
Prevention and Harm Reduction Interventions for Adult Gambling at the Local Level: An Umbrella Review of Empirical Evidence

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
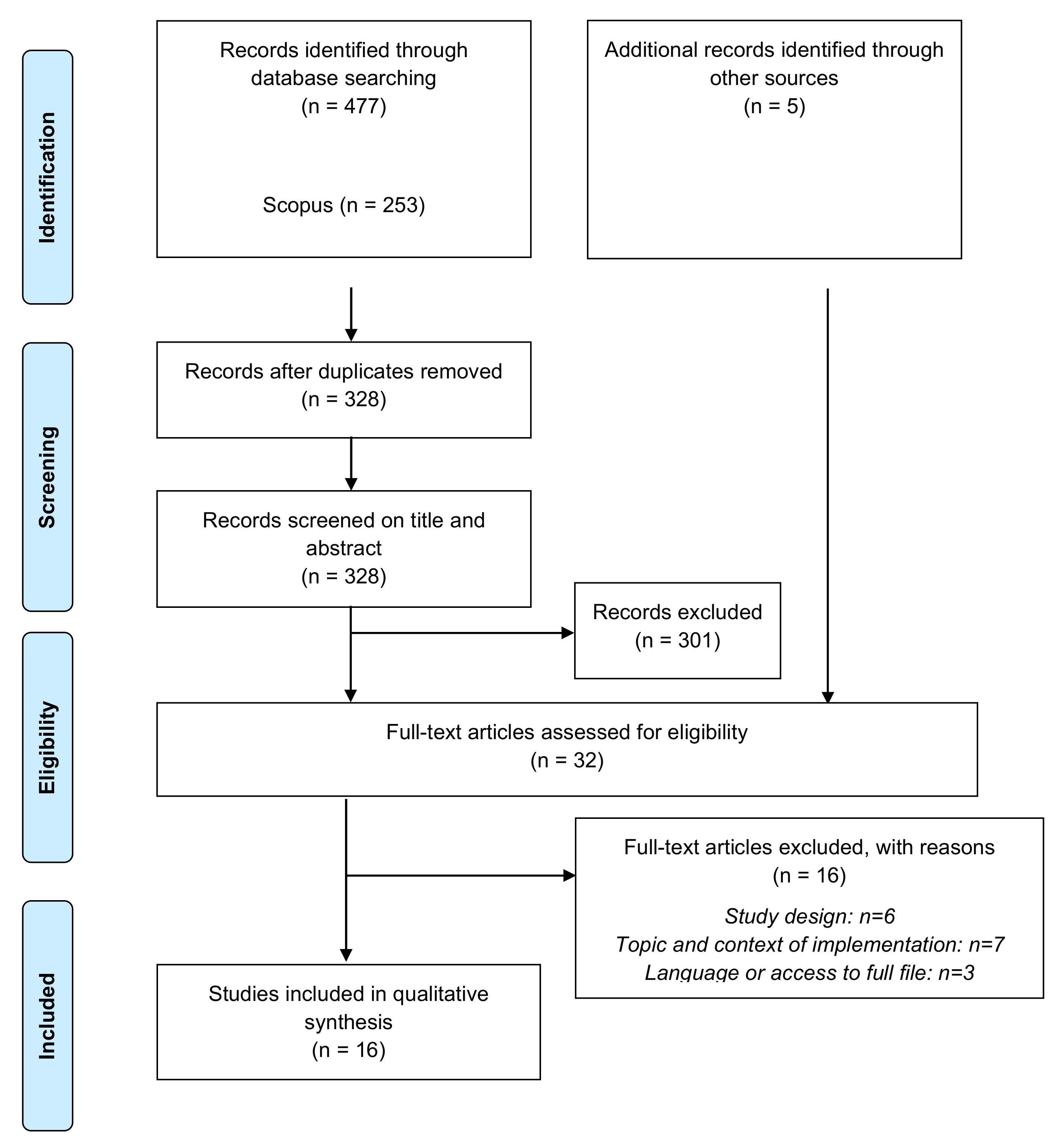
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- Population: Only reviews regarding the adult population were included;
- Intervention: Reviews about the effectiveness of actions, interventions, and policies to prevent or reduce harms and risks of gambling were included. Reviews about risk and protective factors or about gambling disorders treatment were excluded. Only interventions deemed feasible at local level, that can be implemented in specific areas by municipalities, regions, or other local agencies were considered. Reviews about actions which require the involvement of gambling industry or national laws or agreements were excluded;
- Outcomes: Changes in gambling behavior or related harm were considered as primary outcomes; secondary outcomes pertain to gambling attitudes, perceptions, and intentions. Recollections, acceptance of intervention, or knowledge were not considered;
- Comparison: Only systematic reviews and meta-analyses were included. Three mandatory criteria of the Database of Abstracts of Reviews of Effects (DARE) had to be met: the definition of a review question, the inclusion of a search strategy, and the presence of some data synthesis [3,24,25]. Reviews that considered randomized and nonrandomized trials and qualitative studies were included to better identify effective conditions of implementation.
