
Changes in the Trunk and Lower Extremity Kinematics Due to Fatigue Can Predispose to Chronic Injuries in Cycling

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Data Processing and Analysis
2.4. Statistical Analysis
3. Results
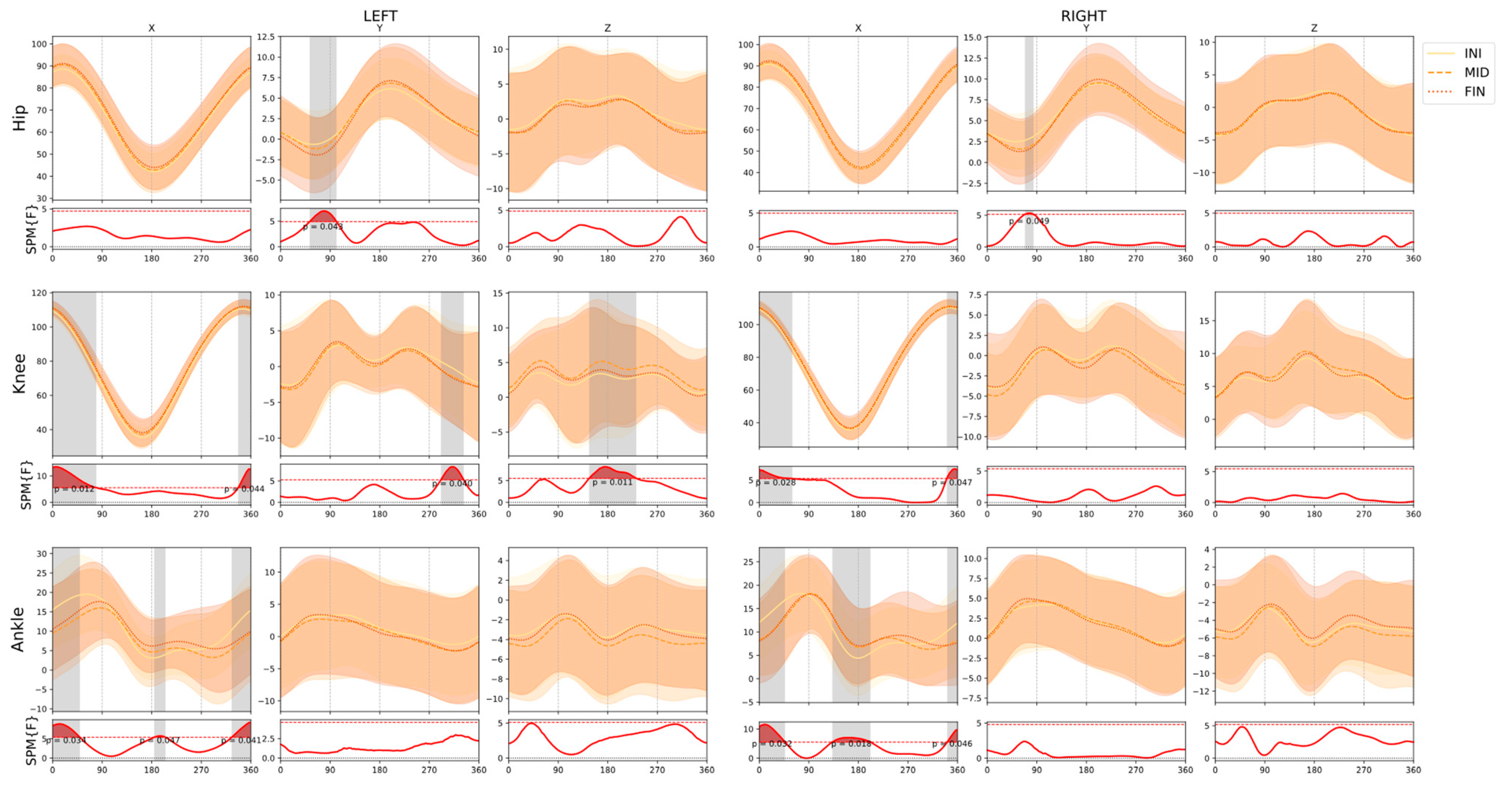
3.1. Effects of Fatigue
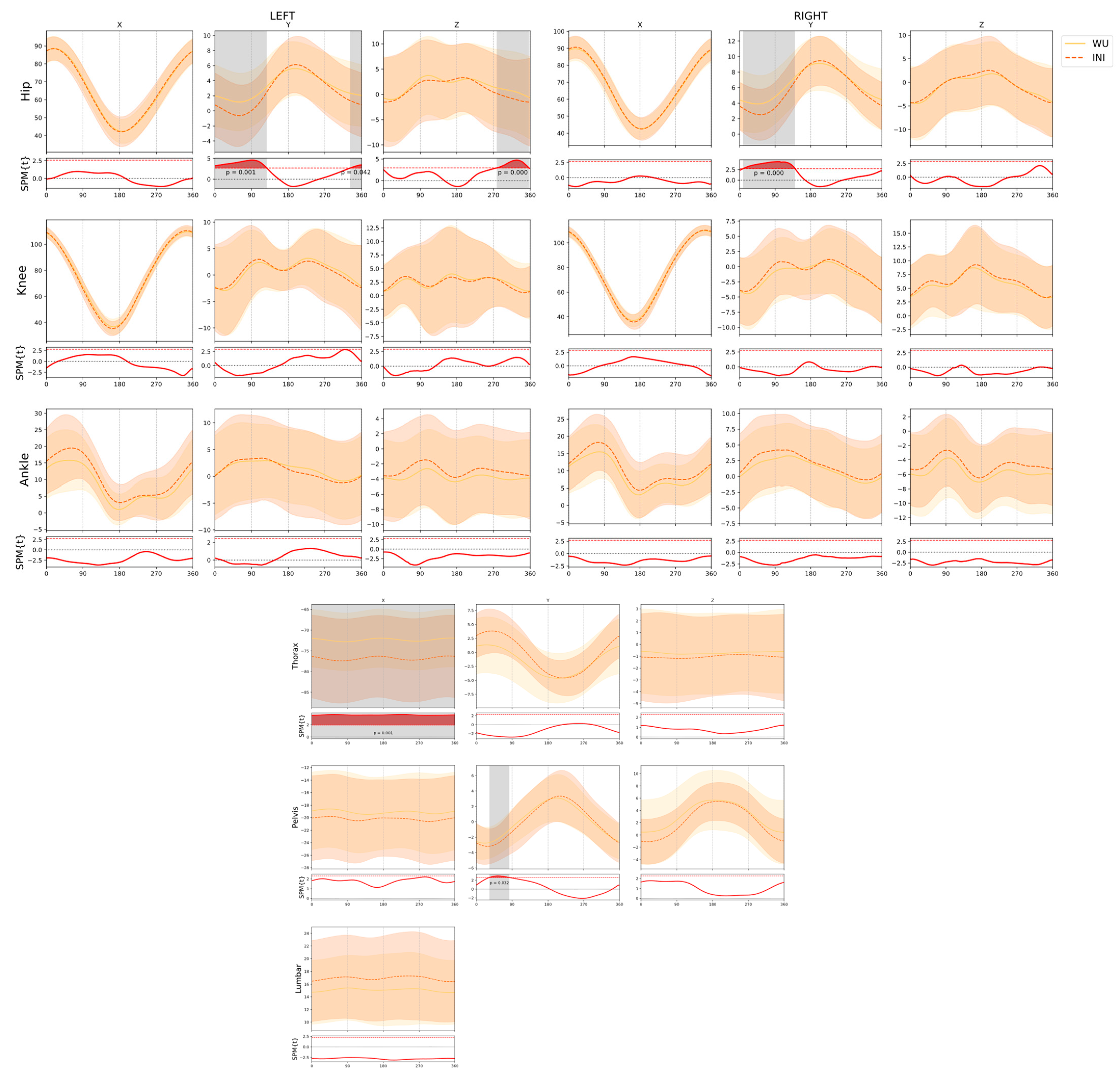
3.2. Effects of Intensity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LBP | Low back pain |
| FTP | Functional threshold power |
| ROM | Range of movement |
| ANOVA | Analysis of variance |
| 2D | Two dimensions |
| 3D | Three dimensions |
| SPM | Statistical parametric mapping |
| WU | Warm-up |
| INI | Initial moment of the test |
| MID | Middle moment of the test |
| FIN | Final moment of the test |
References
- Swart, J.; Holliday, W. Cycling Biomechanics Optimization—The (R) Evolution of Bicycle Fitting. Curr. Sports Med. Rep. 2019, 18, 490–496. [Google Scholar] [CrossRef]
- García-López, J.; Díez-Leal, S.; Ogueta-Alday, A.; Larrazabal, J.; Rodríguez-Marroyo, J.A. Differences in pedalling technique between road cyclists of different competitive levels. J. Sports Sci. 2016, 34, 1619–1626. [Google Scholar] [CrossRef] [PubMed]
- Kordi, M.; Fullerton, C.; Passfield, L.; Parker Simpson, L. Influence of upright versus time trial cycling position on determination of critical power and W′ in trained cyclists. Eur. J. Sport Sci. 2019, 19, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Fintelman, D.; Sterling, M.; Hemida, H.; Li, F.X. Effect of different aerodynamic time trial cycling positions on muscle activation and crank torque. Scand. J. Med. Sci. Sports 2016, 26, 528–534. [Google Scholar] [CrossRef]
- Merkes, P.F.; Menaspà, P.; Abbiss, C.R. Power output, cadence, and torque are similar between the forward standing and traditional sprint cycling positions. Scand. J. Med. Sci. Sports 2020, 30, 64–73. [Google Scholar] [CrossRef]
- Bini, R.R. The need for a link between bike fitting and injury risk. J. Sci. Cycl. 2016, 5, 1–2. [Google Scholar]
- Van Hoof, W.; Volkaerts, K.; O’Sullivan, K.; Verschueren, S.; Dankaerts, W. Comparing lower lumbar kinematics in cyclists with low back pain (flexion pattern) versus asymptomatic controls–field study using a wireless posture monitoring system. Man. Ther. 2012, 17, 312–317. [Google Scholar] [CrossRef]
- Van der Walt, A.; van Rensberg, D.J.; Fletcher, L.; Grant, C.C.; Van Der Walt, A.J. Non-traumatic injury profile of amateur cyclists. S. Afr. J. Sports Med. 2014, 26, 119–122. [Google Scholar] [CrossRef]
