
The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants: Eligibility Criteria and Sample Size Consideration
2.3. Sensorized Insoles
2.4. Interventions
2.5. Measures
- -
- Weight Bearing Absolute Healthy limb (WBAH; Kg)
- -
- Weight Bearing Absolute Surgical limb (WBAS; Kg)
- -
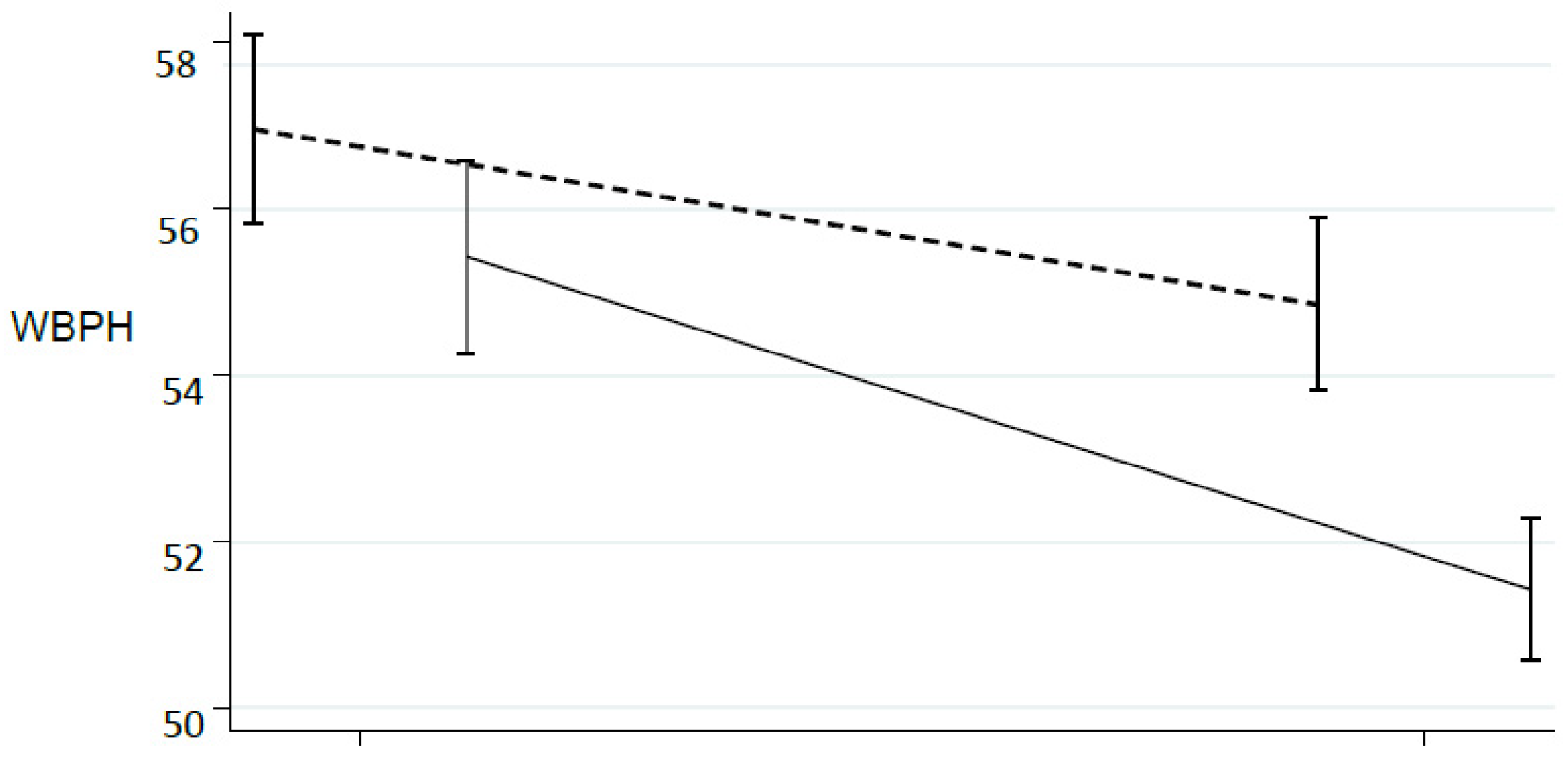
- Weight Bearing Percentage Healthy limb (WBPH; %)
- -
- Weight Bearing Percentage Surgical limb (WBPS; %)
- -
- Step Length Healthy limb (SLH; cm)
- -
- Step Length Surgical limb (SLS; cm)
- -
- Swing Healthy limb (SHL; ms)
- -
- Swing Surgical limb (SSL; ms)
- -
- Double Support Time (DST; ms)
2.6. Blinding
2.7. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, C.; Nevitt, M.C.; Niu, J.; Clancy, M.M.; Lane, N.E.; Link, T.M.; Vlad, S.; Tolstykh, I.; Jungmann, P.M.; Felson, D.T.; et al. Association of hip pain with radiographic evidence of hip osteoarthritis: Diagnostic test study. BMJ 2015, 351, h5983. [Google Scholar] [CrossRef]
- Ewen, A.M.; Stewart, S.; St Clair Gibson, A.; Kashyap, S.N.; Caplan, N. Post-operative gait analysis in total hip replacement patients—A review of current literature and meta-analysis. Gait Posture 2012, 36, 1–6. [Google Scholar] [CrossRef]
- Khan, F.; Ng, L.; Gonzalez, S.; Hale, T.; Turner-Stokes, L. Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. Cochrane Database Syst. Rev. 2008, 2, CD004957. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.; Feger, M.A.; Hart, J.M.; Saliba, S.; Park, J.; Hertel, J. Effects of an auditory biofeedback device on plantar pressure in patients with chronic ankle instability. Gait Posture 2016, 44, 29–36. Available online: https://pubmed.ncbi.nlm.nih.gov/27004629/ (accessed on 19 February 2021). [CrossRef]
- Hershko, E.; Tauber, C.; Carmeli, E. Biofeedback versus physiotherapy in patients with partial weight-bearing. Am. J. Orthop. 2008, 37, E92–E96. Available online: https://europepmc.org/article/med/18587509 (accessed on 19 February 2021). [PubMed]
- Hustedt, J.W.; Blizzard, D.J.; Baumgaertner, M.R.; Leslie, M.P.; Grauer, J.N. Current advances in training orthopaedic patients to comply with partial weight-bearing instructions. Yale J. Biol. Med. 2012, 85, 119–125. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22461750 (accessed on 28 May 2019).
- Rahman, J.; Tang, Q.; Monda, M.; Miles, J.; McCarthy, I. Gait assessment as a functional outcome measure in total knee arthroplasty: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 66. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25886558 (accessed on 8 May 2019). [CrossRef] [PubMed]
