
Uncertainty and Nursing Needs of Parents with Pediatric Cancer Patients in Different Treatment Phases: A Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Samples
2.2. Measurements
2.2.1. Data Collection/Procedure
2.2.2. Instruments
- Uncertainty level
- Nursing needs
2.3. Data Analysis
3. Results
3.1. General Characteristics of Parents and Their Children with Pediatric Cancer
3.1.1. General Characteristics of Pediatric Cancer Patients’ Parents
3.1.2. General Characteristics of Children with Childhood Cancer
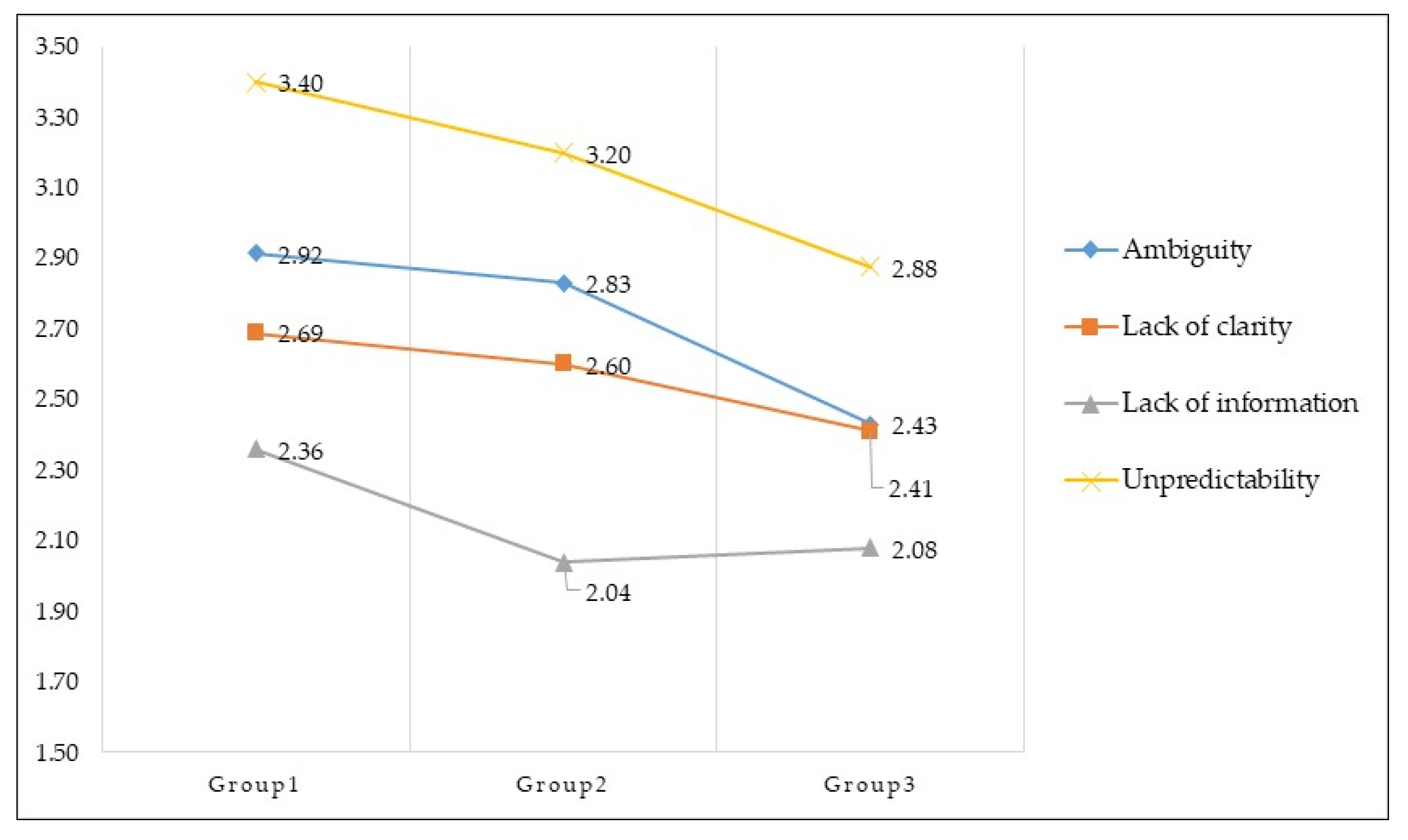
3.2. Parents’ Uncertainty Level by the Treatment Phase of Pediatric Cancer Patients
3.3. The Nursing Needs of Parents According to the Treatment Phase of Pediatric Cancer Patients
3.3.1. Nursing Needs in the Treatment Initiation Group
“I wonder if my child can live the same life as a normal person after a complete recovery. [six times].”
