
Gambling in Spanish Adolescents: Prevalence and Association with Mental Health Indicators

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
- Gambling frequency. The question on the ESTUDES survey was used. It contains two items (online and in person) that evaluate gambling frequency (number of times) on a 5-point Likert scale (never having gambled, not having gambled in the past 12 months, gambled monthly, weekly, or daily).
- Type of game in which they have bet money. The analysis was performed by using an adaptation of the 14-question instrument from the ESTUDES survey, which evaluates different types of gambling. For the two items (online and in person), the participant is asked to indicate the types of gambling in which they have participated in the past 12 months. The 12 options (multiple choice) are Lotteries, Instant lotteries, Football pools, Sport bets, Horse racing bets, Slots and slot machines, Cash games and cards, Bingo, Video games, eSports or electronic sports, Casino games, and Games in gambling halls.
- Gambling intensity. An adaptation of items from the ESTUDES survey was also used. For the two items (online and in person), the questionnaire includes 5 of the 7 questions from the original questionnaire to evaluate the participants who had gambled money in the past 12 months. The five questions are associated with five categories of intensity, corresponding to different maximum amounts of money gambled in a day. The response options were: less than €6, between €6 and €30, between €31 and €60, between €61 and €300, more than €300, I have not bet money in the past 12 months, and I have never bet money.
- Strengths and Difficulties Questionnaire (SDQ) [21]. The SDQ is a widely-used measurement instrument to assess behavioral and emotional difficulties and social skills. In addition, this questionnaire is commonly used as a tool for psychopathological screening and epidemiological analysis of the state of mental health in the youth population. The SDQ, through a brief, simple, and easy to administer questionnaire, makes it possible to obtain reliable samples of conducts related to emotional and behavioral problems (Fonseca, 2017). It is composed of 25 items with a 3-point Likert scale (0 = no, never, 1 = sometimes, 2 = yes, always). The items are grouped in five scales with five items each: Emotional Difficulties; Conduct Problems; Hyperactivity Difficulties; Problems with Peers; and Prosocial Behavior. The first four scales make up the Total Difficulties score. The higher the score, the higher the level of emotional and behavioral difficulties. In contrast, in the case of the Prosocial Behavior scale, a lower score is associated with worse behavioral adjustment [22]. In this study, we used the Spanish version of the scale [23]. The level of internal consistency of the Total difficulties score was 0.84, ranging between 0.71 and 0.75 for the SDQ subscales.
- Rosenberg Self-esteem Scale [24]. It is a unidimensional scale that makes it possible to assess self-esteem. Its 10 items are statements that can be used to assess self-esteem (e.g., I think I have reasons to feel proud). The items have a 4-point Likert scale (from 1 = strongly disagree to 4 = strongly agree). The scale showed good reliability in this sample (α = 0.87).
- Reynolds Adolescent Depression Scale Short Form (RADS-SF) [25]. This instrument, through its 10 items, evaluates the severity of depressive symptomatology in adolescence. The items cover different dimensions (Anhedonia, Somatic complaints, Negative self-evaluation. and Dysphoria), and responses are given on a 4-point Likert scale (from 1 = almost never to 4 = almost always). It is a widely used scale, validated by studies such as the one by Ortuño-Sierra et al. [26].
- Personal Wellbeing Index-School Children (PWI-SC) [27,28]. The PWI-SC is an instrument used to assess subjective wellbeing in school-aged children and adolescents (PWI-SC). It is composed of eight items that measure, in a generic and abstract way, subjective satisfaction with a specific life domain. The items have several response options, ranging from very dissatisfied (score of 0) to very satisfied (score of 10). The first item analyzes "life as a whole", whereas the other seven items refer to satisfaction with: health; standard of living; accomplishments in life; how secure they feel; the groups of people they are part of; future security; and their relationships with other people. The overall score is obtained by adding up the scores on the seven items (except item one). The PWI-SC has been validated in previous studies with adolescents, both nationally and internationally [22]. The scale showed good reliability in this sample (α = 0.94).
