
Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations

 ,
,  , ,
, ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
1. Introduction
2. Health EDRM Workforce
3. Research Needs for Health EDRM Workforce Development
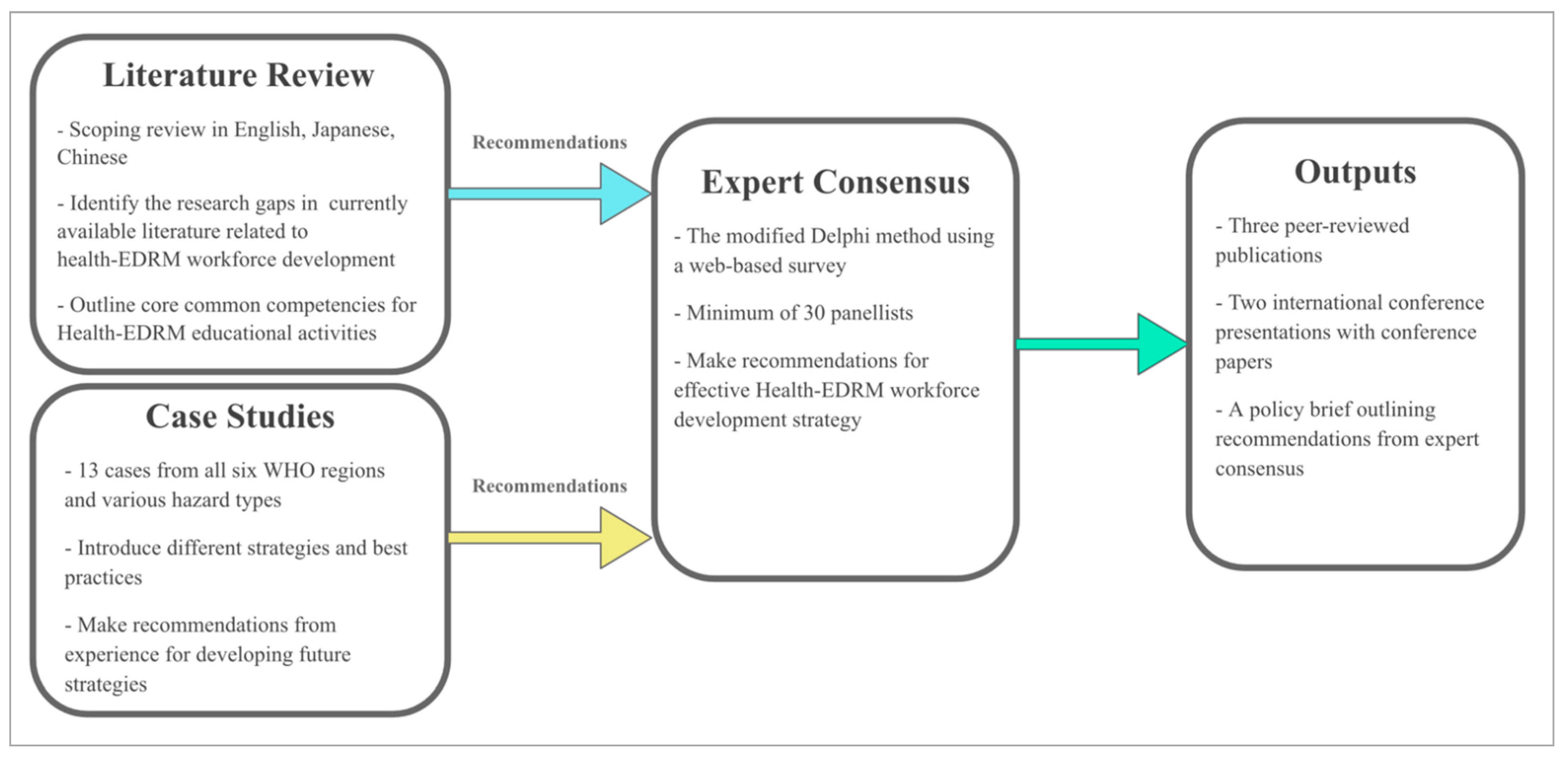
4. Approach to Addressing the Evidence Gap
4.1. Participating Institutions
4.2. Literature Reviews
4.3. Case Studies
4.4. Expert Consensus Study
4.5. Strengths and Limitations of the Current Methodology
5. Importance of Evidence-Based Recommendations for Health EDRM Workforce Development
5.1. Local/Community Level
5.2. National Level
5.3. Regional/Global Level
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- CRED; UNDRR. Human Cost of Disasters: An Overview of the LAST 20 Years 2000–2019. Available online: https://reliefweb.int/report/world/human-cost-disasters-overview-last-20-years-2000-2019 (accessed on 1 February 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 February 2021).