“What I want to know the most is the probability of complete recovery after medical treatments. Psychological treatment will also be necessary. [23 times].”
“I am curious about life after treatment for people who had the same type of disease as similar age of my child. I want to know how they are adjusting to family and social life and at what rate. [nine times].”
3.3.2. Nursing Needs in the Ongoing Treatment Group
“I am curious why the disease occurred and whether it will recur after the end of treatment. Also, will there be any complications or other factors which could be harmful to the human body due to side effects during chemotherapy? Frequent detailed explanations of the patient’s current status during treatment are required. The child is being treated based on unfounded beliefs whereas the information or physical status of the child’s treatment is unknown. [10 times].”
“When introducing a new treatment or drug, I would like an exact explanation of why it is used, its side effects, its intended effects, test results with detailed descriptions, and the exact treatment process. [14 times].”
3.3.3. Nursing Needs in the Post-Treatment Group
“I heard that returning to normal life is possible, but I am curious as to what is allowed and what is not. I am also concerned about the risk of infection. Thus I’m cautious about my outside activities as a parent. Also, I wonder if my child’s immune system is weaker than other person’s after treatment is finished. With my child no longer seeing the doctor as often as they did during treatment, I feel anxious when my child is in poor condition. [27 times].”
“It’s not easy [for my child] to move anymore because of complication: knee necrosis. I would like to know how to alleviate some of the complications and side effects during the treatment process. It will be more helpful to participate in complication relief program information depends on the treatment process in advance. [eight times].”
“I would appreciate if I could receive detailed explanations or things to keep in mind through lectures or social media. I am afraid of my child joining kindergarten, school, and community life even after treatment. [seven times].”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hubbard, A.K.; Spector, L.G.; Fortuna, G.; Marcotte, E.L.; Poynter, J.N. Trends in international incidence of pediatric cancers in children under 5 years of age: 1988–2012. JNCI Cancer Spectr. 2019, 3, pkz007. [Google Scholar] [CrossRef]
- Korea Central Cancer Registry. Available online: https://ncc.re.kr/main.ncc?uri=english/sub04_Statistics (accessed on 15 March 2021).
- Gunter, M.D.; Duke, G. Reducing Uncertainty in Families Dealing With Childhood Cancers: An Integrative Literature Review. Pediatric Nurs. 2018, 44, 21–37. [Google Scholar]
- Siegel, D.A.; Richardson, L.C.; Henley, S.J.; Wilson, R.J.; Dowling, N.F.; Weir, H.K.; Tai, E.W.; Buchanan Lunsford, N. Pediatric cancer mortality and survival in the United States, 2001–2016. Cancer 2020, 126, 4379–4389. [Google Scholar] [CrossRef]
- Santacroce, S.J.; Killela, M.K.; Kerr, G.; Leckey, J.A.; Kneipp, S.M. Fathers’ psychological responses to pediatric cancer–induced financial distress. Pediatric Blood Cancer 2020, 67, e28281. [Google Scholar] [CrossRef]
- Neil, L.; Clarke, S. Learning to live with childhood cancer: A literature review of the parental perspective. Int. J. Palliat. Nurs. 2010, 16, 110–119. [Google Scholar] [CrossRef]
