
The Effect of Multiprobiotics on Memory and Attention in Fibromyalgia: A Pilot Randomized Controlled Trial




Abstract
1. Introduction
2. Materials and Methods
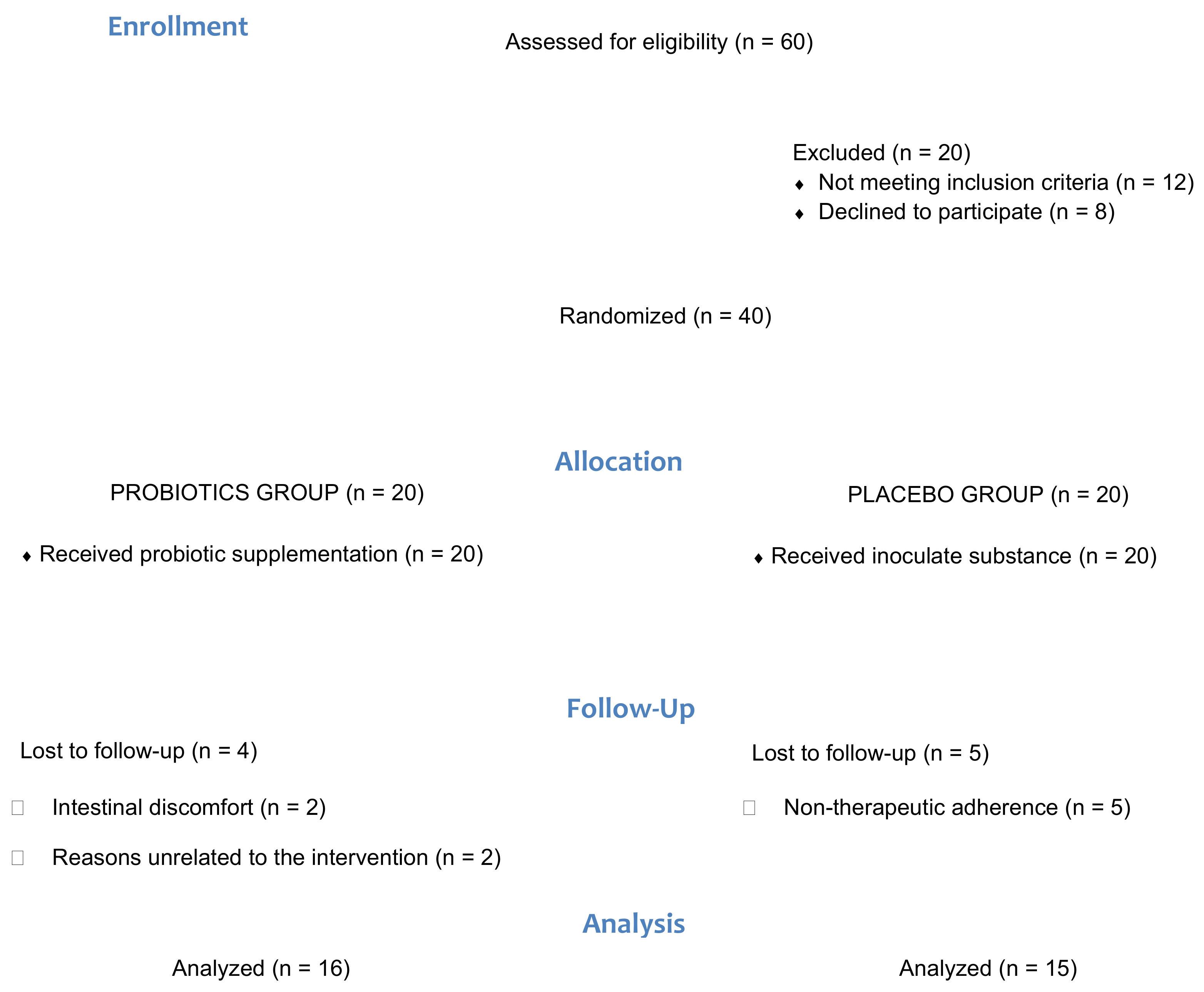
2.1. Study Design and Participants
2.2. Procedure
2.3. Outcome Measures
2.3.1. Demographic Measures
2.3.2. Cognitive Task
Memory Tasks: Working Memory
Attention Tasks
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Performance on Cognitive Task
3.2.1. Memory Task
3.2.2. Attention Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Glass, J.M. Fibromyalgia and cognition. J. Clin. Psychiatry 2008, 69 (Suppl. 2), 20–24. [Google Scholar]
- Glass, J.M. Review of Cognitive Dysfunction in Fibromyalgia: A Convergence on Working Memory and Attentional Control Impairments. Rheum. Dis. Clin. N. Am. 2009, 35, 299–311. [Google Scholar] [CrossRef]
- Verdejo-García, A.; López-Torrecillas, F.; Calandre, E.P.; Delgado-Rodríguez, A.; Bechara, A. Executive function and decision-making in women with fibromyalgia. Arch. Clin. Neuropsychol. 2009, 24, 113–122. [Google Scholar] [CrossRef]
- Park, D.C.; Glass, J.M.; Minear, M.; Crofford, L.J. Cognitive Function in Fibromyalgia Patients. Arthritis Rheum. 2001, 44, 2125–2133. [Google Scholar] [CrossRef]
- Leavitt, F.; Katz, R.S. Normalizing memory recall in fibromyalgia with rehearsal: A distraction-counteracting effect. Arthritis Care Res. 2009, 61, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Glass, J.M.; Williams, D.A.; Fernandez-Sanchez, M.L.; Kairys, A.; Barjola, P.; Heitzeg, M.M.; Clauw, D.J.; Schmidt-Wilcke, T. Executive function in chronic pain patients and healthy controls: Different cortical activation during response inhibition in fibromyalgia. J. Pain 2011, 12, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Minerbi, A.; Gonzalez, E.; Brereton, N.J.B.; Anjarkouchian, A.; Dewar, K.; Fitzcharles, M.A.; Chevalier, S.; Shir, Y. Altered microbiome composition in individuals with fibromyalgia. Pain 2019, 160, 2589–2602. [Google Scholar] [CrossRef]
- Freidin, M.B.; Stalteri, M.A.; Wells, P.M.; Lachance, G.; Baleanu, A.-F.; Bowyer, R.C.E.; Kurilshikov, A.; Zhernakova, A.; Steves, C.J.; Williams, F.M.K. An association between chronic widespread pain and the gut microbiome. Rheumatology 2020. [CrossRef]
- Moloney, R.D.; Johnson, A.C.; O’Mahony, S.M.; Dinan, T.G.; Greenwood-Van Meerveld, B.; Cryan, J.F. Stress and the Microbiota-Gut-Brain Axis in Visceral PaRelevance to Irritable Bowel Syndrome. CNS Neurosci. Ther. 2016, 22, 102–117. [Google Scholar] [CrossRef] [PubMed]
- Logan, A.C.; Katzman, M. Major depressive disorder: Probiotics may be an adjuvant therapy. Med. Hypotheses 2005, 64, 533–538. [Google Scholar] [CrossRef]
