
Effects of a Clinically Indicated Peripheral Intravenous Replacement on Indwelling Time and Complications of Peripheral Intravenous Catheters in Pediatric Patients: A Randomized Controlled Trial


Abstract
1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Design and Population
3.1.1. Design
3.1.2. Participant Sample and Setting
3.1.3. Sample Size Calculation
3.1.4. Ethical Consideration
3.1.5. Intervention Program and Data Collection Process
3.2. Outcome Measures
3.2.1. Pediatric Patients
The Infusion Nurses Society Infiltration Scale (INSIS)
The Occlusion Scale (OS)
The Infusion Nurses Society Phlebitis Scale (INSPS)
Demographic and Clinical Characteristics
3.2.2. Family Caregivers
Demographic and Care Characteristics of Family Caregivers
3.3. Statistical Methods
4. Results
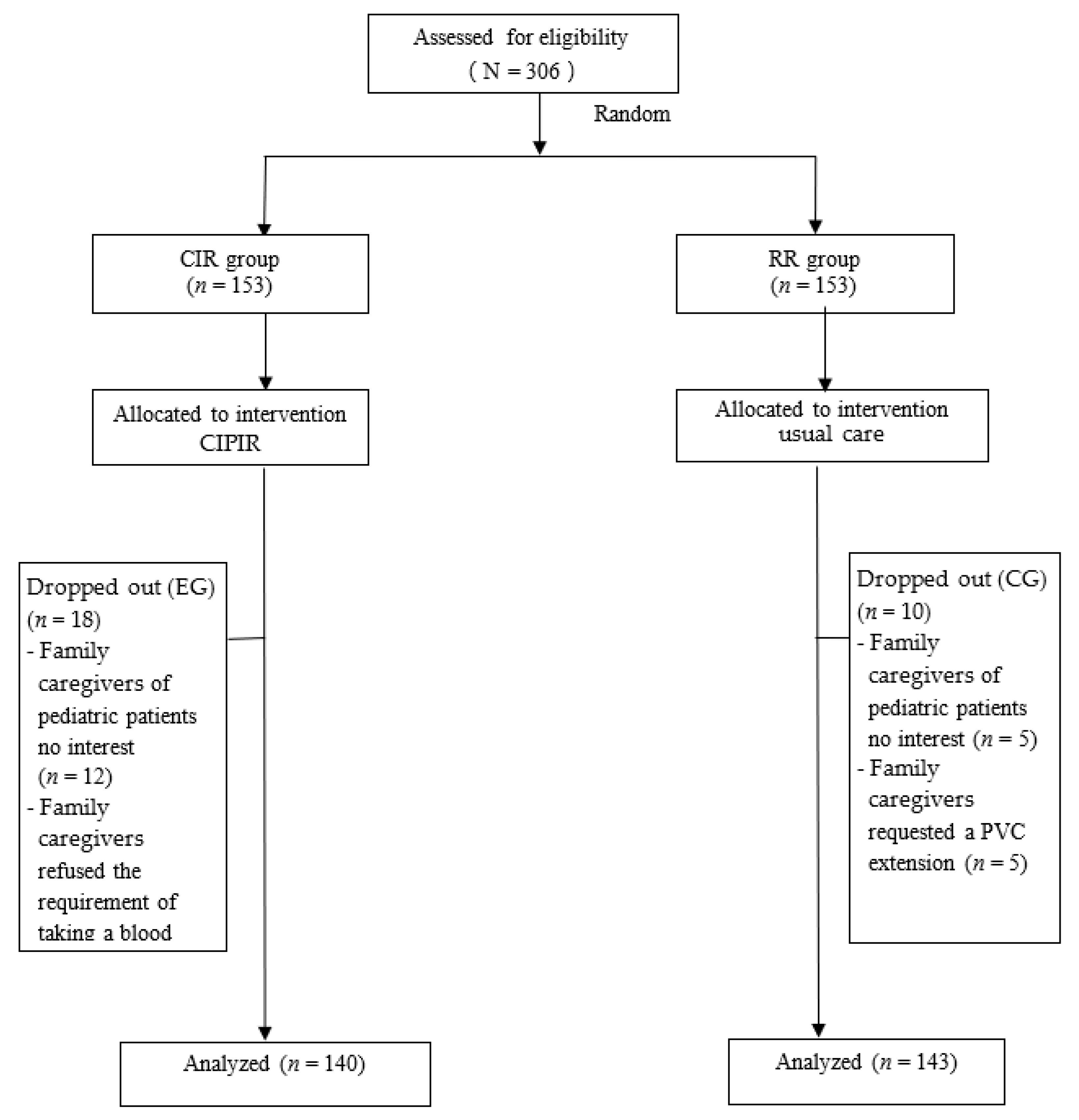
4.1. Study Participant Flow
4.2. Pediatric Patients and Disease Characteristics
4.3. Indwelling Time and Rates of Complications Associated with Peripheral Intravenous Catheters (PVCs) at Post-Test between the Two Groups
4.4. Relative Risk, Number Needed to Treat, Relative Risk Reduction, and Absolute Risk Reduction between the Two Groups
5. Discussion
6. Conclusions
6.1. Conclusion
6.2. Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Compliance with Ethical Standards
References
