
Overuse of Health Care in the Emergency Services in Chile

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Background
2.1. Emergency Service
2.2. The Health Service User
3. Materials and Methods
4. Description of the Attention Process
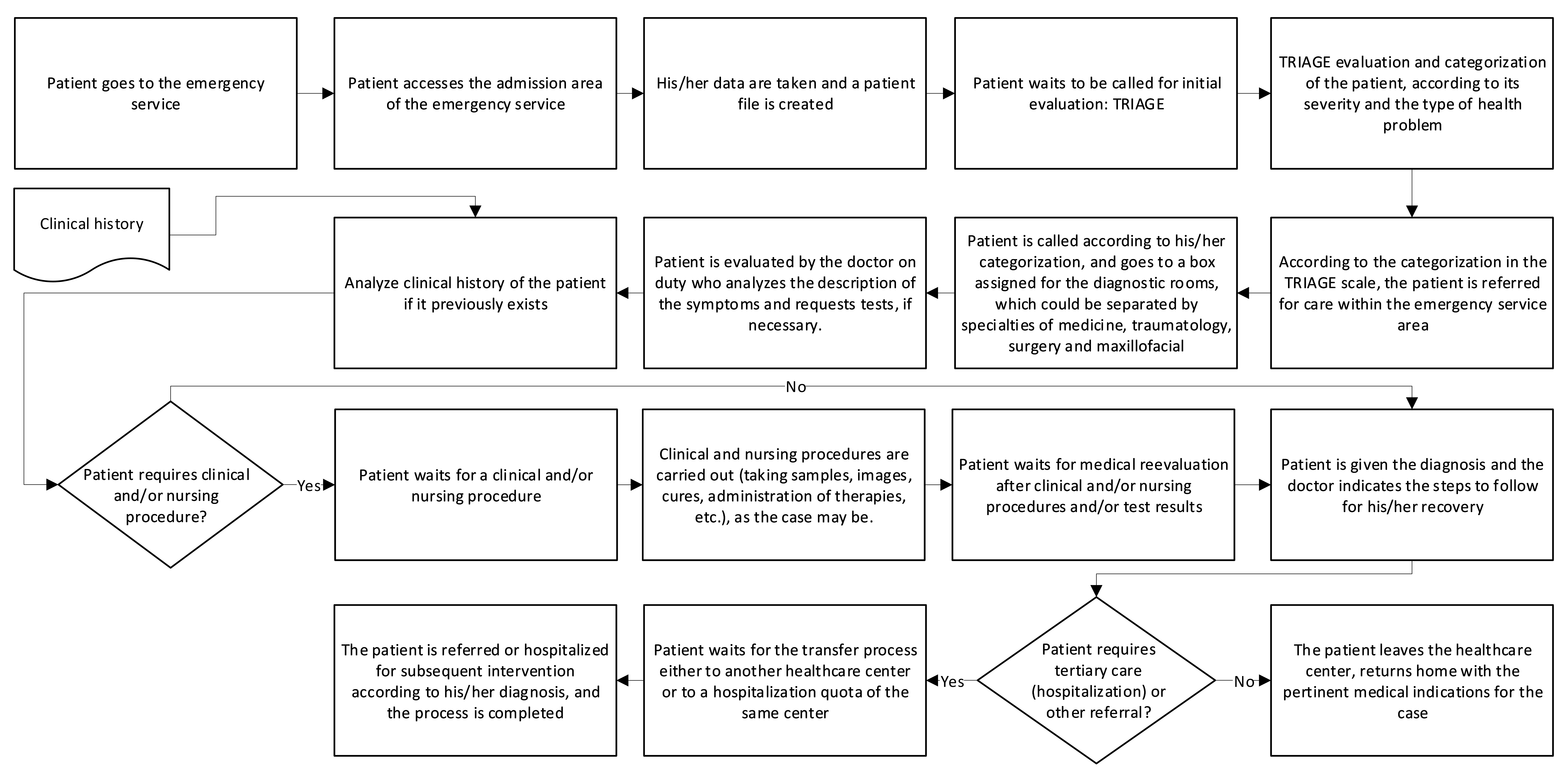
4.1. Emergency Attention Process
- It begins when a person detects an anomaly that must be solved immediately because it causes malaise, pain, fear or some discomfort.
- The patient goes to the Healthcare Center, which has an emergency department, including an admission area of the service [35].
- Patient’s information is registered and a patient file is created.
- After a few minutes of waiting, they are called for an evaluation according to the severity and the type of health problem.
- An evaluation is made and the patient awaits their attention according to the waiting time established in the Triage.
- Notice is given to the patient for their healthcare and according to the categorization, they go to an assigned diagnostic room, which could be separated by specialties such as medicine, traumatology, surgery and maxillofacial sectors.
- The patient is examined by the doctor on duty who asks for a description of the symptoms and requests tests if necessary.
- The patient awaits the diagnosis or the results of its laboratory or radiology tests.
- The diagnosis is given to the patient and the doctor indicates the steps to follow for their recovery.
- The patient leaves the Healthcare Center or is hospitalized for subsequent intervention according to their diagnosis, and the process is completed.
4.2. Causes of Overuse of the Emergency Attention
- Poor coordination between the patients and the health providers. An example of this situation is observed when an extension of the waiting time occurs, generated by the saturation of the facilities because of the excess of demand produced by the people who go to the health facility with non-urgent needs [41].
