | Patients with hypertension and/or hypercholesterolemia | Telehealth intervention by clinical pharmacist specialists (n = 215, 60.9, 15.3%) | Educational control (n = 213, 61.5, 15.0%) | Primary: Framingham cardiovascular disease (CVD) risk score at 6 and 12 months Secondary: systolic blood pressure (sBP), diastolic blood pressure (dBP), total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), body mass index (BMI), HbA1c (for those w/diabetes) at 6 and 12 months | Primary: No significant differences in Framingham CVD risk score, sBP, dBP, LDL, HDL, BMI, HbA1c at 6 or 12 months and total cholesterol at 12 months Secondary: Significant decline in total cholesterol at 6 months in the treatment group compared to the control group (difference: −7.0, 95%CI: −13.4 to −0.6, p = 0.03) | Moderate/Moderate |
| Carter et al. (2018) [28] | 12 months, physician offices and health centers in the U.S. | Patients with diabetes or hypertension | Telephone-based medication therapy management (MTM) (n = 149, 63.7, 46.3%) | Usual care (n = 153, 64.1, 52.9%) | Primary: Adherence to the American Heart Association (AHA)’s guideline developed for individuals with CV conditions Secondary: Changes in key CV risk factors such as blood pressure, HbA1c, and lipids | Primary: Significant improvement in adherence to the guideline only in the treatment group (p = 0.02) Secondary: No significant differences in the secondary outcomes between the treatment group and the control group (p-values ranging from 0.06 to 0.73) | Moderate/Moderate |
| Choudhry (2018) a [29] | 12 months, primary care practice sites in the U.S. | Patients with hyperlipidemia, hypertension, and diabetes | Telephone-based consultation (n = 2038, 60.4, 45.3%) | Usual care (n = 2040, 59.2, 45.0%) | Primary: Medication adherence measured by proportion of days covered (PDC) Secondary: (1) Disease control based on achieved levels of LDL, sBP, and HBA1c for at least one condition and all conditions as well as (2) healthcare service use | Primary: Significantly higher improvement in medication adherence in the treatment group compared to the control group (difference = 4.7%, 95% CI: 3.0–6.4%) Secondary: No significant difference between the two groups in (1) achieving disease control for at least one condition (OR = 1.10, 95% CI:0.94–1.28) and all conditions (OR = 1.05, 95% CI: 0.91–1.22) as well as (2) hospitalization (OR = 1.02, 95% CI: 0.78–1.34) and physician office visits (OR = 1.11, 95% CI: 0.91–1.36) Significantly fewer emergency department visits in the treatment group compared to the control group (OR = 0.62, 95% CI: 0.45–0.85) | Low/Low |
| Eldeib et al. (2018) b [23] | 12 months, National Cancer Institute in Egypt | Patients with metastatic colorectal or gastric cancer | Follow-up telephone call during the treatment cycles (i.e., from cycle 1 to cycle 12) (n= 44, 50.0, 63.6%) | Standard care (n = 38, 44.8, 63.2%) | Primary: Medication adherence measured by the pill count method Secondary: Overall survival (OS) and progression-free survival (PFS) | Primary: No significant difference in medication adherence between the treatment group and the control group for all cycles (98.99% vs. 96.83%, p = 0.354) except for the 11th cycle (100% vs. 92.86%, p = 0.046) Secondary: No significant difference between the two groups in the median OS (10.13 in the treatment group vs. 8.10 in the control group, p = 0.84) and the median PFS (5.20 in the treatment group vs. 6.13 in the control group, p = 0.48) | Moderate/Moderate |
| Gernant et al. (2016) [30] | Two months, home health population in the U.S. | Medicare-insured patients admitted to the home health agencies (HHAs) | Telephone-based MTM (n = 297, 71, 58%) | Usual nursing care (n = 359, 73, 61%) | 60-day all-cause emergency department (ED) utilization | No significant difference in 60-day ED utilization (24.4% in the treatment group vs. 25.1% in the control group, 95% CI: 0.79–1.57) However, significantly lower ED utilization among patients in the lowest risk quartile for the treatment group (OR = 2.52, 95% CI: 1.15–5.49, p = 0.02) | Low/Low |
| Goldfien et al. (2016) [17] | Six months, Kaiser Permanent Northern California patient population in USA | Patients with gout | Telephone-based program (n = 37, 60.9, 2.7%) | Usual care (n = 40, 58.0, 20.0%) | Primary: Achievement of a serum uric acid (sUA) level of 6.0 mg/dL or below Secondary: Mean change in sUA levels | Primary: Higher percent of achievement of sUA level at or below 6.0 mg/dL in the treatment group compared to the control group (35% vs. 13%, p = 0.03) Secondary: Significant change in mean sUA levels in the treatment group compared to the control group (−1.5 mg/dL vs. 0.1 mg/dL, p < 0.001) | Moderate/Moderate |