- UNDRR. Understanding Risk. 2019. Available online: https://www.undrr.org/building-risk-knowledge/understanding-risk (accessed on 1 February 2021).
- UNDRR. Sendai Framework for Disaster Risk Reduction. Available online: https://www.unisdr.org/we/inform/publications/43291 (accessed on 1 February 2021).
- United Nations. Yokohama Strategy and Plan of Action for a Safer World. 1994. Available online: https://www.unisdr.org/files/8241_doc6841contenido1.pdf (accessed on 1 February 2021).
- United Nations. Hyogo Framework for Action 2005–2015: Building the Resilience of Nations and Communities to Disasters. 2005. Available online: http://www.unisdr.org/2005/wcdr/intergover/official-doc/L-docs/Hyogo-framework-for-action-english.pdf (accessed on 1 February 2021).
- World Health Organization. WHO Technical Guidance Notes on Sendai Framework Reporting for Ministries of Health; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Wright, N.; Fagan, L.; Lapitan, J.M.; Kayano, R.; Abrahams, J.; Huda, Q.; Murray, V. Health Emergency and Disaster Risk Management: Five Years into Implementation of the Sendai Framework. Int. J. Disaster Risk Sci. 2020, 11, 206–217. [Google Scholar] [CrossRef]
- World Health Organization. WHO Thematic Platform for Health Emergency and Disaster Risk Management. 2009. Available online: https://www.who.int/hac/techguidance/preparedness/WHO-Thematic-Platform-Health-EDRM-Terms-Reference-2018.pdf?ua=1 (accessed on 11 March 2021).
- World Health Organization. Health Emergency and Disaster Risk Management Framework. 2019. Available online: https://www.who.int/hac/techguidance/preparedness/health-emergency-and-disaster-risk-management-framework-eng.pdf?ua=1 (accessed on 1 February 2021).
- Kayano, R.; Chan, E.Y.; Murray, V.; Abrahams, J.; Barber, S.L. WHO Thematic Platform for Health Emergency and Disaster Risk Management Research Network (TPRN): Report of the Kobe Expert Meeting. Int. J. Environ. Res. Public Health 2019, 16, 1232. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Thematic Platform for Health Emergency and Disaster Risk Management Research Network: Terms of Reference. 2018. Available online: https://www.who.int/hac/techguidance/preparedness/WHO-Thematic-Platform-Health-EDRM-Research-Network-2018.pdf?ua=1 (accessed on 11 March 2021).
- Lo, S.T.; Chan, E.Y.Y.; Chan, G.K.; Murray, V.; Abrahams, J.; Ardalan, A.; Kayano, R.; Yau, J.C. Health emergency and disaster risk management (health-EDRM): Developing the research field within the Sendai framework paradigm. Int. J. Disaster Risk Sci. 2017, 8, 145–149. [Google Scholar] [CrossRef]
- World Health Organization. Thirteenth General Programme of Work 2019–2023. 2018. Available online: https://www.who.int/about/what-we-do/thirteenth-general-programme-of-work-2019---2023 (accessed on 1 February 2021).
- United Nations General Assembly (UNGA). Transforming Our World: The 2030 Agenda for Sustainable Development Goals. 2015. Available online: https://sdgs.un.org/goals (accessed on 1 February 2021).
- United Nations Framework Convention on Climate (UNFCC). The Paris Agreement. 2015. Available online: https://unfccc.int/sites/default/files/english_paris_agreement.pdf (accessed on 1 February 2021).
- World Health Organization. International Health Regulations, 3rd ed.; World Health Organization: Geneva, Switzerland, 2005; Available online: https://www.who.int/publications/i/item/9789241580496 (accessed on 1 February 2021).