- Laudenbach, N.; Braun, C.A.; Klaverkamp, L.; Hedman-Dennis, S. Peripheral IV stabilization and the rate of complications in children: An exploratory study. J. Pediatr. Nurs. 2014, 29, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Reigart, J.R.; Chamberlain, K.H.; Eldridge, D.; O’Brien, E.S.; Freeland, K.D.; Larsen, P.; Goff, D.; Hartzog, T.H. Peripheral Intravenous Access in Pediatric Inpatients. Clin. Pediatr. 2011, 51, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Waitt, C.; Waitt, P.; Pirmohamed, M. Intravenous therapy. Postgrad. Med. J. 2004, 80, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Jeong, I.S.; Kim, K.L.; Park, K.J.; Jung, M.J.; Jun, S.S. The Effect of Intravenous Infiltration Management Program for Hospitalized Children. J. Pediatr. Nurs. 2016, 31, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Whitney, R.; Langhan, M. Vascular Access in Pediatric Patients in the Emergency Department: Types of Access, Indications, and Complications. Pediatr. Emerg. Med. Pract. 2017, 14, 1–20. [Google Scholar]
- O’Grady, N.P.; Alexander, M.; Burns, L.A.; Dellinger, E.P.; Garland, J.; Heard, S.O.; Lipsett, P.A.; Masur, H.; Mermel, L.A.; Pearson, M.L. The Healthcare Infection Control Practices Advisory Committee (HICPAC). Guidelines for the Prevention of Intravascular Catheter-Related Infections. Available online: https://www.cdc.gov/infectioncontrol/guidelines/bsi/index.html (accessed on 2 March 2021).