2.3. Study Selection and Data Extraction
- Supply reduction: strategies aiming to reduce the supply and availability of gambling opportunities for the general population;
- Demand reduction: strategies aiming to reduce the desire to gamble and prevent or reduce initiation of problematic gambling;
- Risk reduction: strategies aiming to reduce the risk factors related to gambling. The target of these actions are gamblers, with the goal of decreasing the probability of developing risky or problematic gambling;
- Harm reduction: strategies targeting risky or problematic gamblers aiming to identify problematic situations and foster the relationship between them and specific health services.
3. Results
3.1. Supply Reduction Strategies
3.1.1. Restricting Gambling Venues and Licenses
3.1.2. Pricing and Taxation
3.1.3. Limiting Gambling Venue Hours of Operation
3.1.4. Legal Age
3.1.5. Limiting Accessibility to Gambling Venues
3.2. Demand Reduction Strategies
3.2.1. Restricting Advertising
3.2.2. Information/Awareness Campaigns
3.2.3. Educational Interventions
3.3. Risk Reduction Strategies
3.3.1. Restricting Access to Cash
3.3.2. Placing Gambling Venues Away from Vulnerable Populations
3.3.3. Ambient Natural Lighting
3.3.4. Clocks and Time Awareness
3.3.5. Machine Location
3.3.6. Smoking Bans/Restrictions
3.3.7. Alcohol Bans/Restrictions
3.4. Harm Reduction Strategies
3.4.1. Gambling Venues Employee Training
3.4.2. Tests and Screening
3.4.3. Helplines and Information about Care Services
3.4.4. Precommitment
3.4.5. Self-Exclusion
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, D.W.; Shaw, M. The epidemiology of gambling disorder. In Gambling Disorder; Heinz, A., Romanczuk-Seiferth, N., Potenza, M., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 29–48. [Google Scholar]
- Pyle, E.I. An Exploration of How Agency and Socio-Cultural Milieu Support Greater or Lesser Controlled Gambling and Recovery from Gambling Addiction; University of Plymouth: Plymouth, UK, 2017. [Google Scholar]
- McMahon, N.; Thomson, K.; Kaner, E.; Bambra, C. Effects of prevention and harm reduction interventions on gambling behaviours and gambling related harm: An umbrella review. Addict. Behav. 2019, 90, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Meyer, G.; Kalke, J.; Hayer, T. The impact of supply reductionon the prevalence of gamblingparticipation and disordered gambling behavior: A systematic review. Sucht 2018, 64, 283–293. [Google Scholar] [CrossRef]
- Grande-Gosende, A.; López-Núñez, C.; García-Fernández, G.; Derevensky, J.; Fernández-Hermida, J.R. Systematic Review of Preventive Programs for Reducing Problem Gambling Behaviors Among Young Adults. J. Gambl. Stud. 2020, 36, 1–22. [Google Scholar] [CrossRef]
- Moodie, C.; Reith, G. Responsible gambling signage on electronic gaming machines, before and after the implementation of the United Kingdom Gambling Act: An observational study. Int. Gambl. Stud. 2009, 9, 5–17. [Google Scholar] [CrossRef]
- Kusev, P.; van Schaik, P.; Alzahrani, S.; Lonigro, S.; Purser, H. Judging the morality of utilitarian actions: How poor utilitarian accessibility makes judges irrational. Psychon. Bull. Rev. 2016, 23, 1961–1967. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.; Kusev, I.; Cooke, A.J.; Baranova, V.; Van Schaik, P.; Kusev, P. Commentary: The Social Dilemma of Autonomous Vehicles. Front. Psychol. 2017, 8, 808. [Google Scholar] [CrossRef] [Green Version]
- Teal, J.; Kusev, P.; Heilman, R.; Martin, R.; Passanisi, A.; Pace, U. Problem Gambling ‘Fuelled on the Fly’. Int. J. Environ. Res. Public Health 2021, 18, 8607. [Google Scholar] [CrossRef]
- WHO. Health in All Policies. Helsinki Statement. Framework for Country Action; World Health Organization: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/112636 (accessed on 18 December 2018).