- Patients have limited Access to the PHC [42] due to the lack of available medical appointments in the short term.
- In the primary care the anomaly situations must be searched for, which allows the detection of the pathology in a timely manner and thus, to achieve a correct referral to the Emergency Services for those patients who require other types of care, if necessary.
- There is not always a medical history of the patients who go to the Emergency Services, which produces delays at the time of their care in a health establishment due to the need of reconstructing their medical records from the beginning. In fact, despite the fact that the patient is registered in the Public Health System and is treated in their corresponding Assistance Network following all its regular channels, there is no online clinical file among the health institutions of the same System.
- Close to 88% of the PHC are of Municipal administration. The others respond to the Ministry of Health [46]. This shows a lack of unification of the service and among administrations.
- Hospitals have legal obligations according to law N 20.584, which regulates the rights and duties of the patients in relation to the actions linked to their health attention and finance; and the Emergency Law N 19,650 which guarantees that people who are in a vital emergency condition be cared for in the healthcare center closest to where they are. Therefore, despite the existence of an abundant flow, they cannot be sent to their homes [47].
- Lack of incentive for general practitioners and health professionals who are part of the PHC structure to specialize in family medicine [48].
- Few economic resources earmarked for the hiring of more professionals for the public health network in the three levels of attention. The medical staff must care for more patients than their capacity. For example, it is common that a nurse assists between 3 and 5 boxes, and a doctor assists between 6 and 10 attention boxes [8], producing a sub-optimal attention, a greater wear of the personnel, and an increase in the risk of making mistakes.
- Greater investments are required for Health Technology Assessment to improve centers, favoring faster and more effective processes to meet the demand of the population [49].
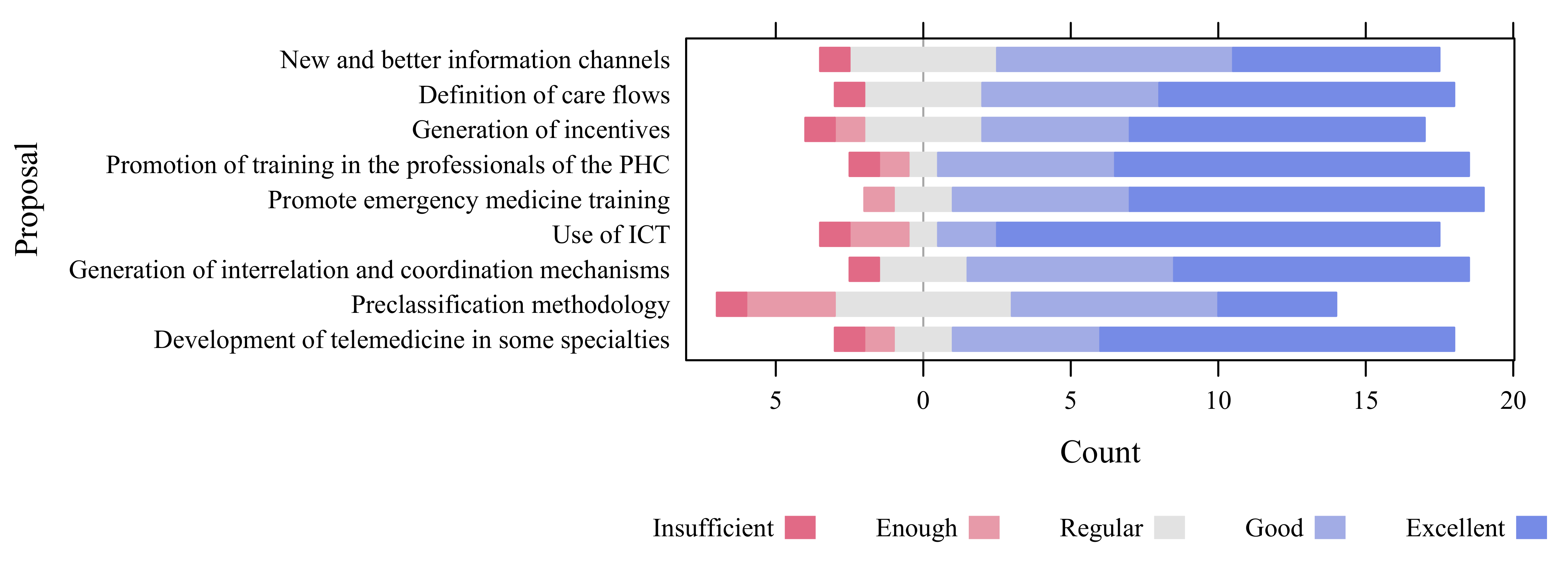
5. Results and Discussion
- Generate new information channels directly among the health centers or through channels as Social Media, so that patients can decide by themselves which health center to go to in order to solve their ailments; and finally, between both parties, be able to get a closer and more human relationship.
- Define the attention flows for the different category of patients, like a fast tracking sector or an area of fast attention for C4 and C5 patients, allowing the observation areas to be purely used by patients that can develop changes in their condition, such as C2 and C3, which have more probabilities of worsening or improving their condition. Managing the demand of patients of medium seriousness and those not serious (C3–C4), waiting times can be reduced, avoiding the misuse of the attention or the resources intended for really serious patients in addition to improving the perception of the service [26].
