
Evaluating the Impact of the Healthy Kids Community Challenge (HKCC) on Physical Activity of Older Youth



Abstract
1. Introduction
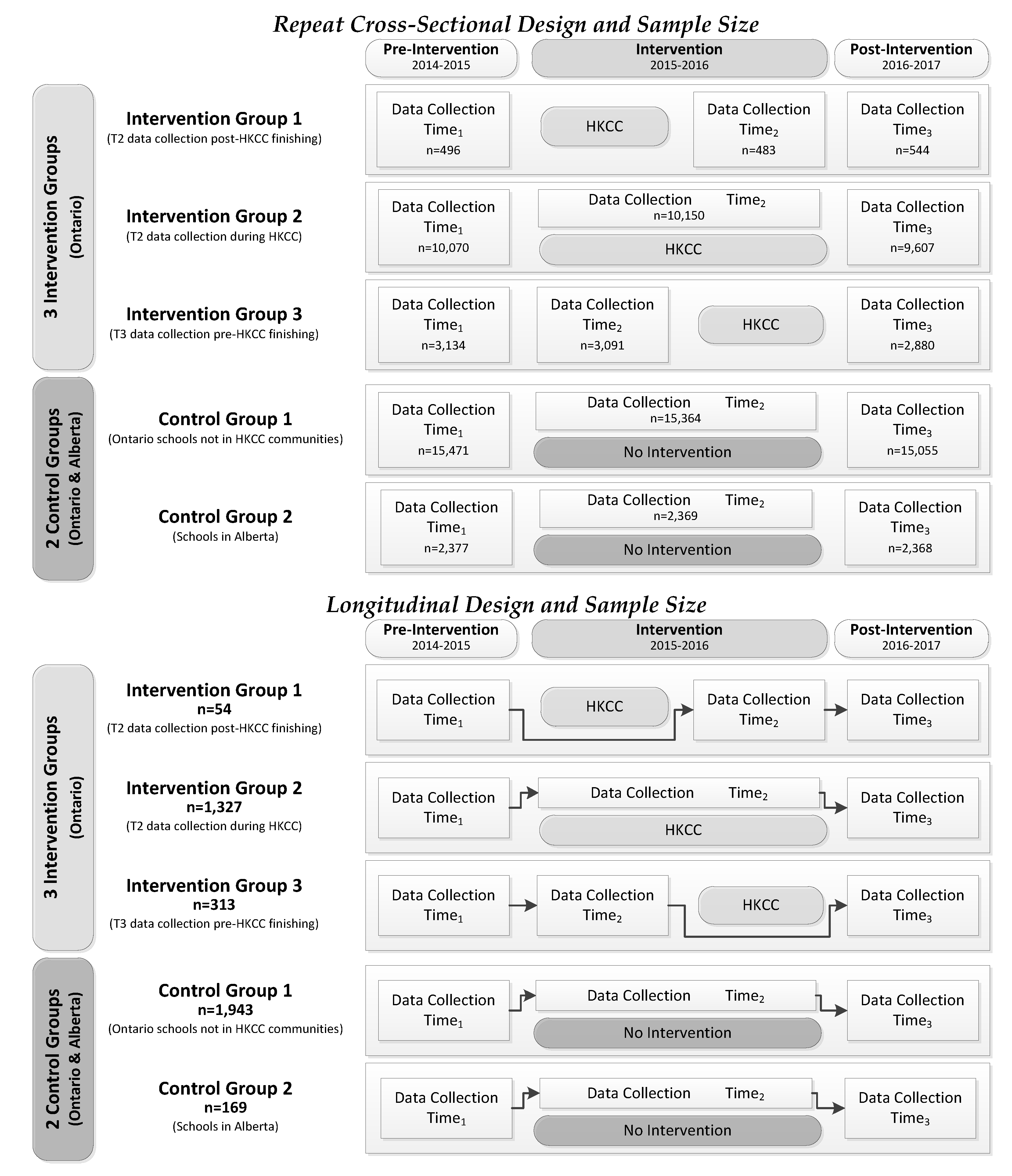
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Analyses
3. Results
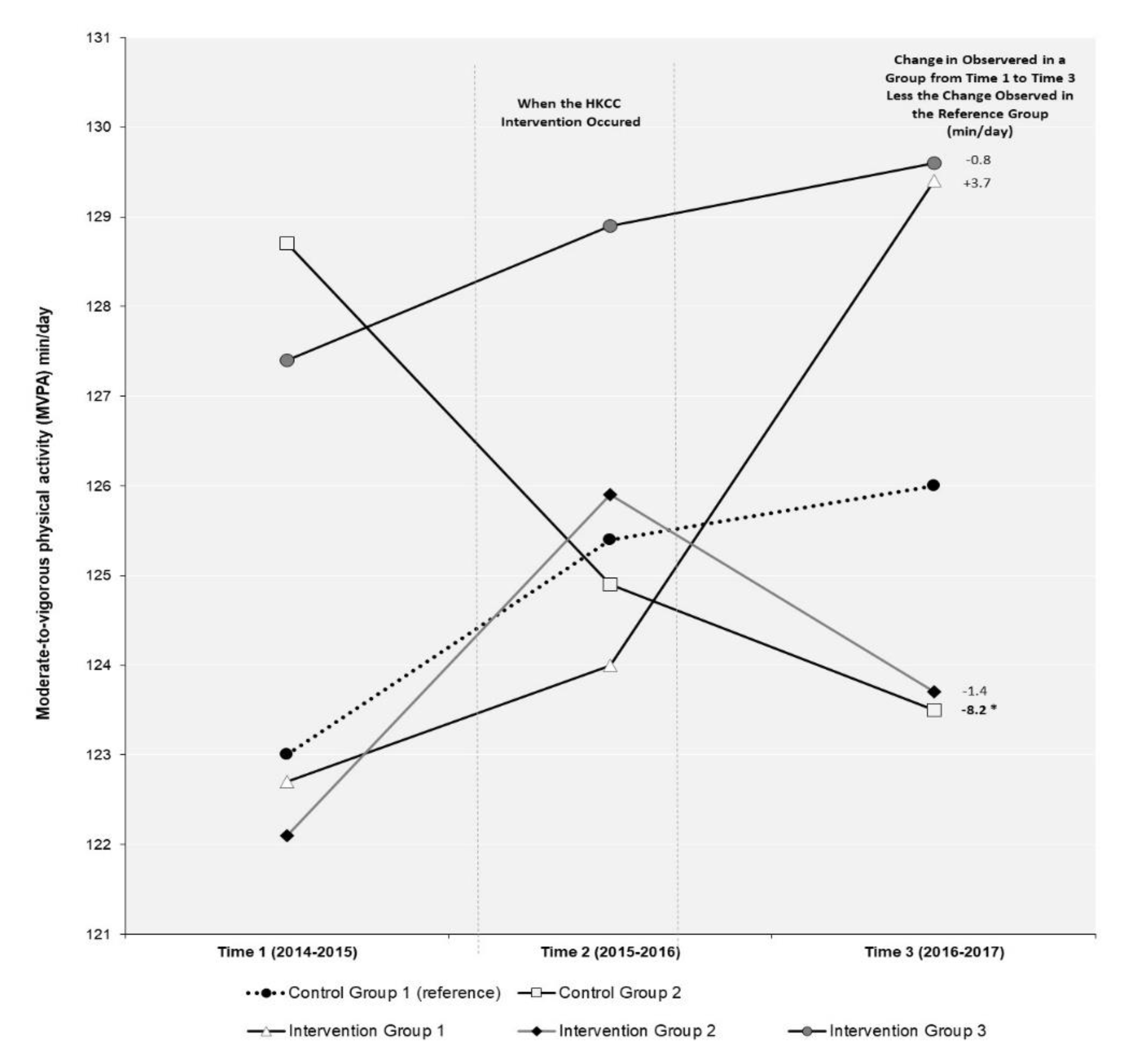
3.1. Moderate-to-Vigorous Physical Activity (MVPA)
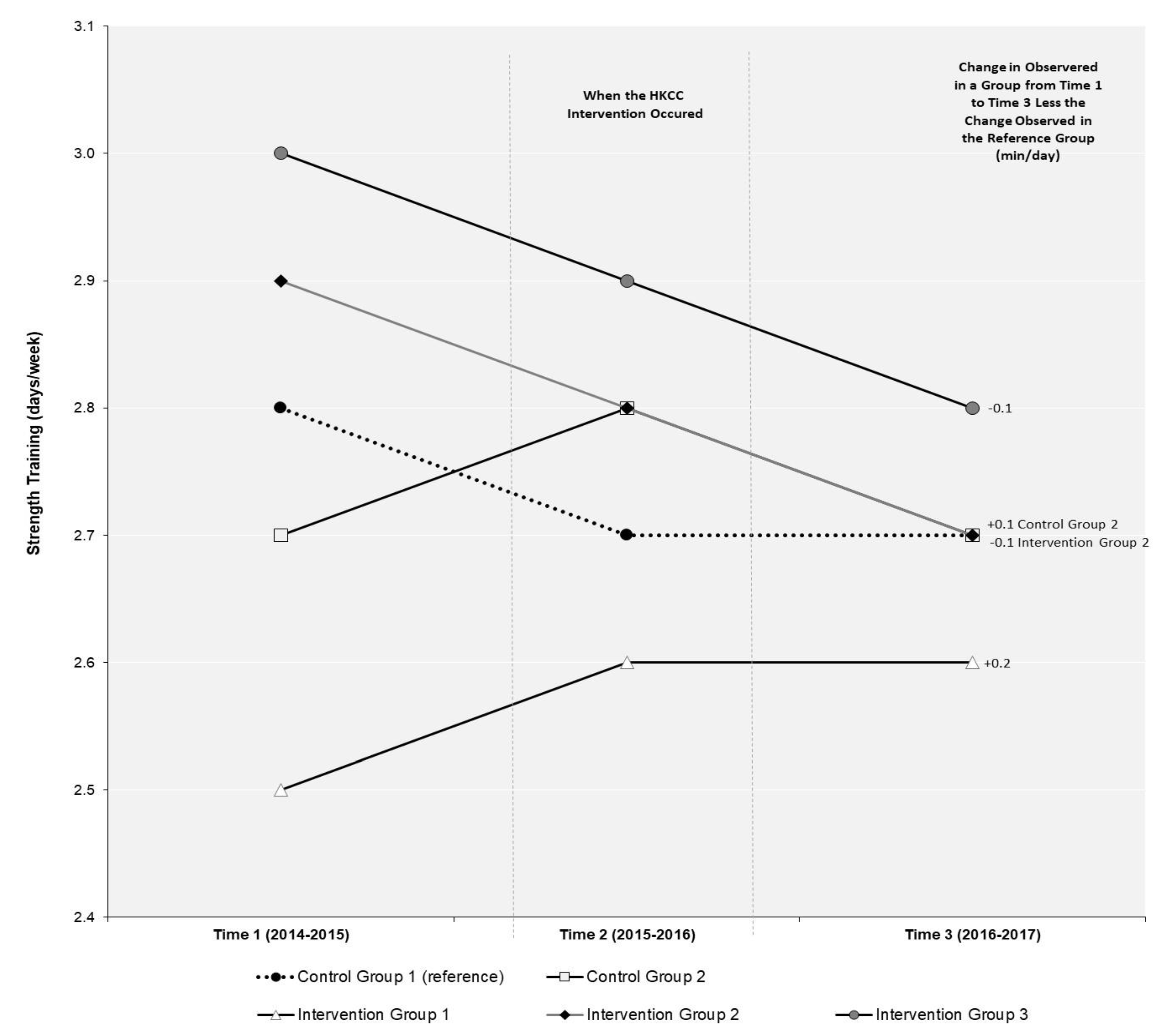
3.2. Strength Training (ST)
3.3. Meeting the 24-Hour Movement Guidelines (24-MG)
4. Discussion
4.1. Implications for Policy and Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, K.C.; Shields, M.; de Groh, M.; Alfred, A.; Jo-Anne, G. Overweight and Obesity in Children and Adolescents: Results from the 2009 to 2011 Canadian Health