- Hutchinson, K.C.; Willard, V.W.; Hardy, K.K.; Bonner, M.J. Adjustment of caregivers of pediatric patients with brain tumors: A cross-sectional analysis. Psycho Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2009, 18, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Flury, M.; Caflisch, U.; Ullmann-Bremi, A.; Spichiger, E. Experiences of parents with caring for their child after a cancer diagnosis. J. Pediatric Oncol. Nurs. 2011, 28, 143–153. [Google Scholar] [CrossRef]
- Mishel, M.H. Uncertainty in illness. Image J. Nurs. Scholarsh. 1988, 20, 225–232. [Google Scholar] [CrossRef]
- Mishel, M.H. Reconceptualization of the uncertainty in illness theory. Image J. Nurs. Scholarsh. 1990, 22, 256–262. [Google Scholar] [CrossRef]
- Cohen, M.H. The triggers of heightened parental uncertainty in chronic, life-threatening childhood illness. Qual. Health Res. 1995, 5, 63–77. [Google Scholar] [CrossRef]
- Boman, K.; Lindahl, A.; Björk, O. Disease-related distress in parents of children with cancer at various stages after the time of diagnosis. Acta Oncol. 2003, 42, 137–146. [Google Scholar] [CrossRef]
- Mauro, A.M.P. Long-term follow-up study of uncertainty and psychosocial adjustment among implantable cardioverter defibrillator recipients. Int. J. Nurs. Stud. 2010, 47, 1080–1088. [Google Scholar] [CrossRef]
- Mishel, M.H. Parents’ perception of uncertainty concerning their hospitalized child. Nurs. Res. 1983, 32, 324–330. [Google Scholar] [CrossRef]
- Edwards, B.; Ung, L. Quality of life instruments for caregivers of patients with cancer: A review of their psychometric properties. Cancer Nurs. 2002, 25, 342–349. [Google Scholar] [CrossRef]
- Kim, M.A.; Yi, J.; Wilford, A.; Kim, S.H. Parenting Changes of Mothers of a Child with Cancer. J. Fam. Issues 2020, 41, 460–482. [Google Scholar] [CrossRef]
- Steliarova-Foucher, E.; Stiller, C.; Lacour, B.; Kaatsch, P. International Classification of Childhood Cancer, third edition. Cancer 2005, 103, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Oh, I.O.; Kim, S. Structural equation model for caregiving experience of families providing care for family members with mental disorders. J. Korean Acad. Nurs. 2015, 45, 97–106. [Google Scholar] [CrossRef]
- Rourke, L.; Anderson, T. Validity in quantitative content analysis. Educ. Technol. Res. Dev. 2004, 52, 5. [Google Scholar] [CrossRef]
- Mu, P.-F.; Ma, F.-C.; Hwang, B.; Chao, Y.-M. Families of children with cancer: The impact on anxiety experienced by fathers. Cancer Nurs. 2002, 25, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kim, O. A Study on Mother’s Perception of Uncertainty and Nursing Need Concernting Child’s Hospitalization; Gangwon National University: Chuncheon, Korea, 2001. [Google Scholar]
- Oh, W.O.; Park, E.S. Uncertainty, Self-Efficacy & Coping in Parents′ of Children with Cancer. Child Health Nurs. Res. 1998, 4, 274–285. [Google Scholar]
- Lee, M.-S.; Kim, H.-J.; Suh, S.-R. Uncertainty and nursing need according to illness phases in cancer patients. Korean J. Adult Nurs. 2008, 20, 1–9. [Google Scholar]
- Park, E.J.; Jeong, J.H.; Jin, S.R.; Cho, E.J.; Kim, J.Y.; Shin, J.H.; Hur, M.E.; Seo, M.J.; Cha, E.K.; Noh, G.O. Nursing needs and satisfaction of family of pediatric cancer patients during chemotherapy. Asian Oncol. Nurs. 2017, 17, 97–106. [Google Scholar] [CrossRef][Green Version]
- Arabiat, D.H.; Altamimi, A. Unmet care needs of parents of children with cancer in Jordan: Implications for bed-side practice. J. Clin. Nurs. 2013, 22, 531–539. [Google Scholar] [CrossRef]
- Seo, J.-Y. Nursing Need and Satisfaction of Families with their Hospitalized Children. Child Health Nurs. Res. 2002, 8, 195–203. [Google Scholar]