- Dingwell, J.B.; Joubert, J.E.; Diefenthaeler, F.; Trinity, J.D. Changes in muscle activity and kinematics of highly trained cyclists during fatigue. IEEE Trans. Biomed. Eng. 2008, 55, 2666–2674. [Google Scholar] [CrossRef]
- Bini, R.R.; Diefenthaeler, F.; Mota, C.B. Fatigue effects on the coordinative pattern during cycling: Kinetics and kinematics evaluation. J. Electromyogr. Kinesiol. 2010, 20, 102–107. [Google Scholar] [CrossRef]
- Sayers, M.G.; Tweddle, A.L.; Every, J.; Wiegand, A. Changes in drive phase lower limb kinematics during a 60 min cycling time trial. J. Sci. Med. Sport 2012, 15, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Sayers, M.; Tweddle, A.L. Thorax and pelvis kinematics change during sustained cycling. Int. J. Sports Med. 2012, 33, 314–390. [Google Scholar] [CrossRef] [PubMed]
- Juker, D.; McGill, S.; Kropf, P. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during cycling. J. Appl. Biomech. 1998, 14, 428–438. [Google Scholar] [CrossRef][Green Version]
- Streisfeld, G.M.; Bartoszek, C.; Creran, E.; Inge, B.; McShane, M.D.; Johnston, T. Relationship between body positioning, muscle activity, and spinal kinematics in cyclists with and without low back pain: A systematic review. Sports Health 2017, 9, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Fife, A.N.; Buddhadev, H.H.; Suprak, D.N.; Paxson, S.B.; San Juan, J.G. Effect of Q-factor manipulation via pedal spacers on lower limb frontal plane kinematics during cycling. J. Sci. Cycl. 2020, 9, 33–43. [Google Scholar] [CrossRef]
- Pouliquen, C.; Nicolas, G.; Bideau, B.; Garo, G.; Megret, A.; Delamarche, P.; Bideau, N. Spatiotemporal analysis of 3D kinematic asymmetry in professional cycling during an incremental test to exhaustion. J. Sports Sci. 2018, 36, 2155–2163. [Google Scholar] [CrossRef]
- Gregersen, C.S.; Hull, M.L. Non-driving intersegmental knee moments in cycling computed using a model that includes three-dimensional kinematics of the shank/foot and the effect of simplifying assumptions. J. Biomech. 2003, 36, 803–813. [Google Scholar] [CrossRef]
- Bini, R.R.; Bini, A.F. Potential factors associated with knee pain in cyclists: A systematic review. Open Access J. Sports Med. 2018, 9, 99. [Google Scholar] [CrossRef]
- Gatti, A.A.; Keir, P.J.; Noseworthy, M.D.; Beauchamp, M.K.; Maly, M.R. Hip and ankle kinematics are the most important predictors of knee joint loading during bicycling. J. Sci. Med. Sport 2021, 24, 98–104. [Google Scholar] [CrossRef]
- Dettori, N.J.; Norvell, D.C. Non-traumatic bicycle injuries. Sports Med. 2006, 36, 7–18. [Google Scholar] [CrossRef]
