
Gait Performance as an Indicator of Cognitive Deficit in Older People

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Materials and Testing
2.2.1. Anthropometric Variables
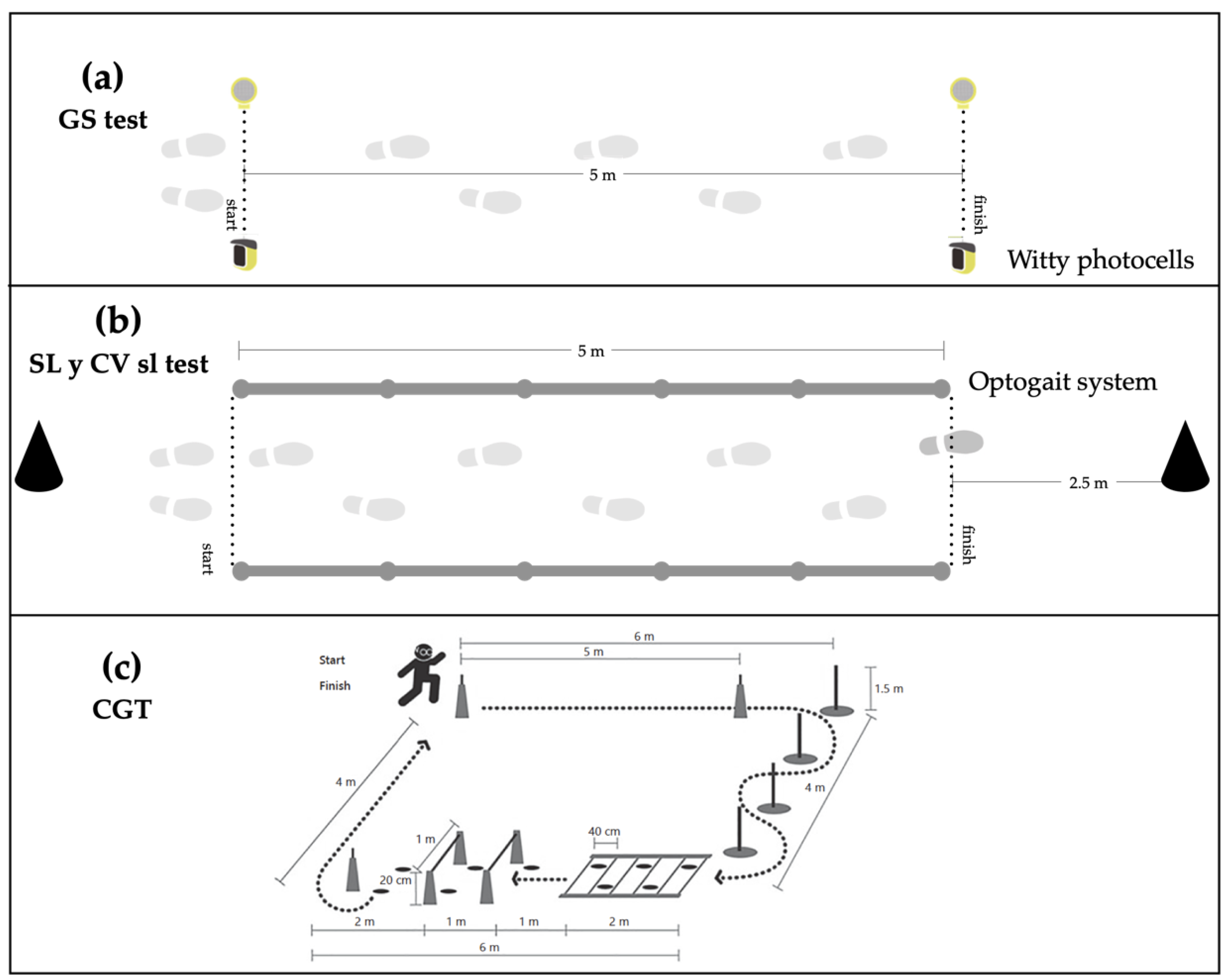
2.2.2. Gait Variables
2.2.3. Cognitive Measures
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CGT | Complex gait test |
| CV | Coefficient of variation |
| CV sl | Step coefficient of variability |
| GS | Gait speed |
| MCI | Mild cognitive impairment |
| MoCA | Montreal Cognitive Assessment |
| SL | Step length |
References
- Clouston, S.A.P.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The Dynamic Relationship Between Physical Function and Cognition in Longitudinal Aging Cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- Maclean, L.M.; Brown, L.J.E.; Khadra, H.; Astell, A.J. Observing prioritization effects on cognition and gait: The effect of increased cognitive load on cognitively healthy older adults’ dual-task performance. Gait Posture 2017, 53, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L.; McBurnie, M.A.; Bittner, V.; Tracy, R.P.; McNamara, R.; Arnold, A.; Newman, A.B. The 6-min Walk Test: A quick measure of functional status in elderly adults. Chest 2003, 123, 387–398. [Google Scholar] [CrossRef]
- De Cock, A.-M.; Fransen, E.; Perkisas, S.; Verhoeven, V.; Beauchet, O.; Remmen, R.; Vandewoude, M. Gait characteristics under different walking conditions: Association with the presence of cognitive impairment in community-dwelling older people. PLoS ONE 2017, 12, e0178566. [Google Scholar] [CrossRef]
- Bessot, N.; Polyte, R.; Quesney, M.; Bulla, J.; Gauthier, A. Diurnal gait fluctuations in single- and dual- task conditions. Chrono Int. 2020, 37, 836–844. [Google Scholar] [CrossRef]
- Hillel, I.; Gazit, E.; Nieuwboer, A.; Avanzino, L.; Rochester, L.; Cereatti, A.; Della Croce, U.; Rikkert, M.O.; Bloem, B.R.; Pelosin, E.; et al. Is every-day walking in older adults more analogous to dual-task walking or to usual walking? Elucidating the gaps between gait performance in the lab and during 24/7 monitoring. Eur. Rev. Aging Phys. Act. 2019, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Maidan, I.; Herman, T.; Deutsch, J.E.; Giladi, N.; Hausdorff, J.M. Virtual Reality for Gait Training: Can It Induce Motor Learning to Enhance Complex Walking and Reduce Fall Risk in Patients With Parkinson’s Disease? J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2011, 66, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef]
- Herrero, A.C.; Izquierdo, M. Ejercicio físico como intervención eficaz en el anciano frágil. An. Sist. Sanit. Navar. 2012, 35, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Mitchell, T.; Starrs, F.; Soucy, J.-P.; Thiel, A.; Paquette, C. Impaired Sensorimotor Processing During Complex Gait Precedes Behavioral Changes in Middle-aged Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2019, 74, 1861–1869. [Google Scholar] [CrossRef]
