
Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study





Abstract
:1. Introduction
2. Materials and Methods
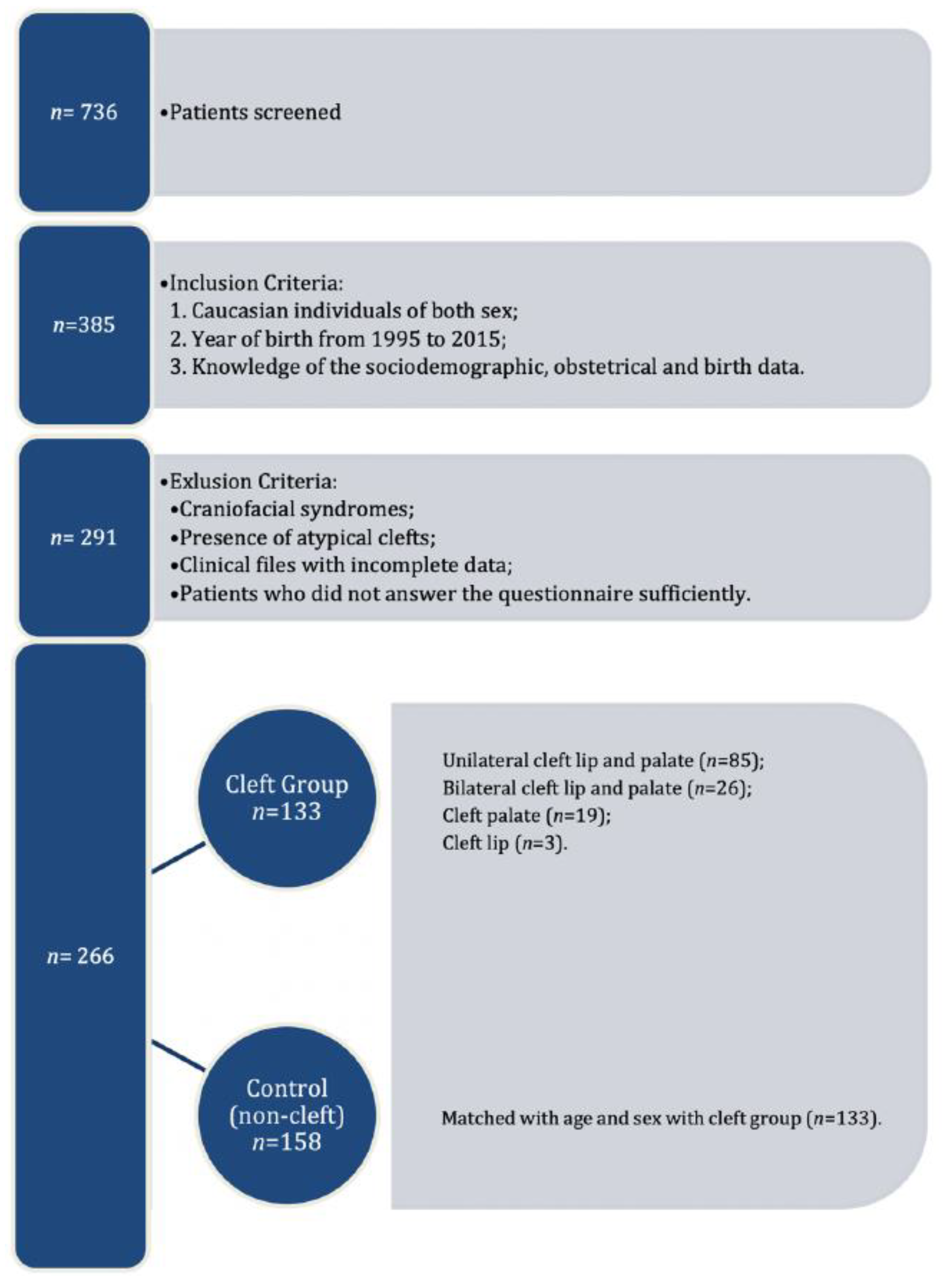
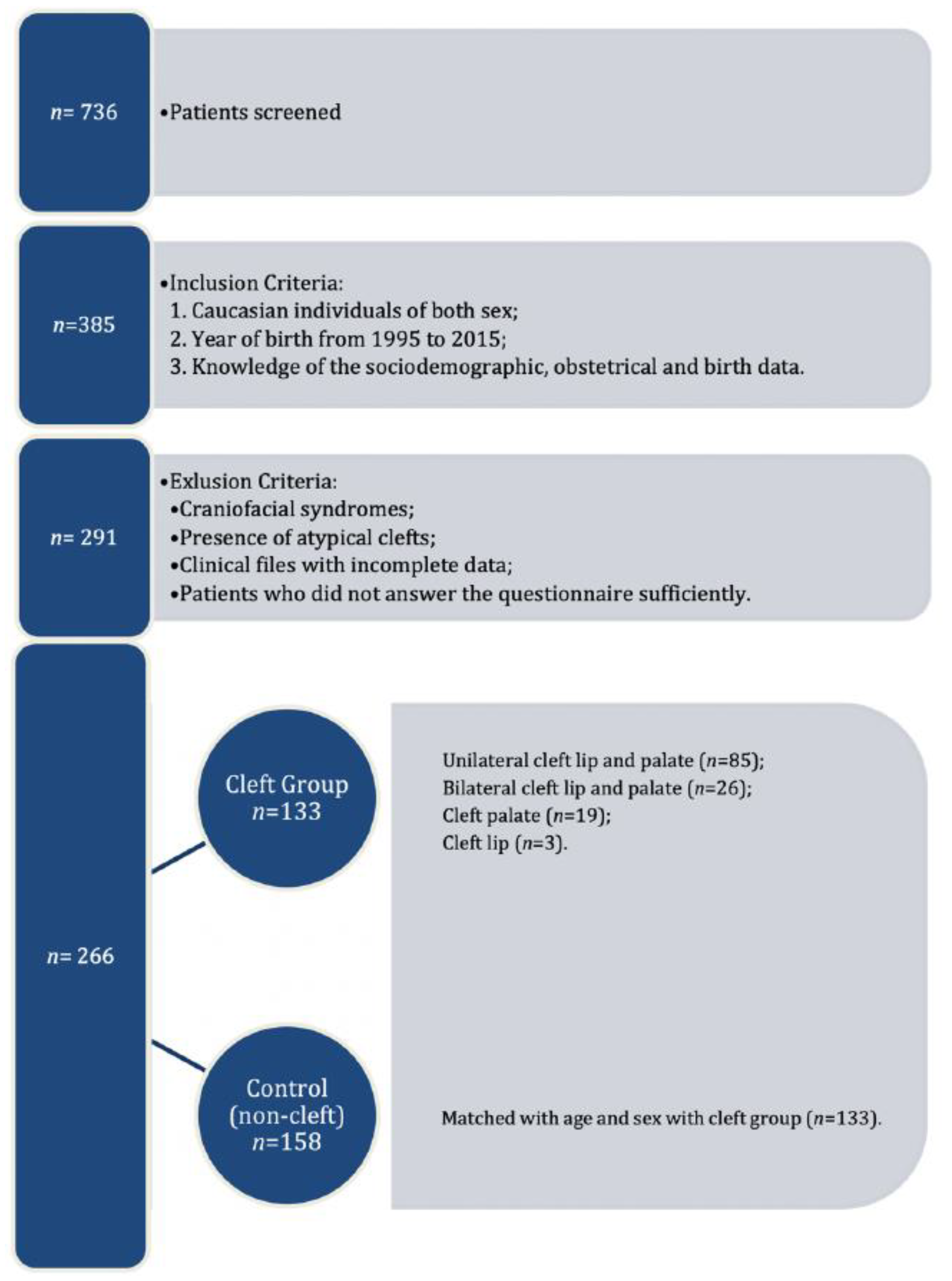
2.1. Study Design
2.2. Data Collection Procedure
- -
- Sociodemographic—age of parents and child; child’s sex.
- -
- Obstetrical data—alcohol intake, smoking, drugs, and pregnancy supplements used, diseases diagnosed before and during pregnancy and exposure to carbon monoxide, recorded by gestational month; early pregnancy body mass index.
- -
- Child birth data—presence and phenotype of cleft, birth weight, birth length, and head circumference at birth.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vieira, A.R.; Orioli, I.M. Birth order and oral clefts: A meta analysis. Teratology 2002, 66, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Mossey, P.A.; Castilla, E. Global Registry and Database on Craniofacial Anomalies. Report of a WHO Registry Meeting on Craniofacial Anomalies. Geneva, Switzerland: WHO. 2003. Available online: https://apps.who.int/iris/bitstream/handle/10665/42840/9241591102.pdf?sequence=1&isAllowed=y (accessed on 23 March 2021).