- Bini, R.R.; Diefenthaeler, F. Kinetics and kinematics analysis of incremental cycling to exhaustion. Sports Biomech. 2010, 9, 223–235. [Google Scholar] [CrossRef]
- Holliday, W.; Theo, R.; Fisher, J.; Swart, J. Cycling: Joint kinematics and muscle activity during differing intensities. Sports Biomech. 2019, 2, 1–15. [Google Scholar] [CrossRef]
- Allen, H.; Coggan, A.R.; McGregor, S. Training and Racing with a Power Meter; VeloPress: Boulder, CO, USA, 2019. [Google Scholar]
- Edeline, O.; Polin, D.; Tourny-Chollet, C.; Weber, J. Effect of workload on bilateral pedaling kinematics in non-trained cyclists. J. Hum. Mov. Stud. 2004, 46, 493–518. [Google Scholar]
- Fonda, B.; Sarabon, N.; Li, F.-X. Validity and reliability of different kinematics methods used for bike fitting. J. Sports Sci. 2014, 32, 940–946. [Google Scholar] [CrossRef]
- Bini, R.R.; Hume, P.A.; Lanferdini, F.J.; Vaz, M.A. Effects of moving forward or backward on the saddle on knee joint forces during cycling. Phys. Ther. Sport 2013, 14, 23–27. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef]
- Zadow, E.K.; Fell, J.W.; Kitic, C.M. The reliability of a laboratory-based 4 km cycle time trial on a Wahoo KICKR power trainer. J. Sci. Cycl. 2016, 5, 23–27. [Google Scholar]
- Fukuchi, R.K.; Fukuchi, C.A.; Duarte, M. A public dataset of running biomechanics and the effects of running speed on lower extremity kinematics and kinetics. PeerJ 2017, 5, e3298. [Google Scholar] [CrossRef]
- Rodrigues, P.; Chang, R.; TenBroek, T.; van Emmerik, R.; Hamill, J. Evaluating the coupling between foot pronation and tibial internal rotation continuously using vector coding. J. Appl. Biomech. 2015, 31, 88–94. [Google Scholar] [CrossRef]
- Bishop, D. Warm-up II: Performance changes following active warm up on exercise performance. Sports Med. 2003, 33, 483–498. [Google Scholar] [CrossRef]
- Muyor, J.; Zabala, M. Road cycling and mountain biking produces adaptations on the spine and hamstring extensibility. Int. J. Sports Med. 2016, 37, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Brown, N.A. Joint-specific power production and fatigue during maximal cycling. J. Biomech. 2009, 42, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Javaloyes, A.; Sarabia, J.M.; Lamberts, R.P.; Plews, D.; Moya-Ramon, M. Training prescription guided by heart rate variability vs. block periodization in well-trained cyclists. J. Strength Cond. Res. 2020, 34, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Harrington, M.; Zavatsky, A.; Lawson, S.; Yuan, Z.; Theologis, T. Prediction of the hip joint centre in adults, children, and patients with cerebral palsy based on magnetic resonance imaging. J. Biomech. 2007, 40, 595–602. [Google Scholar] [CrossRef] [PubMed]