| Huiskes et al. (2019) [18] | One month, hospitals in the Netherlands | Patients visiting outpatient cardiology clinics | Telephone call (n = 90, 65.8, 44.4%) | Usual care (n = 85, 66.2, 37.6%) | Number of drug-related problems (DRPs) one month after visiting the cardiologist | Significant reduction in the number of DRPs in the treatment group compared to the control group (0.3 vs. 0.8, p < 0.001) | Moderate/Moderate |
| Lauffenburger et al. (2019) c [24] | 12 months, privately insured population in the U.S. | Patients with diabetes | Telephone-based consultation (n = 700, 54.9, 34.6%) | Usual care (n = 700, 54.6, 39.8%) | Primary: Change in HbA1c from baseline Secondary: (1) Proportion of patients achieving HbA1c < 8%, and (2) medication adherence measured by PDC | Primary: No significant difference in HbA1c change between the two groups (difference = 0.06, 95% CI: −0.20 to 0.32) Secondary: (1) No significant difference in the proportion of those achieving HbA1c < 8% between the two groups (OR = 0.91, 95% CI: 0.71–1.17) (2) No significant difference in medication adherence between the two groups (OR = 0.92, 95% CI: 0.72–1.17) | Low/Low |
| Ma et al. (2010) [25] | 12 months, medical center in the U.S. | Patients with coronary heart disease (CHD) | Telephone-based counseling (n = 351, 60.4, 40.2%) | Usual care (n = 338, 60.3, 40.2%) | Primary: Percent of patients with a serum LDL-C <100 mg/dL Secondary: Proportion of adherence to statin medication | Primary: No significant difference in the percent of individuals with LDL-C <100 mg/dL between the treatment and control groups (65% vs. 60%, p = 0.29) Secondary: No significant difference in adherence to statin in the two groups (0.88 vs. 0.90, p = 0.51) | Moderate/Low |
| Margolis et al. (2013) d [20] | Six to eighteen months, primary care clinics in the U.S. | Patients with hypertension | Telemonitoring (n = 228, 62.0, 45.2%) | Usual care (n = 222, 60.2, 44.1%) | Primary: Control of BP (sBP < 140 mmHg and dBP < 90 mmHg) at 6 and 12 months Secondary: BP control and change in BP at 18 months | Primary: Significant improvement in BP control in the treatment group compared to the control group at 6 or 12 months (all p-values < 0.001) Secondary: Significant improvement in the treatment group in BP control (p = 0.003) and sBP (p = 0.004), but marginally insignificant in dBP (p = 0.07) at 18 months | Low/Low |
| Salmany et al. (2017) [26] | One month, cancer center in the U.S. | Patients with cancer who were discharged from inpatient services | Follow-up telephone call after hospital discharge (n = 166, 47.2, 54.3%) | No follow-up call (n = 166, 49.2, 52.4%) | ED visits and readmission to hospital within 30 days of discharge | No significant differences between the treatment group and the control groups in ED visit (44% vs. 52%, p = 0.123) and hospital readmission (37% vs. 43%, p = 0.317) within 30 days of discharge | Low/Low |
| Sudas Na Ayutthaya et al. (2018) [21] | Three months, hospital in Thailand | Patients prescribed warfarin upon discharge | Telephone call (n = 25, 56.6, 72%) | Standard pharmacy services (n = 25, 58.7, 48%) | (1) Proportion of international normalized ratio (INR) values in range, (2) proportion of INR out of range, (3) percent of patients with one or more out-of-range INR values, and (4) time in therapeutic range (TTR) | (1) Significantly higher proportion of INR values in range in the treatment group compared to the control group (45.6% vs. 24.1%, p = 0.005) (2) Significantly lower proportion of INR out of range in the treatment group compared to the control group (11.4% vs. 24.1%, p = 0.037) (3) Significantly lower percent of those with one or more out-of-range INR values in the treatment group compared to the control group (84% vs. 100%, p = 0.037) (4) Significantly higher mean TTR in the treatment group compared to the control group (49.8 vs. 28.0, p = 0.017) | Moderate/Low |
| Wu et al. (2006) [19] | Three months, hospital in Hong Kong | Clinically stable patients with prescription of five or more drugs on at least two consecutive visits to clinic | Telephone call midpoint between the two clinic visits (n = 219, 71.2, 51.0%) | No telephone call(n = 223, 70.5, 52.0%) | All-cause mortality | Significant reduction in mortality in the treatment group compared to the control group (relative risk = 0.59, 95% CI: 0.35–0.97, p = 0.039) | Low/Low |