- Martin, K.L.; Blizzard, L.; Wood, A.G.; Srikanth, V.; Thomson, R.; Sanders, L.M.; Callisaya, M.L. Cognitive Function, Gait, and Gait Variability in Older People: A Population-Based Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2013, 68, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Muir, S.W.; Speechley, M. Dual-Task Complexity Affects Gait in People With Mild Cognitive Impairment: The Interplay Between Gait Variability, Dual Tasking, and Risk of Falls. Arch. Phys. Med. Rehabil. 2012, 93, 293–299. [Google Scholar] [CrossRef]
- Armstrong, D.M.; Drew, T. Discharges of pyramidal tract and other motor cortical neurones during locomotion in the cat. J. Physiol. 1984, 346, 471–495. [Google Scholar] [CrossRef]
- Rezola-Pardo, C.; Arrieta, H.; Gil, S.M.; Yanguas, J.J.; Iturburu, M.; Irazusta, J.; Sanz, B.; Rodriguez-Larrad, A. A randomized controlled trial protocol to test the efficacy of a dual-task multicomponent exercise program in the attenuation of frailty in long-term nursing home residents: Aging-ONDUAL-TASK study. BMC Geriatr. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of Physical Exercise Interventions on Gait-Related Dual-Task Interference in Older Adults: A Systematic Review and Meta-Analysis. Gerontology 2015, 62, 94–117. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pinillos, F.; Cozar-Barba, M.; Munoz-Jimenez, M.; Soto-Hermoso, V.; Latorre-Roman, P. Gait speed in older people: An easy test for detecting cognitive impairment, functional independence, and health state. Psychogeriatrics 2016, 16, 165–171. [Google Scholar] [CrossRef]
- Patel, P.; Lamar, M.; Bhatt, T. Effect of type of cognitive task and walking speed on cognitive-motor interference during dual-task walking. Neuroscience 2014, 260, 140–148. [Google Scholar] [CrossRef]
- Dubost, V.; Annweiler, C.; Aminian, K.; Najafi, B.; Herrmann, F.R.; Beauchet, O. Stride-to-stride variability while enumerating animal names among healthy young adults: Result of stride velocity or effect of attention-demanding task? Gait Posture 2008, 27, 138–143. [Google Scholar] [CrossRef]
- Gillain, S.; Dramé, M.; Lekeu, F.; Wojtasik, V.; Ricour, C.; Croisier, J.-L.; Salmon, E.; Petermans, J. Gait speed or gait variability, which one to use as a marker of risk to develop Alzheimer disease? A pilot study. Aging Clin. Exp. Res. 2016, 28, 249–255. [Google Scholar] [CrossRef]
- Kikkert, L.H.J.; Vuillerme, N.; van Campen, J.P.; Hortobágyi, T.; Lamoth, C.J. Walking ability to predict future cognitive decline in old adults: A scoping review. Ageing Res. Rev. 2016, 27, 1–14. [Google Scholar] [CrossRef]
- Tian, Q.; Chastan, N.; Bair, W.-N.; Resnick, S.M.; Ferrucci, L.; Studenski, S.A. The brain map of gait variability in aging, cognitive impairment and dementia—A systematic review. Neurosci. Biobehav. Rev. 2017, 74, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Klotzbier, T.J.; Schott, N. Cognitive-Motor Interference during Walking in Older Adults with Probable Mild Cognitive Impairment. Front. Aging Neurosci. 2017, 9, 350. [Google Scholar] [CrossRef]