Measures Survey. Health Rep. 2012, 23, 37–41. [Google Scholar]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J.M. Tracking of Childhood Overweight into Adulthood: A Systematic Review of the Literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Sassi, F.; Lauer, J.A.; Lee, Y.; Guajardo-Barron, V.; Chisholm, D. Tackling of Unhealthy Diets, Physical Inactivity, and Obesity: Health Effects and Cost-effectiveness. Lancet 2010, 376, 1775–1784. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health Benefits of Physical Activity: The Evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical Activity and Public Health: Recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Colley, R.C.; Carson, V.; Garriguet, D.; Janssen, I.; Roberts, K.C.; Tremblay, M.S. Physical Activity of Canadian Children and Youth, 2007 to 2015. Health Rep. 2017, 28, 8–16. [Google Scholar] [PubMed]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Gorber, S.C.; Kho, M.E.; et al. Systematic Review of the Relationships Between Objectively Measured Physical Activity and Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, 197–239. [Google Scholar] [CrossRef] [PubMed]
- Healthy Kids Panel. No Time to Wait: The Healthy Kids Strategy. Ontario Ministry of Health and Long Term Care; 2013. Available online: http://www.health.gov.on.ca/en/common/ministry/publications/reports/healthy_kids/healthy_kids.pdf (accessed on 20 January 2021).