- Generate incentives for better work environments in resource management, work environment, and equipment so that health professionals are motivated and contribute more to the public health service. In this way, more efficient responses could be delivered to the population.
- Encourage the training of the professionals of the primary attention through the specialization in family medicine, with the goal of giving more accurate diagnosis and educating the population in relation to their health condition.
- Promote the education in emergency medicine for those professionals that are dedicated to this type of attention, so they can give faster and better clinical responses [51].
- Generate more coordination mechanisms among the three levels of primary, secondary and tertiary attention.
- Improve the existing coordination mechanisms between the three levels of primary, secondary and tertiary care.
- Use the methodology of pre-classification or pre-Triage of the patients [51] that reinforce the Triage, where it is possible to separate the demand according to the given classification where the patient is admitted.
- Design the attention flow and the management of spaces for the different kinds of attention, so that a dental consultant patient (C5) does not meet a C2 or C3 patient. This is as long as there are conditions in the physical plant and a prudent number of qualified professionals.
- Define the beginning of the waiting period, since this causes certain difficulties at the moment of assigning the attention boxes, and the priority of later attention.
6. Limitations
- Lack of participation of the external user (patient) in the analysis and execution of the improvement proposals. In Chile, there is no formal Association of patients who participate in public health policies, which is also a relevant issue that limits such actions.
- Bureaucratic aspects in the decision-making process of the Chilean Health System tend to be long and difficult. They end when an initiative benefits a line of action.
- The SARS Cov-2 pandemic has restricted the public agenda related to health issues. The authorities of the Health System have refocused their functions and the allocation of resources towards the health emergency.
- There is a need for allocation of more economic resources to incorporate more technology, train workers, take actions that reduce resistance to change, and encourage innovation.
- There is a need to strengthen the education about health promotion of people.
- There is a need for more efficient and effective management, at the level of primary care in family medicine as well as in specialties, to contribute to a decisive, assertive and quality health care.
- There is a need for more access to the information obtained from records and statistics, which are generally confidential.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AN | Assistance Network |
| FONASA | National Health Fund |
| ICT | Information and Communication Technologies |
| MinSal | Chilean Ministry of Health |
| OECD | Organisation for Economic Co-operation and Development |
| OICS | Office of Information, Claims and Suggestions |
| PHC | Primary Health Care |
References
- Sepulveda, D. La Experiencia en Salud Pública: Centrada en los Pacientes; Memoria de título carrera diseño gráfico, Pontificia Universidad Católica de Valparaíso: Valparaiso, Chile, 2012. [Google Scholar]
- OECD Stat. Health Care Resources: Physicians: Density per 1000 Population (Head Counts). Available online: https://stats.oecd.org/Index.aspx# (accessed on 25 April 2020).
- OECD. Recent Trends in International Migration of Doctors, Nurses and Medical Students; OECD Publishing: Paris, France, 2019; p. 139. [Google Scholar] [CrossRef]
- Guillou, M.; Carabantes C, J.; Bustos F, V. Availability of physicians and specialists in Chile. Rev. Med. Chil. 2011, 139, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lee, D.C.; Chung, M.; Liang, H.; Lock, D.; Sripipatana, A. Patient-Centered Medical Home Recognition and Clinical Performance in U.S. Community Health Centers. Health Serv. Res. 2017, 52, 984–1004. [Google Scholar] [CrossRef]
- Kim, J.; Kwok, E.; Cook, O.; Calder, L. Characterizing highly frequent users of a large Canadian urban emergency department. West. J. Emerg. Med. 2018, 19, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Grigini, V.; Schiavon, G.; Inoue, K.; Lopes de Moraes, N. Reception With Risk Classification: Characteristics of the Demand in an Emergency Unit. Rev. Cogitare Enferm. 2016, 21, 1–8. [Google Scholar] [CrossRef][Green Version]
- Tobar, E.; Retamal, A.; Garrido, N. Elementos de gestión para un Servicio de Urgencia de un hospital universitario. Rev. Hosp. Clínico Univ. Chile 2014, 25, 189–200. [Google Scholar]
- Grasset, E.; Obaíd, M. Especialidades derivadas de la cirugía general: Revisión de brechas e intención de residentes de la especialidad en Chile. Rev. Med. Chil. 2018, 146, 1325–1333. [Google Scholar] [CrossRef]
- Arcos, E.; Vollrath, A.; Sánchez, X.; Bailey, C. Motherhood inmigrant women in Chile: A qualitative study. Midwifery 2018, 66, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Cabieses, B.; Oyarte, M. Health access to immigrants: Identifying gaps for social protection in health. Rev. Saude Publica 2020, 54, 1–13. [Google Scholar] [CrossRef]
- Blukacz, A.; Cabieses, B.; Markkula, N. Inequities in mental health and mental healthcare between international immigrants and locals in Chile: A narrative review. Int. J. Equity Health 2020, 19, 197. [Google Scholar] [CrossRef] [PubMed]
- Morales, C.; Álvarez, N.; Candia, P.; Celedón, F.; Meyer, L.; Daniel, K.; Lombardic, N.; Guiraldes, E. Experiencia con el empleo del examen OSCE en el ciclo de evaluación de competencias clínicas de médicos que revalidan su título. Rev. Med. Chil. 2018, 146, 341–343. [Google Scholar] [CrossRef]
- Bendezu-Quispe, G.; León, F.; Moreno, J.; Inga-Berrospi, F. Características del servicio social para profesionales médicos en los estados andinos. Medwave 2020, 20, e7848. [Google Scholar] [CrossRef]
- Adams, J.G. Emergency Department Overuse: Perceptions and Solutions. JAMA 2013, 309, 1173–1174. [Google Scholar] [CrossRef] [PubMed]
- Klukowska-Röetzler, J.; Eracleous, M.; Müller, M.; Srivastava, D.S.; Krummrey, G.; Keidar, O.; Exadaktylos, A.K. Increased urgent care center visits by southeast european migrants: A retrospective, controlled trial from Switzerland. Int. J. Environ. Res. Public Health 2018, 15, 1857. [Google Scholar] [CrossRef] [PubMed]
- Superintendencia de Salud. Trámites y Servicios: Registro de Prestadores Acreditados; Superintendencia de Salud: Santiago, Chile; Available online: http://www.supersalud.gob.cl/servicios/669/w3-article-6193.html (accessed on 17 January 2021).