- Inzitari, M.; Calle, A.; Esteve, A.; Casas, Á.; Torrents, N.; Martínez, N. ¿Mides la velocidad de la marcha en tu práctica diaria? Una revisión. Rev. Esp. Geriatr. Gerontol. 2017, 52, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Schapira, M.; Soriano, E.R.; Varela, M.; Kaplan, R.; Camera, L.A.; Mayorga, L.M. Gait Velocity as a Single Predictor of Adverse Events in Healthy Seniors Aged 75 Years and Older. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2005, 60, 1304–1309. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Dismobility in Older Adults. Arch. Phys. Med. Rehabil. 2015, 96, 1641–1645. [Google Scholar] [CrossRef]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef]
- Egerton, T.; Paterson, K.; Helbostad, J.L. The Association Between Gait Characteristics and Ambulatory Physical Activity in Older People: A Cross-Sectional and Longitudinal Observational Study Using Generation 100 Data. J. Aging Phys. Act. 2017, 25, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Van Schooten, K.S.; Pijnappels, M.; Rispens, S.M.; Elders, P.J.M.; Lips, P.; Daffertshofer, A.; Beek, P.J.; Van Dieën, J.H. Daily-Life Gait Quality as Predictor of Falls in Older People: A 1-Year Prospective Cohort Study. PLoS ONE 2016, 11, e0158623. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Sanford, A.M.; Orrell, M.; Tolson, D.; Abbatecola, A.M.; Arai, H.; Bauer, J.M.; Cruz-Jentoft, A.J.; Dong, B.; Ga, H.; Goel, A.; et al. An International Definition for “Nursing Home”. J. Am. Med. Dir. Assoc. 2015, 16, 181–184. [Google Scholar] [CrossRef]
- Gobbens, R.J.J.; van Assen, M.A.L.M.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M.G.A. The Tilburg Frailty Indicator: Psychometric Properties. J. Am. Med. Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef]
- Stellmann, J.P.; Neuhaus, A.; Götze, N.; Briken, S.; Lederer, C.; Schimpl, M.; Heesen, C.; Daumer, M. Ecological Validity of Walking Capacity Tests in Multiple Sclerosis. PLoS ONE 2015, 10, e0123822. [Google Scholar] [CrossRef] [PubMed]
- Iluz, T.; Weiss, A.; Gazit, E.; Tankus, A.; Brozgol, M.; Dorfman, M.; Mirelman, A.; Giladi, N.; Hausdorff, J.M. Can a Body-Fixed Sensor Reduce Heisenberg’s Uncertainty When It Comes to the Evaluation of Mobility? Effects of Aging and Fall Risk on Transitions in Daily Living. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2016, 71, 1459–1465. [Google Scholar] [CrossRef]
- Hertzog, C.; Kramer, A.F.; Wilson, R.S.; Lindenberger, U. Enrichment Effects on Adult Cognitive Development. Psychol. Sci. Public Interest 2008, 9, 1–65. [Google Scholar] [CrossRef]