- Rintala, A.; Stegars, T. Increasing incidence of clefts in Finland: Reliability of hospital records and central register of congenital malformations. Scand. J. Plast Reconstr. Surg. 1982, 16, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Little, J.; Cardy, A.; Munger, R.G. Tobacco smoking and oral clefts: A meta-analysis. Bull. World Health Organ. 2004, 82, 213–218. [Google Scholar]
- European Surveillance of Congenital Anomalies. EUROCAT Data and Surveillance—Prevalence (per 10,000 Births) for the Following Registries: All Full Registries, Oro-Facial Clefts, from 2011–2018. Available online: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en (accessed on 27 January 2021).
- Mossey, P. Epidemiology underpinning research in the aetiology of orofacial clefts. Orthod. Craniofac. Res. 2007, 10, 114–120. [Google Scholar] [CrossRef]
- Leslie, E.J.; Marazita, M.L. Genetics of Cleft Lip and Cleft Palate. Am. J. Med. Genet. C Semin. Med. Genet. 2013, 163, 246–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahimov, F.; Jugessur, A.; Murray, J.C. Genetics of nonsyndromic orofacial clefts. Cleft Palate Craniofac. J. 2012, 49, 73–91. [Google Scholar] [CrossRef] [Green Version]
- Spilson, S.V.; Kim, H.J.; Chung, K.C. Association between maternal diabetes mellitus and newborn oral cleft. Ann. Plast. Surg. 2001, 47, 477–481. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X.H.; Zheng, X.M.; Liu, T.Z.; Zhang, W.B.; Zheng, H.; Chen, M.F. Maternal gestational smoking, diabetes, alcohol drinking, pre-pregnancy obesity and the risk of cryptorchidism: A systematic review and meta-analysis of observational studies. PLOS ONE 2015, 10, e0119006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, S.; Takeuchi, M.; Kawakami, C.; Kawakami, K.; Ito, S. Japan Environment and Children’s Study Group. Maternal multivitamin intake and orofacial clefts in offspring: Japan Environment and Children’s Study (JECS) cohort study. BMJ Open 2020, 10, e035817. [Google Scholar] [CrossRef] [Green Version]
- Silva, H.P.V.; Arruda, T.T.S.; Souza, K.S.C.; Bezerra, J.F.; Leite, G.C.P.; Brito, M.E.F.; Lima, V.M.G.D.M.; Luchessi, A.D.; Bortolin, R.H.; Ururahy, M.A.G.; et al. Risk factors and comorbidities in Brazilian patients with orofacial clefts. Braz. Oral Res. 2018, 32, e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheshmi, B.; Jafari, Z.; Naseri, M.A.; Davari, H.A. Assessment of the correlation between various risk factors and orofacial cleft disorder spectrum: A retrospective case-control study. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 26. [Google Scholar] [CrossRef] [PubMed]
- Martelli, D.R.B.; Cruz, K.W.; Barros, L.M.; Silveira, M.F.; Swerts, M.S.O.; Júnior, H.M. Maternal and paternal age, birth order and interpregnancy interval evaluation for cleft lip-palate. Braz. J. Otorhinolaryngol. 2010, 76, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Jamilian, A.; Sarkarat, F.; Jafari, M.; Neshandar, M.; Amini, E.; Khosravi, S.; Ghassemi, A. Family history and risk factors for cleft lip and palate patients and their associated anomalies. Stomatologija 2017, 19, 78–83. [Google Scholar]
- Zhou, Y.; Sinnathamby, V.; Yu, Y.; Sikora, L.; Johnson, C.Y.; Mossey, P.; Little, J. Folate intake, markers of folate status and oral clefts: An updated set of systematic reviews and meta-analyses. Birth Defects Res. 2020, 112, 1699–1719. [Google Scholar] [CrossRef] [PubMed]
