
Prevalence and Factors for Anxiety during the COVID-19 Pandemic among College Students in China




Abstract
1. Introduction
2. Methods
2.1. Study Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Participants
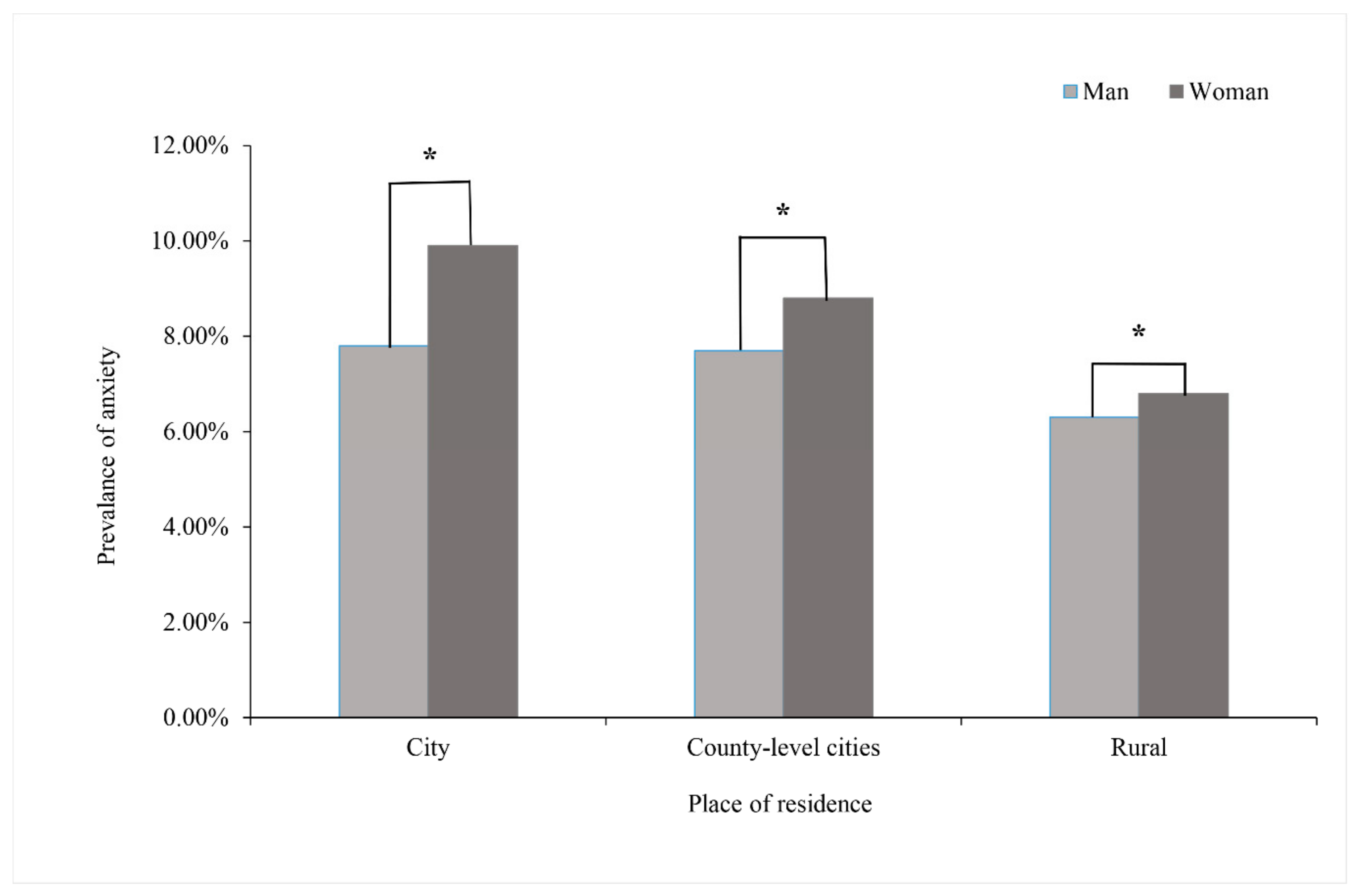
3.2. Prevalence of Anxiety
3.3. The Cognitive Level about COVID-19
3.4. The Positive or Risk Factors of Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, J.; He, W.T.; Wang, L.; Lai, A.; Ji, X.; Zhai, X.; Li, G.; Suchard, M.A.; Tian, J.; Zhou, J.; et al. COVID-19: Epidemiology, Evolution, and Cross-Disciplinary Perspectives. Trends Mol. Med. 2020, 26, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, M.; Putoto, G. COVID-19 in Italy: Momentous decisions and many uncertainties. Lancet Glob. Health 2020, 8, e641–e642. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Christensen, H.; Jorm, A.F.; Mackinnon, A.J.; Korten, A.E.; Jacomb, P.A.; Henderson, A.S.; Rodgers, B. Age differences in depression and anxiety symptoms: A structural equation modelling analysis of data from a general population sample. Psychol. Med. 1999, 29, 325–339. [Google Scholar] [CrossRef]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Kosic, A.; Lindholm, P.; Järvholm, K.; Hedman-Lagerlöf, E.; Axelsson, E. Three decades of increase in health anxiety: Systematic review and meta-analysis of birth cohort changes in university student samples from 1985 to 2017. J. Anxiety Disord. 2020, 71, 102208. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Lam, W.W.; Ng, D.M.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Tian, F.; Li, H.; Tian, S.; Yang, J.; Shao, J.; Tian, C. Psychological symptoms of ordinary Chinese citizens based on SCL-90 during the level I emergency response to COVID-19. Psychiatry Res. 2020, 288, 112992. [Google Scholar] [CrossRef]
- Reardon, S. Ebola’s mental-health wounds linger in Africa. Nature 2015, 519, 13–14. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Prandi, L.; Primiero, G. Effects of misinformation diffusion during a pandemic. Appl. Netw. Sci. 2020, 5, 82. [Google Scholar] [CrossRef]
- Zivin, K.; Eisenberg, D.; Gollust, S.E.; Golberstein, E. Persistence of mental health problems and needs in a college student population. J. Affect. Disord. 2009, 117, 180–185. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef] [PubMed]
- Cyranoski, D. What China's coronavirus response can teach the rest of the world. Nature 2020, 579, 479–480. [Google Scholar] [CrossRef]
- Lasheras, I.; Gracia-García, P.; Lipnicki, D.M.; Bueno-Notivol, J.; López-Antón, R.; de la Cámara, C.; Lobo, A.; Santabárbara, J. Erratum: Lasheras, I.; et al. Prevalence of Anxiety in Medical Students during the COVID-19 Pandemic: A Rapid Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6603. Int. J. Environ. Res. Public Health 2020, 17, 9353. [Google Scholar] [CrossRef]