- Yoo, K.-H.; Kim, A.-J. A study on the nursing needs of parents with hospitalized child. J. Korean Acad. Soc. Nurs. Educ. 2001, 7, 323–332. [Google Scholar]
- Jeong, E.; Kwon, I.S. Nursing needs and nursing performance as perceived by caregivers with hospitalized children. Child Health Nurs. Res. 2015, 21, 244–252. [Google Scholar] [CrossRef][Green Version]
- Tiberius, R.G.; Sackin, H.D.; Tallett, S.E.; Jacobson, S.; Turner, J. Conversations with parents of medically ill children: A study of interactions between medical students and parents and pediatric residents and parents in the clinical setting. Teach. Learn. Med. 2001, 13, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Kerr, L.M.; Harrison, M.B.; Medves, J.; Tranmer, J.E.; Fitch, M.I. Understanding the supportive care needs of parents of children with cancer: An approach to local needs assessment. J. Pediatric Oncol. Nurs. 2007, 24, 279–293. [Google Scholar] [CrossRef]
- Frost, J.; Vermeulen, I.E.; Beekers, N. Anonymity versus privacy: Selective information sharing in online cancer communities. J. Med Internet Res. 2014, 16, e126. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Categories | n (%) | Median/Mean ± SD |
|---|---|---|---|
| Relationship with the pediatric cancer patient | Father | 14 (11.8) | |
| Mother | 105 (88.2) | ||
| Age (years) | 20–29 | 4 (3.4) | 39/39.36 ± 5.42 |
| 30–39 | 56 (47.1) | ||
| 40–49 | 56 (47.1) | ||
| ≥50 | 3 (2.5) | ||
| Religious | None | 58 (48.7) | |
| Yes | 61 (51.3) | ||
| Education | ≤Middle school | 2 (1.7) | |
| High school | 23 (19.3) | ||
| ≥College/University | 94 (79.0) | ||
| Occupation | Employed | 35 (29.4) | |
| Unemployed | 84 (70.6) | ||
| Average monthly household income (KRW 10,000) | ≤199 | 21 (17.6) | |
| 200–299 | 21 (17.6) | ||
| 300–399 | 27 (22.7) | ||
| ≥400 | 50 (42.0) |
| Characteristics | Categories | n (%) | Median/Mean ± SD |
|---|---|---|---|
| Gender | Male | 69 (58.0) | |
| Female | 50 (42.0) | ||
| Type of cancer | Acute lymphoblastic leukemia | 29 (24.4) | |
| Acute myeloid leukemia | 13 (10.9) | ||
| Acute biphenotypic leukemia | 4 (3.4) | ||
| Chronic myeloid leukemia | 1 (0.8) | ||
| Brain tumor | 16 (13.4) | ||
| Non-Hodgkin lymphoma | 14 (11.8) | ||
| Osteosarcoma | 8 (6.7) | ||
| Neuroblastoma | 8 (6.7) | ||
| Retinoblastoma | 7 (5.9) | ||
| Rhabdomyosarcoma | 6 (5.0) | ||
| Germ cell tumor | 5 (4.2) | ||
| Wilms tumor | 4 (3.4) | ||
| Ewing sarcoma | 3 (2.5) | ||
| Hepatoblastoma | 1 (0.8) | ||
| Age | 0–11 months | 7 (5.9) | 3/7.65 ± 4.98 |
| 1–5 years | 36 (30.3) | ||
| 6–10 years | 33 (27.7) | ||
| ≥11 years | 43 (36.1) | ||
| Order of birth | First | 73 (61.3) | |
| Second | 36 (30.3) | ||
| ≥Third | 10 (8.4) | ||
| Time since diagnosis | 1–11 months | 65 (54.6) | |
| ≥12 months | 54 (45.4) | ||
| Relapse | Yes | 23 (19.3) | |
| No | 96 (80.7) | ||
| Transplantation | Yes | 35 (29.4) | |
| No | 84 (70.6) |
| Subdomain | Group 1 a (n = 39) | Group 2 b (n = 40) | Group 3 c (n = 40) | F | p (Post-Hoc Test: Scheffé) |
|---|---|---|---|---|---|
| M ± SD | |||||
| Ambiguity | 37.29 ± 8.04 | 36.80 ± 8.34 | 31.60 ± 6.85 | 7.49 | 0.001 (a, b > c) |
| Lack of clarity | 24.28 ± 4.21 | 23.43 ± 4.47 | 21.75 ± 4.48 | 3.41 | 0.036 (a > c) |
| Lack of information | 11.87 ± 2.71 | 10.23 ± 2.35 | 10.48 ± 2.35 | 5.06 | 0.008 (a > b, c) |
| Unpredictability | 13.69 ± 2.70 | 12.88 ± 3.23 | 11.53 ± 2.49 | 5.94 | 0.003 (a > c) |
| Total | 87.77 ± 13.43 | 83.33 ± 15.10 | 75.35 ± 12.82 | 8.20 | <0.001 (a, b > c) |