- Johansen, A.M.W.; Lie, R.T.; Wilcox, A.J.; Andersen, L.F.; Drevon, C.A. Maternal dietary intake of vitamin A and risk of orofacial clefts: A population-based case-control study in Norway. Am. J. Epidemiol. 2008, 167, 1164–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, G.M.; Carmichael, S.L.; Laurent, C.; Rasmussen, S.A. Maternal nutrient intakes and risk of orofacial clefts. Epidemiology 2006, 17, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Cedergren, M.; Källén, B. Maternal obesity and the risk for orofacial clefts in the offspring. Cleft Palate Craniofac. J. 2005, 42, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Block, S.R.; Watkins, S.M.; Salemi, J.L.; Rutkowski, R.; Tanner, J.P.; Correia, J.A.; Kirby, R.S. Maternal pre-pregnancy body mass index and risk of selected birth defects: Evidence of a dose-response relationship. Paediatr. Perinat. Epidemiol. 2013, 27, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Kutbi, H.; Wehby, G.L.; Uribe, L.M.M.; Romitti, P.A.; Carmichael, S.; Shaw, G.M.; Olshan, A.F.; DeRoo, L.; Rasmussen, S.A.; Murray, J.C.; et al. Maternal underweight and obesity and risk of orofacial clefts in a large international consortium of population-based studies. Int. J. Epidemiol. 2017, 46, 190–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, M.; Svensson, H.; Källén, B. Birth weight, body length, and cranial circumference in newborns with cleft lip or palate. Cleft Palate Craniofac. J. 1998, 35, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Wyszynski, D.F.; Sarkozi, A.; Vargha, P.; Czeizel, A.E. Birth weight and gestational age of newborns with cleft lip with or without cleft palate and with isolated cleft palate. J. Clin. Pediatr. Dent. 2003, 27, 185–190. [Google Scholar] [CrossRef]
- Kruse, T.; Mangold, E.; Braumann, B. Impact of Maternal Smoking on Nonsyndromic Clefts: Sex-Specific Associations with Side and Laterality. Cleft Palate Craniofac. J. 2021, 58, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, J. Growth curves: How to best measure growth of the preterm infant. J. Pediatr. 2013, 162 (Suppl. 3), S2–S6. [Google Scholar] [CrossRef] [PubMed]
- Pereira-da-Silva, L.; Virella, D.; Fusch, C. Nutritional Assessment in Preterm Infants: A Practical Approach in the NICU. Nutrients 2019, 11, 1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herkrath, A.P.C.Q.; Herkrath, F.J.; Rebelo, M.A.B.; Vettore, M.V. Parental age as a risk factor for non-syndromic oral clefts: A meta-analysis. J. Dent. 2012, 40, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, P.H.P.; Machado, R.A.; Reis, S.R.A.; Martelli, D.R.B.; Dias, V.O.; Martelli-Júnior, H. Parental age is related to the occurrence of cleft lip and palate in Brazilian populations. Braz. J. Oral Sci. 2016, 15, 167–170. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, A.C.; Ly, S.; Magee, K.S.; Ihenacho, U.; Baurley, J.W.; Sanchez-Lara, P.A.; Brindopke, F.; Nguyen, T.H.D.; Nguyen, V.; Tangco, M.I.; et al. Parental risk factors for oral clefts among Central Africans, Southeast Asians, and Central Americans. Birth Defects Res. A Clin. Mol. Teratol. 2015, 103, 863–879. [Google Scholar] [CrossRef] [PubMed]
- Hermann, N.V.; Darvann, T.A.; Munch, A.; Kreiborg, S. Parental age in relation to the severity of cleft lip and/or palate. Orthod. Craniofac. Res. 2018, 21, 236–241. [Google Scholar] [CrossRef]
- Berg, E.; Lie, R.T.; Sivertsen, A.; Haaland, Ø.A. Parental age and the risk of isolated cleft lip: A registry-based study. Ann. Epidemiol. 2015, 25, 942–947.e1. [Google Scholar] [CrossRef]
- Stothard, K.J.; Tennant, P.W.G.; Bell, R.; Rankin, J. Maternal overweight and obesity and the risk of congenital anomalies: A systematic review and meta-analysis. JAMA 2009, 301, 636–650. [Google Scholar] [CrossRef]
- Izedonmwen, O.M.; Cunningham, C.; Macfarlane, T.V. What is the Risk of Having Offspring with Cleft Lip/Palate in Pre-Maternal Obese/Overweight Women When Compared to Pre-Maternal Normal Weight Women? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Res. 2015, 6, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, R.; Colombo, A.; Suazo, J. Maternal obesity is a risk factor for orofacial clefts: A meta-analysis. Br. J. Oral Maxillofac. Surg. 2015, 53, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.; Tennant, P.W.G.; Stothard, K.J.; Bythell, M.; Summerbell, C.D.; Bell, R. Maternal body mass index and congenital anomaly risk: A cohort study. Int. J. Obes. 2010, 34, 1371–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jura, M.; Kozak, L.P. Obesity and related consequences to ageing. Age 2016, 38, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauk, K. Gerontological Nursing: Competencies for Care, 2nd ed.; Jones and Bartlett Publishers: London, UK, 2009; p. 869. [Google Scholar]
