
Internet-Related Disorders and Their Effects on Personality Development in Adolescents from Germany—Results from a Prospective Study


 ,
, 
Abstract
:1. Introduction
- (1)
- According to previous findings, we expect that personality will generally be prone to changes in our sample of adolescents. However, since we are looking at a short time period, we expect changes to be of small effects sizes.
- (2)
- Derived from previous findings on trait-pathology-associations, we expect that the development of personality traits will be influenced by IRD. Thus, following recommendations of Durbin and Hicks [27], personality traits are addressed as dependent variables. As this has not been investigated before for IRD, it is difficult to provide specific hypotheses. However, taking the findings of Hicks et al. [28] into account, we expect increases in neuroticism and decreases in extraversion and conscientiousness among adolescents with IRD.
- (3)
- As an additional and exploratory approach, we also investigated personality as moderating factors. Derived from prior results of cross-sectional studies [24], we suppose that changes in neuroticism and conscientiousness will affect the stability of IRD- symptoms over one year.
- (4)
- Based on findings from cross-sectional studies [24], we expect that personality traits, particularly high neuroticism and low conscientiousness at baseline will be predictive of IRD one year later.
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Classification of Symptom-Groups
2.4. Statistical Analyses
3. Results
3.1. Personality as a Predictor and a Moderator of Internet-Related Disorders
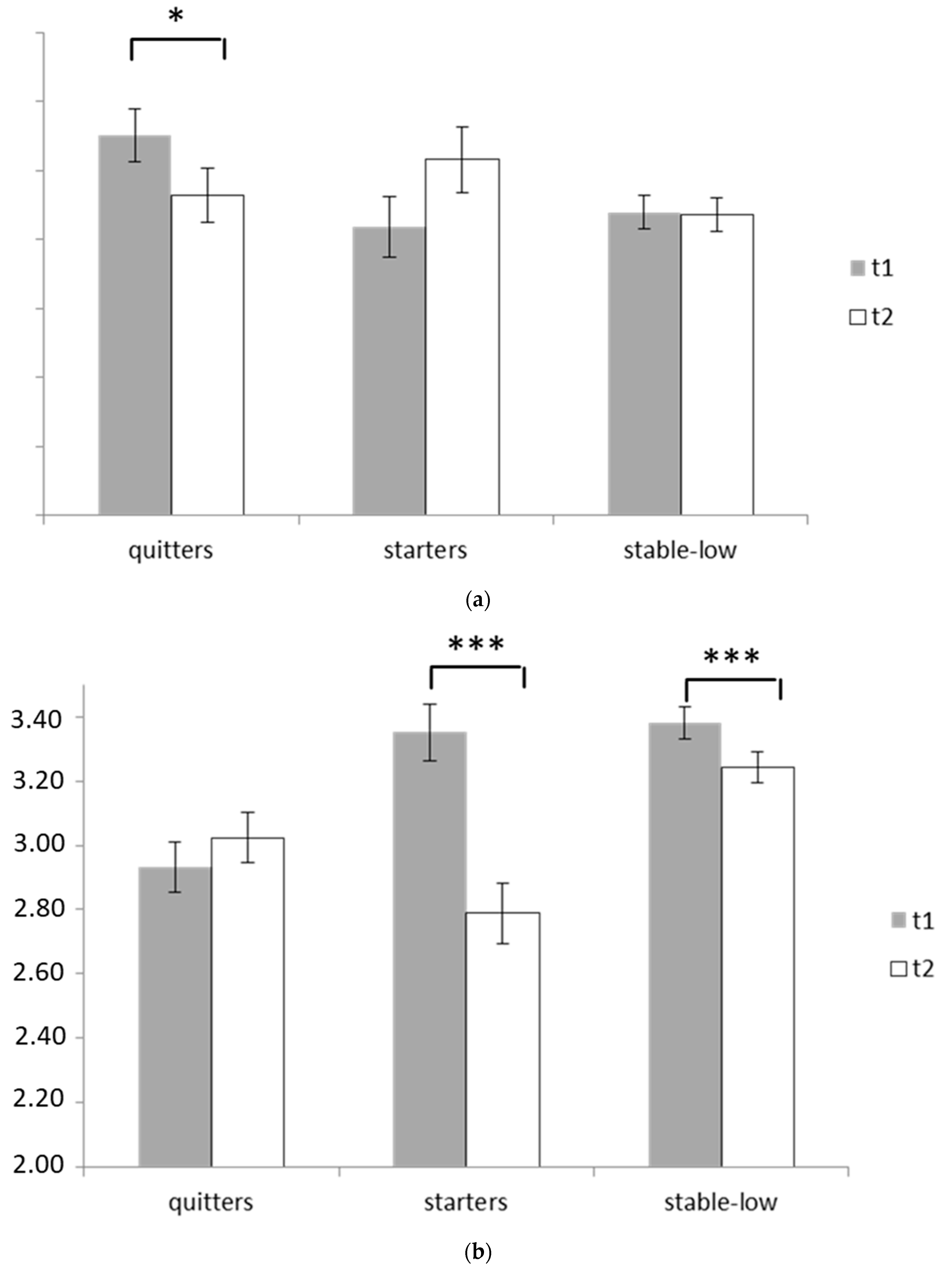
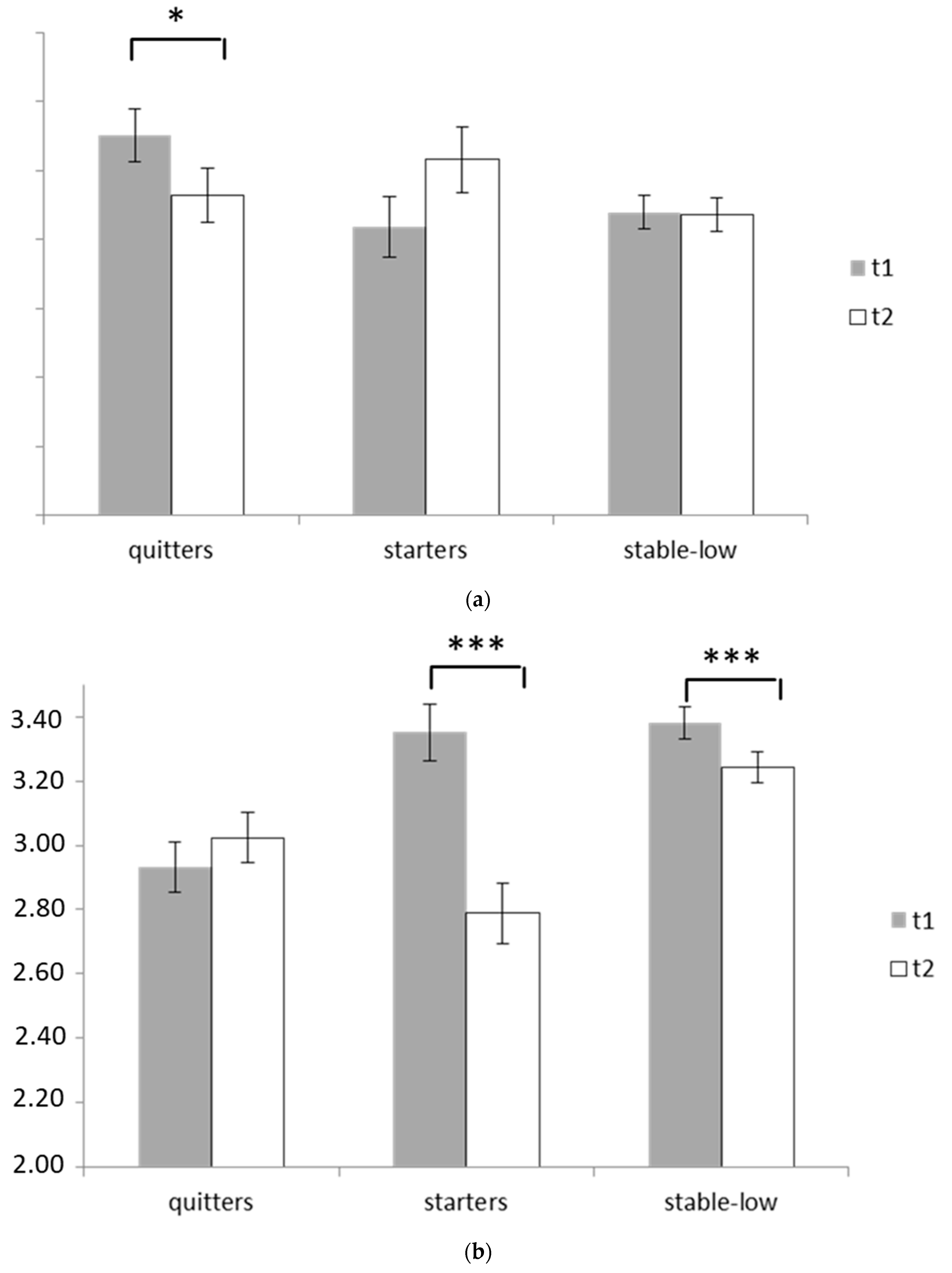
3.2. Mean-Level Changes of Personality and Their Dependence on Symptoms of Internet-Related Disorders
4. Discussion
- (1)
- We found a general, yet slight development of personality traits among adolescents over the course of one year
- (2)
- Adolescents with IRD displayed different patterns in personality development compared to adolescents without IRD. Small to moderate effect sizes were found particularly for differential developmental paths of conscientiousness and neuroticism. Moreover, the changes in personality were partly associated with the stability of IRD-symptoms over the time.