| Item | Group 1 (n = 39) a | Group 2 (n = 40) b | Group 3 (n = 40) c | |
|---|---|---|---|---|
| Mean ± SD | ||||
| Ambiguity: 13 questions | ||||
| 1. | I am unsure if my child’s illness is getting better or worse | 3.44 ± 1.23 | 3.40 ± 1.11 | 2.78 ± 1.14 |
| 2. | It is unclear how bad my child’s pain will be | 3.72 ± 1.19 | 3.63 ± 1.03 | 2.68 ± 1.16 |
| 3. | My child’s symptoms continue to change unpredictably | 2.64 ± 1.11 | 2.73 ± 1.04 | 2.08 ± 0.97 |
| 4. | It is difficult to know if the treatments or medications my child is getting are working | 2.64 ± 0.96 | 2.65 ± 1.10 | 2.60 ± 0.98 |
| 5. | Because of the unpredictability of my child’s illness, I cannot plan for the future | 2.90 ± 1.19 | 2.88 ± 1.02 | 2.75 ± 1.10 |
| 6. | The course of my child’s illness keeps changing. He/she has good and bad days | 2.72 ± 1.05 | 2.83 ± 1.06 | 2.30 ± 0.99 |
| 7. | It’s vague to me how I will manage the care of my child after he/she leaves the hospital | 2.97 ± 1.22 | 2.33 ± 1.02 | 2.25 ± 0.98 |
| 8. | It is not clear what is going to happen to my child | 3.46 ± 1.00 | 3.28 ± 1.04 | 2.93 ± 1.10 |
| 9. | The results of my child’s tests are inconsistent | 2.69 ± 1.13 | 2.38 ± 0.90 | 2.03 ± 0.83 |
| 10. | The effectiveness of the treatment is undetermined | 2.36 ± 0.81 | 2.40 ± 1.01 | 1.80 ± 0.61 |
| 11. | It is difficult to determine how long it will be before I can care for my child by myself | 2.90 ± 0.97 | 2.48 ± 1.13 | 1.83 ± 0.81 |
| 12. | Because of the treatment, what my child can and cannot do keeps changing | 3.46 ± 1.14 | 3.88 ± 0.72 | 3.68 ± 1.02 |
| 13. | I’m certain they will not find anything else wrong with my child | 2.03 ± 1.18 | 1.98 ± 1.07 | 1.93 ± 0.92 |
| Lack of clarity: nine questions | ||||
| 14. | I have a lot of questions without answers | 4.21 ± 1.00 | 3.85 ± 0.83 | 3.73 ± 0.96 |
| 15. | The explanations they give about my child seem hazy to me | 2.36 ± 0.96 | 2.63 ± 0.95 | 2.23 ± 0.86 |
| 16. | The purpose of each treatment for my child is clear to me | 2.51 ± 0.68 | 2.53 ± 0.68 | 2.20 ± 0.76 |
| 17. | I do not know when to expect things will be done to my child | 3.54 ± 1.02 | 3.45 ± 0.93 | 2.63 ± 1.03 |
| 18. | I understand everything explained to me | 2.59 ± 0.72 | 2.43 ± 0.75 | 2.38 ± 0.81 |
| 19. | The doctors say things to me that have many meanings | 2.33 ± 0.81 | 2.40 ± 0.84 | 2.40 ± 1.00 |
| 20. | There are so many different types of staff; it’s unclear who is responsible for what | 2.23 ± 0.84 | 2.15 ± 0.98 | 2.18 ± 0.90 |
| 21. | I can depend on the nurses when I need them | 2.13 ± 1.06 | 1.95 ± 0.75 | 1.95 ± 0.68 |
| 22. | The doctors and nurses use everyday language so I can understand what they are saying | 2.38 ± 0.78 | 2.05 ± 0.64 | 2.08 ± 0.69 |
| Lack of information: five questions | ||||
| 23. | I don’t know what is wrong with my child | 2.08 ± 1.13 | 1.93 ± 0.80 | 2.05 ± 1.01 |
| 24. | My child’s treatment is too complex to figure out | 2.82 ± 0.79 | 2.35 ± 0.98 | 2.10 ± 0.74 |
| 25. | They have not given my child a specific diagnosis | 2.44 ± 1.19 | 2.10 ± 1.01 | 2.08 ± 1.05 |
| 26. | My child’s diagnosis is definite and will not change | 2.49 ± 0.94 | 2.13 ± 0.94 | 2.35 ± 1.10 |
| 27. | The seriousness of my child’s illness has not been determined | 2.05 ± 1.03 | 1.73 ± 0.75 | 1.90 ± 0.81 |
| Unpredictability: four questions | ||||
| 28. | I can predict how long my child’s illness will last and feel ill | 3.69 ± 0.86 | 3.38 ± 1.17 | 3.40 ± 1.01 |
| 29. | I usually don’t know if my child is going to have a good or bad day | 3.33 ± 1.13 | 3.30 ± 1.11 | 2.78 ± 1.07 |