2.3. Procedure
2.4. Data Analysis
3. Results
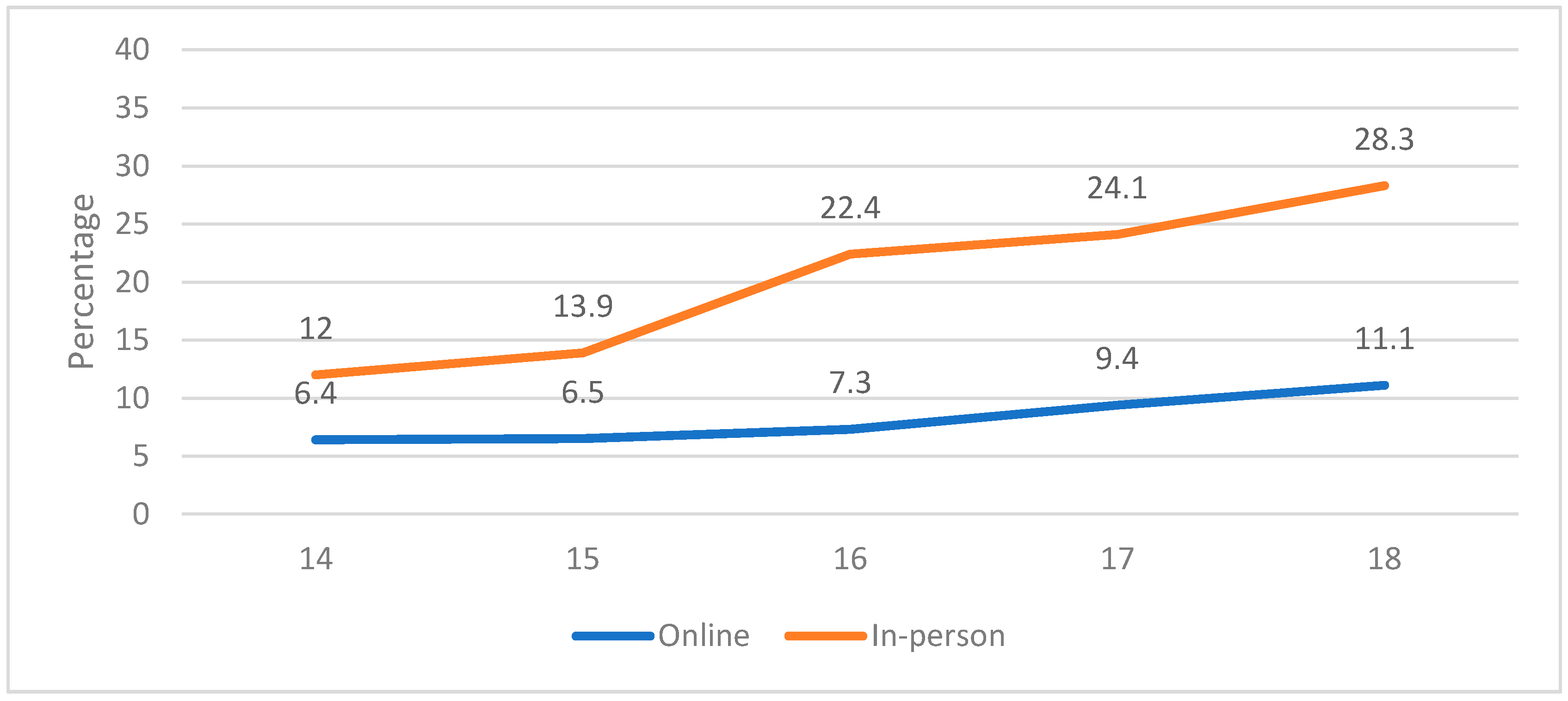
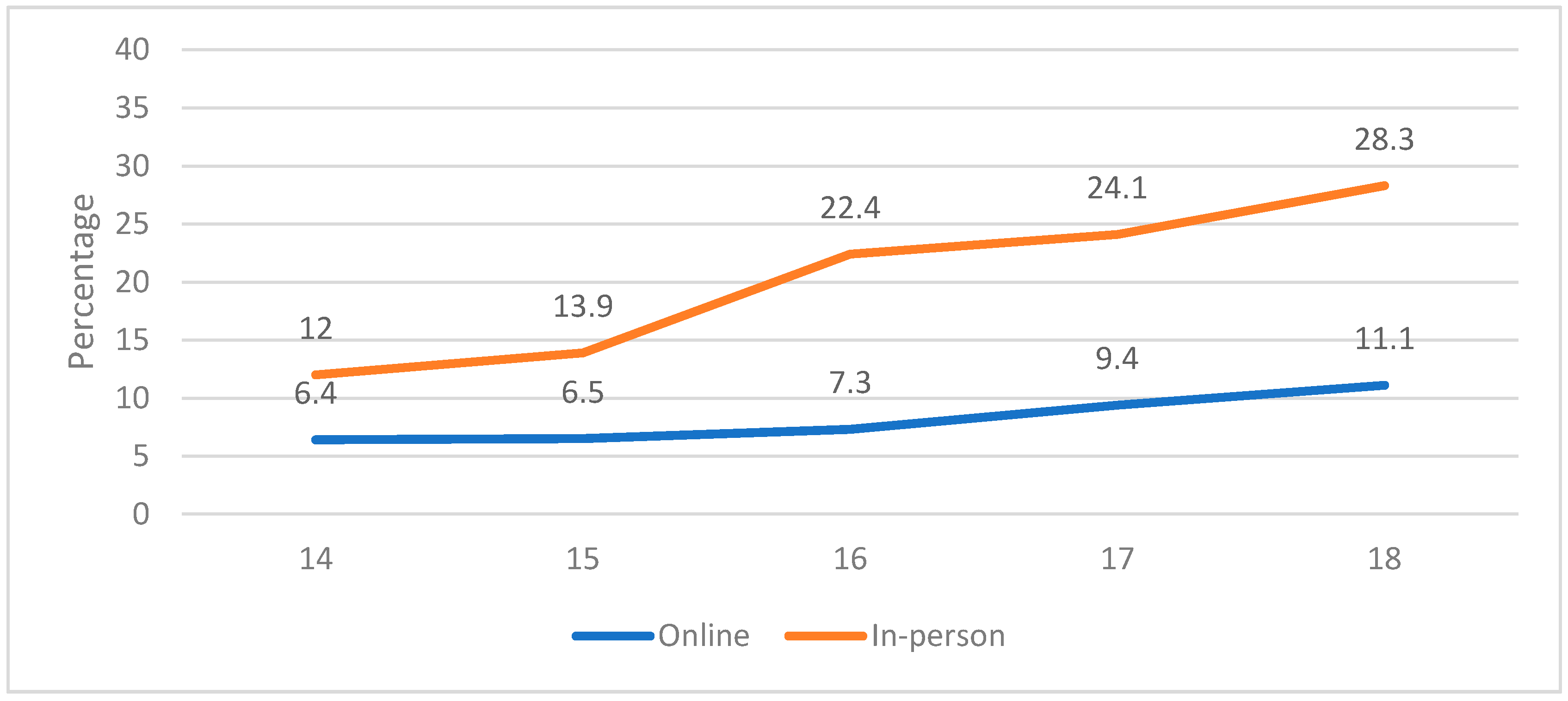
3.1. Prevalence of Gambling: Gender and Age Differences
3.2. Relationship between Gambling and Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zou, Z.; Wang, H.; d’Oleire Uquillas, F.; Wang, X.; Ding, J.; Chen, H. Definition of substance and non-substance addiction. Adv. Exp. Med. Biol. 2017, 1010, 21–41. [Google Scholar] [PubMed]
- ESPAD Group. ESPAD Report 2015: Results from the European School Survey Project on Alcohol and Other Drugs; Publications Office of the European Union: Lisbon, Portugal, 2016. [Google Scholar]
- Petry, N.M.; Zajac, K.; Ginley, M.K. Behavioral addictions as mental disorders: To be or not to be? Ann. Rev. Clin. Psychol. 2018, 14, 399–423. [Google Scholar] [CrossRef] [PubMed]
- Plan Nacional Sobre Drogas. Encuesta Sobre el Uso de Drogas en Enseñanzas Secundarias en España (ESTUDES) 2018–2019; Delegación del Gobierno para el Plan Nacional sobre Drogas, Ministerio de Sanidad, Política Social e Igualdad: Madrid, Spain, 2020. [Google Scholar]
- ESPAD Group. ESPAD Report 2019: Results from the European School Survey Project on Alcohol and Other Drugs; Publications Office of the European Union: Lisbon, Portugal, 2020. [Google Scholar]
- Hammond, C.J.; Mayes, L.C.; Potenza, M.N. Neurobiology of adolescent substance use and addictive behaviors: Prevention and treatment implications. Adolesc. Med. State Art Rev. 2014, 25, 15. [Google Scholar] [PubMed]
- Arnott, S.R.; Alain, C. The auditory dorsal pathway: Orienting vision. Neurosci. Biobehav. Rev. 2011, 35, 2162–2173. [Google Scholar] [CrossRef]
- Oman, R.F.; Vesely, S.; Aspy, C.B.; McLeroy, K.R.; Rodine, S.; Marshall, L. The potential protective effect of youth assets on adolescent alcohol and drug use. Am. J. Public Health 2004, 94, 1425–1430. [Google Scholar] [CrossRef]