- Butt, H.; Dunstan, R.; McGregor, N.; Roberts, T. Bacterial colonosis in patients with persistent fatigue. In Proceedings of the AHMF International Clinical and Scientific Conference, Sydney, Australia, 1–2 December 2001. [Google Scholar]
- Mayer, E.A.; Tillisch, K.; Gupta, A.; Mayer, E.E.A.; Rhee, S.; Pothoulakis, C.; Mayer, E.E.A.; Cryan, J.; Dinan, T.; Mayer, E.E.A.; et al. Gut/brain axis and the microbiota. J. Clin. Investig. 2015, 125, 926–938. [Google Scholar] [CrossRef]
- Bercik, P.; Collins, S.M. The effects of inflammation, infection and antibiotics on the microbiota-gut-brain axis. Adv. Exp. Med. Biol. 2014, 817, 279–289. [Google Scholar]
- De Palma, G.; Collins, S.M.; Bercik, P.; Verdu, E.F. The microbiota-gut-brain axis in gastrointestinal disorders: Stressed bugs, stressed brain or both? J. Physiol. 2014, 592, 2989–2997. [Google Scholar] [CrossRef] [PubMed]
- Al-Nedawi, K.; Mian, M.F.; Hossain, N.; Karimi, K.; Mao, Y.-K.; Forsythe, P.; Min, K.K.; Stanisz, A.M.; Kunze, W.A.; Bienenstock, J. Gut commensal microvesicles reproduce parent bacterial signals to host immune and enteric nervous systems. FASEB J. 2015, 29, 684–695. [Google Scholar] [CrossRef] [PubMed]
- Chichlowski, M.; Rudolph, C. Visceral pain and gastrointestinal microbiome. J. Neurogastroenterol. Motil. 2015, 21, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef] [PubMed]
- WHO. Report of the Joint FAO/WHO Expert Consultation on Evaluation of Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria, Córdoba, Argentina, 1–4 October 2001; Food and Agriculture Organization of the United Nations: Quebec City, QC, Canada, 2001; 30p. [Google Scholar]
- Hardy, H.; Harris, J.; Lyon, E.; Beal, J.; Foey, A.D. Probiotics, prebiotics and immunomodulation of gut mucosal defences: Homeostasis and immunopathology. Nutrients 2013, 5, 1869–1912. [Google Scholar] [CrossRef]
- Wichmann, A.; Allahyar, A.; Greiner, T.U.; Plovier, H.; Lundén, G.Ö.; Larsson, T.; Drucker, D.J.; Delzenne, N.M.; Cani, P.D.; Bäckhed, F. Microbial Modulation of Energy Availability in the Colon Regulates Intestinal Transit. Cell Host Microbe 2013, 14, 582–590. [Google Scholar] [CrossRef]
- Minerbi, A.; Fitzcharles, M.A. Gut microbiome: Pertinence in fibromyalgia. Clin. Exp. Rheumatol. 2020, 38, 99–104. [Google Scholar]
- Rodrigo, L.; Blanco, I.; Bobes, J.; De Serres, F.J. Effect of one year of a gluten-free diet on the clinical evolution of irritable bowel syndrome plus fibromyalgia in patients with associated lymphocytic enteritis: A case-control study. Arthritis Res. Ther. 2014, 16, 1–11. [Google Scholar]