| 30. | I can generally predict the course of my child’s illness | 3.18 ± 1.00 | 3.03 ± 1.05 | 2.73 ± 0.91 |
| 31. | My child’s physical distress is unpredictable; I don’t know when it is going to get better or worse | 3.49 ± 0.97 | 3.18 ± 0.87 | 2.63 ± 1.03 |
| Treatment Phase | Theme (Frequency) | Nursing Needs |
|---|---|---|
| Total | Diet for infection control (68) | Availability of the same meal as usual |
| Low-bacterial diet during the nontreatment period | ||
| Environmental management and activity restrictions to prevent infection (65) | Specific methods of environmental management | |
| The range of normal activity in daily life after discharge | ||
| Current health condition and prognosis (52) | Specific information on the patient’s current condition and prognosis | |
| Possibility of recurrence | ||
| Treatment initiation group | Prognosis and possibility of adoption to normal life (19) | Possibility to return to ordinary life as before |
| Probability of a full recovery after treatment completion | ||
| Infection prevention rules for daily activities (14) | Infection control methods at home (cleaning method, bedding management) | |
| Effective methods for environmental management and infection prevention after discharge | ||
| Ongoing treatment group | Progress of treatment and medication (34) | The severity of the disease currently (compared to the time of diagnosis) |
| Curiosity about the reasons for and side effects of a new procedure or medication | ||
| Caring for your child’s psychological state (14) | Child’s mental health and psychological care | |
| How to play with a child with illness: emotional support is needed | ||
| Adverse effects of treatment and coping strategy (9) | Ways of alleviating the side effects of treatment | |
| Post-treatment group | Prognosis after termination and re-adaptation to school or society (19) | How a child receives care after treatment and how much and how much |
| Degree of risk of recurrence | ||
| Allowable activity in daily life after treatment is over | ||
| Long-term management method and system for disease-related sequelae (15) | Description of post-treatment period from a long-term perspective | |
| Availability of detailed explanations and important points through education, lectures, and social media | ||
| Complication relief program | ||
| Emotional support after treatment ends (10) | Psychotherapy for social adaptation | |
| Relieving a child of loneliness and depression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.; Suh, E.E.; Yu, S.-Y. Uncertainty and Nursing Needs of Parents with Pediatric Cancer Patients in Different Treatment Phases: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4253. https://doi.org/10.3390/ijerph18084253
Park M, Suh EE, Yu S-Y. Uncertainty and Nursing Needs of Parents with Pediatric Cancer Patients in Different Treatment Phases: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(8):4253. https://doi.org/10.3390/ijerph18084253
Chicago/Turabian StylePark, Mijeong, Eunyoung E. Suh, and Soo-Young Yu. 2021. "Uncertainty and Nursing Needs of Parents with Pediatric Cancer Patients in Different Treatment Phases: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 8: 4253. https://doi.org/10.3390/ijerph18084253
APA StylePark, M., Suh, E. E., & Yu, S.-Y. (2021). Uncertainty and Nursing Needs of Parents with Pediatric Cancer Patients in Different Treatment Phases: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(8), 4253. https://doi.org/10.3390/ijerph18084253