| Zillich et al. (2014) [31] | Two months, home healthcare centers in the U.S. | Medicare-insured home healthcare patients | Telephone-based MTM (n = 415, 73, 58%) | Usual home healthcare (n = 480, 73, 62%) | Primary: 60-day all-cause hospitalization Secondary: 30-day all-cause hospitalization | Primary: No significant difference in 60-day all-cause hospitalization between the two groups (p = 0.19) However, significant lower 60-day hospitalization in the lowest baseline risk quartile for the treatment group (p = 0.01) Secondary: No significant difference in 30-day all-cause hospitalization between the two groups (p = 0.30) However, significant lower 30-day hospitalization in the lowest risk quartile for the treatment group (p = 0.01) | Low/Low |
| Web-based intervention | |||||||
| Green et al. (2008) [32] | 12 months, medical centers in the U.S. | Patients with hypertension alone (no diagnosis of diabetes, CV or renal disease, or other serious conditions) | Web-based communications with a pharmacist and home BP monitoring and access to patient web services (n = 261, 59.3, 55.9%) | CTRL 1: Home BP monitoring and access to patient web services (n = 259, 59.5, 45.9%)CTRL 2: Usual care(n = 258, 58.6, 54.7%) | Primary: Changes in sBP, dBP, and the percent of patients with controlled BP (<140/90 mmHg) Secondary: Changes in the number of antihypertensive medications, aspirin use, and BMI | Primary: Significant improvement in changes in sBP, dBP, and the percent with controlled BP in the treatment group compared to the control groups (all p-values < 0.001) Secondary: Significantly more reductions in the number of antihypertensive agents and aspirin use in the treatment group compared to the control groups (all p-values < 0.05) However, no significant difference in BMI change between the treatment group and the control groups (difference: −0.9, 95% CI: −2.1 to 0.3) | Low/Low |
| Magid et al. (2013) [33] | Six months, privately insured population in the U.S. | Patients with hypertension | Web-based blood pressure monitoring and education (n = 175, 60.0, 38.3%) | Usual care (n = 173, 59.1, 41.0%) | Primary: Proportion of patients who attained their goal BP Secondary: Changes in sBP, dBP, antihypertensive medication intensity, and antihypertensive medication adherence measured by medication possession ratio (MPR) | Primary: Significantly higher proportion of patients achieving BP goal in the treatment group compared to the control group (RR = 1.5, 95% CI: 1.2–1.9) Secondary: Significantly higher changes in sBP, dBP, and antihypertensive medication intensity in the treatment group (all p-values < 0.01) No significant difference in MPR between the two groups (0.86 in the treatment group vs. 0.87 in the control group, p = 0.98) | Low/Low |
| Mobile-based intervention | |||||||
| Fleming et al. (2021) [35] | 12 months, university medical center in the U.S. | Kidney transplant recipients | Mobile application for monitoring and managing medication therapy (n = 68, 50.2, 48.5%) | Usual care (n = 68, 51.2, 38.2%) | Intrapatient variability (IPV) | Significant decrease in tacrolimus IPV in the treatment group compared to control group (p = 0.01) | Moderate/Low |
| Gonzales et al. (2021) [34] | 12 months, university medical center in the U.S. | Kidney transplant recipients | Mobile application for monitoring and managing medication therapy (n = 68, 50, 49%) | Usual care (n = 68, 51, 38%) | Primary: Incidence and severity of medication errors and adverse events (AEs) Secondary: Infections and hospitalizations | Primary: Significant reduction in medication errors in the treatment group compared to the control group (incidence risk ratio (IRR) = 0.39, 95% CI: 0.28–0.55) No significant difference in incidence of grade 1 or grade 2 AEs between the two groups, but a significantly lower incidence of grade 3 or higher AEs in the treatment group (IRR = 0.55, 95% CI: 0.30–0.99) Secondary: No significant difference in infection rates between the two groups, but a significantly lower rate of hospitalizations in the treatment group (IRR = 0.46, 95% CI: 0.27–0.77) | Low/Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, T.; Muzumdar, J.; Kim, H. Digital Health Interventions by Clinical Pharmacists: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 532. https://doi.org/10.3390/ijerph19010532
Park T, Muzumdar J, Kim H. Digital Health Interventions by Clinical Pharmacists: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(1):532. https://doi.org/10.3390/ijerph19010532
Chicago/Turabian StylePark, Taehwan, Jagannath Muzumdar, and Hyemin Kim. 2022. "Digital Health Interventions by Clinical Pharmacists: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 1: 532. https://doi.org/10.3390/ijerph19010532
APA StylePark, T., Muzumdar, J., & Kim, H. (2022). Digital Health Interventions by Clinical Pharmacists: A Systematic Review. International Journal of Environmental Research and Public Health, 19(1), 532. https://doi.org/10.3390/ijerph19010532