- World Health Organization. The World Health Report 2006–Working Together for Health; World Health Organization: Geneva, Switzerland, 2006; Available online: http://www.who.int/whr/2006/en/index.html (accessed on 1 February 2021).
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies. Available online: https://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf (accessed on 1 February 2021).
- Aung, M.N.; Murray, V.; Kayano, R. Research Methods and Ethics in Health Emergency and Disaster Risk Management: The Result of the Kobe Expert Meeting. Int. J. Environ. Res. Public Health 2019, 16, 770. [Google Scholar] [CrossRef]
- Daily, E.; Padjen, P.; Birnbaum, M. A review of competencies developed for disaster healthcare providers: Limitations of current processes and applicability. Prehosp. Disaster Med. 2010, 25, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, A.R.; Djalali, A.; Foletti, M.; Ragazzoni, L.; Della Corte, F.; Lupescu, O.; Arculeo, C.; Arnim, G.; Friedl, T.; Ashkenazi, M.; et al. Core Competencies in Disaster Management and Humanitarian Assistance: A Systematic Review. Disaster Med. Public Health Prep. 2015, 5, 1–10. [Google Scholar] [CrossRef]
- Hsu, E.B.; Thomas, T.L.; Bass, E.B.; Whyne, D.; Kelen, G.D.; Green, G.B. Healthcare worker competencies for disaster training. BMC Med. Educ. 2006, 6, 19. [Google Scholar] [CrossRef]
- World Health Organization. Classification and Minimum Standards for Foreign Medical Teams in Sudden Onset Disasters. Available online: https://www.who.int/csr/resources/publications/ebola/foreign-medical-teams/en/ (accessed on 1 February 2021).
- Djalali, A.; Ingrassia, P.L.; Della Corte, F.; Foletti, M.; Gallardo, A.R.; Ragazzoni, L.; Kaptan, K.; Lupescu, O.; Arculeo, C.; Arnim, G.; et al. Identifying Deficiencies in National and Foreign Medical Team Responses through Expert Opinion Surveys: Implications for Education and Training. Prehosp. Disaster Med. 2015, 30, 224. [Google Scholar] [CrossRef]
- Burkle, F.M., Jr. The development of multidisciplinary core competencies: The first step in the professionalization of disaster medicine and public health preparedness on a global scale. Disaster Med. Public Health Prep. 2012, 6, 10–12. [Google Scholar] [CrossRef]
- WHO Ebola Response Team. Ebola virus disease in West Africa—the first 9 months of the epidemic and forward projections. N. Engl. J. Med. 2014, 371, 1481–1495. [Google Scholar]
- Ragazzoni, L.; Ingrassia, P.L.; Echeverri, L.; Maccapani, F.; Berryman, L.; Burkle, F.M., Jr.; Corte, F.D. Virtual Reality Simulation Training for Ebola Deployment. Disaster Med. Public Health Prep. 2015, 9, 543–546. [Google Scholar] [CrossRef]
- Pourhosseini, S.S.; Ardalan, A.; Mehrolhassani, M.H. Key Aspects of Providing Healthcare Services in Disaster Response Stage. Iran J. Public Health 2015, 44, 111–118. [Google Scholar] [PubMed]
- Global Health Workforce Alliance, WHO, IFRC, UNICEF, UNHCR. Scaling-Up the Community-Based Health Workforce for Emergencies. 2011. Available online: https://www.who.int/workforcealliance/knowledge/resources/chwstatement/en/ (accessed on 1 February 2021).