- Blaszczynski, A.; Collins, P.; Fong, D.; Ladouceur, R.; Nower, L.; Shaffer, H.J.; Tavares, H.; Venisse, J.-L. Responsible gambling: General principles and minimal requirements. J. Gambl. Stud. 2011, 27, 565–573. [Google Scholar] [CrossRef]
- Forsström, D.; Spångberg, J.; Petterson, A.; Brolund, A.; Odeberg, J. A systematic review of educational programs and consumer protection measures for gambling: An extension of previous reviews. Addict. Res. Theory 2020, 28, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Pawson, R.; Greenhalgh, T.; Harvey, G.; Walshe, K. Realist review—A new method of systematic review designed for complex policy interventions. J. Health Serv. Res. Policy 2005, 10, 21–34. [Google Scholar] [CrossRef]
- Rycroft-Malone, J.; McCormack, B.; Hutchinson, A.M.; DeCorby, K.; Bucknall, T.K.; Kent, B.; Schultz, A.; Snelgrove-Clarke, E.; Stetler, C.B.; Titler, M.; et al. Realist synthesis: Illustrating the method for implementation research. Implement. Sci. 2012, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- Velasco, V.; Griffin, K.W.; Antichi, M.; Celata, C. A large-scale initiative to disseminate an evidence-based drug abuse prevention program in Italy: Lessons learned for practitioners and researchers. Eval. Program Plann. 2015, 52, 27–38. [Google Scholar] [CrossRef]
- Wandersman, A.; Duffy, J.; Flaspohler, P.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. Am. J. Community Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef]
- Backer, T.E. The failure of success: Challenges of disseminating effective substance abuse prevention programs. J. Community Psychol. 2000, 28, 363–373. [Google Scholar] [CrossRef]
- Bassoli, M.; Marzulli, M.; Pedroni, M. Anti-gambling policies: Framing morality policy in Italy. J. Public Policy 2021, 41, 137–160. [Google Scholar] [CrossRef] [Green Version]
- Rogers, R.D.; Wardle, H.; Sharp, C.A.; Dymond, S.; Davies, T.J.; Hughes, K.; Astbury, G. Framing a Public Health Approach to Gambling Harms in Wales: Challenges and Opportunities; Bangor University: Bangor, UK, 2019; ISBN 9781789860474. [Google Scholar]
- Rolando, S.; Scavarda, A.; Jarre, P.; Beccaria, F. The social debate about gambling regulation in Italy: An analysis of stakeholders’ arguments. Int. Gambl. Stud. 2020, 20, 296–314. [Google Scholar] [CrossRef]
- Billieux, J.; Achab, S.; Savary, J.F.; Simon, O.; Richter, F.; Zullino, D.; Khazaal, Y. Gambling and problem gambling in Switzerland. Addiction 2016, 111, 1677–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Info. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Bambra, C.; Gibson, M.; Sowden, A.; Wright, K.; Whitehead, M.; Petticrew, M. Tackling the wider social determinants of health and health inequalities: Evidence from systematic reviews. J. Epidemiol. Community Health 2010, 64, 284–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairns, J.; Warren, J.; Garthwaite, K.; Greig, G.; Bambra, C. Go slow: An umbrella review of the effects of 20 mph zones and limits on health and health inequalities. J. Public Health 2015, 37, 515–520. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Union. EU Action Plan on Drugs 2017–2020 (2017/C 215/02). Off. J. Eur. Union 2017, 215, 21–58. [Google Scholar]
- Beckett, M.; Keen, B.; Angus, D.J.; Pickering, D.; Blaszczynski, A. Responsible gambling staff training in land-based venues: A systematic review. Int. Gambl. Stud. 2020, 20, 331–367. [Google Scholar] [CrossRef]
- Kotter, R.; Kräplin, A.; Pittig, A.; Bühringer, G. A Systematic Review of Land-Based Self-Exclusion Programs: Demographics, Gambling Behavior, Gambling Problems, Mental Symptoms, and Mental Health. J. Gambl. Stud. 2019, 35, 367–394. [Google Scholar] [CrossRef]
- Matheson, F.I.; Sztainert, T.; Lakman, Y.; Steele, S.J.; Ziegler, C.P.; Ferentzy, P. Prevention and treatment of problem gambling among older adults: A scoping review. J. Gambl. Issues 2018, 2018, 6–66. [Google Scholar] [CrossRef]