- Xu, Q.; Mao, Z.; Wei, D.; Liu, P.; Fan, K.; Wang, J.; Wang, X.; Lou, X.; Lin, H.; Wang, C.; et al. Prevalence and risk factors for anxiety symptoms during the outbreak of COVID-19: A large survey among 373216 junior and senior high school students in China. J. Affect. Disord. 2021, 288, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Schalet, B.D.; Cook, K.F.; Choi, S.W.; Cella, D. Establishing a common metric for self-reported anxiety: Linking the MASQ, PANAS, and GAD-7 to PROMIS Anxiety. J. Anxiety Disord. 2014, 28, 88–96. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Dong, L.; Bouey, J. Public Mental Health Crisis during COVID-19 Pandemic, China. Emerg. Infect. Dis. 2020, 26, 1616–1618. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Kmietowicz, Z. Rules on isolation rooms for suspected covid-19 cases in GP surgeries to be relaxed. BMJ 2020, 368, m707. [Google Scholar] [CrossRef]
- Ma, Z.; Zhao, J.; Li, Y.; Chen, D.; Wang, T.; Zhang, Z.; Chen, Z.; Yu, Q.; Jiang, J.; Fan, F.; et al. Mental health problems and correlates among 746 217 college students during the coronavirus disease 2019 outbreak in China. Epidemiol. Psychiatr. Sci. 2020, 29, e181. [Google Scholar] [CrossRef]
- Bigalke, J.A.; Greenlund, I.M.; Carter, J.R. Sex differences in self-report anxiety and sleep quality during COVID-19 stay-at-home orders. Biol. Sex Differ. 2020, 11, 56. [Google Scholar] [CrossRef]
- Vesga-López, O.; Schneier, F.R.; Wang, S.; Heimberg, R.G.; Liu, S.M.; Hasin, D.S.; Blanco, C. Gender differences in generalized anxiety disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). J. Clin. Psychiatry 2008, 69, 1606–1616. [Google Scholar] [CrossRef]
- Basch, C.H.; Hillyer, G.C.; Meleo-Erwin, Z.C.; Jaime, C.; Mohlman, J.; Basch, C.E. Preventive Behaviors Conveyed on YouTube to Mitigate Transmission of COVID-19: Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e18807. [Google Scholar] [CrossRef]
- Walter, D.; Bohmer, M.; Reiter, S.; Krause, G.; Wichmann, O. Risk perception and information-seeking behaviour during the 2009/10 influenza A(H1N1)pdm09 pandemic in Germany. Eurosurveillance 2012, 17, 20131. [Google Scholar] [CrossRef]
- Erku, D.A.; Belachew, S.A.; Abrha, S.; Sinnollareddy, M.; Thomas, J.; Steadman, K.J.; Tesfaye, W.H. When fear and misinformation go viral: Pharmacists' role in deterring medication misinformation during the 'infodemic’ surrounding COVID-19. Res. Soc. Adm. Pharm. 2021, 17, 1954–1963. [Google Scholar] [CrossRef]
- Wang, X.; Hegde, S.; Son, C.; Keller, B.; Smith, A.; Sasangohar, F. Investigating Mental Health of US College Students during the COVID-19 Pandemic: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e22817. [Google Scholar] [CrossRef]