- Brezing, C.; Derevensky, J.L.; Potenza, M.N. Non–substance-addictive behaviors in youth: Pathological gambling and problematic internet use. Child Adolesc. Psychiatr. Clin. 2010, 19, 625–641. [Google Scholar] [CrossRef] [Green Version]
- Emond, A.M.; Griffiths, M.D. Gambling in children and adolescents. Brit. Med. Bull. 2020, 136, 21–29. [Google Scholar] [CrossRef]
- Mestre-Bach, G.; Steward, T.; Granero, R.; Fernández-Aranda, F.; Mena-Moreno, T.; Vintró-Alcaraz, C.; Lozano-Madrid, M.; Menchón, J.M.; Potenza, M.N.; Jiménez-Murcia, S. Dimensions of Impulsivity in Gambling Disorder. Sci. Rep. 2020, 10, 397. [Google Scholar] [CrossRef]
- Donati, M.A.; Chiesi, F.; Primi, C. A model to explain at-risk/problem gambling among male and female adolescents: Gender similarities and differences. J. Adolesc. 2013, 36, 129–137. [Google Scholar] [CrossRef]
- Mestre-Bach, G.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Potenza, M.N. Emotional regulation in gambling disorder. Curr. Opin. Behav. Sci. 2020, 34, 12–18. [Google Scholar] [CrossRef]
- Potenza, M.N.; Wareham, J.D.; Steinberg, M.A.; Rugle, L.; Cavallo, D.A.; Krishnan-Sarin, S.; Desai, R.A. Correlates of at-risk/problem internet gambling in adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Okunna, N.C.; Rodriguez-Monguio, R.; Smelson, D.A.; Poudel, K.C.; Volberg, R. Gambling involvement indicative of underlying behavioral and mental health disorders. Am. J. Addict. 2016, 25, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Dowling, N.A.; Merkouris, S.S.; Greenwood, C.J.; Oldenhof, E.; Toumbourou, J.W.; Youssef, G.J. Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clin. Psychol. Rev. 2017, 51, 109–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrie, E.K.; Tzavara, C.K.; Tzavela, E.; Richardson, C.; Greydanus, D.; Tsolia, M.; Tsitsika, A.K. Gambling involvement and problem gambling correlates among European adolescents: Results from the European Network for Addictive Behavior study. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 1429–1441. [Google Scholar] [CrossRef]
- Caldeira, K.M.; Arria, A.M.; O’Grady, K.E.; Vincent, K.B.; Robertson, C.; Welsh, C.J. Risk factors for gambling and substance use among recent college students. Drug Alcohol Depend. 2017, 179, 280–290. [Google Scholar] [CrossRef]
- Dussault, F.; Brendgen, M.; Vitaro, F.; Carbonneau, R.; Boivin, M.; Tremblay, R.E. Co-morbidity between gambling problems and depressive symptoms: A longitudinal perspective of risk and protective factors. J. Gambl. Stud. 2015, 32, 547–565. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, W.M.; Laursen, B.; Hoza, B. The snowball effect: Friendship moderates escalations in depressed affect among avoidant and excluded children. Dev. Psychopathol. 2010, 22, 749–757. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, E. Bienestar Emocional en Adolescentes Riojanos. No Hay Salud Sin Salud Mental; Universidad de La Rioja: La Rioja, Spain, 2017. [Google Scholar]
- Ortuño-Sierra, J.; Chocarro, E.; Fonseca-Pedrero, E.; Sastre i Riba, S.; Muñiz, J. The assessment of emotional and Behavioural problems: Internal structure of The Strengths and Difficulties Questionnaire. Int. J. Clin. Health Psychol. 2015, 15, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M. The Measurement of Self-Esteem, Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Reynolds, W.M. Reynolds Adolescent Depression Scale; Psychological Assessment Resources: Lutz, FL, USA, 2002. [Google Scholar]