- Montagu, D. Accreditation and other external quality assessment systems for healthcare. DFID Health Syst. Resour. Cent. 2003, 1, 1–38. [Google Scholar]
- Nadkarni, A.; Weobong, B.; Weiss, H.A.; McCambridge, J.; Bhat, B.; Katti, B.; Murthy, P.; King, M.; McDaid, D.; Park, A.L.; et al. Counselling for Alcohol Problems (CAP), a lay counsellor-delivered brief psychological treatment for harmful drinking in men, in primary care in India: A randomised controlled trial. Lancet 2017, 389, 186–195. [Google Scholar] [CrossRef]
- Shah, M.N.; Gillespie, S.M.; Wood, N.; Wasserman, E.B.; Nelson, D.L.; Dozier, A.; McConnochie, K.M. High-intensity telemedicine-enhanced acute care for older adults: An innovative healthcare delivery model. J. Am. Geriatr. Soc. 2013, 61, 2000–2007. [Google Scholar] [CrossRef]
- Huang, J.A.; Tsai, W.C.; Chen, Y.C.; Hu, W.H.; Yang, D.Y. Factors associated with frequent use of emergency services in a medical center. J. Formos. Med. Assoc. 2003, 102, 222–228. [Google Scholar] [PubMed]
- Klejne, T.; Jayamaha, A.R. Knowledge of the in-hospital resuscitation algorithm among medical staff of selected hospital departments. Crit. Care Innov. 2019, 2, 9–16. [Google Scholar] [CrossRef]
- Freed, G.L.; Gafforini, S.; Carson, N. Age distribution of emergency department presentations in Victoria. EMA Emerg. Med. Australas. 2015, 27, 102–107. [Google Scholar] [CrossRef]
- Keogh, B.; Monks, T. The impact of delayed transfers of care on emergency departments: Common sense arguments, evidence and confounding. Emerg. Med. J. 2020, 37, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, G.; González, A.; Hernández, S.; Hernández, M. Análisis del servicio de Urgencias aplicando teoría de líneas de espera. Contad. Adm. 2017, 62, 719–732. [Google Scholar] [CrossRef]
- Gómez, J. Clasificación de pacientes en los servicios de urgencias y emergencias: Hacia un modelo de triaje estructurado de urgencias y emergencias. Emergencias 2003, 15, 165–174. [Google Scholar]
- Anderson, J.S.; Burke, R.C.; Augusto, K.D.; Beagan, B.M.; Rodrigues-Belong, M.L.; Frazer, L.S.; Stack, C.; Shukla, A.; Pope, J.V. The Effect of a Rapid Assessment Zone on Emergency Department Operations and Throughput. Ann. Emerg. Med. 2020, 75, 236–245. [Google Scholar] [CrossRef]
- Improta, G.; Romano, M.; Di Cicco, M.V.; Ferraro, A.; Borrelli, A.; Verdoliva, C.; Triassi, M.; Cesarelli, M. Lean thinking to improve emergency department throughput at AORN Cardarelli hospital. BMC Health Serv. Res. 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mix, A.; Pérez, P.; Saavedra, C.; Rodríguez, M.; del Fierro, V.; Price, Y.; Fischer, E.; Araos, F.; Cartagena, L.; Labra, L.M.; et al. Orientaciones Técnicas para el Rediseño al Proceso de Atención de Urgencia de Adulto, en las Unidades de Emergencia Hospitalaria; Ministerio de Salud: Santiago, Chile, 2018; p. 42.
- Ganapathy, K. Telemedicine and neurosciences. Neurol. India 2018, 66, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Mechanic, O.J.; Persaud, Y.; Kimball, A.B. Telehealth Systems. In StatPearls [Internet]; StatPearls Publishing: Bethesda, MD, USA, 2020. [Google Scholar]
- Asch, J.M.; Asch, D.A.; Klinger, E.V.; Marks, J.; Sadek, N.; Merchant, R.M. Google search histories of patients presenting to an emergency department: An observational study. BMJ Open 2019, 9, e024791. [Google Scholar] [CrossRef] [PubMed]
- Banham, D.; Karnon, J.; Densley, K.; Lynch, J.W. How much emergency department use by vulnerable populations is potentially preventable?: A period prevalence study of linked public hospital data in South Australia. BMJ Open 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Departamento de Estadísticas e Información de Salud (DEIS). Atenciones de Urgencia por Causa y Semanas estadísticas. Available online: http://cognos.deis.cl/ibmcognos/cgi-bin/cognos.cgi# (accessed on 27 January 2020).
