Abstract
(1) Background: The aim of this study is to provide a better understanding of the requirements to improve routine health information systems (RHISs) for the management of health systems, including the identification of best practices, opportunities, and challenges in the 53 countries and territories of the WHO European region. (2) Methods: We conducted an overview of systematics reviews and searched the literature in the databases MEDLINE/PubMed, Cochrane, EMBASE, and Web of Science electronic databases. After a meticulous screening, we identified 20 that met the inclusion criteria, and RHIS evaluation results were presented according to the Performance of Routine Information System Management (PRISM) framework. (3) Results: The reviews were published between 2007 and 2020, focusing on the use of different systems or technologies and aimed to analyze interventions on professionals, centers, or patients’ outcomes. All reviews examined showed variability in results in accordance with the variability of interventions and target populations. We have found different areas for improvement for RHISs according to the three determinants of the PRISM framework that influence the configuration of RHISs: technical, organizational, or behavioral elements. (4) Conclusions: RHIS interventions in the European region are promising. However, new global and international strategies and the development of tools and mechanisms should be promoted to highly integrate platforms among European countries.
1. Introduction
High-quality data supporting health management decisions are key to effective governance, leadership, and management [,,,,,]. Informational support for all levels of health management enables planning, policymaking, operational management, and continuous quality improvement []. A health information system (HIS) is a set of components (technical, organizational, behavioral) and procedures “organized to generate information that allows improving health management decisions at all levels of the health system” []. When a HIS produces high-quality, timely, and reliable data, it enables health program managers to monitor, evaluate, and improve health system performance and make evidence-based decisions. This information can then aid decision making, including the prioritization of funding and the allocation of other resources, and to assess which information or sources of in-formation are missing, uncertain, or of low quality []. These data can be used to system-atically explore new ideas, while formulating basic strategies to support them (WHO Eu-ropean Health Information Initiative (EHII)) [].
Healthcare providers routinely collect data on health services, statuses, and re-sources. In turn, public health advisors, hospital and healthcare managers, and ongoing surveys of health facilities also provide information. The data provide a snapshot of the state of health, health services, and health resources. The sources of these data are generally records of services rendered, individual medical records, and records of health resources. They provide information about the health of the patients and the type of treatments and tests they receive. Other information may be collected by managers on human resources, finances, drugs, and supply systems.
Routine medical information may originate from a variety of data sources that include information related to the provision of clinical services (e.g., clinical records, laboratory, and other diagnostic systems service records) and administrative record systems of routine (e.g., staff timesheets), which can be collected during regular periods (daily, monthly, quarterly, annually). A routine health information system (RHIS, also called a health facility and community information system) is any system of data collection, distribution, and use that provides information at regular intervals that is produced through routine mechanisms to address predictable health information needs []. Routine data on health service delivery, utilization, and clinical outcomes are reported more frequently, but an RHIS also includes routine data sets related to other health system functions (human resources management, finance, drug and equipment supply chains, and governance and management) [].
RHISs generate data at regular intervals (one year or less) that have been collected from public and private health facilities and institutions, and community-level healthcare posts and clinics. An RHIS effectively and efficiently supports management decision making if it produces good quality data with timely, relevant, accurate, complete, and accessible information. If this is the case, optimal impact can be achieved in health outcomes and the functioning of health systems. The data produced by RHISs allow evidence-based decisions to be made for the governance and management of health systems and services for planning, monitoring and evaluation, and quality improvement.
An effective RHIS has two main objectives: first, to produce high-quality, routine health information; and second, the effective use of routine health information for decision making [,,]. The ultimate objective of an RHIS is not information for its own sake but to “improve health services management through optimal informational support” []. A robust RHIS can be achieved by improving data production (data quality and accessibility) or data use (the capacity and processes for effective, data-informed decision making).
Given the centrality of routine information to management decision making and the challenge of making decisions when these systems are not optimal, we need to know what works in which settings for RHISs to support health system management decision-making effectively [,,,,]. Synthesized evidence from research studies that evaluated interventions to address this challenge can help offer solutions to improve RHISs, and in turn to strengthen health system management.
An RHIS mainly focuses on high-level information management (national, regional, and district levels) without obligatory feedback to lower levels such as physicians. This stratification is counterproductive because, in cases of emergencies, pandemics, or natural disasters, those health personnel are the first in contact with the population. Thus, RHIS at local, provincial or state, and national levels need to be strengthened, so they can provide relief personnel with up-to-date information for planning [].
RHISs also can assist physicians in making evidence-based decisions to enhance the local health system’s performance. Positive health outcomes can be improved with the right implementation of an RHIS at both the hospital and primary care levels []. An optimally functioning RHIS could remove obstacles between individual care and public health information systems, ultimately improving individuals’ health statuses and strengthening the global health system with more effective and efficient management and planning.
The Performance of Routine Information System Management (PRISM) framework is an innovative approach to designing, strengthening, and evaluating RHIS performance by incorporating organizational, technical, and behavioral determinants of performance []. The PRISM framework identifies two main functions of an RHIS and three key domains that are influential in shaping RHIS. The two main functions of an RHIS are the production of quality data and the effective use of data for decision making. These three key domains also represent areas for improving RHIS:
Technical: Technical interventions to improve an RHIS are usually intended to improve the design and the technical aspects of the RHIS, such as the usefulness and functionality of registers and computer hardware and software.
Behavioral: Behavioral interventions aim to improve staff motivation and skills to collect, extract, and use data effectively.
Organizational: Organizational interventions are meant to strengthen organizational rules, values, and support practices aimed at building a culture of data use for decision making.
RHIS interventions can address any of the components described in the PRISM framework [,]. An example of using multiple data streams for disease surveillance is influenza surveillance [].
In this systematic review, we recognize that reliable health information and data that are embedded in a fully functioning and high-quality HIS form the foundation for sound decision making in healthcare and are essential for health system policy development. The aim of this systematic review is to provide a better understanding of the requirements to improve RHIS for the management of health systems, including the identification of best practices, opportunities, and challenges in the 53 countries and territories of the WHO European region.
The article makes a new contribution, from a number of perspectives, to the literature on this topic. Firstly, a systematic review of mostly Europe-centered literature is performed, taking into consideration the multidimensional set of routine practices undertaken within the HIS context. This has involved the conceptualization and delimitation of RHIS within the HIS family. Moreover, a PRISM framework approach has been taken to the literature review. This framework is widely used in the literature on the topic of HIS technologies but is rarely used within the context of RHIS. In this regard, a set of drivers and, in particular, barriers have been identified. These barriers limit the use of RHIS and the generation of RHIS-based outputs and outcomes. Lastly, this review makes a unique contribution because it supplements the results identified in the literature in two ways. First, it analyzes the link between RHIS and new health management systems based on big data or machine-learning behavior prediction algorithms. Second, it reflects on how RHISs have helped in managing the COVID-19 pandemic.
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
This study is a systematic review of reviews that assessed “data collection” and “health information system assessments” with a focus on routine health information systems (RHISs). The study was conducted in accordance with the AMSTAR 2 [] checklists and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [] to ensure the quality of the review and the methodological considerations when using existing systematic reviews. It has been conveniently registered in the PROSPERO database with the number CRD42020207267. The risk of bias was assessed, and disagreements regarding bias and the interpretation of results were resolved by consensus discussions.