- McClelland, J.A.; Webster, K.E.; Grant, C.; Feller, J. Alternative modelling procedures for pelvic marker occlusion during motion analysis. Gait Posture 2010, 31, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Akagi, M.; Nakamura, T. The functional flexion-extension axis of the knee corresponds to the surgical epicondylar axis: In vivo analysis using a biplanar image-matching technique. J. Arthroplast. 2005, 20, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Churchill, D.L.; Incavo, S.J.; Johnson, C.C.; Beynnon, B.D. The transepicondylar axis approximates the optimal flexion axis of the knee. Clin. Orthop. Relat. Res. 1998, 356, 111–118. [Google Scholar] [CrossRef]
- Nair, S.P.; Gibbs, S.; Arnold, G.; Abboud, R.; Wang, W. A method to calculate the centre of the ankle joint: A comparison with the Vicon® Plug-in-Gait model. Clin. Biomech. 2010, 25, 582–587. [Google Scholar] [CrossRef]
- Vanwanseele, B.; Parker, D.; Coolican, M. Frontal knee alignment: Three-dimensional marker positions and clinical assessment. Clin. Orthop. Relat. Res. 2009, 467, 504–509. [Google Scholar] [CrossRef]
- Hamill, J.; Selbie, W.S.; Kepple, T.M. Three-dimensional kinematics. In Research Methods in Biomechanics, 2nd ed.; Robertson, G., Caldwell, G., Hamill, J., Kamen, G., Whittlesey, S., Eds.; Human Kinetics: Champaign, IL, USA, 2014; pp. 35–60. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Davis, K.; Marras, W. The effects of motion on trunk biomechanics. Clin. Biomech. 2000, 15, 703–717. [Google Scholar] [CrossRef]
- Joseph, S.; Ganason, R.; Jalil, A.P.; Aizam, Z.S.; Wilson, B. A functional biomechanical analysis of an elite cyclist. In Proceedings of the ISBS-Conference Proceedings Archive, Salzburg, Austria, 14–18 July 2006. [Google Scholar]
- Sánchez-Zuriaga, D.; Adams, M.A.; Dolan, P. Is activation of the back muscles impaired by creep or muscle fatigue? Spine 2010, 35, 517–525. [Google Scholar] [CrossRef]
- Clarsen, B.; Krosshaug, T.; Bahr, R. Overuse injuries in professional road cyclists. Am. J. Sports Med. 2010, 38, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, J.; Balasubramanian, V. Low back pain and muscle fatigue due to road cycling—An sEMG study. J. Bodyw. Mov. Ther. 2007, 11, 260–266. [Google Scholar] [CrossRef]
- Burnett, A.F.; Cornelius, M.W.; Dankaerts, W.; O’Sullivan, P.B. Spinal kinematics and trunk muscle activity in cyclists: A comparison between healthy controls and non-specific chronic low back pain subjects—A pilot investigation. Man. Ther. 2004, 9, 211–219. [Google Scholar] [CrossRef]