- Pusceddu, M.M.; Murray, K.; Gareau, M.G. Targeting the Microbiota, From Irritable Bowel Syndrome to Mood Disorders: Focus on Probiotics and Prebiotics. Curr. Pathobiol. Rep. 2018, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Penfold, S.; Denis, E.S.; Mazhar, M.N. The association between borderline personality disorder, fibromyalgia and chronic fatigue syndrome: Systematic review. BJPsych Open 2016, 2, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Roman, P.; Carrillo-Trabalón, F.; Sánchez-Labraca, N.; Cañadas, F.; Estévez, A.F.; Cardona, D. Are probiotic treatments useful on fibromyalgia syndrome or chronic fatigue syndrome patients? A systematic review. Benef. Microbes 2018, 9, 603–611. [Google Scholar] [CrossRef]
- Nelson, J.; Sjöblom, H.; Gjertsson, I.; Ulven, S.M.; Lindqvist, H.M.; Bärebring, L. Do Interventions with Diet or Dietary Supplements Reduce the Disease Activity Score in Rheumatoid Arthritis? A Systematic Review of Randomized Controlled Trials. Nutrients 2020, 12, 2991. [Google Scholar] [CrossRef] [PubMed]
- Erdrich, S.; Hawrelak, J.A.; Myers, S.P.; Harnett, J.E. Determining the association between fibromyalgia, the gut microbiome and its biomarkers: A systematic review. BMC Musculoskelet. Disord. 2020, 21, 1–12. [Google Scholar] [CrossRef]
- Pagliai, G.; Giangrandi, I.; Dinu, M.; Sofi, F.; Colombini, B. Nutritional interventions in the management of fibromyalgia syndrome. Nutrients 2020, 12, 2525. [Google Scholar] [CrossRef]
- Roman, P.; Estévez, Á.F.; Sánchez-Labraca, N.; Cañadas, F.; Miras, A.; Cardona Mena, D. Probióticos en fibromialgia: Diseño de un estudio piloto doble ciego y randomizado. Nutr. Hosp. 2017, 34, 1246–1251. [Google Scholar]
- Roman, P.; Estévez, A.F.; Miras, A.; Sánchez-Labraca, N.; Cañadas, F.; Vivas, A.B.; Cardona, D. A Pilot Randomized Controlled Trial to Explore Cognitive and Emotional Effects of Probiotics in Fibromyalgia. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Kato-Kataoka, A.; Nishida, K.; Takada, M.; Suda, K.; Kawai, M.; Shimizu, K.; Kushiro, A.; Hoshi, R.; Watanabe, O.; Igarashi, T.; et al. Fermented milk containing Lactobacillus casei strain Shirota prevents the onset of physical symptoms in medical students under academic examination stress. Benef. Microbes 2016, 7, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Allen, A.P.; Temko, A.; Hutch, W.; Kennedy, P.J.; Farid, N.; Murphy, E.; Boylan, G.; Bienenstock, J.; Cryan, J.F.; et al. Lost in translation? The potential psychobiotic Lactobacillus rhamnosus (JB-1) fails to modulate stress or cognitive performance in healthy male subjects. Brain. Behav. Immun. 