A literature search was performed using MEDLINE (accessed through PubMed), Cochrane (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Database of Abstracts of Reviews of Effects, National Health Service Economic Evaluation Database), EMBASE, and Web of Science electronic databases in August 2020, using the following set of keywords:
Routine Health Information Systems:
“Health informatics” [TIAB] OR “health information system *” [TIAB] OR “hospital information system *” [TIAB] OR “management information system *” [TIAB] OR “ambulatory care information system *” [TIAB] OR “clinical laboratory information system *” [TIAB] OR “clinical pharmacy information system *” [TIAB] OR “radiology information system *” [TIAB] OR “medical order entry system *” [TIAB] OR “health information management” [TIAB] OR “decision support system *” [TIAB] OR “health information exchange” [TIAB] OR “interoperability” [TIAB] OR “information system *” [TIAB] OR “medical informatic *” [TIAB] OR “dental informatic *” [TIAB] OR “health information” [TIAB] OR “nursing informatic *” [TIAB] OR “public health informatic *” [TIAB] OR “medical record *” [TIAB] OR “electronic health record *” [TIAB] OR “personal health record *” [TIAB] OR “individual health record *” [TIAB] OR “RHIS” [TIAB] OR “routine health information system *” [TIAB] OR “eHealth” [TIAB] OR “e-Health” [TIAB].
WHO European region (53 countries and territories):
“Albania” [TIAB] OR “Andorra” [TIAB] OR “Armenia” [TIAB] OR “Austria” [TIAB] OR “Azerbaijan” [TIAB] OR “Belarus” [TIAB] OR “Belgium” [TIAB] OR “Bosnia and Herzegovina” [TIAB] OR “Bulgaria” [TIAB] OR “Croatia” [TIAB] OR “Cyprus” [TIAB] OR “Czechia” [TIAB] OR “Denmark” [TIAB] OR “Estonia” [TIAB] OR “Finland” [TIAB] OR “France” [TIAB] OR “Georgia” [TIAB] OR “Germany” [TIAB] OR “Greece” [TIAB] OR “Hungary” [TIAB] OR “Iceland” [TIAB] OR “Ireland” [TIAB] OR “Israel” [TIAB] OR “italy” [TIAB] OR “Kazakhstan” [TIAB] OR “Kyrgyzstan” [TIAB] OR “Latvia” [TIAB] OR “Lithuania” [TIAB] OR “Luxembourg” [TIAB] OR “Malta” [TIAB] OR “Monaco” [TIAB] OR “Montenegro” [TIAB] OR “Netherlands” [TIAB] OR “North Macedonia” [TIAB] OR “Norway” [TIAB] OR “Poland” [TIAB] OR “Portugal” [TIAB] OR “Moldova” [TIAB] OR “Romania” [TIAB] OR “Russia” [TIAB] OR “San Marino” [TIAB] OR “Serbia” [TIAB] OR “Slovakia” [TIAB] OR “Slovenia” [TIAB] OR “Spain” [TIAB] OR “Sweden” [TIAB] OR “Switzerland” [TIAB] OR “Tajikistan” [TIAB] OR “Turkey” [TIAB] OR “Turkmenistan” [TIAB] OR “Ukraine” [TIAB] OR “United Kingdom” [TIAB] OR “Uzbekistan”.
The search was restricted to systematic reviews, by publication date (from 1 January 2000 up to 15 August 2020), and by publication language (English and Spanish).
2.2. Study Selection
The systematic review includes data from reviews that covered any practice targeting any component or dimension of an RHIS, with at least one component related to health services performance or management in at least one WHO European country or territory. Exclusion criteria were (1) studies written in languages other than English, and those for which the full text was not available online; and (2) conference abstracts.
Initial screening was based on titles and abstracts by three researchers (J.J.P.-R, J.T.-S., and F.S.-R.). Disagreement on bias assessment and the interpretation of results was resolved by two investigators (D.N.-O. and H.E.). Abstracts lacking information were retrieved for full-text evaluation. Subsequently, the same investigators independently evaluated full-text articles and determined eligibility. Disagreement on bias assessment and the interpretation of results was resolved by consensus discussions. Authorship, journal, and years were not blinded.
2.3. Data Extraction and Quality Assessment
Three investigators conducted data extraction following standardized criteria, and results were reviewed by two senior researchers. The following data were extracted: journal, publication year, databases searched, time period, setting, system or technology, data type and collection, intervention type, number of studies, total number and countries of patients, study design, whether a review of systematic reviews or meta-analysis or bibliometric analysis was performed, outcomes, lessons and barriers for implementation, main results, main limitations, implications: challenges and opportunities, and information systems evaluation (see Tables S1 and S2 in Supplementary Materials).
3. Results
A flow chart of the literature search and study selection results is shown in Figure 1. The first database search resulted in 45,614 articles; the updated search resulted in 280 articles. After exclusion of duplicates, 249 articles were screened, and 196 were excluded. Full texts of 53 eligible articles were reviewed. Out of these, 33 were excluded for not meeting the criteria relating to study type, intervention, or outcome. The 20 remaining studies were included in this systematic review.
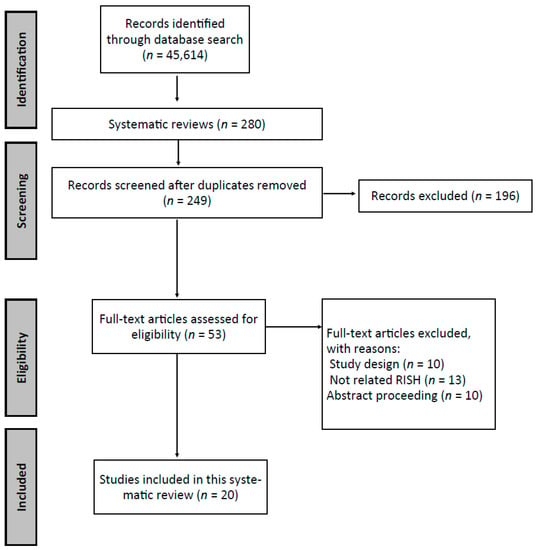
Figure 1.
Flow of information through the different phases of the systematic review.
3.1. Descriptive Analysis of the Systematic Reviews
3.1.1. General Characteristics of Reviewed Papers
The 20 systematic reviews included in our review were published between 2007 and 2020 in 12 unique journals. In these reviews, systematic literature searches were performed from 1974 to 2019, and all reviews were international (covering between 3 and 14 countries). The system or technology analyzed was varied, the most frequent being general ICT systems, medical health records, automated alert and reminder systems, and support systems for clinical decision making. The most frequently applied setting on which the technology focused and aligned were hospital care, primary care, and emergency services; two studies focused on aging, and one on AIDS and hypertension.
Almost all the studies included a multidatabase search, except for Anker et al., who only searched PsychInfo [], and Marschollek, who searched PubMed []. The number of studies included in the systematic reviews ranged between 4 and 99, the majority between 20 and 40 studies. Only 2 of the 20 systematic reviews also included a meta-analysis [,] (see Table S1 in Supplementary Materials).
The studies included in the systematic reviews were diverse. Most included both randomized and nonrandomized clinical trials, including retrospective case series, case–controls, descriptive cohorts, and qualitative studies.