- Ladouceur, R.; Shaffer, P.; Blaszczynski, A.; Shaffer, H.J. Responsible gambling: A synthesis of the empirical evidence. Addict. Res. Theory 2017, 25, 225–235. [Google Scholar] [CrossRef]
- Drawson, A.S.; Tanner, J.; Mushquash, C.J.; Mushquash, A.R.; Mazmanian, D. The Use of Protective Behavioural Strategies in Gambling: A Systematic Review. Int. J. Ment. Health Addict. 2017, 15, 1302–1319. [Google Scholar] [CrossRef]
- Tanner, J.; Drawson, A.S.; Mushquash, C.J.; Mushquash, A.R.; Mazmanian, D. Harm reduction in gambling: A systematic review of industry strategies. Addict. Res. Theory 2017, 25, 485–494. [Google Scholar] [CrossRef]
- Gainsbury, S.M.; Blankers, M.; Wilkinson, C.; Schelleman-Offermans, K.; Cousijn, J. Recommendations for international gambling harm-minimisation guidelines: Comparison with effective public health policy. J. Gambl. Stud. 2014, 30, 771–788. [Google Scholar] [CrossRef] [Green Version]
- Babor, T.F.; Caetano, R.; Casswell, S.; Griffith, E.; Giesbrecht, N.; Graham, K.; Grube, J.W.; Hill, L.; Holder, H.; Homel, R.; et al. Alcohol: No Ordinary Commodity: Research and Public Policy; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Gainsbury, S.M. Review of Self-exclusion from Gambling Venues as an Intervention for Problem Gambling. J. Gambl. Stud. 2014, 30, 229–251. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, C.; Rintoul, A.; Francis, L. What is the evidence for harm minimisation measures in gambling venues? Evid. Base 2014, 2014, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Ariyabuddhiphongs, V. Problem Gambling Prevention: Before, During, and After Measures. Int. J. Ment. Health Addict. 2013, 11, 568–582. [Google Scholar] [CrossRef]
- Ladouceur, R.; Blaszczynski, A.; Lalande, D.R. Pre-commitment in gambling: A review of the empirical evidence. Int. Gambl. Stud. 2012, 12, 215–230. [Google Scholar] [CrossRef]
- Williams, R.J.; West, B.L.; Simpson, R.I. Prevention of Problem Gambling: A Comprehensive Review of the Evidence and Identified Best Practices; Ontario Problem Gambling Research Centre, Ontario Ministry of Health and Long Term Care: Alberta, CA, USA, 2012.
- Young, M.; Tyler, W. Mediating Markets: Gambling Venues, Communities and Social Harm. Gambl. Res. J. Natl. Assoc. Gambl. Stud. 2008, 20, 50. [Google Scholar]
- McMillen, J.; Pitt, S. Review of the ACT Government’s Harm Minimisation Measures; Centre for Gambling Research, Australian National University: Canberra, ACT, Australia, 2005. [Google Scholar]
- Kundu, P.V.; Pilver, C.E.; Desai, R.A.; Steinberg, M.A.; Rugle, L.; Krishnan-Sarin, S.; Potenza, M.N. Gambling-related attitudes and behaviors in adolescents having received instant (scratch) lottery tickets as gifts. J. Adolesc. Health 2013, 52, 456–464. [Google Scholar] [CrossRef] [Green Version]
- Binde, P. Selling dreams-causing nightmares? J. Gambl. Issues 2007, 20, 167–192. [Google Scholar] [CrossRef] [Green Version]
- Thomas, A.; Pfeifer, J.; Moore, S.; Meyer, D.; Yap, L.; Armstrong, A. Evaluation of the Removal of ATMs from Gaming Venues in Victoria, Australia; Office of Liquor, Gaming and Racing, Department of Justice: Melbourne, VIC, Australia, 2013.
- Blaszczynski, A.; Ladouceur, R.; Shaffer, H.J. A Science-Based Framework for Responsible Gambling: The Reno Model. J. Gambl. Stud. 2004, 20, 301–317. [Google Scholar] [CrossRef]
- Lal, A.; Siahpush, M. The effect of smoke-free policies on electronic gaming machine expenditure in Victoria, Australia. J. Epidemiol. Community Health 2008, 62, 11–15. [Google Scholar] [CrossRef]
- O’Neil, M.; Whetton, S.; Neal, P.; Dolman, B.; Dolman, M.; Giannopoulos, V. Study of the Impact of Caps on Electronic Gaming Machines; Office of Gaming and Racing, Department of Justice of Victoria: Melbourne, VIC, Australia, 2005.
- Victoria Department of Human Services. Annual Report, 2001–2002; State Government Victoria: Melbourne, VIC, Australia, 2002.