2017, 61, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gonzalez, C.; Roman, P.; Rueda-Ruzafa, L.; Rodriguez-Arrastia, M.; Cardona, D. Effects of probiotics supplementation on dementia and cognitive impairment: A systematic review and meta-analysis of preclinical and clinical studies. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 110189. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Williams, C.; Brown, A. Impact of consuming a milk drink containing a probiotic on mood and cognition. Eur. J. Clin. Nutr. 2007, 61, 355–361. [Google Scholar] [CrossRef]
- Ibor, J. Escala de Inteligencia de Wechsler para Adultos III. Schizophr. Res. 2005, 147–156. [Google Scholar]
- Casey, B.J.; Trainor, R.J.; Orendi, J.L.; Schubert, A.B.; Nystrom, L.E.; Giedd, J.N.; Castellanos, F.X.; Haxby, J.V.; Noll, D.C.; Cohen, J.D.; et al. A developmental functional MRI study of prefrontal activation during performance of a Go-No-Go task. J. Cogn. Neurosci. 1997, 9, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Mayas, J.; Fuentes, L.J.; Ballesteros, S. Stroop interference and negative priming (NP) suppression in normal aging. Arch. Gerontol. Geriatr. 2012, 54, 333–338. [Google Scholar] [CrossRef]
- Inoue, T.; Kobayashi, Y.; Mori, N.; Sakagawa, M.; Xiao, J.Z.; Moritani, T.; Sakane, N.; Nagai, N. Effect of combined bifidobacteria supplementation and resistance training on cognitive function, body composition and bowel habits of healthy elderly subjects. Benef. Microbes 2018, 9, 843–853. [Google Scholar] [CrossRef]
- Rezaeiasl, Z.; Salami, M.; Sepehri, G. The effects of probiotic Lactobacillus and Bifidobacterium strains on memory and learning behavior, long-term potentiation (LTP), and some biochemical parameters in β-amyloid-induced rat’s model of Alzheimer’s disease. Prev. Nutr. Food Sci. 2019, 24, 265–273. [Google Scholar] [CrossRef]
- Rezaei Asl, Z.; Sepehri, G.; Salami, M. Probiotic treatment improves the impaired spatial cognitive performance and restores synaptic plasticity in an animal model of Alzheimer’s disease. Behav. Brain Res. 2019, 376, 112183. [Google Scholar] [CrossRef]
- Hwang, Y.H.; Park, S.; Paik, J.W.; Chae, S.W.; Kim, D.H.; Jeong, D.G.; Ha, E.; Kim, M.; Hong, G.; Park, S.H.; et al. Efficacy and safety of lactobacillus plantarum C29-fermented soybean (DW2009) in individuals with mild cognitive impairment: A 12-week, multi-center, randomized, double-blind, placebo-controlled clinical trial. Nutrients 2019, 11, 305. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Kuhara, T.; Oki, M.; Xiao, J.Z. Effects of bifidobacterium breve a1 on the cognitive function of older adults with memory complaints: A randomised, double-blind, placebo-controlled trial. Benef. Microbes 2019, 10, 511–520. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef]