3.1.2. Aims
Most of the reviews aimed to analyze the impact of interventions on the outcomes of the professional (readmission), centers (drug alerts, patient decisions), or of the patients (independent aging, healthy behaviors). Some studies analyzed factors that generally influenced practitioners in the use of patient data collection applications. One article explored the barriers and facilitators in the use of health information exchange systems.
3.1.3. Intervention
The reviews included studies with interventions based on different technologies or systems. Most of the studies were based on EHR and contextual patient information in intensive and emergency care [,,]; ambulatory or primary care [,,]; healthcare settings, including hospitals []; patient results, performance, and safety []; and prescription alerts via EHR []. Other systems evaluated were health smart homes (HSHs) and home-based consumer health (HCH) for the activity of elderly people [], and clinical decision support for the management of AIDS []. Other reviews included combinations of several systems, such as CDSS, computerized provider order entry (CPOE), and electronic prescribing [,]. Lastly, some reviews analyzed generic RHISs [,] (see Table S1 in Supplementary Materials).
3.2. Outcomes
The reviews naturally showed variability in results in accordance with the variability of interventions and target populations. Studies that focused on evaluating an intervention generally show weak evidence in favor of its use. This occurs, for example, in the Arditi [] reminder study, in which they concluded that reminders to professionals can probably improve the quality of care in various contexts and under various conditions. Even studies about some interventions, such as technologies for independent aging [], did not find strong evidence to support the technology.
Some reviews analyzed the use of different clinical information systems in different settings [,,,,,,,]. These will likely provide the most encouraging results. Several studies conclude that using an RHIS makes it possible to improve efficiency both in management (reduction of missed appointments, waiting times, etc.) [] and for clinicians (better communication with patients and colleagues, patient information in real time), which allows better coordination, decision making, and health outcomes [,].
Some studies value RHISs as administrative, public health, or epidemiology tools and also consider them useful assets for various medical specialties such as emergency and critical care in hospital medicine or primary care (GP clinics) [,,,,,]. Studies also analyzed communication systems between patients and healthcare workers, particularly nurses. From the results obtained, ICTs showed to improve the nurse–patient relationship and increase empowerment, knowledge, well-being, and even the state of health [].
A study analyzed the employment of health-smart homes (HSHs) and home-based consumer health (HCH) technologies to support aging at home [], but due to the design and quality of the studies—sample sizes, etc.—there was insufficient evidence to support the role of these systems in improving independent living in the homes of the elderly. The systems used in monitoring older adults do not adequately collect or are not designed for the purpose of being assessed by an RHIS. The collected data mostly reflects the patient’s current status and is then discarded [].
Baysari et al. used information technology as decision-making support systems integrated into EMR decisions for prescribing antibiotics []. These systems can help improve the use of antibiotics in the hospital environment. However, there is mixed evidence of the impact on final health outcomes such as mortality or length of stay. Great variability was also found in the designs of the studies; therefore, more evidence is needed to conclude that these systems can help organizations improve their prescribing. Bayoumi et al. also evaluated computerized alerts to improve prescribing []. Analyzed results showed a reduction of adverse events and hospitalization; clinical outcomes such as reduction in hypoglycemia and optimization in the maintenance of INR in therapeutic range for anticoagulants; and finally, changes in prescription behavior, which had the most immediate impact and evidence. This means that an RHIS can also affect medical audits by validating probable errors in medication [], laboratory results [], undeclared medication side effects [], etc.
The use of different software applications for data collection [] and the hesitancy to share health data with competitors []—especially in countries where health systems are private—are major drawbacks in global data generation. Hence, it should be recognized that RHISs follow strong privacy and safety protections for ethical use and collection of useful information. Unfortunately, some information sources such as EHR failed to present adequate or correctly used data []; in some cases, doctors inputted data poorly because of low computer literacy []. With these problems solved, RHISs would also be useful for improving access to information by making it more visible and contextualized []. Educating health personnel on the correct management of EHRs could alleviate this problem [,].
Other initiatives, such as the development of strategic frameworks, clinical leadership that values technology skills [,], financial resources for training [], and the development of strategies to overcome resistance to change in health personnel [,] could improve the RHIS’s ability to gather better information.
Another group of interventions analyzed focused on ICTs in general, as well as the use of the internet and social media [,,].
Effective RHIS function requires the interaction between physicians, technical personnel, technology, the clinical environment, and the social system to work [], along with the correct data input, adequate policies, and leadership from key players in the system. Table S3 in Supplementary Materials shows an overview of the attributes of the dimensions of success measured in the 20 systematic reviews.
3.3. Areas for Improvement for RHISs According to the PRISM Framework
To evaluate RHIS, we used the PRISM framework. This conceptual framework hypothesizes that technical, behavioral, and organizational determinants (inputs) influence data collection, transmission, processing, and presentation (Table 1). These, in turn, influence data quality and use (outputs), which include technical, organizational, and behavioral aspects related to the effective use of information for decision making (Table 2), health system performance (outcomes), and ultimately, health outcomes that represent a health impact (Table 3) []. According to the three determinants of the PRISM framework that influence the configuration of RHIS (technical, organizational, or behavioral elements) we have found the following areas for improvement for RHISs.

Table 1.
Data collection tools + data flow systems.
Table 2.
New electronic data systems + motivation, training, and support.
Table 3.
Use-related data for service improvements.
Regarding the inputs, the literature review shows that there is a set of actions that could foster more efficient and effective use of RHISs. Firstly, the use of contextual frameworks or theoretical models would enable an analysis of RHIS use-related behavior to be performed. One of the problems identified in the literature is the lack of theoretical references in the explanation of RHIS acceptance by healthcare professionals [,]. Linked to this first element, the review has also highlighted the need for a much better connection between RHIS use and people’s skills and organizations’ abilities [,,,,,]. Relationships of complementarity between RHIS, healthcare professionals’ competencies and skills, and less bureaucratic organizational forms that are better adapted to evidence-based decision making [,,,] are also especially important when it comes to fostering RHIS use. Additionally, third, from the input perspective, the literature also highlights the need to overcome the technical and technological limitations that undermine the effective use of RHISs [,,]. Among such limitations are problems associated with connectivity, bandwidth, usability, and interoperability between systems [].
Regarding RHIS use-related outputs, the review also points to a set of elements that could facilitate more effective uses and returns. Firstly, a whole set of elements linked to data management has been emphasized. The management of privacy, security, and confidentiality of RHIS health data input and output is of vital importance []. Within this context, the importance of developing confidentiality protocols that are compatible with the use of data for evidence-based decision making has been noted []. In addition, issues linked to the security and adaptability (e.g., to generational preferences [,,]) of RHIS input data collection and storage devices have also been emphasized [,].
Regarding RHIS outcomes, the literature review also offers some relevant conclusions. First, it is important to note that, despite the importance of using RHIS to support evidence-based decision making in health systems, the available evidence on its outcomes is very limited to analyses of effectiveness in specific areas [,,]. There is little evidence of findings on the effects of RHIS use for health systems as a whole [,,,,]. Second, and taking into account the reluctance to use RHISs and the limitations of the information obtained from them, the review also highlights the need to incorporate the needs of professionals who use RHISs [,,]. Once again, this leads us to the question of relationships of complementarity with people and organizations [,]. To ensure that RHISs have efficient and effective outcomes, it is vital to consider both healthcare professionals’ digital competencies and information management skills, as well as a flattening of organizational hierarchies and “top-down” mechanisms [,,].