- Calloni, L.; Capriulo, A.P.; Torri, A.; Parisi, G.; Meroni, C.; Olivadoti, S.; Celata, C. Una “comunità competente” per la prevenzione ed il contrasto al Gioco d’Azzardo Patologico (GAP): Esperienze in corso nei territori lombardi. Psicol. Di Comunità 2020, 2, 23–40. [Google Scholar] [CrossRef]

{kind=link}
| Author | Year | Main Goal | N | Main Findings |
|---|---|---|---|---|
| Grande-Gosende [5] | 2020 | To critically assess the existing literature on the effectiveness of prevention programs aimed at reducing the prevalence of gambling problems among young adults and identify the specific preventive components used. | 9 | Gambling prevention programs mostly followed a selective or indicated prevention strategy. The personalized normative feedback (PNF) approach is the preferred strategy for reducing at-risk or problem gambling among young adults, showing at least a moderate positive effect in most of the included studies. Improving mathematical knowledge based on a gambling framework was shown to increase the ability to calculate gambling odds and resistance to gambling fallacies at the long-term assessment but did not reflect an overall reduction in gambling behavior. |
| Forsström [12] | 2020 | To assess the certainty of the evidence relating to different gambling preventive measures in the context of educational programs and consumer protection measures. To present and discuss the shortcomings identified in eligible studies to better understand how preventive measures should be designed and tentatively identify the probable results of future studies. | 28 | Results indicate a potential effect of PF interventions. For the remaining interventions, the certainty of evidence was very low. |
| Beckett [28] | 2020 | To evaluate the current evidence of the impact venue staff training programs in responsible gambling have on venue staff and gamblers. | 22 | Staff training programs provide some benefit to staff members. Few studies evaluated the effects on venue gamblers and there is insufficient evidence to make a clear causal link between responsible gambling staff training programs and the reduction of gambling harm in customers. |
| McMahon [3] | 2019 | To evaluate the systematic review evidence base on the effects of prevention and harm reduction interventions on gambling behaviors, and gambling-related harm. To examine differential effects of interventions across sociodemographic groups. | 10 | Precommitment and limit setting showed positive findings, but such interventions are limited by the extent to which users adhere to voluntary systems. Potential negative unintended consequences are possible for high-risk and problem gamblers. There was some preliminary support for reduced opening hours of gaming machines; smoking bans; personalized feedback interventions; removal of large note acceptors; maximum bets; and removal of ATMs. The quality of the included systematic reviews was found to be low. |
| Kotter [29] | 2019 | To understand who is participating in land-based self-exclusion programs, and the differences between excluders from casinos and those from other land-based gambling venues. To investigate how gambling behavior changes after self-exclusion for abstinence, reduction, increasing, breaching and relocation. To detect the prevalence of gambling problems and symptoms of other mental disorders in self-excluders. To understand whether exclusion reduces prevalence rates, other mental disorders, and improves mental health. | 19 | The results revealed wide ranges of changes in gambling behavior after exclusion. Gambling-related problems declined after self-exclusion, and several aspects of mental health improved. However, many self-excluders continued gambling inside or outside the excluded venues. Improvements in practice are needed. |
| Matheson [30] | 2018 | To summarize the literature and available evidence on the prevention and treatment of PG among older adults. To inform interventions for prevention and treatment and identify literature gaps. | 247 | Education for seniors should consider cultural differences, comorbidities, stigma associated with help seeking, and family supports. It should include awareness of the potential risks of gambling, self-diagnosis, cognitive distortions, and odds delivered in various formats to accommodate cognitive ability (e.g., dementia). Given that older adults engage in gambling as a social activity, it may be necessary to monitor accessibility to venues and frequency of patronage. Prevention training for the gambling industry should provide information on risk factors specific to older adults. Education in prevention for primary care professionals is imperative to ensure that older adults who access health-care services with gambling concerns are identified quickly. Training of staff at gambling venues, family, primary care staff, and staff working at senior residences is crucial. |
| Ladouceur [31] | 2017 | To identify empirically grounded responsible gambling studies to guide evidenced-based effective responsible gambling strategies. | 29 | Self-exclusion programs demonstrate some effectiveness as a component of RG programs despite various limitations including low utilization rates, breaching the agreement, and minimal evidence about the long-term outcomes. Although there is an increase in research focusing on behavioral indicators of gambling-related problems, the current state of knowledge remains underdeveloped. There is a lack of conclusive evidence about integrating these tools within fully developed RG programs. There is empirical evidence that suggests that limit setting can be effective for promoting RG. However, it is important to remember that limit setting is only effective for some individuals; it can increase gambling problems for others. Venue staff providing assistance to patrons experiencing problem gambling demonstrates partial effectiveness as a useful RG initiative. |