- Garland, J.S.; Dunne, W.M., Jr.; Havens, P.; Hintermeyer, M.; Bozzette, M.A.; Wincek, J.; Bromberger, T.; Seavers, M. Peripheral intravenous catheter complications in critically ill children: A prospective study. Pediatrics 1992, 89, 1145–1150. [Google Scholar] [PubMed]
- Oishi, L.A. The necessity of routinely replacing peripheral intravenous catheters in hospitalized children: A review of the literature. J. Intraven. Nurs. Off. Publ. Intraven. Nurses Soc. 2001, 24, 174–179. [Google Scholar]
- Shimandle, R.B.; Johnson, D.; Baker, M.; Stotland, N.; Karrison, T.; Arnow, P.M. Safety of Peripheral Intravenous Catheters in Children. Infect. Control Hosp. Epidemiol. 1999, 20, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Foster, L.; Wallis, M.; Paterson, B.; James, H. A Descriptive Study of Peripheral Intravenous Catheters in Patients Admitted to a Pediatric Unit in One Australian Hospital. J. Infus. Nurs. 2002, 25, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Chen, L.; Kong, D.; Lyu, F.; Luan, L.; Yang, L. Incidence, risk factors and medical cost of peripheral intravenous catheter-related complications in hospitalised adult patients. J. Vasc. Access 2020, 10, 1129729820978124. [Google Scholar] [CrossRef]
- King, M.A.; Garrison, M.M.; Vavilala, M.S.; Zimmerman, J.J.; Rivara, F.P. Complications associated with arterial catheterization in children. Pediatr. Crit. Care Med. 2008, 9, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Cicolini, G.; Manzoli, L.; Simonetti, V.; Flacco, M.E.; Comparcini, D.; Capasso, L.; Di Baldassarre, A.; Eltaji Elfarouki, G. Phlebitis risk varies by peripheral venous catheter site and increases after 96 hours: A large multi-centre prospective study. J. Adv. Nurs. 2014, 70, 2539–2549. [Google Scholar] [CrossRef]
- Bregenzer, T.; Conen, D.; Sakmann, P.; Widmer, A.F. Is Routine Replacement of Peripheral Intravenous Catheters Necessary? Arch. Intern. Med. 1998, 158, 151–156. [Google Scholar] [CrossRef]
- Rickard, C.M.; Webster, J.; Wallis, M.C.; Marsh, N.; McGrail, M.R.; French, V.; Foster, L.; Gallagher, P.; Gowardman, J.R.; Zhang, L. Routine versus clinically indicated replacement of peripheral intravenous catheters: A ran-domised controlled equivalence trial. Lancet 2012, 380, 1066–1074. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Tutorials Quant. Methods Psychol. 2007, 3, 79. [Google Scholar] [CrossRef][Green Version]
- Webster, J.; Osborne, S.; Rickard, C.M.; Marsh, N. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst. Rev. 2019, 1, CD007798. [Google Scholar] [CrossRef] [PubMed]
- Infusion Nurses Society. Infusion nursing standards of practice. J. Infus. Nurs. 2006, 9, S1–S92.
- Groll, D.; Davies, B.; Mac Donald, J.; Nelson, S.; Virani, T. Evaluation of the psychometric properties of the phlebitis and infil-tration scales for the assessment of complications of peripheral vascular access devices. J. Infus. Nurs. 2010, 33, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Morrison, K.; Holt, K.E. The Effectiveness of Clinically Indicated Replacement of Peripheral Intravenous Catheters: An Evidence Review With Implications for Clinical Practice. Worldviews Evid. Based Nurs. 2015, 12, 187–198. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | EG (n = 140) | CG (n = 143) | χ2/t | p |
|---|---|---|---|---|
| n(%)/Mean (SE) | n(%)/Mean (SE) | |||
| Age | 3.44(0.34) | 4.42(0.36) | 1.939 | 0.053 |
| Gender | 1.849 | 0.174 | ||