- Zhou, S.J.; Zhang, L.G.; Wang, L.L.; Guo, Z.C.; Wang, J.Q.; Chen, J.C.; Liu, M.; Chen, X.; Chen, J.X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Main, A.; Zhou, Q.; Ma, Y.; Luecken, L.J.; Liu, X. Relations of SARS-related stressors and coping to Chinese college students’ psychological adjustment during the 2003 Beijing SARS epidemic. J. Couns. Psychol. 2011, 58, 410–423. [Google Scholar] [CrossRef]
- Zhong, B.L.; Luo, W.; Li, H.M.; Zhang, Q.Q.; Liu, X.G.; Li, W.T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Tan, W.; Hao, F.; McIntyre, R.S.; Jiang, L.; Jiang, X.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav. Immun. 2020, 87, 84–92. [Google Scholar] [CrossRef]
- Wang, C.; Chudzicka-Czupała, A.; Grabowski, D.; Pan, R.; Adamus, K.; Wan, X.; Hetnał, M.; Tan, Y.; Olszewska-Guizzo, A.; Xu, L.; et al. The Association between Physical and Mental Health and Face Mask Use during the COVID-19 Pandemic: A Comparison of Two Countries with Different Views and Practices. Front. Psychiatry 2020, 11, 569981. [Google Scholar] [CrossRef]
- Yan, T.; Zhizhong, W.; Jianzhong, Z.; Yubo, Y.; Jie, L.; Junjun, Z.; Guangtian, L. Depressive and Anxiety Symptoms among People under Quarantine during the COVID-19 Epidemic in China: A Cross-Sectional Study. Front. Psychiatry 2021, 12, 566241. [Google Scholar] [CrossRef]
- Neil, A.L.; Christensen, H. Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety. Clin. Psychol. Rev. 2009, 29, 208–215. [Google Scholar] [CrossRef]
- Weckesser, L.J.; Dietz, F.; Schmidt, K.; Grass, J.; Kirschbaum, C.; Miller, R. The psychometric properties and temporal dynamics of subjective stress, retrospectively assessed by different informants and questionnaires, and hair cortisol concentrations. Sci. Rep. 2019, 9, 1098. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | All Participants n = 24,678 | No Anxiety n = 22,876 | Anxiety n = 1802 |
|---|---|---|---|
| Sex (%) | |||
| Man | 13,630 (55.2) | 12,693 (55.5) | 937 (52.0) |
| Woman | 11,048 (44.8) | 10,183 (44.5) | 865 (48.0) |
| Place of resident (%) | |||
| City | 4360 (17.7) | 3974 (17.4) | 386 (21.5) |
| Rural | 5063 (20.5) | 4648 (20.3) | 415 (23.0) |
| County-level city | 15,255 (61.7) | 14,254 (62.3) | 1001 (55.5) |
| Worried level (%) | |||
| High | 18,012 (73.0) | 16,340 (71.4) | 1672 (92.8) |
| Moderate/Low/None | 6666 (27.0) | 6536 (28.6) | 130 (7.2) |
| Fear level (%) | |||
| High | 10,796 (43.7) | 9313 (40.7) | 1483 (82.3) |
| Moderate/Low/None | 13,882 (56.3) | 13,563 (59.3) | 319 (17.7) |
| Cognition level (%) | |||
| High | 11,436 (46.3) | 11,436 (46.3) | 783 (43.5) |
| Moderate | 7107 (28.8) | 6566 (28.7) | 541 (30.0) |
| Low | 6135 (24.9) | 5657 (24.7) | 478 (26.5) |
| Behavior Status (%) | |||
| Negative | 6432 (26.0) | 5810 (25.4) | 622 (34.5) |