| Drawson [32] | 2017 | To collate the empirical evidence to date on the effectiveness of protective behavioral strategies in gambling. | 33 | Self-exclusion was the only strategy with sufficient evidence to be recommended; however, even the quality of this evidence was not high and requires improvement in future studies before clinical recommendations can be made. The findings on time-limit setting were inconsistent. Setting a monetary limit was much more highly endorsed than setting a time limit. Conclusions about the usefulness of other behavioral strategies for gamblers cannot be made |
| Tanner [33] | 2017 | To identify and evaluate industry/environmental-level harm reduction approaches to gambling. | 27 | Further research is needed to determine effectiveness of mandatory shutdowns to identify the most effective length of time and time of day for shutdowns. Few studies examined the effectiveness of on-screen clocks. Anecdotal results are available. While there is little research into EGM caps, preliminary evidence seems to suggest that it is an ineffective strategy to change gambling behavior. Smoking bans have been found to be effective. Overall gambling expenditure even though few individuals perceive a change in their gambling behavior. Alcohol use and gambling commonly co-occur and research suggests that alcohol may disinhibit gambling behavior but this is an area in need of further research to determine if it may be an effective harm reduction strategy. |
| Gainsbury [34] | 2014 | To provide recommendations for international guidelines for harm-minimization policy for gambling including Internet gambling. These recommendations will be based on the framework provided by Babor et al. [35] in relation to evidence-based alcohol policies. | 1 | Many of the public health policies implemented for substance use may be adaptable to addressing gambling-related harms. The most potential effective policies are legal age limit and regulation of licenses and monopolicies. Other potential effective policies are: price and tax regulation, grief interventions with at-risk and problematic gamblers and opening hours and outlet density reduction. |
| Gainsbury [36] | 2014 | To provide a comprehensive understanding of the available evidence to date that is relevant to the establishment and implementation of a self-exclusion program. | 14 | The assessments of self-exclusion programs internationally generally find that the majority of participants benefit from such schemes. However, the current programs are in need of improvements to improve utilization rates and outcomes over time. A key deficit in current self-exclusion programs is that the majority of problem gamblers do not enter into these agreements. |
| Livingstone [37] | 2014 | To review the available evidence for a range of harm minimization practices, particularly those implemented within EGM venues via “codes of practice.” | ns | There is only modest evidence supporting the harm minimization practices. Self-exclusion: there is modest evidence that SE programs are an effective intervention for changing individual (rather than population-wide) gambler behavior and reducing gambling-related harm Signals: there is no evidence of effectiveness. Venue staff screening: there is little evidence of practices where venue staff identify problem gambling behavior and then interact with gamblers so identified. Precommitment: while the evidence base is somewhat limited in demonstrating the effectiveness of universal and binding precommitment systems, it does demonstrate that partial–or optional–systems are not effective population-wide harm reduction strategies. ATM removal: there is modest but reasonable evidence of its effectiveness. |
| Ariyabuddhiphongs [38] | 2013 | To review the literature on problem gambling prevention measures, considering both harm reduction and responsible gambling models | 70 | Problem gambling prevention measures may be classified into the temporal sequence of before, during, and after gambling. The “before prevention measures” aim to correct misconceptions on and change attitudes toward gambling; their success in reducing gambling behaviors seems limited. The “during measures” that involve structural changes to gambling machines and insertion of warning signage appear to yield mixed results. The “after measures” that feature problem gamblers’ voluntary self-exclusion yield limited success; self-excluded gamblers breach the agreement by returning to the venues to gamble. |
| Ladouceur [39] | 2012 | To review the effectiveness of voluntary or mandatory precommitment systems for electronic gaming machines. | 17 | The presence of methodological limitations preclude any conclusive statement on the effectiveness of precommitment systems on gamblers. |
| Williams [40] | 2012 | To propose an etiological framework for understanding how problem gambling develops based on the available evidence and drawing from established models of addictive behavior. To comprehensively evaluate the effectiveness of the various initiatives that have been used around the world to prevent problem gambling based on their demonstrated efficacy and/or their similarity to initiatives that are empirically effective in preventing other addictive behavior. To identify current “best practices” for the prevention of problem gambling. | ns | A very large number of different prevention initiatives exist. There are a few initiatives where almost no direct evidence exists concerning their efficacy, many initiatives where some direct evidence exists, and a small number of initiatives where extensive evidence exists. The most commonly adopted prevention measures tend to be among the least effective ones. When potentially more effective initiatives are implemented, they are typically done in such an inconsequential or perfunctory fashion as to virtually ensure lack of impact. Some best practices suggested are: decrease the general availability of gambling; restrict the use of tobacco and alcohol while gambling; restrict access to money while gambling; and impart knowledge, attitudes, and skills to gamblers to inhibit the progression to problem gambling. |