| Male | 68(48.6) | 81(56.6) | ||
| Female | 72(51.4) | 62(43.4) | ||
| Diagnosis | 10.734 | 0.294 a | ||
| Respiratory system | 59(42.2) | 76(53.1) | ||
| Cardiovascular System | 0(0) | 1(0.7) | ||
| Blood system | 1(0.7) | 1(0.7) | ||
| Gastrointestinal system | 24(17.2) | 16(11.2) | ||
| Urinary tract system | 34(24.3) | 28(19.6) | ||
| Nervous system | 1(0.7) | 3(2.1) | ||
| Skin system | 10(7.1) | 3(2.1) | ||
| Musculoskeletal system | 1(0.7) | 1(0.7) | ||
| Immune system | 2(1.4) | 3(2.1) | ||
| Virus infection | 8(5.7) | 11(7.7) | ||
| Catheter site | 0.652 | 0.885 | ||
| Right forearm or hand | 60(42.9) | 62(43.4) | ||
| Left forearm or hand | 64(45.7) | 68(47.5) | ||
| Right lower extremity | 10(7.1) | 7(4.9) | ||
| Left lower extremity | 6(4.3) | 6(4.2) | ||
| Hospital length of stay (LOS) | 6.46(0.23) | 5.88(0.24) |
| Characteristics | EG (n = 140) | CG (n = 143) | χ2/t | p |
|---|---|---|---|---|
| n(%)/Mean (SE) | n(%)/Mean (SE) | |||
| Indwelling time of PVCs (hour) | 113.06(2.42) | 65.67(0.88) | −18.447 | 0.001 |
| Complication | ||||
| Infiltration | 2.193 | 0.139 | ||
| No | 125(89.3) | 119(83.2) | ||
| Yes | 15(10.7) | 24(16.8) | ||
| Occlusion | 0.498 | 0.481 | ||
| No | 133(95.0) | 133(93.0) | ||
| Yes | 7(5.0) | 10(7.0) | ||
| Phlebitis | 3.865 a | 0.050 | ||
| Level 0 | 132(94.3) | 141(98.6) | ||
| Level 1 | 8(100) | 2(100) | ||
| Level 2 | 0(0) | 0(0) | ||
| Level 3 | 0(0) | 0(0) | ||
| Level 4 | 0(0) | 0(0) |
| Characteristics | EG (n = 140) | CG (n = 143) | Odds Ratio | 95%CI |
|---|---|---|---|---|
| n(%)/Mean (SE) | n(%)/Mean (SE) | |||
| Infiltration | 0.595 a | 0.298–1.189 | ||
| No | 125(89.3) | 119(83.2) | ||
| Yes | 15(10.7) | 24(16.8) | ||
| Occlusion | 0.700 a | 0.259–1.894 | ||
| No | 133(95.0) | 133(93.0) | ||
| Yes | 7(5.0) | 10(7.0) | ||
| Phlebitis | 4.273 a | 0.891–20.488 | ||
| Level 0 | 132(94.3) | 141(98.6) | ||
| Level 1 | 8(100) | 2(100) | ||
| Level 2 | 0(0) | 0(0) | ||
| Level 3 | 0(0) | 0(0) | ||
| Level 4 | 0(0) | 0(0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-W.; Chen, S.-C.; Huang, F.-Y.; Lee, M.-Y.; Chang, C.-C. Effects of a Clinically Indicated Peripheral Intravenous Replacement on Indwelling Time and Complications of Peripheral Intravenous Catheters in Pediatric Patients: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3795. https://doi.org/10.3390/ijerph18073795
Lin S-W, Chen S-C, Huang F-Y, Lee M-Y, Chang C-C. Effects of a Clinically Indicated Peripheral Intravenous Replacement on Indwelling Time and Complications of Peripheral Intravenous Catheters in Pediatric Patients: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(7):3795. https://doi.org/10.3390/ijerph18073795
Chicago/Turabian StyleLin, Su-Wen, Shu-Ching Chen, Fang-Yi Huang, Ming-Ying Lee, and Chun-Chu Chang. 2021. "Effects of a Clinically Indicated Peripheral Intravenous Replacement on Indwelling Time and Complications of Peripheral Intravenous Catheters in Pediatric Patients: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 7: 3795. https://doi.org/10.3390/ijerph18073795
APA StyleLin, S.-W., Chen, S.-C., Huang, F.-Y., Lee, M.-Y., & Chang, C.-C. (2021). Effects of a Clinically Indicated Peripheral Intravenous Replacement on Indwelling Time and Complications of Peripheral Intravenous Catheters in Pediatric Patients: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(7), 3795. https://doi.org/10.3390/ijerph18073795