- Cometto, G.; Buchan, J.; Dussault, G. Developing the health workforce for universal health coverage. Bull. World Health Organ. 2020, 98, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Belfroid, E.; Roβkamp, D.; Fraser, G.; Corien, S.; Aura, T. Towards defining core principles of public health emergency preparedness: Scoping review and Delphi consultation among European Union country experts. BMC Public Health 2020, 20, 1482. [Google Scholar] [CrossRef] [PubMed]
- Pyda, J.; Patterson, R.H.; Caddell, L.; Wurdeman, T.; Koch, R.; Polatty, D.; Card, B.; Meara, J.; Corlew, D.S. Towards resilient health systems: Opportunities to align surgical and disaster planning. BMJ Glob. Health 2019, 4, e001493. [Google Scholar] [CrossRef]
- Teklehaimanot, H.D.; Teklehaimanot, A. Human resource development for a community-based health extension program: A case study from Ethiopia. Hum. Resour. Health 2013, 11, 39. [Google Scholar] [CrossRef]
- Varpilah, S.T.; Safer, M.; Frenkel, E.; Baba, D.; Massaquoi, M.; Barrow, G. Rebuilding human resources for health: A case study from Liberia. Hum. Resour. Health 2011, 9, 11. [Google Scholar] [CrossRef]
- Fujita, N.; Zwi, A.B.; Nagai, M.; Akashi, H. A comprehensive framework for human resources for health system development in fragile and post-conflict states. PLoS Med. 2011, 8, e1001146. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H. Guidance for Conducting Systematic Scoping Reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. Available online: https://www.acpjournals.org/doi/10.7326/M18-0850 (accessed on 24 March 2021). [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods, 5th ed.; Sage: Los Angeles, CA, USA, 2014. [Google Scholar]
- Santella, A.J. Master of Public Health Competencies: A Case Study Approach; Jones & Bartlett Learning: Burlington, MA, USA, 2020. [Google Scholar]
- Crowe, S.; Cresswell, K.; Robertson, A.; Huby, G.; Avery, A.; Sheikh, A. The case study approach. BMC Med. Res. Methodol. 2011, 11, 100. [Google Scholar] [CrossRef]
- Keeney, S.; Hasson, F.; McKenna, H. The Delphi Technique. In The Delphi Technique in Nursing and Health Research; Wiley-Blackwell: Chichester, UK, 2011; Chapter 1; pp. 1–17. [Google Scholar]
- James, D.; Warren-Forward, H. Research methods for formal consensus development. Nurse Res. 2015, 14, 22. [Google Scholar] [CrossRef]
- Jorm, A.F. Using the Delphi expert consensus method in mental health research. Aust. N. Z. J. Psychiatry 2015, 49, 887–897. [Google Scholar] [CrossRef]
- Trevelyan, E.G.; Robinson, N. Delphi methodology in health research: How to do it? Eur. J. Integr. Med. 2015, 7, 423–428. [Google Scholar] [CrossRef]
- Khan, Y.; Brown, A.D.; Gagliardi, A.R.; O’Sullivan, T.; Lacarte, S.; Henry, B.; Schwartz, C. Are we prepared? The development of performance indicators for public health emergency preparedness using a modified Delphi approach. PLoS ONE 2019, 14, e0226489. [Google Scholar] [CrossRef]
- 8IFRC. One Billion Coalition for Resilience. Available online: https://media.ifrc.org/1bc/alt-about-the-coalition/ (accessed on 1 February 2021).
- IFRC. World Disasters Report 2015: Focus on Local Actors, the Key to Humanitarian Effectiveness. 2015. Available online: https://media.ifrc.org/ifrc/document/world-disasters-report-2015-focus-local-actors-key-humanitarian-effectiveness/ (accessed on 1 February 2021).
- Shaw, R. Community-Based Disaster Risk Reduction. Oxford Research Encyclopedia of Natural Hazard Science. 2016. Available online: https://oxfordre.com/naturalhazardscience/view/10.1093/acrefore/9780199389407.001.0001/acrefore-9780199389407-e-47 (accessed on 1 February 2021).