- Health Promotion Division. Presentation to the Association of Local Public Health Agencies (alPHa). Ontario Ministry of Health and Long Term Care. 2014. Available online: https://cdn.ymaws.com/www.alphaweb.org/resource/collection/9221E880-473D-46C9-A428-F4F1A67305F8/KMS_HealthyKidsChallenge_210214.pdf (accessed on 20 January 2021).
- Borys, J.M.; Le Bodo, Y.; Jebb, S.A.; Seidell, J.C.; Summerbell, C.; Richard, D.; de Henauw, S.; Moreno, L.A.; Romon, M.; Visscher, T.L.S.; et al. SwinburnEPODE Approach for Childhood Obesity Prevention: Methods, Progress and International Development. Obes. Rev. 2012, 13, 299–315. [Google Scholar] [CrossRef]
- Healthy Kids Community Challenge–Evaluation. Process Implementation Evaluation. Public Health Ontario. 2018. Available online: https://www.publichealthontario.ca/en/health-topics/health-promotion/child-youth-health/hkcc?tab=2 (accessed on 20 January 2021).
- Ontario’s Healthy Kids Community Challenge–Program Logic Model. Public Health Ontario. 2016. Available online: https://www.publichealthontario.ca/-/media/documents/hkcc-logic-model.pdf?la=en (accessed on 20 January 2021).
- Moher, D. Healthy Kids Community Challenge, Year 1 Update. Healthy Kids Community Challenge Peterborough. 2016. Available online: https://sustainablepeterborough.ca/wp-content/uploads/2016/02/HKCC-Pres-to-SP-Sep15.2016.pdf (accessed on 20 January 2021).
- Healthy Kids Community Challenge–Evaluation. Outcome Evaluation. Public Health Ontario. 2018. Available online: https://www.publichealthontario.ca/en/health-topics/health-promotion/child-youth-health/hkcc?tab=1 (accessed on 15 May 2019).
- Rao, D.P.; Kropac, E.; Do, M.T.; Roberts, K.C.; Jayaraman, G.C. Childhood Overweight and Obesity Trends in Canada. Health Rep. 2016, 36, 194–198. [Google Scholar] [CrossRef]
- Janakiraman, R.; Sismeiro, C.; Dutta, S. Perception Spillovers Across Competing Brands: A Disaggregate Model of how and when. J. Market Res. 2009, 46, 467–481. [Google Scholar] [CrossRef]
- Trickett, E.J. Multilevel Community-Based Culturally Situated Interventions and Community Impact: An Ecological Perspective. Am. J. Community Psychol. 2009, 43, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Leatherdale, S.T. Natural Experiment Methodology for Research: A Review of how Different Methods can Support Real-World Research. Int. J. Soc. Res. Method 2018, 22, 19–35. [Google Scholar] [CrossRef]
- Leatherdale, S.T.; Brown, K.S.; Carson, V.; Childs, R.A.; Dubin, J.A.; Elliott, S.J.; Faulkner, G.; Hammond, D.; Manske, S.; Catherine, M.; et al. The COMPASS Study: A Longitudinal Hierarchical Research Platform for Evaluating Natural Experiments Related to Changes in School-Level Programs, Policies and Built Environment Resources. BMC Pub. Health 2014, 14, 331. [Google Scholar] [CrossRef]
- Leatherdale, S.T.; Laxer, R.E.; Faulkner, G. Reliability and Validity of the Physical Activity and Sedentary Behaviour Measures in the COMPASS Study; COMPASS Technical Report Series; University of Waterloo: Waterloo, ON, Canada, 2014; p. 2. Available online: https://uwaterloo.ca/compass-system/publications/reliability-and-validity-physical-activity-and-sedentary (accessed on 14 May 2019).