- Johnson, K.D.; Punches, B.E.; Smith, C.R. Perceptions of the Essential Components of Triage: A Qualitative Analysis. J. Emerg. Nurs. 2021, 47, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Méndez, C.A.; Greer, S.L.; McKee, M. The 2019 crisis in Chile: Fundamental change needed, not just technical fixes to the health system. J. Public Health Policy 2020, 41, 535–543. [Google Scholar] [CrossRef]
- Zhang, S.; Morgenstern, H.; Albertus, P.; Nallamothu, B.K.; He, K.; Saran, R. Emergency department visits and hospitalizations among hemodialysis patients by day of the week and dialysis schedule in the United States. PLoS ONE 2019, 14, e0220966. [Google Scholar] [CrossRef] [PubMed]
- Ibanez-Sanchez, G.; Fernandez-Llatas, C.; Martinez-Millana, A.; Celda, A.; Mandingorra, J.; Aparici-Tortajada, L.; Valero-Ramon, Z.; Munoz-Gama, J.; Sepúlveda, M.; Rojas, E.; et al. Toward value-based healthcare through interactive process mining in emergency rooms: The stroke case. Int. J. Environ. Res. Public Health 2019, 16, 1783. [Google Scholar] [CrossRef] [PubMed]
- Abidova, A.; da Silva, P.A.; Moreira, S. Predictors of patient satisfaction and the perceived quality of healthcare in an emergency department in Portugal. West. J. Emerg. Med. 2020, 21, 391–403. [Google Scholar] [CrossRef]
- Lagos Tissie, D.; Bravo R., L. Mediación en el sistema público de salud: Oportunidades para mejorar. Rev. Med. Chil. 2020, 148, 211–215. [Google Scholar] [CrossRef]
- Lee, S.; Lee, Y.H. Improving Emergency Department E ffi ciency by Reinforcement Learning. Healthcare 2020, 8, 77. [Google Scholar] [CrossRef] [PubMed]
- Santelices, E.; Luis Santelices, J. Descripción y análisis del sistema de red de urgencia (Rdu) en Chile. Recomendaciones desde una mirada sistémica. Rev. Méd. Clín. Condes 2017, 28, 186–198. [Google Scholar] [CrossRef]
- Savage, D.W.; Woolford, D.G.; Weaver, B.; Wood, D. Developing emergency department physician shift schedules optimized to meet patient demand. Can. J. Emerg. Med. 2015, 17, 3–12. [Google Scholar] [CrossRef]
- Echeverría, G.; Tiboni, O.; Berkowitz, L.; Pinto, V.; Samith, B.; von Schultzendorff, A.; Pedrals, N.; Bitran, M.; Ruini, C.; Ryff, C.D.; et al. Mediterranean lifestyle to promote physical, mental, and environmental health: The case of Chile. Int. J. Environ. Res. Public Health 2020, 17, 8482. [Google Scholar] [CrossRef] [PubMed]
- Abramo, L.; Cecchini, S.; Ullmann, H. Addressing health inequalities in Latin America: The role of social protection. Cien. Saude Colet. 2020, 25, 1587–1598. [Google Scholar] [CrossRef] [PubMed]
- Subsecretaría de Redes Asistenciales. Eje Gestión de Recursos Financieros en Atención Primaria; Technical report; Ministerio de Salud, Gobierno de Chile: Santiago, Chile, 2015.