- National Research Council. Chapter: 5 Building Local Capacity and Accelerating Progress: Resilience from the Bottom Up. In Disaster Resilience: A National Imperative; The National Academies Press: Washington, DC, USA, 2012; pp. 117–158. [Google Scholar]
- Van Niekerk, D.; Nemakonde, L.D.; Kruger, L.; Forbes-Genade, K. Community-Based Disaster Risk Management. In Handbook of Disaster Research; Rodríguez, H., Donner, W., Trainor, J., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- McNeish, R.; Rigg, K.K.; Tran, Q.; Hodges, S. Community-Based Behavioral Health Interventions: Developing Strong Community Partnerships. Eval. Program Plan. 2019, 73, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Chibanda, D.; Weiss, H.A.; Verhey, R.; Simms, V.; Munjoma, R.; Rusakaniko, S. Effect of a Primary Care–Based Psychological Intervention on Symptoms of Common Mental Disorders in Zimbabwe: A Randomized Clinical Trial. JAMA 2016, 316, 2618–2626. [Google Scholar] [CrossRef] [PubMed]
- Rigg, K.K.; Engelman, D.; Ramirez, J. A Community-Based Approach to Primary Health Care. In Dimensions of Community-Based Projects in Health Care; Arxer, S., Murphy, J., Eds.; International Perspectives on Social Policy, Administration, and Practice; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Phinse, P.; Srinivasan, K.; Neetu, P. Community-based interventions for health promotion and disease prevention in noncommunicable diseases: A narrative review. J. Educ. Health Promot. 2018, 7. [Google Scholar] [CrossRef]
- Chan, E.Y.Y. Bottom-up disaster resilience. Nat. Geosci. 2013, 6, 201. [Google Scholar] [CrossRef]
- Rosenbaum, S.J.D. Principles to Consider for the Implementation of a Community Health Needs Assessment Process. Department of Health Policy School of Public Health and Health Services, George Washington University. 2013. Available online: https://hsrc.himmelfarb.gwu.edu/sphhs_policy_facpubs/863 (accessed on 1 February 2021).
- Dennis, S.; Hetherington, S.A.; Borodzicz, J.A.; Hermiz, O.; Zwar, N.A. Challenges to establishing successful partnerships in community health promotion programs: Local experiences from the national implementation of healthy eating activity and lifestyle (HEALTM) program. Health Promot. J. Aust. 2015, 26, 45–51. [Google Scholar] [CrossRef]
- Nicholls, K.; Picou, S.; McCord, S. Training Community Health Workers to Enhance Disaster Resilience. J. Public Health Manag. Pract. 2017, 23, S78–S84. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guideline on Health Policy and System Support to Optimize Community Health Worker Programmes. 2018. Available online: https://www.who.int/hrh/resources/health-policy-system-support-hw-programmes/en/ (accessed on 25 February 2021).
- World Health Organization. Comprehensive Safe Hospital Framework. 2015. Available online: https://www.who.int/publications/i/item/comprehensive-safe-hospital-framework (accessed on 1 February 2021).
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030. Available online: https://www.who.int/hrh/resources/pub_globstrathrh-2030/en/ (accessed on 1 February 2021).
- World Health Organization: Emergency Medical Team. Available online: https://www.who.int/emergencies/partners/emergency-medical-teams (accessed on 1 February 2021).
- World Organization and International Council of Nurses. ICN Framework of Disaster Nursing Competencies. Geneva; ICN. 2009. Available online: https://www.icn.ch/sites/default/files/inline-files/ICN_Disaster-Comp-Report_WEB_final.pdf 9 (accessed on 1 February 2021).
- Hutton, A.; Veenema, T.G.; Gebbie, K. Review of the International Council of Nurses (ICN) Framework of Disaster Nursing Competencies. Prehosp. Disaster Med. 2016, 31, 680–683. [Google Scholar] [CrossRef] [PubMed]
- World Health Organizations. OpenWHO. 2020. Available online: https://openwho.org/ (accessed on 24 March 2021).
- World Health Organization. Global Outbreak Alert and Response Network. Available online: https://extranet.who.int/goarn/ (accessed on 1 February 2021).