- Ortuño-Sierra, J.; Aritio-Solana, R.; Inchausti, F.; Chocarro, E.; Lucas-Molina, B.; Pérez-Albéniz, A.; Fonseca-Pedrero, E. Screening for depressive symptoms in adolescents at school: New validity evidences on the short form of the Reynolds Depression Scale. PLoS ONE 2017, 12, e0170950. [Google Scholar] [CrossRef]
- Cummins, R.A.; Lau, A.L. Personal Wellbeing Index–School Children; School of Psychology, Deakin University: Melbourne, Australia, 2005. [Google Scholar]
- Tomyn, A.J.; Norrish, J.M.; Cummins, R.A. The subjective wellbeing of indigenous Australian adolescents: Validating the personal wellbeing index-school children. Soc. Indic. Res. 2013, 110, 1013–1031. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Calado, F.; Alexandre, J.; Griffiths, M.D. Prevalence of adolescent problem gambling: A systematic review of recent research. J. Gambl. Stud. 2017, 33, 397–424. [Google Scholar] [CrossRef] [Green Version]
- Cámara, P.C.; Perona, V.C.; Irles, D.L. Prevalencia del juego de apuestas en adolescentes. Un análisis de los factores asociados. Salud Drogas 2018, 18, 165–173. [Google Scholar]
- Elton-Marshall, T.; Leatherdale, S.T.; Turner, N.E. An examination of internet and land-based gambling among adolescents in three Canadian provinces: Results from the youth gambling survey (YGS). BMC Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dirección General de Ordenación del Juego. Estudio Sobre Prevalencia, Comportamiento y Características de los Usuarios de Juegos de Azar en España 2015; Ministerio de Hacienda y Administración Pública: Madrid, Spain, 2016. [Google Scholar]
- Lloret, D.; Cabrera, V.; Cánovas, M.; Castaños, A.; Martínez, V.; Moreno, A. El Juego de Apuestas en Adolescentes de la Provincia de Alicante. Prevalencia y Factores Asociados; Provincial Government of Alicante: Alicante, Spain, 2016.