| Positive | 18,246 (74.0) | 17,066 (74.6) | 1180 (65.5) |
| Questions | n (%) of Correct Responses | |
|---|---|---|
| Knowledge about COVID-19 | ||
| Q1 | Awareness condition | 24,580 (99.6%) |
| Q2 | Timely learning of epidemic news | 24,657 (99.9%) |
| Q3 | The route of transmission | 24,550 (99.3%) |
| Q4 | The correct expression of COVID-19 | 15,124 (61.3%) |
| Q5 | Infectivity | 9363 (37.9%) |
| Q6 | The period of quarantine | 21,586 (87.5%) |
| Q7 | The typical post-infection symptoms | 9414 (38.1%) |
| Q8 | The effective precautions | 10,520 (42.6%) |
| Q9 | The selection of effective protection masks | 16,324 (66.1%) |
| Characteristics | All Participants OR (95%CI) | |
|---|---|---|
| Model 1 | Model 2 | |
| Sex | ||
| Women | 1.00 (ref) | 1.00 (ref) |
| Men | 0.869 (0.789, 0.957) | 1.051 (0.951, 1.162) |
| Place of residence | ||
| Rural | 1.00 (ref) | 1.00 (ref) |
| County-level city | 1.271 (1.129, 1.432) | 1.288 (1.140, 1.457) |
| City | 1.383 (1.224, 1.563) | 1.404 (1.237, 1.595) |
| Worried level | ||
| Moderate/Low/None | 1.00 (ref) | 1.00 (ref) |
| High | 5.145 (4.294, 6.164) | 1.803 (1.467, 2.217) |
| Fear level | ||
| Moderate/Low/None | 1.00(ref) | 1.00 (ref) |
| High | 6.770 (5.932, 7.663) | 5.505 (4.783, 6.337) |
| Cognition level | ||
| High | 1.00 (ref) | 1.00 (ref) |
| Moderate | 1.150 (1.021, 1.294) | 1.104 (0.982, 1.242) |
| Low | 1.121 (1.000, 1.256) | 1.149 (1.016, 1.300) |
| Behavior status | ||
| Positive | 1.00 (ref) | 1.00 (ref) |
| Negative | 1.548 (1.399, 1.714) | 1.596 (1.437, 1.773) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guan, J.; Wu, C.; Wei, D.; Xu, Q.; Wang, J.; Lin, H.; Wang, C.; Mao, Z. Prevalence and Factors for Anxiety during the COVID-19 Pandemic among College Students in China. Int. J. Environ. Res. Public Health 2021, 18, 4974. https://doi.org/10.3390/ijerph18094974
Guan J, Wu C, Wei D, Xu Q, Wang J, Lin H, Wang C, Mao Z. Prevalence and Factors for Anxiety during the COVID-19 Pandemic among College Students in China. International Journal of Environmental Research and Public Health. 2021; 18(9):4974. https://doi.org/10.3390/ijerph18094974
Chicago/Turabian StyleGuan, Jing, Cuiping Wu, Dandan Wei, Qingqing Xu, Juan Wang, Hualiang Lin, Chongjian Wang, and Zhenxing Mao. 2021. "Prevalence and Factors for Anxiety during the COVID-19 Pandemic among College Students in China" International Journal of Environmental Research and Public Health 18, no. 9: 4974. https://doi.org/10.3390/ijerph18094974
APA StyleGuan, J., Wu, C., Wei, D., Xu, Q., Wang, J., Lin, H., Wang, C., & Mao, Z. (2021). Prevalence and Factors for Anxiety during the COVID-19 Pandemic among College Students in China. International Journal of Environmental Research and Public Health, 18(9), 4974. https://doi.org/10.3390/ijerph18094974