- Baumfeld, D.; Baumfeld, T.; da Rocha, R.L.; Macedo, B.; Raduan, F.; Zambelli, R.; Alves Silva, T.A.; Nery, C. Reliability of Baropodometry on the Evaluation of Plantar Load Distribution: A Transversal Study. Biomed. Res. Int. 2017, 2017, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Correale, L.; Carnevale Pellino, V.; Marin, L.; Febbi, M.; Vandoni, M. Comparison of an Inertial Measurement Unit System and Baropodometric Platform for Measuring Spatiotemporal Parameters and Walking Speed in Healthy Adults. Motor Control 2020, 25, 89–99. Available online: https://pubmed.ncbi.nlm.nih.gov/33207319/ (accessed on 18 February 2021). [CrossRef] [PubMed]
- Marin, L.; Lovecchio, N.; Kawczynski, A.; Febbi, M.; Silvestri, D.; Pellino, V.C.; Gibellini, R.; Vandoni, M. Intensive Rehabilitation Program in Arterial Occlusive Disease Patients. Appl. Sci. 2021, 11, 1184. Available online: https://www.mdpi.com/2076-3417/11/3/1184 (accessed on 19 February 2021). [CrossRef]
- Hara, D.; Nakashima, Y.; Hamai, S.; Higaki, H.; Ikebe, S.; Shimoto, T.; Yoshimoto, K.; Iwamoto, Y. Dynamic hip kinematics in patients with hip osteoarthritis during weight-bearing activities. Clin. Biomech. 2016, 32, 150–156. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0268003315003216 (accessed on 28 May 2019). [CrossRef]
- Moufawad El Achkar, C.; Lenoble-Hoskovec, C.; Paraschiv-Ionescu, A.; Major, K.; Büla, C.; Aminian, K. Physical Behavior in Older Persons during Daily Life: Insights from Instrumented Shoes. Sensors 2016, 16, 1225. Available online: https://www.mdpi.com/1424-8220/16/8/1225 (accessed on 8 May 2019). [CrossRef]
- Khurelbaatar, T.; Kim, K.; Lee, S.; Kim, Y.H. Consistent accuracy in whole-body joint kinetics during gait using wearable inertial motion sensors and in-shoe pressure sensors. Gait Posture 2015, 42, 65–69. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0966636215004488 (accessed on 19 May 2019). [CrossRef]
- Shanahan, C.J.; Boonstra, F.M.C.; Cofré Lizama, L.E.; Strik, M.; Moffat, B.A.; Khan, F.; Kilpatrick, T.J.; van der Walt, A.; Galea, M.P.; Kolbe, S.C. Technologies for Advanced Gait and Balance Assessments in People with Multiple Sclerosis. Front Neurol. 2017, 8, 708. Available online: http://journal.frontiersin.org/article/10.3389/fneur.2017.00708/full (accessed on 8 May 2019). [CrossRef] [PubMed]
- Barbour, V.; Bhui, K.; Chescheir, N.; Clavien, P.A.; Diener, M.K.; Glasziou, P.; Golub, R.M.; Grimshaw, J.M.; Groves, T.; Hopewell, S.; et al. CONSORT Statement for randomized Trials of nonpharmacologic treatments: A 2017 update and a CONSORT extension for nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. Available online: https://pubmed.ncbi.nlm.nih.gov/28630973/ (accessed on 19 February 2021).