- Chinapaw, M.J.; Mokkink, L.B.; van Poppel, M.N.; Mokkink, L.B.; Terwee, C.B.; Dietz, P. Physical Activity Questionnaires for Youth: A Systematic Review of Measurement Properties. Sports Med. 2010, 40, 539–563. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, 311–327. [Google Scholar] [CrossRef]
- SAS 9.4 [Computer Program]; SAS Institute Inc.: Cary, NC, USA, 2016.
- Roux, L.; Pratt, M.; Tengs, T.O.; Yore, M.M.; Yanagawa, T.L.; van den Bos, J.; Rutt, C.; Brownson, R.C.; Powell, K.E.; Heath, G. Cost Effectiveness of Community-Based Physical Activity Interventions. Am. J. Prev. Med. 2008, 35, 578–588. [Google Scholar] [CrossRef]
- van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of Interventions to Promote Physical Activity in Children and Adolescents: Systematic Review of Controlled Trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef] [PubMed]
- Brand, T.; Pischke, C.R.; Steenbock, B.; Schoenbach, J.; Poettgen, S.; Samkange-Zeeb, F.; Zeeb, H. What Works in Community-Based Interventions Promoting Physical Activity and Healthy Eating? A Review of Reviews. Int. J. Environ. Res. Public Health 2014, 11, 5866–5888. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, B.; Henley, W.; Wilkin, T. Effectiveness of Intervention on Physical Activity of Children: Systematic Review and Meta-Analysis of Controlled Trials with Objectively Measured Outcomes (EarlyBird 54). BMJ 2012, 345, 5888. [Google Scholar] [CrossRef] [PubMed]
- Bock, C.; Jarczok, M.N.; Litaker, D. Community-Based Efforts to Promote physical Activity: A Systematic Review of Interventions Considering Mode of Delivery, Study Quality and Population Subgroups. J. Sci. Med. Sport. 2014, 17, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Vine, M.M.; Jarvis, J.W.; Chong, E.; Laxer, R.E.; Ladak, A.; Manson, H. An Early Implementation Assessment of Ontario’s Healthy Kids Community Challenge: Results from a Survey of Key Stakeholders. BMC Pub. Health 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Saunders, R.P.; Ward, D.S.; Felton, G.; Trost, S.G.; Dowda, M. Evaluation of a Community-Based Intervention to Promote Physical Activity in Youth: Lessons from Active Winners. Am. J. Health Prom. 2003, 17, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Cooper, C.; Gunnell, D.; Haw, S.; Lawson, K.; Macintyre, S.; Ogilvie, D.; Petticrew, M.; Reeves, B.; Sutton, M.; et al. Using Natural Experiments to Evaluate Population Health Interventions: New Medical Research Council guidance. J. Epidemio. Community Health 2012, 66, 1182–1186. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Repeat Cross-Sectional Sample | Longitudinal Sample | |||||
|---|---|---|---|---|---|---|
| Time 1 (2014–2015) N = 31,548 | Time 2 (2015–2016) N = 31,457 | Time 3 (2016–2017) N = 30,454 | Time 1 (2014–2015) (n = 3906) | Time 2 (2015–2016) (n = 3906) | Time 3 (2016–2017) (n = 3906) | |
| Mean | Mean | Mean | Mean | Mean | Mean | |
| Moderate-to-Vigorous Physical Activity (min/day) | 123.5 | 125.8 | 125.4 | 123.8 | 120.0 | 112.5 |
| Control Group 1 a | 123.0 | 125.4 | 126.0 | 121.5 | 121.5 | 113.1 |
| Control Group 2 b | 128.7 | 124.9 | 123.5 | 123.0 | 107.5 | 98.8 |
| Intervention Group 1 c | 122.7 | 124.0 | 129.4 | 116.8 | 117.2 | 112.6 |
| Intervention Group 2 d | 122.1 | 125.9 | 123.7 | 128.1 | 120.7 | 114.1 |
| Intervention Group 3 e | 127.4 | 128.9 | 129.6 | 121.2 | 115.3 | 110.2 |
| Strength Training (days/week) | 2.8 | 2.8 | 2.7 | 2.9 | 2.7 | 2.5 |