- Savica, R.; Wennberg, A.M.V.; Hagen, C.; Edwards, K.; Roberts, R.O.; Hollman, J.H.; Knopman, D.S.; Boeve, B.F.; Machulda, M.M.; Petersen, R.C.; et al. Comparison of Gait Parameters for Predicting Cognitive Decline: The Mayo Clinic Study of Aging. J. Alzheimer’s Dis. 2016, 55, 559–567. [Google Scholar] [CrossRef]
- Byun, S.; Han, J.W.; Kim, T.H.; Kim, K.; Park, J.Y.; Suh, S.W.; Seo, J.Y.; So, Y.; Lee, K.H.; Lee, J.R.; et al. Gait Variability Can Predict the Risk of Cognitive Decline in Cognitively Normal Older People. Dement. Geriatr. Cogn. Disord. 2018, 45, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Vergara, I.; Bilbao, A.; Orive, M.; García-Gutierrez, S.; Navarro, G.; Quintana, J.M. Validation of the Spanish version of the Lawton IADL Scale for its application in elderly people. Health Qual. Life Outcomes 2012, 10, 130. [Google Scholar] [CrossRef]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Lienhard, K.; Schneider, D.; Maffiuletti, N.A. Validity of the Optogait photoelectric system for the assessment of spatiotemporal gait parameters. Med. Eng. Phys. 2013, 35, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Román, P.Á.; Muñoz-Jiménez, M.; Salas-Sánchez, J.; Consuegra-González, P.; Moreno Del Castillo, R.; Herrador-Sánchez, J.A.; López-Ivanco, M.D.A.; Linares-Jiménez, C.; Navas-Morales, J.F.; Párraga-Montilla, J.A. Complex Gait Is Related to Cognitive Functioning in Older People: A Cross-Sectional Study Providing an Innovative Test. Gerontology 2020, 66, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Maruta, C.; Guerreiro, M.; De Mendonça, A.; Hort, J.; Scheltens, P. The use of neuropsychological tests across Europe: The need for a consensus in the use of assessment tools for dementia. Eur. J. Neurol. 2011, 18, 279–285. [Google Scholar] [CrossRef]
- Tan, J.-P.; Li, N.; Gao, J.; Wang, L.-N.; Zhao, Y.-M.; Yu, B.-C.; Du, W.; Zhang, W.-J.; Cui, L.-Q.; Wang, Q.-S.; et al. Optimal Cutoff Scores for Dementia and Mild Cognitive Impairment of the Montreal Cognitive Assessment among Elderly and Oldest-Old Chinese Population. J. Alzheimer’s Dis. 2014, 43, 1403–1412. [Google Scholar] [CrossRef]
- Delgado, C.; Araneda, A.; Behrens, M.I. Validation of the Spanish-language version of the Montreal Cogni-tive Assessment test in adults older than 60 years. Neurologia 2019, 34, 376–385. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Ijmker, T.; Lamoth, C.J.C. Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 2012, 35, 126–130. [Google Scholar] [CrossRef]
- Pinedo, L.V.; Saavedra, P.J.O.; Jimeno, H.C. Velocidad de la marcha como indicador de fragilidad en adultos mayores de la comunidad en Lima, Perú. Rev. Esp. Geriatr. Gerontol. 2010, 45, 22–25. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Sarquis-Adamson, Y.; Kamkar, N.; Pieruccini-Faria, F.; Bray, N.; Cullen, S.; Mahon, J.; Titus, J.; Camicioli, R.; Borrie, M.; et al. Dual-task gait speed assessments with an electronic walkway and a stopwatch in older adults. A reliability study. Exp. Gerontol. 2020, 142, 111102. [Google Scholar] [CrossRef]