4. Discussion
RHISs are an evolution of HISs. Much broader in scope, they are complex, nested systems for health data collection and management. The novelty of RHISs rests on two main elements: the regularity of data captured and the effective use of these data for decision making. With these two novel elements, RHISs facilitate data production and enable isolated data-driven decisions to be made. The aim is to provide support for integral decision making in healthcare through information systems containing regular, optimal data.
To evaluate RHISs, we used the PRISM framework. This conceptual framework is useful for evaluating the effectiveness of an RHIS by defining and relating its inputs, outputs, and outcomes. The PRISM framework draws a flow diagram in which:
- Based on an intervention in the HIS, a set of technological, organizational, and behavioral drivers and barriers arise;
- The interaction between the intervention and the drivers and barriers generates RHIS inputs, i.e., the data that will be used. To achieve this, the data’s needs, production, availability, and use requirements must be precisely defined;
- Once the data have been generated, they are transformed into RHIS outputs, to the extent that they can generate high-quality health information, and then that health information is used effectively for decision making;
- Once health information has been generated and used effectively, the RHIS is ready to generate outcomes, i.e., the results of its implementation. In general, these results refer to the effectiveness of either the information system itself or the health system in general. The ultimate intention is to improve citizens’ health statuses.
Through PRISM and a systematic literature review of 20 scientific articles that reviewed the literature on the various practical dimensions of HISs, we reached the following main conclusions:
4.1. Inputs
We have found four key aspects that need to be improved:
First, RHISs need to incorporate new underlying frameworks to predict behaviors for adoption and use. In this context, and with regard to modeling, it would be useful to have updates of the unified theory of acceptance and use of technology (UTAUT) [], the theory of planned behavior (TPB) [,], the theory of diffusion of innovations (DOI) [], and the theory of organization and environment (TOE) []. These frameworks have all been used in literature that investigates the motivations for the use of technology in various contexts, including healthcare [,,,,,].
Second, the usability and interoperability between RHISs and their ability to connect with each other need to be improved considerably. In addition, the choice of the HIS provider is key for their subsequent development. In this respect, health organizations must gain a better understanding of the information systems market in general and the HIS market in particular.
Third, the changing nature of information systems and technology use suggests improvement in some aspects of organizations. One example is training professionals in digital skills, in information systems in general and HIS in particular, such as training physicians to input data more accurately into the EHR. Medical professionals must prioritize developing skills in transformational leadership and management of healthcare organizations, crucial to overcoming probable resistance present in some healthcare professionals. Additionally, collaborative networks must be created between technical and healthcare professionals in the context of HISs. Furthermore, organizational culture must be developed among healthcare personnel to make evidence-based decisions in healthcare organizations, and, in particular, in the evaluation of healthcare policies. Additionally, organizations must establish investment-financing mechanisms because of the economic effort involved in developing and maintaining RHISs, including public–private partnerships and learning from the experiences of other sectors. Furthermore, it is advisable to promote connections between medical science systems and information systems and technologies. The connection between medical research and the medical device market is well developed, but the same cannot be said for the connection between medical research and HIS development. Connecting the medical research, technology, and management sectors is crucial for the efficient and useful development and implementation of RHISs. In this sense, the creation of a specific training agreement would be useful. Finally, operational groups and tasks of the data scientists office (DSO) must be incorporated into health organizations and public health policy evaluation teams.
Fourth, RHISs also have information and communication infrastructure requirements. However advanced the HIS might be, it cannot be effective within contexts with connectivity and bandwidth problems. In this regard, 5G technology offers possibilities.
4.2. Outputs
Issues of privacy, confidentiality, and security of the data generated and used in RHISs are of vital importance. RHISs should reinforce the protocols ensuring that any data obtained are used confidentially and securely, without limiting their potential to be used to improve decision making in healthcare.
The emergence of big data and data-driven management is a great opportunity for RHISs. Unlike earlier methods, big data allows initially unstructured mass data to be collected and processed. For example, through social listening methodologies that can be matched to clinical and behavioral data, healthcare management can have access to broader, more accurate, and robust information about any dimension of health. This is especially important in the acute management of situations such as the coronavirus pandemic, where an immense amount of patient data is being recorded that cannot feasibly be reviewed manually. A good structured and reliable system could be extremely useful for the prevention of the disease in obtaining data to avoid spreading, appropriate diagnosis, and diagnostic possibilities of proven benefit. Big data is also well known as a health management tool to prevent future risks, reduce unnecessary expenses, decrease health disparities, and encourage efficient use of material (antibiotics, beds, medications, etc.) []. However, without the data to generate it, its use becomes aspirational. For physicians, this tool can provide valuable information to guide options for certain patients, as shown in a study-oriented on the critical patient that observed that numerous systems can predict a wide variety of health conditions []. However, most of these studies were single-center studies, which limited the generalizability of results and conclusions.
The combination of RHIS and big data is especially useful for the analysis and evaluation of the health problems of, and policies for, specific groups, particularly the chronically ill and elderly. We must adapt the information technology or system to the specific needs of each group. For example, chronically ill young people might prefer wearables, whereas a combination of face-to-face care and virtual follow-up would work better for older patients. Not all technologies or information systems are equally effective for the management of health problems. Consequently, the training of health personnel accompanied by the development of appropriate programs may allow the data obtained from smart homes and wearable devices to be dedicated to casual or sporadic monitoring and be a valid source of data for establishing global strategies for specific groups.
The difficulty that older adults have in handling technology is widely known, often due to unclear instructions or poor support, and hence, their perceptions of technology must be recorded to maximize and facilitate its use in their daily activities []. Therefore, the data obtained from smart homes, especially those where the elderly reside, become vital to evaluate because projects can be created that allow them to better manage their problems, complications, and even comorbidities. However, a study [] that focused on elderly individuals found limitations in the technologies and also found that their main use is monitoring healthcare and not as an intermediary for information.
4.3. Outcomes
While an array of partial evidence shows how certain HISs, PHRs, or clinical decision support (CDSS) technologies and systems have positive impacts on the effectiveness of health systems, joint (multiple information systems), representative, and longitudinal evidence from population samples is very scarce. Social research into the health, organizational, and healthcare policy effects of RHIS use should be considerably expanded. It is especially important to consider the relationships of complementarity between RHIS and the technologies of the second digital wave, such as big data or data-driven management, artificial intelligence (AI) and machine learning, and collaborative platforms, among others.
The implementation of information technologies and digital systems in healthcare tends to be rejected by the general public. This rejection is linked to the generalized idea that investment in these systems is made to the detriment of investment in people who provide face-to-face care to others (the classic model of health care). RHIS implementation is often top down, and this is rejected by professionals and patient associations, who perceive that technology is being prioritized over people. Consequently, the opinions of professionals on the timing of the RHIS implementation must be incorporated and complement the launch with the necessary information technology and IS support. Crucially, the neutrality of the technology can be affected by the implementation of a specific technique. RHIS implementation should occur while considering the maximization or minimization of any foreseeable positive or negative effects. On the other hand, we must work on the permeability and connection of health organizations regarding RHIS and its justification and explanation to society about its needs and benefits for health systems. As with other information technologies and systems, the effective implementation of an RHIS is not possible unless there is general acceptance by its potential users (healthcare professionals and the general public).