| Control Group 1 a | 2.8 | 2.7 | 2.7 | 2.9 | 2.6 | 2.5 |
| Control Group 2 b | 2.7 | 2.8 | 2.7 | 2.6 | 2.6 | 2.4 |
| Intervention Group 1 c | 2.5 | 2.6 | 2.6 | 2.5 | 2.5 | 2.6 |
| Intervention Group 2 d | 2.9 | 2.8 | 2.7 | 3.1 | 2.7 | 2.5 |
| Intervention Group 3 e | 3.0 | 2.9 | 2.8 | 2.9 | 3.0 | 2.6 |
| % | % | % | % | % | % | |
| Meets Canadian 24-Hour Movement Guidelines (yes) | 48.4 | 50.4 | 50.5 | 48.7 | 50.3 | 46.8 |
| Control Group 1 a | 47.9 | 50.3 | 50.3 | 46.4 | 50.7 | 46.2 |
| Control Group 2 b | 48.4 | 48.2 | 48.4 | 46.3 | 47.3 | 32.5 |
| Intervention Group 1 c | 48.4 | 48.4 | 51.7 | 50.9 | 54.9 | 42.0 |
| Intervention Group 2 d | 47.9 | 50.4 | 50.4 | 51.8 | 50.2 | 49.0 |
| Intervention Group 3 e | 52.4 | 53.4 | 53.0 | 50.7 | 49.8 | 50.2 |
| Pre-Intervention (T1) | Intervention (T1 to T2) | Post-Intervention (T1 to T3) | |
|---|---|---|---|
| Meets Canadian 24-Hour Movement Guidelines (yes) | % | Relative Risk Ratio (RRR) | |
| Control Group 1 a (reference) | 47.9 | 1.00 | 1.00 |
| Control Group 2 b | 48.4 | 0.95 | 0.95 |
| Intervention Group 1 c | 48.4 | 0.95 | 1.02 |
| Intervention Group 2 d | 47.9 | 1.00 | 1.00 |
| Intervention Group 3 e | 52.4 | 0.97 | 0.95 |
| Model 1: Moderate-to-vigorous physical activity (min/day) | Longitudinal Linear Regression β (95% CI) |
| Control Group 1 a (reference) | 1.00 |
| Control Group 2 b | −8.70 (−15.57, −1.83) * |
| Intervention Group 1 c | 2.75 (−9.55, 15.05) |
| Intervention Group 2 d | −3.15 (−6.19, −0.11) * |
| Intervention Group 3 e | −1.40 (−6.57, 3.77) |
| Model 2: Strength Training (days/week) | Longitudinal Ordinal Regression OR (95% CI) |
| Control Group 1 a (reference) | 1.00 |
| Control Group 2 b | 0.08 (0.23, −0.08) |
| Intervention Group 1 c | 0.13 (0.50, −0.23) |
| Intervention Group 2 d | 0.04 (0.35, −0.27) |
| Intervention Group 3 e | 0.07 (0.31, −0.17) |
| Model 3: Meets Canadian 24-Hour Movement Guidelines (%) | Longitudinal Logistic Regression OR (95% CI) |
| Control Group 1 a (reference) | 1.00 |
| Control Group 2 b | 0.73 (0.60, 0.89) * |
| Intervention Group 1 c | 0.84 (0.59, 1.19) |
| Intervention Group 2 d | 0.95 (0.86, 1.03) |
| Intervention Group 3 e | 0.99 (0.85, 1.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leatherdale, S.T.; Burns, K.E.; Qian, W.; Faulkner, G.; Carson, V. Evaluating the Impact of the Healthy Kids Community Challenge (HKCC) on Physical Activity of Older Youth. Int. J. Environ. Res. Public Health 2021, 18, 3083. https://doi.org/10.3390/ijerph18063083
Leatherdale ST, Burns KE, Qian W, Faulkner G, Carson V. Evaluating the Impact of the Healthy Kids Community Challenge (HKCC) on Physical Activity of Older Youth. International Journal of Environmental Research and Public Health. 2021; 18(6):3083. https://doi.org/10.3390/ijerph18063083
Chicago/Turabian StyleLeatherdale, Scott T., Kathleen E. Burns, Wei Qian, Guy Faulkner, and Valerie Carson. 2021. "Evaluating the Impact of the Healthy Kids Community Challenge (HKCC) on Physical Activity of Older Youth" International Journal of Environmental Research and Public Health 18, no. 6: 3083. https://doi.org/10.3390/ijerph18063083
APA StyleLeatherdale, S. T., Burns, K. E., Qian, W., Faulkner, G., & Carson, V. (2021). Evaluating the Impact of the Healthy Kids Community Challenge (HKCC) on Physical Activity of Older Youth. International Journal of Environmental Research and Public Health, 18(6), 3083. https://doi.org/10.3390/ijerph18063083