| Young and Tyler [41] | 2008 | To review the potential social impacts of changes in the supply structure of gambling opportunities | 272 | Several structural characteristics of venues affect participation and problem gambling levels. These include distance from markets, type of gambling, number of EGMs, range of nongambling facilities, the structure of catchments, the level of community involvement, and different systems of ownership and control. More attention needs to be directed towards the socio-spatial relationships between venues and their local clienteles. |
| Strategies | Reviews (Number of Studies) | N | Summary of Findings on | Recommendations | |
|---|---|---|---|---|---|
| Effectiveness | Implementation Conditions | ||||
| Supply reduction strategies | |||||
| 1. Restricting gambling venues and licenses | Gainsbury, 2014; McMahon, 2019 (2); Tanner, 2017 (2); Williams, 2012 (11) | 13 | This is one of the most important strategies to reduce gambling supply. However, the quality of empirical research in this area should improve. Preliminary evidence suggests that the EGM caps is an ineffective strategy. | The limitations often last for a short time. Long-term policies should be implemented. | To evaluate long-term policies’ implementation. |
| 2. Pricing and taxation | Gainsbury, 2014; Williams, 2012 (1) | 1 | This is considered an effective strategy to reduce the gambling supply. | Increasing the price of participating in the legal market may increase the attractiveness of illegal markets. Illegal markets need to be under control for a tax increase to be effective. | |
| 3. Limiting gambling venue hours of operation | Gainsbury, 2014; McMahhon, 2019 (4); Tanner, 2017 (4); Williams, 2012 (3) | 6 | This seems to have an impact on reducing gambling harms and risk factors. | The consistency of opening hours across sites and the compliance with the regulation within the local context are fundamental. | Further research is needed to determine effectiveness of mandatory shutdowns to identify the most effective length of time and time of day for shutdowns. |
| 4. Legal age | Gainsbury, 2014; Williams, 2012 (8) | 8 | Prohibition of youth gambling seems successful in reducing gambling problems and requires adult involvement. Evidence shows the link between parental facilitation and increased gambling behaviors. | The implementation of this age limit is problematic. More controls and families’ sensibilization strategies are needed. | |
| 5. Limiting accessibility to gambling venues | Gainsbury, 2014; Williams, 2012 (8); Young & Tyler, 2008 (20) | 27 | This is a controversial strategy in literature, but it is considered potentially effective. | The efficacy of these actions is susceptible to contextual variations and factors related to interactions. | The interaction with other contextual factors should be considered. |
| Demand reduction strategies | |||||
| 6. Restricting advertising | Williams, 2012 (13) | 13 | It is reasonable to hypothesize that advertising contributes to a positive attitude about gambling, an increase in engagement when it is offered and to social acceptability. | Further research is needed to understand the impact of gambling advertising. | |
| 7. Information/awareness campaigns | Ariyabuddhiphongs, 2013 (2); Gainsbury, 2014; Livingstone et al., 2014 (2); Williams, 2012 (8) | 12 | They seem to raise awareness of the role of probability laws and skills in gambling, avoiding gambling fallacies. However, they are not associated with any decreases in actual gambling behavior. There is no evidence of effectiveness of venue signage. Specific campaigns targeted at parents may be effective in increasing awareness of the importance of restricting youth gambling. | More targeted campaigns should be developed. Parents are a potential target. | |
| 8. Educational interventions | Ariyabuddhiphongs, 2013 (3); Forsström, 2020 (9); Gainsbury, 2014; Grande-Gosende, 2020 (9); McMahon, 2019 (2); Matheson, 2018 (3); Williams, 2012 (21) | 38 | Most adult educational interventions had little impact on behaviors. Specific programs aimed at developing participants’ skills, change attitudes and restructure cognitive processes seem to be successful. An evaluation of RGICs showed that visitors appeared to modify misconceptions but did not have any impact on gambling behavior. PNF or PFI is considered a potentially effective, low-cost and easily disseminated strategy. | It is important to involve professionals with close relationship with participants. The PNF or PFI implementation should be cautious because it may cause a “boomerang effect” when targeting low-frequency gamblers. | To develop and evaluate new adult educational programs and parent training. |
| Risk reduction strategies | |||||
| 9. Restricting access to cash | Livingstone, 2014 (1); McMahon, 2019 (2); Tanner, 2017 (2); Williams, 2012 (7) | 9 | ATM removal in the vicinity of gambling venues can be considered as a moderately effective strategy. Reviews identify a lack of empirical research. | Other cash sources are not considered. | Additional research about its effectiveness is needed. Other cash sources should be considered. |