- (3)
- The moderated regression analyses further showed that openness and conscientiousness influenced the probability of displaying IRD-symptoms one year later. Thus, these traits can be perceived as important moderating variables.
- (4)
- Finally, conscientiousness at baseline was revealed to be a direct predictor of IRD-symptoms one year later and thus might be understood as a risk factor.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Schulenberg, J.E.; Sameroff, A.J.; Cicchetti, D. The transition to adulthood as a critical juncture in the course of psychopathology and mental health. Dev. Psychopathol. 2004, 16, 799–806. [Google Scholar] [CrossRef] [Green Version]
- Cicchetti, D.; Rogosch, F.A. A developmental psychopathology perspective on adolescence. J. Consult. Clin. Psychol. 2002, 70, 6–20. [Google Scholar] [CrossRef]
- Moffitt, T.E. Life-course-persistent and adolescence-limited antisocial behavior: A 10-year research review and a research agenda. In Causes of Conduct Disorder and Juvenile Delinquency; Lahey, B.B., Moffitt, T.E., Caspi, A., Eds.; The Guilford Press: New York, NY, USA, 2003; pp. 49–75. [Google Scholar]
- Griffiths, M.; Van Rooij, A.J.; Kardefeldt-Winther, D.; Starcevic, V.; Király, O.; Pallesen, S.; Müller, K.W.; Dreier, M.; Carras, M.; Prause, N.; et al. Working towards an international consensus on criteria for assessing Internet Gaming Disorder: A critical commentary on Petry et al. (2014). Addiction 2016, 111, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.; Rehbein, F.; Gentile, D.A.; Lemmens, J.S.; Rumpf, H.J.; Mößle, T.; Bischof, G.; Tao, R.; Fung, D.S.S.; Borges, G.; et al. An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction 2014, 109, 1399–1406. [Google Scholar] [CrossRef]
- Kuss, D.J.; Griffiths, M.D.; Pontes, H.M. Chaos and confusion in DSM-5 diagnosis of Internet Gaming Disorder: Issues, concerns, and recommendations for clarity in the field. J. Behav. Addict. 2017, 6, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Pawlikowski, M.; Nader, I.W.; Burger, C.; Stieger, S.; Brand, M. Pathological Internet use–It is a multidimensional and not a unidimensional construct. Addict. Res. Theory 2014, 22, 166–175. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The ICD-11 Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Müller, K.W.; Beutel, M.E.; Dreier, M.; Wölfling, K. A clinical evaluation of the DSM-5 criteria for Internet Gaming Disorder and a pilot study on their applicability to further internet-related disorders. J. Behav. Addict. 2019, 8, 16–24. [Google Scholar] [CrossRef]
- Wartberg, L.; Zieglmeier, M.; Kammerl, R. An Empirical Exploration of Longitudinal Predictors for Problematic Internet Use and Problematic Gaming Behavior. Psychol. Rep. 2021. [Google Scholar] [CrossRef]
- Fineberg, N.A.; Demetrovics, Z.; Stein, D.J.; Ioannidis, K.; Potenza, M.N.; Grünblatt, E.; Brand, M.; Billieux, J.; Carmi, L.; King, D.L.; et al. Manifesto for a European research network into Problematic Usage of the Internet. Eur. Neuropsychopharmacol. 2018, 28, 1232–1246. [Google Scholar] [CrossRef]
- Müller, K.W.; Janikian, M.; Dreier, M.; Wölfling, K.; Beutel, M.E.; Tzavara, C.; Richardson, C.; Tsitsika, A. Regular gaming behavior and Internet Gaming Disorder in European adolescents: Results from a cross-national representative survey of prevalence, predictors and psychopathological correlates. Eur. Child Adolesc. Psychiatry 2015, 24, 565–574. [Google Scholar] [CrossRef]