- Marsden, M. Lower back pain in cyclists: A review of epidemiology, pathomechanics and risk factors. Int. Sportmed. J. 2010, 11, 216–225. [Google Scholar]
- Zajac, F.E.; Neptune, R.R.; Kautz, S.A. Biomechanics and muscle coordination of human walking: Part I: Introduction to concepts, power transfer, dynamics and simulations. Gait Posture 2002, 16, 215–232. [Google Scholar] [CrossRef]
- Buckeridge, E.M.; Bull, A.M.; McGregor, A.H. Biomechanical determinants of elite rowing technique and performance. Scand. J. Med. Sci. Sports 2015, 25, e176–e183. [Google Scholar] [CrossRef]
- Ferrer-Roca, V.; Bescós, R.; Roig, A.; Galilea, P.; Valero, O.; García-López, J. Acute effects of small changes in bicycle saddle height on gross efficiency and lower limb kinematics. J. Strength Cond. Res. 2014, 28, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Korff, T.; Romer, L.M.; Mayhew, I.; Martin, J.C. Effect of pedaling technique on mechanical effectiveness and efficiency in cyclists. Med. Sci. Sports Exerc. 2007, 39, 991. [Google Scholar] [CrossRef] [PubMed]
- Carpes, F.P.; Mota, C.B.; Faria, I.E. On the bilateral asymmetry during running and cycling–A review considering leg preference. Phys. Ther. Sport 2010, 11, 136–142. [Google Scholar] [CrossRef]
- Bailey, M.; Maillardet, F.; Messenger, N. Kinematics of cycling in relation to anterior knee pain and patellar tendinitis. J. Sports Sci. 2003, 21, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Abt, J.P.; Smoliga, J.M.; Brick, M.J.; Jolly, J.T.; Lephart, S.M.; Fu, F.H. Relationship between cycling mechanics and core stability. J. Strength Cond. Res. 2007, 21, 1300–1304. [Google Scholar] [PubMed]
- Asplund, C.; Ross, M. Core stability and bicycling. Curr. Sports Med. Rep. 2010, 9, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Barbado, D.; Irles-Vidal, B.; Prat-Luri, A.; García-Vaquero, M.P.; Vera-Garcia, F.J. Training intensity quantification of core stability exercises based on a smartphone accelerometer. PLoS ONE 2018, 13, e0208262. [Google Scholar] [CrossRef]
- Bini, R.R.; Dagnese, F.; Rocha, E.; Silveira, M.C.; Carpes, F.P.; Mota, C.B. Three-dimensional kinematics of competitive and recreational cyclists across different workloads during cycling. Eur. J. Sport Sci. 2016, 16, 553–559. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Joint and Axis | Cluster (Crank Angle) | p | Effect Size |
|---|---|---|---|---|
| INI vs. MID | Left Ankle_x | [329, 49] | 0.044 | 0.51 |