- Association, W.M. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. Available online: www.jama.com (accessed on 19 February 2021).
- RANDOM.ORG-True Random Number Service. Available online: https://www.random.org/ (accessed on 2 March 2021).
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; MacIntyre, N.R.; McKay, R.T.; Johnson, D.; Wanger, J.S.; Zeballos, R.J.; Bittner, V.; et al. ATS statement: Guidelines for the six-minute walk test Vol. 166, American Journal of Respiratory and Critical Care Medicine. Am. Lung Assoc. 2002, 166, 111–117. Available online: http://www.atsjournals.org/doi/abs/10.1164/ajrccm.166.1.at1102 (accessed on 2 March 2021).
- Paoli, A.; Sekulic, D.; Messina, G.; Palma, A.; Gagey, P.M.; Şahin, N.; Patti, A.; Bianco, A.; Iovane, A. Postural control and balance in a cohort of healthy people living in Europe. Medicine 2018, 97, e13835. [Google Scholar]
- Vanhelst, J.; Fardy, P.S.; Salleron, J.; Béghin, L. Disability and Rehabilitation The six-minute walk test in obese youth: Reproducibility, validity, and prediction equation to assess aerobic power. Disabil. Rehabil. 2013, 35, 479–482. Available online: https://www.tandfonline.com/action/journalInformation?journalCode=idre20 (accessed on 3 December 2019). [CrossRef] [PubMed]
- Unver, B.; Kahraman, T.; Kalkan, S.; Yuksel, E.; Karatosun, V. Reliability of the six-minute walk test after total hip arthroplasty. Hip. Int. 2013, 23, 541–545. Available online: http://journals.sagepub.com/doi/10.5301/hipint.5000073 (accessed on 19 May 2019). [CrossRef]
- Pataky, Z.; De León Rodriguez, D.; Golay, A.; Assal, M.; Assal, J.-P.; Hauert, C.-A. Biofeedback Training for Partial Weight Bearing in Patients After Total Hip Arthroplasty. Arch. Phys. Med. Rehabil. 2009, 90, 1435–1438. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19651281 (accessed on 8 May 2019). [CrossRef]
- Baj, A.; Lovecchio, N.; Bolzoni, A.; Mapelli, A.; Giannì, A.B.; Sforza, C. Stair ascent and descent in assessing donor-site morbidity following osteocutaneous free fibula transfer: A preliminary study. J. Oral. Maxillofac. Surg. 2015, 73, 184–193. Available online: https://pubmed.ncbi.nlm.nih.gov/25511965/ (accessed on 18 February 2021). [CrossRef]
- Lovecchio, N.; Sciumè, L.; Zago, M.; Panella, L.; Lopresti, M.; Sforza, C. Lower limbs kinematic assessment of the effect of a gym and hydrotherapy rehabilitation protocol after knee megaprosthesis: A case report. J. Phys. Ther. Sci. 2016, 28, 1064–1070. Available online: https://pubmed.ncbi.nlm.nih.gov/27134413/ (accessed on 18 February 2021). [CrossRef] [PubMed][Green Version]
- Lovecchio, N.; Zago, M.; Sciumè, L.; Lopresti, M.; Sforza, C. Squat exercise to estimate knee megaprosthesis rehabilitation: A pilot study. J. Phys. Ther. Sci. 2015, 27, 2409–2412. Available online: /pmc/articles/PMC4540892/ (accessed on 18 February 2021). [CrossRef] [PubMed][Green Version]
- Allet, L.; Knols, R.H.; Shirato, K.; de Bruin, E.D. Wearable systems for monitoring mobility-related activities in chronic disease: A systematic review. Sensors 2010, 10, 9026–9052. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.; Karunamuni, N.; Lytvyak, E.; Penfold, C.; Schopflocher, D.; Imayama, I.; Johnson, S.T.; Raine, K. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health 2015, 15, 1195. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26619838 (accessed on 8 May 2019). [CrossRef] [PubMed]
- Schack, T.; Ritter, H. The cognitive nature of action-functional links between cognitive psychology, movement science, and robotics. Prog. Brain Res. 2009, 174, 231–250. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0079612309013193 (accessed on 8 May 2019).