- Rudzki, L.; Ostrowska, L.; Pawlak, D.; Małus, A.; Pawlak, K.; Waszkiewicz, N.; Szulc, A. Probiotic Lactobacillus Plantarum 299v decreases kynurenine concentration and improves cognitive functions in patients with major depression: A double-blind, randomized, placebo controlled study. Psychoneuroendocrinology 2019, 100, 213–222. [Google Scholar] [CrossRef]
- Chong, H.X.; Yusoff, N.A.A.; Hor, Y.Y.; Lew, L.C.; Jaafar, M.H.; Choi, S.B.; Yusoff, M.S.B.; Wahid, N.; Abdullah, M.F.I.L.; Zakaria, N.; et al. Lactobacillus plantarum DR7 alleviates stress and anxiety in adults: A randomised, double-blind, placebo-controlled study. Benef. Microbes 2019, 10, 355–373. [Google Scholar] [CrossRef]
- Lv, T.; Ye, M.; Luo, F.; Hu, B.; Wang, A.; Chen, J.; Yan, J.; He, Z.; Chen, F.; Qian, C.; et al. Probiotics treatment improves cognitive impairment in patients and animals: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 120, 159–172. [Google Scholar] [CrossRef]
- Frank, M.G.; Fonken, L.K.; Watkins, L.R.; Maier, S.F.; Lowry, C.A. Could Probiotics Be Used to Mitigate Neuroinflammation? ACS Chem. Neurosci. 2019, 10, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Claesson, M.J.; Cusack, S.; O’Sullivan, O.; Greene-Diniz, R.; De Weerd, H.; Flannery, E.; Marchesi, J.R.; Falush, D.; Dinan, T.; Fitzgerald, G.; et al. Composition, variability, and temporal stability of the intestinal microbiota of the elderly. Proc. Natl. Acad. Sci. USA 2011, 108, 4586–4591. [Google Scholar] [CrossRef]
- Blasco, G.; Moreno-Navarrete, J.M.; Rivero, M.; Pérez-Brocal, V.; Garre-Olmo, J.; Puig, J.; Daunis-i-Estadella, P.; Biarnés, C.; Gich, J.; Fernández-Aranda, F.; et al. The gut metagenome changes in parallel to waist circumference, brain iron deposition, and cognitive function. J. Clin. Endocrinol. Metab. 2017, 102, 2962–2973. [Google Scholar] [CrossRef] [PubMed]
- Heyck, M.; Ibarra, A. Microbiota and memory: A symbiotic therapy to counter cognitive decline? Brain Circ. 2019, 5, 124. [Google Scholar] [PubMed]
- Brüssow, H. Microbiota and healthy ageing: Observational and nutritional intervention studies. Microb. Biotechnol. 2013, 6, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Tsilioni, I.; Bawazeer, M. Mast Cells, Neuroinflammation and Pain in Fibromyalgia Syndrome. Front. Cell. Neurosci. 2019, 13, 353. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PROBIOTIC (n = 16) | PLACEBO (n = 15) | |
|---|---|---|
| Gender (%) | ||
| Men | 6.25 | 13.33 |
| Women | 93.75 | 86.67 |
| Age | 55.00 ± 8.37 | 50.27 ± 7.86 |