RHISs represent major cultural changes for healthcare professionals and the general public. RHISs are not developed in isolation. Rather, they are a more effective instrument for organizations and healthcare policy to promote citizen empowerment regarding their own health. Empowered by multiple practices of information generation and digital communication in healthcare, citizens seek to be cared for in accordance with new criteria governing the doctor–patient relationship, which no longer needs to be the traditional passive one. At the same time, many citizens, mainly—though not solely—older ones, will still seek traditional services. RHIS can be useful for segmenting these different needs into personal categories depending on the health status of individuals and for developing different care methodologies and policies.
RHISs also offer significantly innovative and disruptive alternatives for health system organizations. Within this context, complementarity between RHIS, big data, and AI is especially important for the development of digital health platforms. Digital spaces can provide infinite possibilities for agents to connect with one another, in which the traditional separation between the roles of professional and patient becomes blurred and the limitations of place, time, and connection between equals are largely overcome. Moreover, 20th-century hospitals and primary care centers may be partially replaced by 21st-century digital health platforms. These platforms would serve as digital intermediaries between healthcare or wellness providers (not necessarily healthcare professionals), and those seeking healthcare.
4.4. Efficiency of RHISs in the Prevention/Treatment of COVID-19 Transmission
The development of an RHIS intervention would also be useful during the COVID-19 pandemic. That is because the pandemic has generated a series of new data (data related to procedures, trips, the movement of people, immigration, etc.) on top of the data already existing in health systems. Thus, through digital surveillance evidence and unstructured data profiling, this new and large amount of raw data can be turned into useful big data. These data must also be represented in RHISs in order to make better decisions and to take advantage of other data generated by digital sources (e.g., social media, train routes, Google Trends, etc.). Thus, using the data obtained by RHIS, it would be possible, for example, to examine patterns of use in selected health services. This is the case of Singapore, where the data obtained by RHIS were used to predict the health service use levels and thus better understand the pattern and magnitude of the COVID-19 effect on the use of certain services []. Bangladesh used prepandemic RHIS to develop a model that would predict total health service utilization, including an estimate of health service use levels if the pandemic had not occurred []. This should provide very important data to assess costs and develop health policies based on the results, compared to those obtained by RHIS in the current pandemic. In China, a similar system was used to quantify the effect of the COVID-19 pandemic on the use of health services. In this case, detailed monthly data were used, which included data for previous years, for the year the pandemic started, and even for the periods after the various waves of the pandemic. These analyses show that RHIS data are of great significance for timely and effective tracking of the performance of the health system in low- and middle-income countries [].
RHISs could be useful for COVID-19 surveillance. In Bulgaria, contact tracing has been implemented by RHIS. Therefore, when someone who has had close contact with a person with confirmed COVID-19, he or she is registered and has to be tested [].
WHO has incorporated RHIS data standards into key projects such as immunization, HIV, malaria, tuberculosis, and reproductive, maternal, newborn, child and adolescent health (RMNCAH), and continues to include other data in its own digital health package to be able to report health data that has proven to be a key need [], especially in the era of the COVID-19 pandemic. However, not everything is perfect in the use of RHIS in relation to COVID-19. For example, an RHIS may not be able to capture the full impact of the COVID-19 epidemic in populations that have health services that do not report data to it (nongovernmental or religious organizations), or in those in which health services are provided by the private sector. In addition, many countries (especially low- and middle-income ones) do not have systems in place for the routine assessment of data quality. These systems are often beset with data entry errors and with an inconsistent application of reporting definitions, due to a failure to use standards [].
4.5. Policy Implications
In 2015, the WHO Regional Office for Europe developed a tool to guide the assessment of HISs and the development of a national health information strategy []. According to a survey of European members, it was agreed necessary and desirable to improve the integration of HISs at the national level. Better sharing of these health data allows for more and better comparative health research, international benchmarks, and national and EU-wide public health monitoring []. However, some countries lack the resources to implement the program properly or even specify the financial resources for the preparation of the program in the budget, which may challenge the desired integration. Participants in one study mentioned various other challenges that have different relevance to countries, such as data availability, opportunities for linking data sources, legal restrictions, technical restrictions, and institutional issues [].
Several European nations are considered leaders in the use of electronic medical records (especially in primary care). In these, HISs have been used for much longer than in other nations of the world []. Nevertheless, RHISs continue to display a gap between recording, reporting, and the effective use of data; therefore, strengthening RHISs has become a global priority for tracking and addressing national health goals []. The operations of RHISs in low-income countries fall below the globally expected standard due to the production and use of poor quality data, or to not using high-quality data to make informed decisions [,]. Despite investment in RHISs in low- and middle-income countries, several problems still persist (technical, organizational, financial), thus preventing proper use of RHIS (incorrect data and nonuse of data already in the system) []. The use of RHISs in various low-income countries in Latin America and in Africa is associated with the most significant local public health problems, such as interventions to improve maternal and newborn health [], or to reduce communication delays and improve quality of care via a tuberculosis laboratory information system in Peru []. RHIS data from the research and health policy community in Mozambique will help build sustainable long-term capabilities to manage and evaluate health conditions effectively []. In Ethiopia, the Ministry of Health and the Bill & Melinda Gates Foundation (Bill & Melinda Gates Foundation) launched “Operational Research and Coaching for Analysts” (ORCA) as a method for developing data collection and reporting [].
Despite a large number of studies and reviews on HISs, contradictory results continue to be evidenced. This is because some parts of the systems are unpredictable, such as the users, the flow of information, and the settings []. Even if they present a number of problems, RHISs can help to strengthen policy decision making in local health systems, especially in low-income countries. Therefore, it is necessary to establish a suitable strategy based on the digitization of data processing, which allows indicator use to be simplified and reports to be saved and delivered, thus leading to a modern and effective data use structure.
To establish improvement strategies, it is necessary to know what the current problems and weaknesses in the evaluated studies are. Indeed, we can find various aspects in need of improvement within them, including the lack of a strategy for RHIS system implementation and evaluation [,]; the lack of financial, personnel, and equipment resources, making it impossible to correctly collect data capable of providing the best results [,,]; data capture systems (software) that are not intuitive enough and require extra training, which hinders their use [,,] and causes rejection by their users (especially doctors) [,,]. Moreover, the lack of interoperability between systems (medical records, databases, etc.) further complicates the proper use of data [,,,]. Without adequate planning to overcome poor communication between technical, administrative, and health personnel [], the results obtained from such data are only able to give an overview that is of little benefit to local entities [,,,,].
By identifying such problems, strategies can be established to solve them. These strategies should be established and grouped by the specific determinants found: technical, organizational, and behavioral []. The reason for doing so is that it is practically impossible to generalize an answer within a single overall strategy.
Technical strategies: The records must be simplified in a standardized way to facilitate data entry. Ideally, creating intuitive software is an excellent choice that may even increase user acceptance. The development of tools to improve the results of poor RHIS data has been described in other studies with good results []. These tools could even allow data availability and usability to be improved (by both uploading new data and reviewing data that is already available), possibly by using cloud storage services to enable easy access from anywhere and by having a common standard that allows for interoperability of systems in different locations.