- Tay, L.; Becerra, C. Ley de urgencia y riesgo vital. Rev. Méd. Clín. Condes 2011, 22, 585–591. [Google Scholar] [CrossRef][Green Version]
- González Calbano, A.; Padula Anderson, M.I.; Tamez Rodríguez, A.R.; Godoy, A.C.; Barreto Quintana, H.M.; Martins, I.; Perozo García, J.C.; Muñoz, K.; Orellana, P.; Carrasco, R.V.; et al. Expansión de la medicina familiar en América Latina: Desafíos y líneas de acción. Rev. Panam. Salud Pública 2018, 42, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Manterola, C.; Otzen, T.; Castro, M.; Grande, L. Evaluación de tecnologías sanitarias (ETESA) una visión global del concepto y de sus alcances. Int. J. Morphol. 2018, 36, 1134–1142. [Google Scholar] [CrossRef][Green Version]
- Gasperini, B.; Pierri, F.; Espinosa, E.; Fazi, A.; Maracchini, G.; Cherubini, A. Is the fast-track process efficient and safe for older adults admitted to the emergency department? BMC Geriatr. 2020, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Visintin, F.; Caprara, C.; Puggelli, F. Experimental design and simulation applied to a paediatric emergency department: A case study. Comput. Ind. Eng. 2019, 128, 755–781. [Google Scholar] [CrossRef]
- Faujdar, D.S.; Sahay, S.; Singh, T.; Kaur, M.; Kumar, R. Field testing of a digital health information system for primary health care: A quasi-experimental study from India. Int. J. Med. Inform. 2020, 141, 104235. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.C.; Macy, M.L.; Simon, N.J.; Stephen, R.; Lehnig, K.; Bohling, K.; Schinasi, D.A. Emergency Care Connect: Extending Pediatric Emergency Care Expertise to General Emergency Departments Through Telemedicine. Acad. Pediatr. 2020, 20, 577–584. [Google Scholar] [CrossRef]
- Leszczyński, P.; Gotlib, J.; Kopański, Z.; Wejnarski, A.; Świezewski, S.; Gałazkowski, R. Analysis of Web-based learning methods in emergency medicine: Randomized controlled trial. Arch. Med. Sci. 2018, 14, 687–694. [Google Scholar] [CrossRef]
- Sun, S.; Lu, S.F.; Rui, H. Does Telemedicine Reduce Emergency Room Congestion? Evidence from New York State. Inf. Syst. Res. 2020, 31, 972–986. [Google Scholar] [CrossRef]
- Shah, M.N.; Wasserman, E.B.; Wang, H.; Gillespie, S.M.; Noyes, K.; Wood, N.E.; Nelson, D.; Dozier, A.; McConnochie, K.M. High-Intensity Telemedicine Decreases Emergency Department Use by Senior Living Community Residents. Telemed. e-Health 2015, 22, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Jedwab, R.M.; Chalmers, C.; Dobroff, N.; Redley, B. Measuring nursing benefits of an electronic medical record system: A scoping review. Collegian 2019, 26, 562–582. [Google Scholar] [CrossRef]
- Heiberger, R.M.; Burt Holland, B.H. Statistical Analysis and Data Display: An Intermediate Course with Examples in R, 2nd ed.; Springer Texts Statistics; Springer: New York, NY, USA, 2015; p. 898. [Google Scholar] [CrossRef]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020, 18, 329. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Region | Emergency Care | Primary Care | Specialties Care | Total | Emergency | People in Health | Population | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | % | Number | % | Number | % | Care | 1000 in hab. | 10,000 in hab. | ||
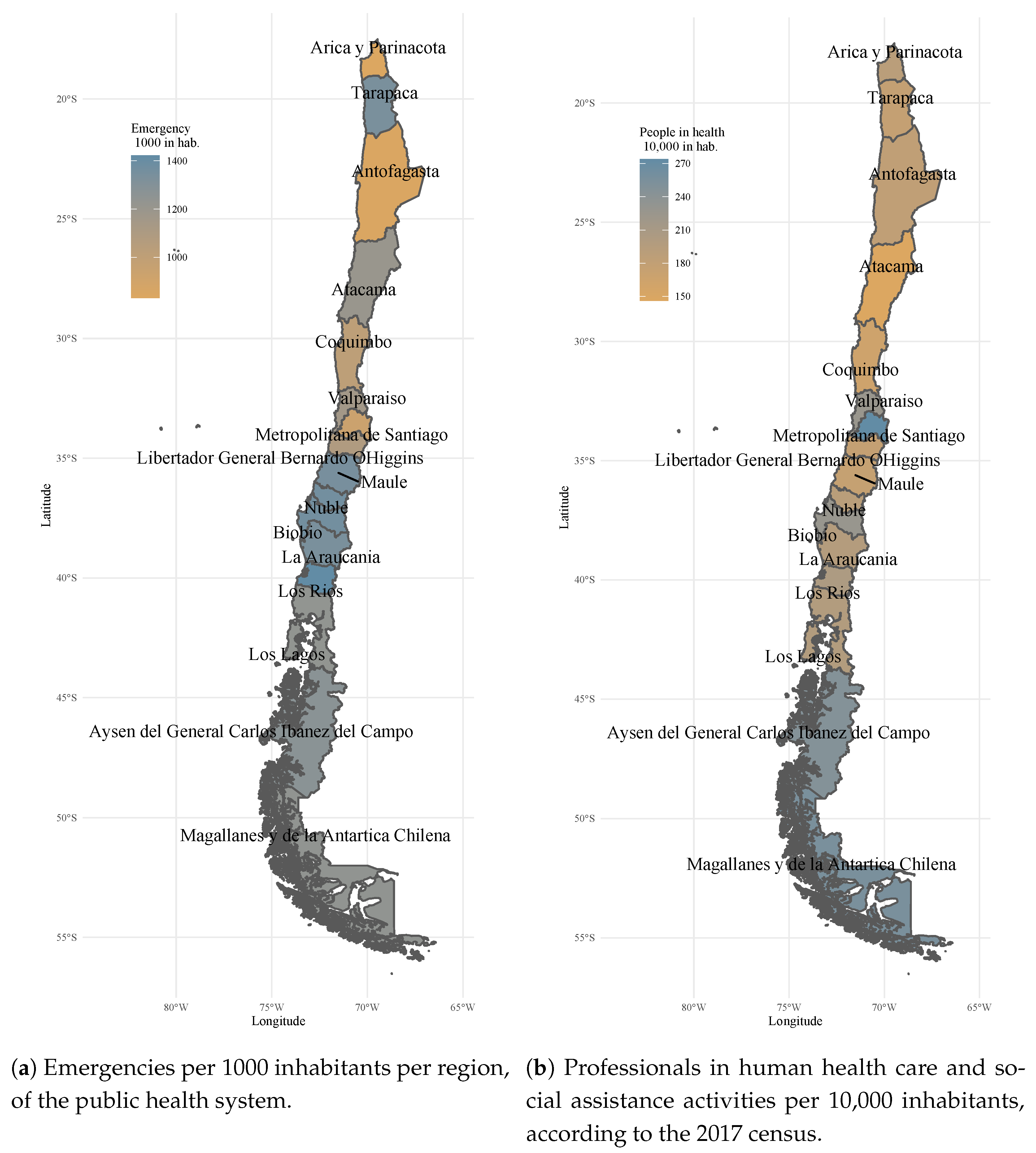
| Arica and Parinacota | 188,358 | 38.1% | 175,268 | 35.4% | 130,961 | 26.5% | 494,587 | 833 | 189 | 226,068 |
| Tarapacá | 442,356 | 48.6% | 332,969 | 36.6% | 134,111 | 14.7% | 909,436 | 1338 | 177 | 330,558 |
| Antofagasta | 512,673 | 44.3% | 387,985 | 33.5% | 256,491 | 22.2% | 1,157,149 | 844 | 182 | 607,534 |
| Atacama | 343,906 | 49.0% | 230,483 | 32.9% | 126,833 | 18.1% | 701,222 | 1202 | 146 | 286,168 |
| Coquimbo | 768,004 | 43.8% | 639,912 | 36.5% | 346,521 | 19.8% | 1,754,437 | 1014 | 164 | 757,586 |
| Valparaíso | 2,092,230 | 46.9% | 1,641,461 | 36.8% | 724,375 | 16.2% | 4,458,066 | 1152 | 226 | 1,815,902 |
| Metropolitan of Santiago | 6,666,899 | 40.9% | 6,445,116 | 39.5% | 3,203,522 | 19.6% | 16,315,537 | 937 | 274 | 7,112,808 |
| Libertador General Bernardo O’Higgins | 993,010 | 42.3% | 980,250 | 41.7% | 375,563 | 16.0% | 2,348,823 | 1086 | 177 | 914,555 |
| Maule | 1,407,230 | 46.5% | 1,096,038 | 36.2% | 523,404 | 17.3% | 3,026,672 | 1347 | 175 | 1,044,950 |
| Biobío and Ñuble | 2,778,550 | 43.4% | 2,482,816 | 38.7% | 1,146,719 | 17.9% | 6,408,085 | 1364 | 219 | 2037,414 |
| La Araucanía | 1,281,165 | 44.4% | 1,168,756 | 40.5% | 437,066 | 15.1% | 2,886,987 | 1338 | 198 | 957,224 |
| Los Ríos | 547,319 | 47.5% | 393,777 | 34.2% | 211,553 | 18.4% | 1,152,649 | 1422 | 204 | 384,837 |
| Los Lagos | 1,022,731 | 46.1% | 786,680 | 35.4% | 410,217 | 18.5% | 2,219,628 | 1234 | 198 | 828,708 |