- Sierra, I.; Pérez, I.; García de Salazar, H. Jóvenes y Juegos de Azar: Estudio Sobre la Participación en Juegos de Azar de la Juventud de Vitoria-Gasteiz; Observatorio de la Realidad de las Personas Jóvenes de Vitoria-Gasteiz: Vitoria-Gasteiz, Spain, 2019. [Google Scholar]
- Lamas, J.; Virtudes, M.; Aragón, M.; Santolaria, R.; Estévez, A.; Jáuregui, P. Guía Clínica Específica, Jóvenes y Juego Online; Federación Española de Jugadores de Azar Rehabilitados (FEJAR) y Ministerio de Sanidad de España: La Coruña, Spain, 2018. [Google Scholar]
- Ricketts, T.; Macaskill, A. Gambling as emotion management: Developing a grounded theory of problem gambling. Addict Res. Theory 2003, 11, 383–400. [Google Scholar] [CrossRef]
- Kaare, P.R.; Mottus, R.; Konstabel, K. Pathological gambling in Estonia: Relationships with personality, self-esteem, emotional states and cognitive ability. J. Gambl. Stud. 2009, 25, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Paleologou, A.; Lazaratou, H.; Anagnostopoulos, D.; Economou, M.; Malliori, M.; Papadimitriou, G.; Papageorgiou, C. Problem gambling and concurrent emotional/behavioral problems among Greek adolescents. Turk. Arch. Pediatr. 2019, 54, 166. [Google Scholar] [CrossRef]
- Welte, J.W.; Barnes, G.M.; Tidwell, M.C.O.; Hoffman, J.H. Association between problem gambling and conduct disorder in a national survey of adolescents and young adults in the United States. J. Adolesc. Health 2009, 45, 396–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retz, W.; Ringling, J.; Retz-Junginger, P.; Vogelgesang, M.; Rösler, M. Association of attention-deficit/hyperactivity disorder with gambling disorder. J. Neural Transm. Suppl. 2016, 123, 1013–1019. [Google Scholar] [CrossRef]
- Romo, L.; Rémond, J.J.; Coeffec, A.; Kotbagi, G.; Plantey, S.; Boz, F.; Kern, L. Gambling and Attention Deficit Hyperactivity Disorders (ADHD) in a population of French students. J. Gambl. Stud. 2015, 31, 1261–1272. [Google Scholar] [CrossRef]
- Faregh, N.; Derevensky, J. Gambling behavior among adolescents with attention deficit/hyperactivity disorder. J. Gambl. Stud. 2011, 27, 243–256. [Google Scholar] [CrossRef]
- Zheng, J.; Zhong, Y.; Liu, Y. Effects of self-esteem level on risk preference in different tasks. Soc. Behav. Personal. 2013, 41, 815–818. [Google Scholar] [CrossRef]
- Moodie, C.; Finnigan, F. Association of pathological gambling with depression in Scotland. Psychol. Rep. 2006, 99, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Sanscartier, M.D.; Edgerton, J.D.; Roberts, L.W. A latent class analysis of gambling activity patterns in a Canadian university sample of emerging adults: Socio-demographic, motivational, and mental health correlates. J. Gambl. Stud. 2018, 34, 863–880. [Google Scholar] [CrossRef] [PubMed]
- Oei, T.P.; Goh, Z. Interactions between risk and protective factors on problem gambling in Asia. J. Gambl. Stud. 2014, 31, 557–572. [Google Scholar] [CrossRef] [PubMed]
- Pérez, S. Juventud y Juegos de Azar, Una Visión General del Juego en los Jóvenes; Instituto de la Juventud en España: Madrid, Spain, 2018. [Google Scholar]
- Neighbors, C.; Lostutter, T.W.; Cronce, J.M.; Larimer, M.E. Exploring college student gambling motivation. J. Gambl. Stud. 2002, 18, 361–370. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gambling | In Person | Online | Total | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | Total | M | F | Total | M | F | Total | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| I didn’t gamble for money | 494 | 60.5 | 838 | 87.2 | 1345 | 75.1 | 662 | 81.1 | 933 | 97.1 | 1608 | 89.8 | 533 | 65.3 | 878 | 91.4 | 1411 | 79.4 |