- Cheng, C.; Li, A.Y.L. Internet addiction prevalence and quality of (real) life: A meta-analysis of 31 nations across seven world regions. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 755–760. [Google Scholar] [CrossRef] [Green Version]
- Wartberg, L.; Kriston, L.; Zieglmeier, M.; Lincoln, T.; Kammerl, R. A longitudinal study on psychosocial causes and consequences of Internet gaming disorder in adolescence. Psychol. Med. 2019, 49, 287–294. [Google Scholar] [CrossRef]
- Brand, M.; Wegmann, E.; Stark, R.; Müller, A.; Wölfling, K.; Robbins, T.W.; Potenza, M.N. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond Internet-use disorders, and specification of the process character of addictive behaviors. Neurosci. Biobehav. Rev. 2019, 104, 1–10. [Google Scholar] [CrossRef]
- Wölfling, K.; Müller, K.W.; : Dreier, M.; Ruckes, C.; Deuster, O.; Batra, A.; Mann, K.; Musalek, M.; Schuster, A.; Lemenager, T.; et al. Efficacy of Short-term Treatment of Internet and Computer game Addiction (STICA): A multicenter randomized controlled trial. JAMA Psychiatry 2019, 76, 1018–1025. [Google Scholar] [CrossRef]
- Müller, K.W.; Werthmann, J.; Beutel, M.E.; Wölfling, K.; Egloff, B. Maladaptive personality traits and their interaction with outcome expectancies in gaming disorder and internet-related disorders. Int. J. Environ. Res. Public Health 2021, 18, 3967. [Google Scholar] [CrossRef]
- Braun, B.; Stopfer, J.M.; Müller, K.W.; Beutel, M.E.; Egloff, B. Comparing regular gamers, non-gamers, and gaming addicts and differentiating between game genres. Comput. Hum. Behav. 2016, 55, 406–412. [Google Scholar] [CrossRef]
- Koronczai, B.; Kökönyei, G.; Griffiths, M.D.; Demetrovics, Z. The Relationship Between Personality Traits, Psychopathological Symptoms, and Problematic Internet Use: A Complex Mediation Model. J. Med. Internet. Res. 2019, 21, e11837. [Google Scholar] [CrossRef] [Green Version]
- Müller, K.W.; Beutel, M.E.; Egloff, B.; Wölfling, K. Investigating risk factors for Internet Gaming Disorder: A comparison of patients with addictive gaming, pathological gamblers and healthy controls regarding the Big Five personality traits. Eur. Addict. Res. 2014, 20, 129–136. [Google Scholar] [CrossRef]
- Wang, C.W.; Ho, R.T.; Chan, C.L.; Tse, S. Exploring personality characteristics of Chinese adolescents with internet-related addictive behaviors: Trait differences for gaming addiction and social networking addiction. Addict. Behav. 2015, 42, 32–35. [Google Scholar] [CrossRef]
- Kayiş, A.R.; Satici, S.A.; Yilmaz, M.F.; Şimşek, D.; Ceyhan, E.; Bakioğlu, F. Big five-personality trait and internet addiction: A meta-analytic review. Comput. Hum. Behav. 2016, 63, 35–40. [Google Scholar] [CrossRef]
- Roberts, B.W.; Mroczek, D. Personality trait change in adulthood. Curr. Dir. Psychol. Sci. 2008, 17, 31–35. [Google Scholar] [CrossRef] [Green Version]
- Specht, J.; Egloff, B.; Schmukle, S.C. Stability and change of personality across the life course: The impact of age and major life events on mean-level and rank-order stability of the Big Five. J. Personal. Soc. Psychol. 2011, 101, 862. [Google Scholar] [CrossRef] [Green Version]
- Durbin, C.E.; Hicks, B.M. Personality and psychopathology: A stagnant field in need of development. Eur. J. Personal. 2014, 28, 362–386. [Google Scholar] [CrossRef]
- Hicks, B.M.; Durbin, C.E.; Blonigen, D.M.; Iacono, W.G.; McGue, M. Relationship between personality change and the onset and course of alcohol dependence in young adulthood. Addiction 2012, 107, 540–548. [Google Scholar] [CrossRef] [Green Version]