| Aysén of general Carlos lbáñez del Campo | 131,300 | 38.1% | 126,528 | 36.7% | 86,929 | 25.2% | 344,757 | 1273 | 247 | 103,158 |
| Magallanes and Chilean Antartic | 206,326 | 45.6% | 121,621 | 26.9% | 124,699 | 27.5% | 452,646 | 1239 | 256 | 166,533 |
| Total country | 19,382,057 | 43.4% | 17,009,660 | 38.1% | 8,238,964 | 18.5% | 44,630,681 | 1103 | 229 | 17,574,003 |
| Category | Description of Seriousness |
|---|---|
| C1 | Patients in vital risk, i.e., those that require reanimation and/or immediate stabilization, because of the imminent vital risk. They have direct priority access to the reanimation box, and their attention must be immediate. Whoever recognizes the patient emergency activates the emergency alarm. |
| C2 | High complexity patients that require diagnostic and/or therapeutic actions, such as an evaluation, treatment and control for a period of time, which may require hospitalization and/or specialists’ consultation. Its most frequent characteristic is hemodynamics instability. The patient goes quickly to the box and the waiting time must not be more than 10 min. |
| C3 | Medium complexity patients that due to the nature of their pathology require diagnostic-therapeutic measures to determine a brief period of observation and subsequent discharge. The patient goes to the medical care box, where they are evaluated by the doctor according to availability. The waiting time should not be more than 60 min. |
| C4 | Patients with no real emergency. They are patients requiring a diagnostic procedure or a therapeutical one, including medical attention. |
| C5 | General consultation, i.e., any clinical situation that appears spontaneously and/or for a long-term that can produce only general discomfort in the patient. Because of the associated clinical condition, both the medical attention as well as the initial indication of treatment can be solved through the Primary Health Care (PHC). |
| TRIAGE | TRIAGE Categorization | Medical Evaluation | Clinical Procedures | Medical Reassessment | Referral, Transfer or Hospitalization | Total |
|---|---|---|---|---|---|---|
| C1 | As these are life-threatened patients, waiting times from C2 to C5 are not generated | |||||
| C2 | 18.1 | 22.2 | 32.5 | 38.2 | 37.5 | 148.5 |
| C3 | 32.3 | 48.5 | 70.4 | 49.6 | 188.7 | 389.5 |
| C4 | 40.5 | 90.3 | 75.5 | 128.4 | 52.7 | 387.4 |
| C5 | 39.2 | 101.9 | 98.3 | 196.8 | 64.3 | 500.5 |
| Proposal | Causes of the Problem of Interest | Description of the Solution | Measurement | Observations |
|---|---|---|---|---|
| (1) New and better information channels | Poor coordination between the patients and the health providers. Little education and promotion in relation to the preventive health in the patients and the good use of the service in general terms. Lack of unification of the service at PHC and differences among administrations. | Generation of new information channels making the distinction of the existence of a particular channel for the health center, the patients, and between them. Improve the connection of the information channels with the external user with the aim of guiding them in relation to the corresponding healthcare network, and improving the management of the reservation of medical appointments. | Impact | Patients would find themselves informed about the health centers and about the management of the reservation of medical appointments. |
| (2) Definition of medical care flows | Hospitals have legal obligations according to law, causing saturation of the system. | Definition of care flows for the different category of patients, such as a fast tracking or area for quick attention of C4 and C5 patients, leaving the observation areas only for the patients that can develop changes in their health state, such as C2 and C3 patients that have more probabilities of worsening or improving their condition. Management of the medium severity and not serious patients (C3-C4) demand can reduce the waiting time that can put in danger the care or the resources intended for the serious ill patients; as well as improve the perception of the service. | Effectiveness | It would considerably improve medical care flows. It requires the reinforcement of the medical staff and the infrastructure of the place. |
| (3) Generation of incentives | Lack of incentive for general practitioners and health professionals who are part of the PHC structure. Few economic resources earmarked for the hiring of more professionals for the public health network in the three levels of attention. | Generate an incentive in the health professionals so that the bet is the contribution of the public health service. To obtain more professionals that can give responses to the population. | Impact/ Effectiveness | The increase of the budget is required for public health. |