Organizational strategies: The management of resources is essential, of both those available and those needed, and that is why it is very important to have a protocol for project implementation before any project is actually carried out. It is necessary to assess what can be achieved with the financial and human resources that are presently available, as well as the possibility of making improvements by obtaining new resources. To solve organizational problems, projects must be correctly established from the start. This should include follow-up measures (based on variables) and evaluation so that any post-evaluation improvements can be made so as to enhance the use of the data obtained. In addition, the possibility of establishing a project monitoring and evaluation director position should be considered. This is because leadership within projects such as these is essential to guide, monitor, and resolve any issues that team members may have. These teams must be made up of professionals from the various areas participating in the project since this will help to create the right tools, which should be useful to all potential users, and also be easy to use.
Behavioral strategies: These aim to improve the staff members’ competence and motivation to collect, extract, and use data effectively []. One of the most commonly encountered problems is the participants’ (mostly health practitioners’) refusal to use an RHIS because they consider that using a new tool will not bring any benefits. This can be resolved through educational interventions to show the benefits of RHISs and by training staff to use them properly. These actions have been shown to improve staff members’ abilities to use data []. Here, a leadership figure is very important for the purpose of providing guidance during project rollout. This is because workshops and educational interventions do not always achieve the expected results, whereas the combination of leadership and motivation can have a powerful behavioral and organizational impact on data improvement [].
In order to achieve the integration of issues, it is important to clearly understand what should be integrated, how it should be integrated, what activities should be considered, and the benefits that can be obtained. Through current technological advances, certain basic information system improvements can be demonstrated (providing quality data, data recordkeeping, legislative and technical infrastructure, and personnel improvements) that promote process integration in Europe. To accomplish this, proper leadership and good management are key to improving RHIS architecture and infrastructure [].
4.6. Limitations
Although this systematic review was conducted according to the suggested methodology, we acknowledge that our study has some limitations. We searched four databases and focused only on systematic reviews, meta-analysis, and bibliometric analysis. Consequently, our search may not be exhaustive. On the other hand, the inferior quality scores based on AMSTAR-2 tools might reflect incomplete reports rather than unqualified review methods (see Table S4 on Supplementary Materials). Finally, the large number of publications required an optimized approach. However, we have ensured transparency by clearly outlining the process followed in the Methods Section. Therefore, we expect this review will only serve as a temporary system review and can be further updated as needed.
5. Conclusions
The use and development of plans for RHIS at the national level in European countries would also be desirable at the continental level. Our research is based on a variety of available related articles, showing the possibility of coordinating work in various areas and creating integrated recommendations.
Some strategies have been developed. However, some countries in the European region are still not working in concordance with the development of RHIS, including legislatively. To alleviate this obstacle, new global and international strategies should be planned, and the development of tools and mechanisms should be promoted in order to highly integrate platforms among European countries.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph18094622/s1. Table S1. Summary of included studies’ characteristics. Table S2. Summary of included studies’ results. Table S3. Attribute of different success factors. Table S4. Quality assessment judgment using the AMSTAR 2 tool.
Author Contributions
Conceptualization, D.N.-O., N.A.-M., F.S.-R. and J.J.P.-R.; methodology, D.N.-O., F.S.-R., J.J.P.-R. and J.T.-S.; validation, D.N.-O., F.S.-R. and J.J.P.-R.; formal analysis, F.S.-R., J.J.P.-R., J.T.-S. and H.E.; writing—original draft preparation, F.S.-R., J.J.P.-R., J.T.-S. and H.E.; writing—review and editing, D.N.-O., N.A.-M., F.S.-R. and J.J.P.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No additional data available.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AI | Artificial Intelligence |
| AIDS | Acquired Immunodeficiency Syndrome |
| AMSTAR | A Measurement Tool to Assess Systematic Reviews |
| CAAS | Computerized Antimicrobial Approval Systems |
| CDSS | Clinical Decision Support System |
| CIS | Clinical Information System |
| CPOE | Computerized Provider Order Entry |
| DOI | Theory of Diffusion of Innovations |
| D-RHIS | Disease-specific RHIS |
| DSO | Data Scientists Office |
| EHII | European Health Information Initiative |
| EHR | Electronic Health Records |
| EMR | Electronic Medical Records |
| GP | General Practitioner |
| HCH | Home-based Consumer Health |
| HCI | Human–computer Interaction |
| HIE | Health Information Exchange |
| HIS | Health Information System |
| HIT | Health Information Technology |
| HIV | Human Immunodeficiency Virus |
| HSH | Health Smart Homes |
| ICT | Information and Communications Technology |
| INR | International Normalized Ratio (prothrombin time) |
| I-RHIS | Integrated RHIS |
| IT | Information Technology |
| LTC | Long-Term Care |
| PHR | Personal Health records |
| PRISM | Performance of Routine Information System Management |
| RHIO | Regional Health Information Organizations |
| RHIS | Routine Health Information System, Regional Health Information System |
| SS | Surveillance Systems |
| TOE | Theory of Organization and Environment |
| TPB | Theory of Planned Behaviour |
| UTAUT | Unified Theory of Acceptance and Use of Technology |
| WHO | World Health Organization |
References
- WHO. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Health Metrics Network & World Health Organization. Framework and Standards for Country Health Information Systems, 2nd ed. 2008. Available online: https://apps.who.int/iris/handle/10665/43872 (accessed on 9 April 2021).
- Dixon-Woods, M.; Redwood, S.; Leslie, M.; Minion, J.; Martin, G.P.; Coleman, J.J. Improving Quality and Safety of Care Using “Technovigilance”: An Ethnographic Case Study of Secondary Use of Data from an Electronic Prescribing and Decision Support System. Milbank Q. 2013, 91, 424–454. [Google Scholar] [CrossRef]
- Riley, P.L.; Zuber, A.; Vindigni, S.M.; Gupta, N.; Verani, A.R.; Sunderland, N.L.; Friedman, M.; Zurn, P.; Okoro, C.; Patrick, H.; et al. Information systems on human resources for health: A global review. Hum. Resour. Health 2012, 10, 7. [Google Scholar] [CrossRef]
- Willis, C.D.; Riley, B.L.; Herbert, C.P.; Best, A. Networks to Strengthen Health Systems for Chronic Disease Prevention. Am. J. Public Health 2013, 103, e39–e48. [Google Scholar] [CrossRef]
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Morton, S.C.; Shekelle, P.G. Systematic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care. Ann. Intern. Med. 2006, 144, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Lippeveld, T.; Sauerborn, R.; Bodart, C.; World Health Organization (Eds.) Design and Implementation of Health Information Systems; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- European Health Report 2018: More than Numbers—Evidence for All. Highlights 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/380478/HEALTH_REPORT_HIGHLIGHTS_2018_EN.PDF (accessed on 13 April 2021).