- Wölfling, K.; Beutel, M.E.; Müller, K.W. OSV-S–Skala zum Onlinesuchtverhalten. In Diagnostische Verfahren in der Psychotherapie (Diagnostik für Klinik und Praxis); Geue, K., Strauß, B., Brähler, E., Eds.; Hogrefe: Göttingen, Germany, 2016; pp. 362–366. [Google Scholar]
- King, D.L.; Chamberlain, S.; Carragher, N.; Billieux, J.; Stein, D.; Müller, K.; Potenza, M.; Rumpf, H.; Saunders, J.; Starcevic, V.; et al. Screening and assessment tools for gaming disorder: A comprehensive systematic review. Clin. Psychol. Rev. 2020. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Soto, C.J.; John, O.P.; Gosling, S.D.; Potter, J. Age differences in personality traits from 10 to 65: Big Five domains and facets in a large cross-sectional sample. J. Personal. Soc. Psychol. 2011, 100, 330–348. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, R.D.; Friedman, H.S. Health Status and the Five-factor Personality Traits in a Nationally Representative Sample. J. Health Psychol. 2006, 11, 643–654. [Google Scholar] [CrossRef]
- Malouff, J.M.; Thorsteinsson, E.B.; Schutte, N.S. The relationship between the five-factor model of personality and symptoms of clinical disorders: A meta-analysis. J. Psychopathol. Behav. 2005, 27, 101–114. [Google Scholar] [CrossRef]
- Gullone, E.; Moore, S. Adolescent risk-taking and the five-factor model of personality. J Adolesc. 2000, 23, 393–407. [Google Scholar] [CrossRef]
- Graziano, W.G.; Ward, D. Probing the Big Five in adolescence: Personality and adjustment during a developmental transition. J. Personal. 1992, 60, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Mihara, S.; Higuchi, S. Cross-sectional and longitudinal epidemiological studies of I nternet gaming disorder: A systematic review of the literature. Psychiatry Clin. Neurosci. 2017, 71, 425–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, P.G.; Rau, H.K.; Cribbet, M.R.; Gunn, H.E. Openness to experience and stress regulation. J. Res. Personal. 2009, 43, 777–784. [Google Scholar] [CrossRef]
- Bean, A.M.; Nielsen, R.K.; Van Rooij, A.J.; Ferguson, C.J. Video game addiction: The push to pathologize video games. Prof. Psychol.-Res. Pract. 2017, 48, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Kardefelt-Winther, D.; Heeren, A.; Schimmenti, A.; van Rooij, A.; Maurage, P.; Carras, M.; Edman, J.; Blaszczynski, A.; Khazaal, Y.; Billieux, J. How can we conceptualize behavioural addiction without pathologizing common behaviours? Addiction 2017, 112, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Magidson, J.F.; Roberts, B.W.; Collado-Rodriguez, A.; Lejuez, C.W. Theory-driven intervention for changing personality: Expectancy value theory, behavioral activation, and conscientiousness. Dev. Psychol. 2014, 50, 1442–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Sociodemographics and Baseline Variables | Wave 1 (n = 1313) | Wave 2 (n = 941) |
|---|---|---|
| Sex; n (%) | ||
| female | 701(53.4) | 520 (55.3) |
| male | 612 (46.3) | 421 (44.7) |
| School type; n (%) | ||
| Lower secondary and secondary | 102 (7.8) | 82 (8.7) |
| Integrated, comprehensive | 270 (20.6) | 215 (22.8) |
| High school | 941 (71.7) | 644 (68.4) |
| Migration background; n (%) | ||
| Yes | 43 (3.3) | 33 (3.5) |
| no | 1214 (92.5) | 878 (93.3) |
| Missing | 56 (4.3) | 30 (3.2) |
| Residence (region); n (%) | ||
| rural | 497 (37.8) | 392 (41.7) |
| small town | 444 (33.8) | 237 (25.2) |
| city | 372 (28.3) | 312 (33.2) |
| Baseline measures; M (SD) | ||
| AICA-S | 3.9 (3.29) | 4.5 (3.23) |
| BFI: Neuroticism | 2.9 (0.96) | 2.9 (0.99) |
| BFI: Extraversion | 3.5 (0.88) | 3.5 (0.97) |
| BFI: Openness | 3.5 (1.02) | 3.4 (1.03) |