- Miranda, G.S.; Marques, I.L.; Barros, S.P.; Arena, E.P.; Souza, L. Weight, Length, and Body Mass Index Growth of Children under 2 Years of Age with Cleft Lip and Palate. Cleft Palate Craniofac. J. 2016, 53, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Mossey, P.A.; Little, J.; Munger, R.G.; Dixon, M.J.; Shaw, W.C. Cleft lip and palate. Lancet 2009, 374, 1773–1785. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Control (133) | Orofacial Cleft (133) | p |
|---|---|---|---|
| Sex (M/F) | 85/48 (63.9%/36.1%) | 85/48 (63.9%/36.1%) | 1.000 # |
| Maternal age (years) a | 31 (4.2) 28.0/34.0 | 28 (5.6) 25.0/32.0 | <0.001 § |
| Paternal age (years) a | 33 (4.9) 29.0/36.0 | 31 (6.3) 27.0/35.0 | 0.016 § |
| Maternal BMI (kg/m2) a | 23 (3.9) 20.8/25.1 | 25 (4.3) 21.9/28.3 | <0.001 § |
| Birth Length (cm) a | 49 (2.1) 48.0/50.0 | 48 (2.9) 47.0/50.0 | 0.519 § |
| Birth Weight (kg) a | 3 (0.5) 3.0/3.6 | 3 (0.5) 2.8/3.4 | 0.033 § |
| Birth Head circumference (cm) a | 35 (2.2) 33.5/35.0 | 34 (2.3) 33.5/35.0 | 0.457 § |
| Variables | B | p | OR | CI95% |
|---|---|---|---|---|
| Maternal age (years) | −0.102 | <0.001 | 0.903 | [0.856; 0.953] |
| Maternal BMI (kg/m2) | 0.131 | <0.001 | 1.140 | [1.068; 1.216] |
| Birth Weight (kg) | −0.833 | 0.003 | 0.435 | [0.253; 0.746] |
| 2.477 | 0.062 | 11.904 |
| Variables | Unilateral Cleft Lip and Palate (n = 85) | Bilateral Cleft Lip and Palate (n = 26) | Cleft Palate (n = 19) | Cleft Lip (n = 3) | p |
|---|---|---|---|---|---|
| Maternal age (years) a | 28 (5.4) 25.0/31.0 | 28 (5.8) 24.0/31.0 | 30 (5.8) 26.0/37.0 | 30 (9.1) 23.0/40.0 | 0.4271 § |
| Paternal age (years) a | 31 (6.2) 27.0/34.0 | 32 (6.9) 28.0/34.0 | 34 (5.4) 29.0/38.0 | 27 (3.2) 25.0/31.0 | 0.121 £ |
| Maternal BMI (kg/m2) a | 25 (4.2) 22.3/27.6 | 25 (5.0) 20.3/29.1 | 25 (3.6) 21.8/26.4 | 33 (1.7) 30.8/34.2 | 0.023 £ |
| Birth Length (cm) a | 48 (2.7) 47.0/50.0 | 48 (2.6) 47.0/50.0 | 49 (4.3) 48.0/51.0 | 48 (1.2) 47.0/49.0 | 0.452 § |
| Birth Weight (kg) a | 3 (0.5) 2.8/3.4 | 3 (0.5) 2.9/3.5 | 3 (0.4) 2.9/3.4 | 3 (0.7) 2.2/3.6 | 0.505 £ |
| Birth Head circumference (cm) a | 34 (1.7) 33.0/35.0 | 34 (1.2) 33.5/35.0 | 36 (4.3) 33.5/36.0 | 33 (2.6) 30.0/35.0 | 0.702 § |
| Phenotype of Cleft | p |
|---|---|
| Unilateral cleft lip and palate vs. bilateral cleft lip and palate | p = 0.990 |
| Unilateral cleft lip and palate vs. cleft palate | p = 0.947 |
| Unilateral cleft lip and palate vs. cleft lip | p = 0.016 |
| Bilateral cleft lip and palate vs. cleft palate | p = 0.995 |
| Bilateral cleft lip and palate vs. cleft lip | p = 0.016 |
| Cleft palate vs. cleft lip | p = 0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francisco, I.; Caramelo, F.; Fernandes, M.H.; Vale, F. Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 4615. https://doi.org/10.3390/ijerph18094615
Francisco I, Caramelo F, Fernandes MH, Vale F. Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4615. https://doi.org/10.3390/ijerph18094615
Chicago/Turabian StyleFrancisco, Inês, Francisco Caramelo, Maria Helena Fernandes, and Francisco Vale. 2021. "Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study" International Journal of Environmental Research and Public Health 18, no. 9: 4615. https://doi.org/10.3390/ijerph18094615
APA StyleFrancisco, I., Caramelo, F., Fernandes, M. H., & Vale, F. (2021). Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study. International Journal of Environmental Research and Public Health, 18(9), 4615. https://doi.org/10.3390/ijerph18094615