- Hotchkiss, D.R.; Diana, M.L.; Foreit, K.G.F. How Can Routine Health Information Systems Improve Health Systems Functioning in Lowand Middle-Income Countries? Assessing the Evidence Base; Emerald Group Publishing Ltd.: Bingley, UK, 2012. [Google Scholar] [CrossRef]
- Arah, O.A.; Klazinga, N.S.; Delnoij, D.M.J.; Asbroek, A.H.A.T.; Custers, T. Conceptual frameworks for health systems performance: A quest for effectiveness, quality, and improvement. Int. J. Qual. Health Care 2003, 15, 377–398. [Google Scholar] [CrossRef]
- Lippeveld, T.; Sauerborn, R.; Sapirie, S. Health information systems—Making them work. World Health Forum. 1997, 18, 176–184. [Google Scholar]
- Aqil, A.; Lippeveld, T.; Hozumi, D. PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy Plan. 2009, 24, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, D.R.; Aqil, A.; Lippeveld, T.; Mukooyo, E. Evaluation of the Performance of Routine Information System Management (PRISM) framework: Evidence from Uganda. BMC Health Serv. Res. 2010, 10, 188. [Google Scholar] [CrossRef]
- Sligo, J.; Gauld, R.; Roberts, V.; Villa, L. A literature review for large-scale health information system project planning, implementation and evaluation. Int. J. Med. Inform. 2017, 97, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Tursunbayeva, A.; Bunduchi, R.; Franco, M.; Pagliari, C. Human resource information systems in health care: A systematic evidence review. J. Am. Med. Inform. Assoc. 2017, 24, 633–654. [Google Scholar] [CrossRef] [PubMed]
- Aung, E.; Whittaker, M. Preparing routine health information systems for immediate health responses to disasters. Health Policy Plan. 2012, 28, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, C.; Mion, L.C.; Willens, D.E.; Roumie, C.L.; Kripalani, S. Implementing routine health literacy assessment in hospital and primary care patients. Jt. Comm. J. Qual. Patient Saf. 2014, 40, 68–76. [Google Scholar] [CrossRef]
- Cheng, C.K.; Ip, D.K.; Cowling, B.J.; Ho, L.M.; Leung, G.M.; Lau, E.H.; Uglow, D.; Timpka, T. Digital Dashboard Design Using Multiple Data Streams for Disease Surveillance With Influenza Surveillance as an Example. J. Med. Internet Res. 2011, 13, e85. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G.; Powell, J.; Englesakis, M.; Rizo, C.; Stern, A. Health related virtual communities and electronic support groups: Systematic review of the effects of online peer to peer interactions. BMJ 2004, 328, 1166. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare inter-ventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Anker, A.E.; Reinhart, A.M.; Feeley, T.H. Health information seeking: A review of measures and methods. Patient Educ. Couns. 2011, 82, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Marschollek, M.; Mix, S.; Wolf, K.-H.; Effertz, B.; Haux, R.; Steinhagen-Thiessen, E. ICT-based health information services for elderly people: Past experiences, current trends, and future strategies. Med. Inform. Internet Med. 2007, 32, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Bayoumi, I.; Al Balas, M.; Handler, S.M.; Dolovich, L.; Hutchison, B.; Holbrook, A. The effectiveness of computerized drug-lab alerts: A systematic review and meta-analysis. Int. J. Med. Inform. 2014, 83, 406–415. [Google Scholar] [CrossRef]
- Baysari, M.T.; Lehnbom, E.C.; Li, L.; Hargreaves, A.; Day, R.O.; Westbrook, J.I. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: A systematic review and meta-analysis. Int. J. Med. Inform. 2016, 92, 15–34. [Google Scholar] [CrossRef]
- Eden, K.B.; Totten, A.M.; Kassakian, S.Z.; Gorman, P.N.; McDonagh, M.S.; Devine, B.; Pappas, M.; Daeges, M.; Woods, S.; Hersh, W.R. Barriers and facilitators to exchanging health information: A systematic review. Int. J. Med. Inform. 2016, 88, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Medic, G.; Kließ, M.K.; Atallah, L.; Weichert, J.; Panda, S.; Postma, M.; El-Kerdi, A. Evidence-based Clinical Decision Support Systems for the prediction and detection of three disease states in critical care: A systematic literature review. F1000Research 2019, 8, 1728. [Google Scholar] [CrossRef]
- Wisner, K.; Lyndon, A.; Chesla, C.A. The electronic health record’s impact on nurses’ cognitive work: An integrative review. Int. J. Nurs. Stud. 2019, 94, 74–84. [Google Scholar] [CrossRef]
- Gentil, M.-L.; Cuggia, M.; Fiquet, L.; Hagenbourger, C.; Le Berre, T.; Banâtre, A.; Renault, E.; Bouzille, G.; Chapron, A. Factors influencing the development of primary care data collection projects from electronic health records: A systematic review of the literature. BMC Med. Inform. Decis. Mak. 2017, 17, 139. [Google Scholar] [CrossRef]
- Arditi, C.; Rège-Walther, M.; Durieux, P.; Burnand, B. Computer-generated reminders delivered on paper to healthcare professionals: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 2017, CD001175. [Google Scholar] [CrossRef]
- Mahmoudi, E.; Kamdar, N.; Kim, N.; Gonzales, G.; Singh, K.; Waljee, A.K. Use of electronic medical records in development and validation of risk prediction models of hospital readmission: Systematic review. BMJ 2020, 369, m958. [Google Scholar] [CrossRef]
- Ingebrigtsen, T.; Georgiou, A.; Clay-Williams, R.; Magrabi, F.; Hordern, A.; Prgomet, M.; Li, J.; Westbrook, J.; Braithwaite, J. The impact of clinical leadership on health information technology adoption: Systematic review. Int. J. Med. Inform. 2014, 83, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Reeder, B.; Meyer, E.; Lazar, A.; Chaudhuri, S.; Thompson, H.J.; Demiris, G. Framing the evidence for health smart homes and home-based consumer health technologies as a public health intervention for independent aging: A systematic review. Int. J. Med. Inform. 2013, 82, 565–579. [Google Scholar] [CrossRef]
- Oluoch, T.; Santas, X.; Kwaro, D.; Were, M.C.; Biondich, P.G.; Bailey, C.; Abu-Hanna, A.; De Keizer, N. The effect of electronic medical record-based clinical decision support on HIV care in resource-constrained settings: A systematic review. Int. J. Med. Inform. 2012, 81, e83–e92. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, K.; Sheikh, A. Organizational issues in the implementation and adoption of health information technology innovations: An interpretative review. Int. J. Med. Inform. 2013, 82, e73–e86. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.L.; Georgiou, A.; Doughty, K.; Hornblow, A.; Livingstone, A.; Dougherty, M.; Jacobs, S.; Fisk, M.J. Advancing health information technology roadmaps in long term care. Int. J. Med. Inform. 2020, 136, 104088. [Google Scholar] [CrossRef] [PubMed]
- Mäenpää, T.; Suominen, T.; Asikainen, P.; Maass, M.; Rostila, I. The outcomes of regional healthcare information systems in health care: A review of the research literature. Int. J. Med. Inform. 2009, 78, 757–771. [Google Scholar] [CrossRef]
- Åkesson, K.M.; Saveman, B.I.B.-I.; Nilsson, G. Health care consumers’ experiences of information communication technolo-gy-A summary of literatura. Int. J. Med. Inform. 2007, 76, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Weir, C.R.; Staggers, N.; Laukert, T. Reviewing the impact of computerized provider order entry on clinical outcomes: The quality of systematic reviews. Int. J. Med. Inform. 2012, 81, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Andargoli, A.E.; Scheepers, H.; Rajendran, D.; Sohal, A. Health information systems evaluation frameworks: A systematic review. Int. J. Med. Inform. 2017, 97, 195–209. [Google Scholar] [CrossRef] [PubMed]
- Meidiawati, Y.; Siregar, K.N.; Srimayarti, B.N. Potential Use of Personal Health Records in Managing Hypertension: A Systematic Review. Indian J. Public Health Res. Dev. 2020, 11. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G. Davis User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. Attitudes, Personality, and Behavior, Berksh; Open Press: England, UK; New York, NY, USA, 2005. [Google Scholar]
- Rogers, E.M. Diffusion of Innovations, Free Press. 2003. Available online: https://books.google.es/books/about/Diffusion_of_Innovations_5th_Edition.html?id=9U1K5LjUOwEC&redir_esc=y (accessed on 8 September 2017).