| BFI: Agreeableness | 3.3 (0.84) | 3.2 (0.84) |
| BFI: Conscientiousness | 3.3 (0.92) | 3.1 (0.91) |
| Sociodemographics | Course of IRD-Symptoms According to AICA-S | Statistical Comparison | ||
|---|---|---|---|---|
| Stable-Low (n = 395) | Quitters (n = 154) | Starters (n = 111) | ||
| Age; M (SD) | 13.1 (1.03) | 13.1 (1.05) | 12.9 (1.06) | p = 0.343 |
| sex; n (%) | ||||
| Female | 226 (57.2) | 94 (61.0) | 66 (59.5) | p = 0.698 |
| school type; n (%) | p = 0.195 | |||
| Lower secondary and secondary | 37 (9.4) | 19 (12.3) | 8 (7.2) | |
| Integrated, comprehensive | 82 (20.8) | 36 (23.4) | 33 (29.7) | |
| High school | 276 (69.9) | 99 (64.3) | 70 (63.1) | |
| migration background; n (%) | p = 0.147 | |||
| yes | 8 (2.1) | 6 (3.9) | 6 (5.6) | |
| Personality Traits and Cluster | Assessments (Time) | (1) Main effect | |
|---|---|---|---|
| (2) Interaction effect | |||
| t1 M (SD) | t2 M (SD) | ||
| Neuroticism | |||
| Starters | 2.84 (0.93) | 3.03 (1.01) | (1) n.s. (2) F(2642) = 3.56, p = 0.029; η2 = 0.011 |
| Quitters | 3.09 (0.96) a | 2.93 (0.97) b | |
| Stable-low | 2.88 (0.99) | 2.87 (0.97) | |
| Extraversion | |||
| Starters | 3.53 (0.86 | 3.59 (0.94 | (1) n.s. (2) n.s. |
| Quitters | 3.46 (0.95) | 3.43 (1.01) | |
| Stable-low | 3.41 (0.90) | 3.43 (0.98) | |
| Openness | |||
| Starters | 3.52 (0.90) a | 3.29 (1.08) b | (1) n.s. (2) F(2645) = 2.67, p = 0.070; η2 = 0.008 |
| Quitters | 3.40 (1.06) | 3.48 (1.02) | |
| Stable-low | 3.54 (0.99) | 3.52 (1.00) | |
| Agreeableness | |||
| Starters | 3.37 (0.92) | 3.08 (0.83) | (1) F(1647) = 18.63, p = 0.001; η2 = 0.028 (2) n.s. |
| Quitters | 3.29 (0.80) | 3.18 (0.87) | |
| Stable-low | 3.40 (0.82) | 3.24 (0.82) | |
| Conscientiousness | |||
| Starters | 3.35 (0.90) a | 2.79 (0.80) b | (1) F(1646) = 26.84, p = 0.001; η2 = 0.040 (2) F(2646) = 17.59, p = 0.001; η2 = 0.052 |
| Quitters | 2.93 (1.00) | 3.02 (0.96) | |
| Stable-low | 3.38 (0.91) a | 3.24 (0.90) b | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, K.W.; Beutel, M.E.; Reinecke, L.; Dreier, M.; Schemer, C.; Weber, M.; Schnauber-Stockmann, A.; Stark, B.; Quiring, O.; Wölfling, K. Internet-Related Disorders and Their Effects on Personality Development in Adolescents from Germany—Results from a Prospective Study. Int. J. Environ. Res. Public Health 2022, 19, 529. https://doi.org/10.3390/ijerph19010529
Müller KW, Beutel ME, Reinecke L, Dreier M, Schemer C, Weber M, Schnauber-Stockmann A, Stark B, Quiring O, Wölfling K. Internet-Related Disorders and Their Effects on Personality Development in Adolescents from Germany—Results from a Prospective Study. International Journal of Environmental Research and Public Health. 2022; 19(1):529. https://doi.org/10.3390/ijerph19010529
Chicago/Turabian StyleMüller, Kai W., Manfred E. Beutel, Leonard Reinecke, Michael Dreier, Christian Schemer, Mathias Weber, Anna Schnauber-Stockmann, Birgit Stark, Oliver Quiring, and Klaus Wölfling. 2022. "Internet-Related Disorders and Their Effects on Personality Development in Adolescents from Germany—Results from a Prospective Study" International Journal of Environmental Research and Public Health 19, no. 1: 529. https://doi.org/10.3390/ijerph19010529
APA StyleMüller, K. W., Beutel, M. E., Reinecke, L., Dreier, M., Schemer, C., Weber, M., Schnauber-Stockmann, A., Stark, B., Quiring, O., & Wölfling, K. (2022). Internet-Related Disorders and Their Effects on Personality Development in Adolescents from Germany—Results from a Prospective Study. International Journal of Environmental Research and Public Health, 19(1), 529. https://doi.org/10.3390/ijerph19010529