- Bielak, A.A.M.; Brydges, C.R.; Gutchess, A. Can Intraindividual Variability in Cognitive Speed Be Reduced by Physical Exercise? Results from the LIFE Study. J. Gerontol. Ser. B 2018, 74, 1335–1344. [Google Scholar] [CrossRef]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; Van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef]
- Muir, B.C.; Rietdyk, S.; Haddad, J.M. Gait initiation: The first four steps in adults aged 20–25 years, 65–79 years, and 80–91 years. Gait Posture 2014, 39, 490–494. [Google Scholar] [CrossRef]
- Bruening, D.A.; Baird, A.R.; Weaver, K.J.; Rasmussen, A.T. Whole body kinematic sex differences persist across non-dimensional gait speeds. PLoS ONE 2020, 15, e0237449. [Google Scholar] [CrossRef] [PubMed]
- Callisaya, M.L.; Blizzard, L.; Schmidt, M.D.; McGinley, J.L.; Srikanth, V.K. Ageing and gait variability--a population-based study of older people. Age Ageing 2010, 39, 191–197. [Google Scholar] [CrossRef]
- Ko, S.-U.; Tolea, M.I.; Hausdorff, J.M.; Ferrucci, L. Sex-specific differences in gait patterns of healthy older adults: Results from the Baltimore Longitudinal Study of Aging. J. Biomech. 2011, 44, 1974–1979. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Park, J.; Lee, B.-I.; Shin, K.J.; Yoo, S.; Kim, H.; Jang, W.; Kim, J.S.; Youn, J.; Oh, E. The Correlation between Cognition Screening Scores and Gait Status from Three-Dimensional Gait Analysis. J. Clin. Neurol. 2019, 15, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.; Triolo, F.; Nuara, A.; Welmer, A.-K.; Fratiglioni, L.; Vetrano, D.L. Measuring gait speed to better identify prodromal dementia. Exp. Gerontol. 2019, 124, 110625. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | n | Total Mean (SD) | n | Men Mean (SD) | n | Women Mean (SD) | p-Valor | n | 60–69 Years Mean (SD) a | n | 70–79 Years Mean (SD) b | n | >79 Years Mean (SD) c | p-Valor | Post Hoc Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 65 | 73.88 (9.56) | 22 | 74.86 (9.77) | 43 | 73.37 (9.52) | 0.556 | 25 | 65.08 (3.12) | 25 | 73.24 (2.36) | 16 | 88.06 (5.19) | <0.001 | |
| BMI (kg/m2) | 63 | 26.98 (3.44) | 21 | 27.51 (3.43) | 42 | 26.71 (3.46) | 0.394 | 23 | 26.31 (3.29) | 25 | 26.96 (3.36) | 15 | 28.04 (3.77) | 0.325 | |
| TV (hour/day) | 51 | 2.89 (1.52) | 18 | 3.02 (1.33) | 33 | 2.81 (1.62) | 0.643 | 19 | 2.76 (1.41) | 16 | 3.37 (1.14) | 16 | 2.56 (1.89) | 0.292 | |
| PA (day/week) | 52 | 4.00 (2.15) | 18 | 3.94 (2.31) | 34 | 4.03 (2.09) | 0.894 | 19 | 4.47 (1.83) | 17 | 4.35 (1.93) | 16 | 3.06 (2.51) | 0.109 | |
| Falls (number) | 52 | 0.73 (1.15) | 17 | 0.47 (1.00) | 35 | 0.86 (1.21) | 0.262 | 19 | 0.58 (1.01) | 17 | 0.65 (0.86) | 16 | 1.00 (1.54) | 0.536 | |
| Lawton index (point *) | 48 | 6.00 (2.53) | 17 | 5.436 (2.45) | 31 | 6.26 (2.58) | 0.346 | 18 | 7.00 (1.87) | 15 | 7.13 (1.72) | 15 | 3.67 (2.41) | <0.001 | a < c ***; b < c *** |