| 10. Placing gambling venues away from vulnerable populations | Williams, 2012 (5); Young and Tyler 2008 (11) | 16 | This has good empirical support. | A clear definition of vulnerable populations is necessary. | |
| 11. Ambient natural lighting | Williams, 2012 (4) | 4 | The lack of lighting and other design elements seems to promote gambling behavior mainly among current gamblers. | No information about different levels of light is available. | Additional research is needed. |
| 12. Clocks and time awareness | Drawson, 2017 (2); Ladouceur, 2017 (2); Tanner, 2017 (2); Williams, 2012 (3) | 4 | Most of the studies are focused on on-screen clocks. Few studies focus on room clocks. It does not seem effective in reducing session length or expenditure. | Other strategies to facilitate time awareness should be investigated because time awareness can have a positive influence. | |
| 13. Machine location | Matheson, 2018 (2); Williams, 2012 (4) | 5 | There is conflicting evidence about this strategy but, overall, reviews suggest this is an efficient way to counteract gambling. | Both visibility and isolation effects should be considered. | |
| 14. Smoking bans/restrictions | McMahon, 2019 (2); Tanner, 2017 (2); Williams, 2012 (9) | 11 | This is considered as one of the most effective strategies. | ||
| 15. Alcohol bans/restrictions | Williams, 2012 (10) | 10 | This has significant potential as a harm minimization strategy. | Additional research about its effectiveness is needed. | |
| Harm reduction strategies | |||||
| 16. Gambling venue employee training | Ariyabuddhiphongs, 2013 (3); Beckett, 2020 (22); Gainsbury, 2014; Ladouceur, 2017 (3); Matheson, 2018 (5); Williams, 2012 (12) | 31 | Staff training programs are effective in changing staff members’ knowledge, attitudes, and self-confidence. However, they fail in promoting a proactive strategy and in facilitating intervention with some gamblers. Some training interventions have a short-term effect if not supported by the different stakeholders involved. There is insufficient evidence about effects in customers. | The main target is problematic gamblers, but all gamblers should be considered to encourage responsible behaviors. Behavioral skills training is necessary. Stakeholders’ involvement improves effectiveness. | More research about design, implementation and evaluation of employee training is needed. Training aimed at developing staff members’ behavioral skills should be designed. |
| 17. Test and screening | Gainsbury, 2014; Livingstone, 2014 (2); Matheson, 2018 (1) | 3 | This is most likely effective. | Many barriers intervene: lack of time, skills, motivation, and organizational factors. These interventions are more effective when combined with specific training. | Additional research about the implementation is needed. |
| 18. Helplines and care services information | Livingstone, 2014 (2); Williams, 2012 (4) | 6 | Results are inconsistent. | More studies are needed. | |
| 19. Precommitment | Kotter, 2019 (19); Ladouceur, 2012 17); Ladouceur, 2017 (5); Livingstone, 2014 (15); McMahon, 2019 (13); Matheson, 2018 (7); Williams, 2012 (11) | 47 | A conclusive statement on the effectiveness of pre-precommitment cannot yet be offered because of methodological problems, implementation discrepancy and inconsistent results. | It is important to distinguish the target to avoid boomerang effects; universal and binding precommitment systems are effective; a focus on limiting the time spent is priority. | To better design implementation conditions and monitor fidelity. |
| 20. Self-exclusion | Ariyabuddhiphongs, 2013 (10); Drawson, 2017 (14); Gainsbury, 2014 (14); Ladouceur, 2017 (9); Livingstone, 2014 (18); McMahon, 2019 (11); Matheson, 2018 (7); Williams, 2012 (16) | 47 | A conclusive statement on the effectiveness of self-exclusion cannot yet be offered because of methodological problems, implementation discrepancy and inconsistent results. Self-excluders generally experience benefits from the program. | The reviews analyzed offer several suggestions about the effectiveness of implementation conditions and elements that should be included in self-exclusion programs were suggested. | To better design implementation conditions and monitor fidelity. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasco, V.; Scattola, P.; Gavazzeni, L.; Marchesi, L.; Nita, I.E.; Giudici, G. Prevention and Harm Reduction Interventions for Adult Gambling at the Local Level: An Umbrella Review of Empirical Evidence. Int. J. Environ. Res. Public Health 2021, 18, 9484. https://doi.org/10.3390/ijerph18189484
Velasco V, Scattola P, Gavazzeni L, Marchesi L, Nita IE, Giudici G. Prevention and Harm Reduction Interventions for Adult Gambling at the Local Level: An Umbrella Review of Empirical Evidence. International Journal of Environmental Research and Public Health. 2021; 18(18):9484. https://doi.org/10.3390/ijerph18189484
Chicago/Turabian StyleVelasco, Veronica, Paola Scattola, Laura Gavazzeni, Lara Marchesi, Ioana Elena Nita, and Gilberto Giudici. 2021. "Prevention and Harm Reduction Interventions for Adult Gambling at the Local Level: An Umbrella Review of Empirical Evidence" International Journal of Environmental Research and Public Health 18, no. 18: 9484. https://doi.org/10.3390/ijerph18189484
APA StyleVelasco, V., Scattola, P., Gavazzeni, L., Marchesi, L., Nita, I. E., & Giudici, G. (2021). Prevention and Harm Reduction Interventions for Adult Gambling at the Local Level: An Umbrella Review of Empirical Evidence. International Journal of Environmental Research and Public Health, 18(18), 9484. https://doi.org/10.3390/ijerph18189484