- Schega, L.; Bertram, D.; Fölsch, C.; Hamacher, D.; Hamacher, D. The influence of visual feedback on the mental representation of gait in patients with THR: A new approach for an experimental rehabilitation strategy. Appl. Psychophysiol. Biofeedback 2014, 39, 37–43. Available online: http://link.springer.com/10.1007/s10484-014-9239-8 (accessed on 8 May 2019). [CrossRef]
- Agostini, V.; Ganio, D.; Facchin, K.; Cane, L.; Moreira Carneiro, S.; Knaflitz, M. Gait parameters and muscle activation patterns at 3, 6 and 12 months after total hip arthroplasty. J. Arthroplast. 2014, 29, 1265–1272. [Google Scholar] [CrossRef]
- Schack, T.; Mechsner, F. Representation of motor skills in human long-term memory. Neurosci. Lett. 2006, 391, 77–81. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0304394005011596 (accessed on 8 May 2019). [CrossRef]
- Tveit, M.; Kärrholm, J. Low effectiveness of prescribed partial weight bearing. Continuous recording of vertical loads using a new pressure-sensitive insole. J. Rehabil. Med. 2001, 33, 42–46. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11480470 (accessed on 19 May 2019). [PubMed]
- Buccino, G. Action observation treatment: A novel tool in neurorehabilitation. Philos. Trans. R Soc. B Biol. Sci. 2014, 369, 20130185. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24778380 (accessed on 28 May 2019). [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Days after Surgery | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Enrollment | x | ||||||||
| Randomization | x | ||||||||
| Evaluation | x | x | |||||||
| Intervention | x | x | x | x | x | x | x | ||
| Outcomes | All | EG (n = 19) | CG (n = 21) | p Value |
|---|---|---|---|---|
| Age (years) | 62.58 (9.06) | 64.12 (7.48) | 61.30 (9.74) | 0.058 |
| Height (cm) | 169.35 (9.99) | 166.42 (9.77) | 172.00 (9.65) | 0.077 |
| Weight (kg) | 79.85 (12.94) | 72.74 (9.49) | 86.29 (12.41) | <0.001 |
| BMI | 27.87 (4.09) | 26.34 (3.6) | 29.25 (4.1) | 0.023 |
| Outcomes | EG | CG | p between Groups | ||
|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | ||
| WBAH (Kg) | 40.2 (6.5) | 37.4 (5.5) * | 49.1 (8.5) | 47.4 (8.3) * | 0.151 |
| WBAS (Kg) | 32.5 (5.7) | 35.4 (5.4) * | 37.1 (6.8) | 39.8 (8.0) * | 0.985 |
| ΔWBA (Kg) | 7.7 (7.6) | 2.0 (5.3) * | 12.1 (9.2) | 7.62 (11.2) * | 0.024 |
| 6MWT (m) | 194.3 (82.6) | 308.4 (119.3) * | 187.5 (84.2) | 310.2 (105.1) * | 0.897 |
| NRS (score) | 3.7 (2.1) | 0.7 (0.3) * | 3.19 (2.29) | 1.1 (0.5) * | 0.877 |
| Pre | Post | |||||
|---|---|---|---|---|---|---|
| Group | Weight (kg) | Sum of WB on the Two Side (kg) | Δ of Weight and Sum of WB | Weight (kg) | Sum of WB on the Two Side (kg) | Δ of Weight and Sum of WB |
| EC | 72.74 | 73 | −0.26 | 70.74 | 72.8 | −2.06 |
| CG | 86.29 | 86.2 | 0.09 | 84.29 | 87.2 | −2.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, L.; Vandoni, M.; Zaza, G.; Febbi, M.; Pedrotti, L.; Chiodaroli, M.; Lovecchio, N.; Manzoni, F. The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement. Int. J. Environ. Res. Public Health 2021, 18, 3346. https://doi.org/10.3390/ijerph18073346
Marin L, Vandoni M, Zaza G, Febbi M, Pedrotti L, Chiodaroli M, Lovecchio N, Manzoni F. The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement. International Journal of Environmental Research and Public Health. 2021; 18(7):3346. https://doi.org/10.3390/ijerph18073346
Chicago/Turabian StyleMarin, Luca, Matteo Vandoni, Giancarlo Zaza, Massimiliano Febbi, Luisella Pedrotti, Matteo Chiodaroli, Nicola Lovecchio, and Federica Manzoni. 2021. "The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement" International Journal of Environmental Research and Public Health 18, no. 7: 3346. https://doi.org/10.3390/ijerph18073346
APA StyleMarin, L., Vandoni, M., Zaza, G., Febbi, M., Pedrotti, L., Chiodaroli, M., Lovecchio, N., & Manzoni, F. (2021). The Effects of Insole-Based Visual Feedback on Weight-Bearing in Patients Undergoing Total Hip Replacement. International Journal of Environmental Research and Public Health, 18(7), 3346. https://doi.org/10.3390/ijerph18073346