| I gambled for money | 332 | 39.5 | 123 | 12.8 | 445 | 24.9 | 154 | 18.9 | 28 | 2.9 | 182 | 10.2 | 283 | 34.7 | 83 | 8.6 | 366 | 20.6 |
| Prevalence In-Person Gambling | Prevalence Online Gambling | |||
|---|---|---|---|---|
| Types | n | % | n | % |
| Lotteries | 58 | 7.4 | 22 | 7.1 |
| Instant lotteries | 43 | 5.5 | 17 | 5.5 |
| Football pools | 90 | 11.5 | 31 | 10 |
| Sport bets | 219 | 28 | 99 | 32 |
| Betting on horse races | 20 | 2.6 | 7 | 2.3 |
| Slot machines | 57 | 7.3 | 9 | 2.3 |
| Card games with money | 105 | 13.4 | 29 | 9.4 |
| Bingo | 88 | 11.2 | 4 | 1.3 |
| Videogames | 25 | 3.2 | 68 | 22 |
| eSports or electronic sports | 13 | 1.7 | 15 | 4.9 |
| Casino games | 28 | 3.6 | 6 | 2 |
| Games in gambling halls | 36 | 4.6 | 2 | 0.7 |
| Mean | In-Person Game | Online Game |
|---|---|---|
| General | 14.31 | 14.47 |
| Male | 14.39 | 14.48 |
| Female | 14.05 | 14.38 |
| In-Person Gambling | Online Gambling | |||||
|---|---|---|---|---|---|---|
| Categories | Total | M | F | Total | M | F |
| Less than 6 euros | 70.6 | 70.3 | 71.6 | 55.1 | 53.9 | 66.7 |
| Between 6 and 30 euros | 20.3 | 19.6 | 22 | 30.1 | 30.5 | 26.7 |
| Between 31 and 60 euros | 5.3 | 5.9 | 3.7 | 7.7 | 8.5 | 0.0 |
| Between 61 and 300 euros | 2.8 | 2.8 | 2.8 | 5.1 | 5.0 | 6.7 |
| More than 300 euros | 1 | 1.4 | 0.0 | 1.9 | 2.1 | 0.0 |
| Gambled Money in the Past Year (n = 365) | Did not Gamble Money in the Past Year (n = 1416) | ||||
|---|---|---|---|---|---|
| M (SD) | M (SD) | F | p | Partial η2 | |
| Emotional symptoms | 2.85 (2.13) | 3.60 (2.45) | 28.265 | 0.000 | 0.016 |
| Behavioral problems | 2.20 (1.65) | 1.61 (1.50) | 43.052 | 0.000 | 0.024 |
| Peer problems | 1.26 (1.30) | 1.50 (1.65) | 6.274 | 0.012 | 0.004 |
| Hyperactivity | 4.79 (2.16) | 4.24 (2.16) | 19.069 | 0.000 | 0.011 |
| Prosocial | 8.23 (1.50) | 8.65 (1.39) | 24.791 | 0.000 | 0.014 |
| Total difficulties | 11.11 (4.64) | 10.95 (5.23) | 0.296 | 0.587 | 0.000 |
| Self-esteem | 32.17 (4.87) | 30.46 (5.67) | 27.962 | 0.000 | 0.015 |
| Depression | 15.96 (3.78) | 16.53 (4.66) | 4.688 | 0.031 | 0.003 |
| Subjective well-being | 7.97 (1.67) | 7.70 (1.91) | 6.095 | 0.014 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Albéniz, A.; Gil, M.; Díez-Gómez, A.; Martín-Seoane, G.; Lucas-Molina, B. Gambling in Spanish Adolescents: Prevalence and Association with Mental Health Indicators. Int. J. Environ. Res. Public Health 2022, 19, 129. https://doi.org/10.3390/ijerph19010129
Pérez-Albéniz A, Gil M, Díez-Gómez A, Martín-Seoane G, Lucas-Molina B. Gambling in Spanish Adolescents: Prevalence and Association with Mental Health Indicators. International Journal of Environmental Research and Public Health. 2022; 19(1):129. https://doi.org/10.3390/ijerph19010129
Chicago/Turabian StylePérez-Albéniz, Alicia, Mario Gil, Adriana Díez-Gómez, Gema Martín-Seoane, and Beatriz Lucas-Molina. 2022. "Gambling in Spanish Adolescents: Prevalence and Association with Mental Health Indicators" International Journal of Environmental Research and Public Health 19, no. 1: 129. https://doi.org/10.3390/ijerph19010129
APA StylePérez-Albéniz, A., Gil, M., Díez-Gómez, A., Martín-Seoane, G., & Lucas-Molina, B. (2022). Gambling in Spanish Adolescents: Prevalence and Association with Mental Health Indicators. International Journal of Environmental Research and Public Health, 19(1), 129. https://doi.org/10.3390/ijerph19010129