| Years of diagnosis | 8.56 ± 5.90 | 8.47 ± 5.80 |
| Formal education (years) | 12.75 ± 0.95 | 12.27 ± 1.29 |
| BMI (kg/m2) | 29.40 ± 1.64 | 30.23 ± 1.63 |
| PLACEBO (n = 15) | PROBIOTIC (n = 16) | |||
|---|---|---|---|---|
| PRE- | POST- | PRE- | POST- | |
| Forward | 8.42 (0.48) | 8.78 (0.48) | 8.06 (0.54) | 8.31 (0.59) |
| Reverse | 5.35 (0.26) | 5.50 (0.47) | 5.56 (0.60) | 5.62 (0.56) |
| PLACEBO (n = 12) | PROBIOTIC (n = 13) | |||
|---|---|---|---|---|
| PRE- | POST- | PRE- | POST- | |
| Forward | 4.92 (337) | 5.08 (37) | 5.00 (311) | 5.39 (288) |
| Reverse | 4.50 (324) | 4.83 (299) | 5.08 (356) | 4.92 (356) |
| PLACEBO (n = 12) | PROBIOTIC (n = 13) | |||
|---|---|---|---|---|
| PRE- | POST- | PRE- | POST- | |
| Forward | 4602 (378) | 4600 (474) | 3823 (362) | 3839 (454) |
| Reverse | 3998 (316) | 4520 (417) | 3911 (303) | 3615 (399) |
| PLACEBO (n = 12) | PROBIOTIC (n = 14) | |||
|---|---|---|---|---|
| PRE- | POST- | PRE- | POST- | |
| Go trials | 400 (47.3) | 378 (35.7) | 344 (43.8) | 365 (33.1) |
| PLACEBO (n = 11) | PROBIOTIC (n = 12) | |||
|---|---|---|---|---|
| PRE- | POST- | PRE- | POST- | |
| RTs | ||||
| Congruent | 1013 (60) | 998 (59) | 987 (58) | 979 (57) |
| Incongruent | 1094 (69) | 1044 (61) | 1075 (66) | 1065 (58) |
| Control | 1076 (68) | 1036 (57) | 1061 (66) | 1045 (55) |
| Ignored | 1051 (72) | 1023 (69) | 1052 (69) | 1050 (66) |
| Errors | ||||
| Congruent | 0.6 (0.4) | 0.5 (0.2) | 0.5 (0.4) | 0.7 (0.2) |
| Incongruent | 3.1 (2.8) | 2.3 (0.9) | 4.7 (2.7) | 1.6 (0.8) |
| Control | 2.5 (1.6) | 2.5 (0.9) | 4.8 (2.5) | 0.7 (0.9) |
| Ignored | 3.4 (2.5) | 1.4 (0.5) | 4.4 (2.4) | 0.7 (0.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardona, D.; Roman, P.; Cañadas, F.; Sánchez-Labraca, N. The Effect of Multiprobiotics on Memory and Attention in Fibromyalgia: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3543. https://doi.org/10.3390/ijerph18073543
Cardona D, Roman P, Cañadas F, Sánchez-Labraca N. The Effect of Multiprobiotics on Memory and Attention in Fibromyalgia: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(7):3543. https://doi.org/10.3390/ijerph18073543
Chicago/Turabian StyleCardona, Diana, Pablo Roman, Fernando Cañadas, and Nuria Sánchez-Labraca. 2021. "The Effect of Multiprobiotics on Memory and Attention in Fibromyalgia: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 7: 3543. https://doi.org/10.3390/ijerph18073543
APA StyleCardona, D., Roman, P., Cañadas, F., & Sánchez-Labraca, N. (2021). The Effect of Multiprobiotics on Memory and Attention in Fibromyalgia: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(7), 3543. https://doi.org/10.3390/ijerph18073543