| Right Ankle_x | [341, 46] | <0.01 | 0.44 | |
| [133, 201] | <0.01 | 0.30 | ||
| Right Hip_y | [68, 83] | 0.022 | 0.31 | |
| Left Knee_x | [339, 39] | 0.045 | 0.31 | |
| Right Knee_x | [341, 59] | 0.018 | 0.24 | |
| Left Knee_y | [291, 331] | 0.023 | 0.18 | |
| Left Knee_z | [146, 231] | <0.01 | 0.19 | |
| Pelvis_y | [0, 13] | 0.049 | 0.40 | |
| Thorax_y | [172, 267] | 0.035 | 0.65 | |
| Thorax_z | [32, 53] | 0.016 | 0.22 | |
| INI vs. FIN | Left Ankle_x | [337, 31] | 0.040 | 0.49 |
| [184, 204] | <0.01 | 0.52 | ||
| Left Hip_y_ | [53, 101] | <0.01 | 0.31 | |
| Right Hip_y | [68, 83] | 0.017 | 0.36 | |
| Left Knee_x | [338, 78] | 0.045 | 0.28 | |
| Right Knee_x | [0, 33] | 0.033 | 0.24 | |
| Left Knee_y | [291, 332] | 0.011 | 0.20 | |
| Lumbar_x | [44, 60] | 0.049 | 0.39 | |
| [202, 242] | 0.047 | 0.38 | ||
| Pelvis_y | [336, 63] | <0.01 | 0.40 | |
| Thorax_y | [8, 71] | <0.01 | 0.48 | |
| [159, 277] | <0.01 | 0.70 | ||
| Thorax_z | [32, 53] | 0.036 | 0.31 | |
| MED vs. FIN | Left Knee_z | [158, 230] | <0.01 | 0.14 |
| Thorax_x | [347, 116] | 0.049 | 0.31 | |
| [204, 262] | 0.047 | 0.31 | ||
| Thorax_y | [8, 70] | 0.033 | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galindo-Martínez, A.; López-Valenciano, A.; Albaladejo-García, C.; Vallés-González, J.M.; Elvira, J.L.L. Changes in the Trunk and Lower Extremity Kinematics Due to Fatigue Can Predispose to Chronic Injuries in Cycling. Int. J. Environ. Res. Public Health 2021, 18, 3719. https://doi.org/10.3390/ijerph18073719
Galindo-Martínez A, López-Valenciano A, Albaladejo-García C, Vallés-González JM, Elvira JLL. Changes in the Trunk and Lower Extremity Kinematics Due to Fatigue Can Predispose to Chronic Injuries in Cycling. International Journal of Environmental Research and Public Health. 2021; 18(7):3719. https://doi.org/10.3390/ijerph18073719
Chicago/Turabian StyleGalindo-Martínez, Alberto, Alejandro López-Valenciano, Carlos Albaladejo-García, Juan M. Vallés-González, and Jose L. L. Elvira. 2021. "Changes in the Trunk and Lower Extremity Kinematics Due to Fatigue Can Predispose to Chronic Injuries in Cycling" International Journal of Environmental Research and Public Health 18, no. 7: 3719. https://doi.org/10.3390/ijerph18073719
APA StyleGalindo-Martínez, A., López-Valenciano, A., Albaladejo-García, C., Vallés-González, J. M., & Elvira, J. L. L. (2021). Changes in the Trunk and Lower Extremity Kinematics Due to Fatigue Can Predispose to Chronic Injuries in Cycling. International Journal of Environmental Research and Public Health, 18(7), 3719. https://doi.org/10.3390/ijerph18073719