- Kuan, K.K.; Chau, P.Y. A perception-based model for EDI adoption in small businesses using a technology–organization–environment framework. Inf. Manag. 2001, 38, 507–521. [Google Scholar] [CrossRef]
- Alaiad, A.; Zhou, L. The determinants of home healthcare robots adoption: An empirical investigation. Int. J. Med. Inform. 2014, 83, 825–840. [Google Scholar] [CrossRef]
- Alaiad, A.; AlSharo, M.; Alnsour, Y. The Determinants of M-Health Adoption in Developing Countries: An Empirical Investigation. Appl. Clin. Inform. 2019, 10, 820–840. [Google Scholar] [CrossRef]
- Cook, E.J.; Randhawa, G.; Sharp, C.; Ali, N.; Guppy, A.; Barton, G.; Bateman, A.; Crawford-White, J. Exploring the factors that influence the decision to adopt and engage with an integrated assistive telehealth and telecare service in Cambridgeshire, UK: A nested qualitative study of patient ‘users’ and ‘non-users’. BMC Health Serv. Res. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.-C.; Jen, W.-Y. The Adoption of Mobile Health Management Services: An Empirical Study. J. Med. Syst. 2010, 36, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Raymond, L.; de Guinea, A.O.; Poba-Nzaou, P.; Trudel, M.-C.; Marsan, J.; Micheneau, T. Barriers to organizational adoption of EMR systems in family physician practices: A mixed-methods study in Canada. Int. J. Med. Inform. 2014, 83, 548–558. [Google Scholar] [CrossRef]
- Hoque, R. An empirical study of mHealth adoption in a developing country: The moderating effect of gender concern. BMC Med. Inform. Decis. Mak. 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Zhang, X.; Pérez-Stable, E.J.; Bourne, P.E.; Peprah, E.; Duru, O.K.; Breen, N.; Berrigan, D.; Wood, F.; Jackson, J.S.; Wong, D.W.; et al. Big Data Science: Opportunities and Challenges to Address Minority Health and Health Disparities in the 21st Century. Ethn. Dis. 2017, 27, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Vaportzis, E.; Clausen, M.G.; Gow, A.J. Older Adults Perceptions of Technology and Barriers to Interacting with Tablet Computers: A Focus Group Study. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Data for Impact. Estimating the Effect of COVID-19 on Total Utilization of Health Services in Bangladesh—DataForIm-pactProject. 2021. Available online: https://www.data4impactproject.org/publications/estimating-the-effect-of-covid-19-on-total-utilization-of-health-services-in-bangladesh/ (accessed on 9 April 2021).
- Xiao, H.; Dai, X.; Wagenaar, B.H.; Liu, F.; Augusto, O.; Guo, Y.; Unger, J.M. The impact of the COVID-19 pandemic on health services utilization in China: Time-series analyses for 2016–2020. Lancet Reg. Health West. Pac. 2021, 9. [Google Scholar] [CrossRef]
- The Health System Response Monitor (HSRM). COVID-19 Health System Response Monitor. Policy Responses for Bulgaria: Monitoring and Surveillance. Available online: https://www.covid19healthsystem.org/mainpage.aspx (accessed on 9 April 2021).
- World Health Organization. Health Service Data—WHO. World Health Data Platform/Data Collection Tools/Health Service Data. 2021. Available online: https://www.who.int/data/data-collection-tools/health-service-data (accessed on 9 April 2021).
- World Health Organization. Analysing and Using Routine Data to Monitor the Effects of COVID-19 on Essential Health Ser-vices: Practical Guide for National and Subnational Decision-Makers. COVID-19: Essential Health Services. 2021. Available online: https://www.who.int/publications/i/item/who-2019-nCoV-essential-health-services-monitoring-2021-1 (accessed on 9 April 2021).
- Michelsen, K.; Helmut, P.; Achterberg, J. Wilkinson, Promoting Better Integration of Health Information Systems: Best Practices and Challenges Health Evidence Network Synthesis Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Bogaert, P.; For BRIDGE Health; Van Oyen, H. An integrated and sustainable EU health information system: National public health institutes’ needs and possible benefits. Arch. Public Health 2017, 75, 1–5. [Google Scholar] [CrossRef]
- Lau, F.; Kuziemsky, C.; Price, M.; Gardner, J. A review on systematic reviews of health information system studies. J. Am. Med. Inform. Assoc. 2010, 17, 637–645. [Google Scholar] [CrossRef]
- Busza, J.; Lemma, S.; Janson, A.; Adem, S.O.; Berhanu, D.; Defar, A.; Persson, L.-Å.; Källestål, C. Strengthening routine health data analysis in Ethiopia: The Operational Research and Coaching for Analysts (ORCA) experience. Glob. Health Action 2021, 14, 1901390. [Google Scholar] [CrossRef]
- Leon, N.; Balakrishna, Y.; Hohlfeld, A.; Odendaal, W.A.; Schmidt, B.-M.; Zweigenthal, V.; Watkins, J.A.; Daniels, K. Routine Health Information System (RHIS) improvements for strengthened health system management. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Nguefack-Tsague, G.; Tamfon, B.B.; Ngnie-Teta, I.; Ngoufack, M.N.; Keugoung, B.; Bataliack, S.M.; Ndongo, C.B. Factors associated with the performance of routine health information system in Yaoundé-Cameroon: A cross-sectional survey. BMC Med. Inform. Decis. Mak. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Hoxha, K.; Hung, Y.W.; Irwin, B.R.; Grépin, K.A. Understanding the challenges associated with the use of data from routine health information systems in low- and middle-income countries: A systematic review. Health Inf. Manag. J. 2020, 2020. [Google Scholar] [CrossRef]
- Dossa, N.I.; Philibert, A.; Dumont, A. Using routine health data and intermittent community surveys to assess the impact of maternal and neonatal health interventions in low-income countries: A systematic review. Int. J. Gynecol. Obstet. 2016, 135, S64–S71. [Google Scholar] [CrossRef] [PubMed]
- Blaya, J.A.; Shin, S.S.; Yagui, M.; Contreras, C.; Cegielski, P.; Yale, G.; Suárez, C.; Asencios, L.; Bayona, J.; Kim, J.; et al. Reducing Communication Delays and Improving Quality of Care with a Tuberculosis Laboratory Information System in Resource Poor Environments: A Cluster Randomized Controlled Trial. PLoS ONE 2014, 9, e90110. [Google Scholar] [CrossRef]
- Wagenaar, B.H.; Sherr, K.; Fernandes, Q.; Wagenaar, A.C. Using routine health information systems for well-designed health evaluations in low- and middle-income countries. Health Policy Plan. 2016, 31, 129–135. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).