- Chan, E.Y.Y.; Murray, V. What are the health research needs for the Sendai Framework? Lancet 2017, 390, e35–e36. [Google Scholar] [CrossRef]


{kind=link}
| Research Needs | Rationales |
|---|---|
|
|
|
|
|
|
| University | Literature Review | Case Studies | Expert Consensus |
|---|---|---|---|
| The Chinese University of Hong Kong, Hong Kong SAR, China | Overall coordination and delivery of the project Leading the English and Chinese literature review | Overall coordination of case studies and the creation of 3 case studies:
| Overall coordination of the Delphi research |
| Harvard University, USA |
| All participants will contribute their expertise in study design and be invited as a panellist as appropriate | |
| Sichuan University, China |
| ||
| Tohoku University, Japan | Supporting the Japanese literature review |
| |
| University of Hyogo, Japan | Leading the Japanese literature review |
| |
| University of Piemonte Orientale, Italy |
| ||
| University of the Philippines Manila, Philippines |
| ||
| WHO India, India |
| ||
| Outputs | Literature review in 3 languages 1 peer reviewed publication 1 international conference presentation | 13 case studies 1 peer reviewed publication 1 international conference presentation | Expert consensus recommendations Policy brief |
| Inclusion Criteria |
|
| Exclusion Criteria |
|
| Cases | Description | Data Source |
|---|---|---|
| 1: Pharmacy workforce in post-conflict sub-Saharan African countries | Make recommendations to better inform pharmacy workforce development policies in post-conflict areas | Literature review Key informant interviews |
| 2: Community health workers for future disasters in Nepal | Explore the roles of female community health volunteers during and following the 2015 earthquake | Literature review Key informant interviews |
| 3: Community disaster education initiative in rural China | Describe planning and implementation process of a Health EDRM education initiative in China | Literature review Personal experience of programme managers/implementers |
| 4: Health workforce demands in Lebanon | Describe how Lebanon’s health system and workforce coped with a rapid 25% population increase | Literature review Key informant interviews |
| 5: Earthquake response teams in Chile | Describe the training regimens and best practices from the experience of the Earthquake Response in Chile | Literature review Discussion with responders |
| 6. Logistic Support for Emergency Medical Teams in China | Summarise the experience, lessons and development of logistics support | Literature/policy reviews |
| 7. Multidisciplinary conductor type disaster health workforce development program | Review the comprehensive disaster training programme in Japan, focusing on its development and deployment | Literature review Personal Experience |
| 8. Competency framework of Japan DMAT and specialised assistance teams. | Identify good practice and gaps in the education programme | Literature review |
| 9. Disaster Relief Nursing in Japan | Describe disaster relief nurse programme in Japan focusing on training, registration, dispatch and operation | Literature review Personal experience |
| 10. Undergraduate medical training in Disaster Medicine | Present a disaster medicine training programme and discuss its cost-effective and reproducible solutions | Literature review Personal experience |
| 11. Emergency Medical Teams (EMTs) Training | Highlight coordination and quality assurance mechanisms for the training programme | Literature review Personal experience |
| 12: Disaster nursing training and management in the Philippines | Describe a national training of trainers’ programme in disaster nursing management in the Philippines | Literature review Key informant interviews |
| 13. Hospital Emergency Preparedness and Planning in India | Summarise safe hospital initiatives in India | Literature/policy reviews Personal experience |
| Level | Potential Impacts of Recommendations |
|---|---|
| Local/Community |
|
| |
| |
| |
| National |
|
| |
| |
| Regional/Global |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.K.C.; Mashino, S.; Chan, E.Y.Y.; MacDermot, M.K.; Balsari, S.; Ciottone, G.R.; Della Corte, F.; Dell’Aringa, M.F.; Egawa, S.; Evio, B.D.; et al. Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations. Int. J. Environ. Res. Public Health 2021, 18, 3382. https://doi.org/10.3390/ijerph18073382
Hung KKC, Mashino S, Chan EYY, MacDermot MK, Balsari S, Ciottone GR, Della Corte F, Dell’Aringa MF, Egawa S, Evio BD, et al. Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations. International Journal of Environmental Research and Public Health. 2021; 18(7):3382. https://doi.org/10.3390/ijerph18073382
Chicago/Turabian StyleHung, Kevin K. C., Sonoe Mashino, Emily Y. Y. Chan, Makiko K. MacDermot, Satchit Balsari, Gregory R. Ciottone, Francesco Della Corte, Marcelo F. Dell’Aringa, Shinichi Egawa, Bettina D. Evio, and et al. 2021. "Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations" International Journal of Environmental Research and Public Health 18, no. 7: 3382. https://doi.org/10.3390/ijerph18073382
APA StyleHung, K. K. C., Mashino, S., Chan, E. Y. Y., MacDermot, M. K., Balsari, S., Ciottone, G. R., Della Corte, F., Dell’Aringa, M. F., Egawa, S., Evio, B. D., Hart, A., Hu, H., Ishii, T., Ragazzoni, L., Sasaki, H., Walline, J. H., Wong, C. S., Bhattarai, H. K., Dalal, S., ... Graham, C. A. (2021). Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations. International Journal of Environmental Research and Public Health, 18(7), 3382. https://doi.org/10.3390/ijerph18073382