| Variable | n | Total Mean (SD) | n | Men Mean (SD) | n | Women Mean (SD) | p-Valor | n | 60–69 Years Mean (SD) a | n | 70–79 Years Mean (SD) b | n | >79 Years Mean (SD) c | n | p-Valor | Post Hoc Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SL (cm) | 52 | 61.82 (11.13) | 19 | 63.33 (13.68) | 33 | 60.95 (9.49) | 0.350 | 21 | 67.61 (8.88) | 17 | 64.30 (8.67) | 14 | 50.15 (7.95) | 52 | <0.001 | a > c ***; b > c *** |
| CV sl (%) | 50 | 10.44 (11.07) | 19 | 10.64 (8.71) | 33 | 10.32 (12.36) | 0.247 | 21 | 5.34 (5.52) | 17 | 5.94 (4.07) | 14 | 23.55 (12.67) | 52 | <0.001 | a > c ***; b > c *** |
| GS (m·s−1) | 61 | 1.12 (0.52) | 20 | 1.10 (0.59) | 41 | 1.12 (0.49) | 0.222 | 21 | 1.23 (0.53) | 24 | 1.30 (0.52) | 16 | 0.70 (0.22) | 61 | <0.001 | a > c *; b > c ** |
| CGT (s) | 65 | 21.64 (8.48) | 22 | 21.41 (8.66) | 43 | 21.76 (8.50) | 0.332 | 24 | 18.00 (5.87) | 25 | 18.84 (5.27) | 16 | 31.47 (8.52) | 65 | <0.001 | a < c ***; b < c *** |
| MoCA (0–30 point) | 65 | (19.43 (7.23) | 22 | 19.50 (7.24) | 43 | 19.40 (7.30) | 0.709 | 24 | 22.58 (5.96) | 25 | 20.66 (6.55) | 16 | 12.81 (5.87) | 65 | <0.001 | a > c ***; b > c *** |
| MoCa | |||
|---|---|---|---|
| Beta | p-Valor | R2 | |
| Sex | −0.006 | 0.961 | <0.001 |
| Age (years) | −0.477 | <0.001 | 0.228 |
| BMI (Kg/m2) | −0.312 | 0.005 | 0.332 |
| Lawton index (0–8) | 0.697 | <0.001 | 0.621 |
| Number of falls | −0.212 | 0.084 | 0.301 |
| SL (cm) | 0.446 | 0.002 | 0.386 |
| CV sl (%) | −0.669 | <0.001 | 0.516 |
| GS (m·s−1) | 0.069 | 0.592 | 0.217 |
| CGT (s) | −0.458 | 0.001 | 0.357 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Párraga-Montilla, J.A.; Pozuelo-Carrascosa, D.P.; Carmona-Torres, J.M.; Laredo-Aguilera, J.A.; Cobo-Cuenca, A.I.; Latorre-Román, P.Á. Gait Performance as an Indicator of Cognitive Deficit in Older People. Int. J. Environ. Res. Public Health 2021, 18, 3428. https://doi.org/10.3390/ijerph18073428
Párraga-Montilla JA, Pozuelo-Carrascosa DP, Carmona-Torres JM, Laredo-Aguilera JA, Cobo-Cuenca AI, Latorre-Román PÁ. Gait Performance as an Indicator of Cognitive Deficit in Older People. International Journal of Environmental Research and Public Health. 2021; 18(7):3428. https://doi.org/10.3390/ijerph18073428
Chicago/Turabian StylePárraga-Montilla, Juan Antonio, Diana Patricia Pozuelo-Carrascosa, Juan Manuel Carmona-Torres, José Alberto Laredo-Aguilera, Ana Isabel Cobo-Cuenca, and Pedro Ángel Latorre-Román. 2021. "Gait Performance as an Indicator of Cognitive Deficit in Older People" International Journal of Environmental Research and Public Health 18, no. 7: 3428. https://doi.org/10.3390/ijerph18073428
APA StylePárraga-Montilla, J. A., Pozuelo-Carrascosa, D. P., Carmona-Torres, J. M., Laredo-Aguilera, J. A., Cobo-Cuenca, A. I., & Latorre-Román, P. Á. (2021). Gait Performance as an Indicator of Cognitive Deficit in Older People. International Journal of Environmental Research and Public Health, 18(7), 3428. https://doi.org/10.3390/ijerph18073428