| (4) Promotion of training in the professionals of the PHC | Patients have limited access to the PHC. Little education and promotion in relation to the preventive health in the patients and the good use of the service in general terms. Lack of incentives for general practitioners and health professionals who are part of the PHC structure. | Promotion of the training of decision-making skills in the primary attention professionals, through the specialization in family medicine so they can give an accurate diagnosis, in order to educate the population in relation to their health condition. | Efectiveness | The doctor must have received professional training, and later made an effort through some type of integral training, diplomas and/or Master’s among others to favour this opportunity. |
| (5) Promote emergency medicine training | Few economic resources earmarked for the hiring of more professionals for the public health network in the three levels of attention. | Promotion of emergency medicine training for those who dedicate themselves to this type of attention, so they can sharpen their clinical eye on the immediate response. | Effectiveness | The doctor must have received professional training, and later make an effort through some type of integral training, diplomas and/or Master’s among others to favour this opportunity. |
| (6) Use of ICT | There is not always a medical record of the patients who go to the Emergency Services. Greater investments are required for Health Technology Assessment to improve centers. | Use of ICT to create systems allowing the access to the medical history of the patients, making this information available in any type of facility where the patient has arrived to ask for care. Creation of an electronic medical record system containing the patient medical history [57], and thus, favour the communication mechanisms among the various health centers at the time of provision of the medical care. | Impact/ Effectiveness | It will allow a prompt medical care through accessing the clinical history of the person attended, helping the diagnosis be faster and more accurate. |
| (7) Generation of interrelation and coordination mechanisms | Poor coordination between the patients and the health providers. | Generation of interrelations and coordination mechanisms among the three levels of care: primary, secondary and tertiary. | Impact | It will favor the communication and will be a more effective provision of services among all the actors. |
| (8) Pre-classification methodology | Hospitals have legal obligations according to law, causing saturation of the system. | Use of a pre-classification methodology of patients that reinforces the Triage [51], to separate the demand according to the classification given at the moment in which the patient is admitted. Designing care flows and management of the spaces for the different types of attentions required by C5 patients, or for a dental consultation, so that they do not run into a C2 or C3 patient attention sector (as long as there are conditions of the physical plant and a prudent amount of qualified professionals). | Effectiveness | It could be effective as long as the demand of staff is reinforced. On the contrary, it would be difficult for the simple fact that the experience is what determines, most of the time, the emergency that the patient is facing. |
| (9) Development of telemedicine in some specialties | Patients have limited Access to the PHC. Little education and promotion in relation to the preventive health in the patients and the good use of the service in general terms. Greater investments are required for Health Technology Assessment to improve medical centers. | Promotion of the use and development of telemedicine in some medical specialties to favor a more efficient and faster care flow in terms of immediate responses. | Impact | Its use will help various specialties which can be cared for from distance so it does not generate an increased flow of patients. In addition, this will allow the generation of a follow-up of the condition of the more immediate patient. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvial, X.; Rojas, A.; Carrasco, R.; Durán, C.; Fernández-Campusano, C. Overuse of Health Care in the Emergency Services in Chile. Int. J. Environ. Res. Public Health 2021, 18, 3082. https://doi.org/10.3390/ijerph18063082
Alvial X, Rojas A, Carrasco R, Durán C, Fernández-Campusano C. Overuse of Health Care in the Emergency Services in Chile. International Journal of Environmental Research and Public Health. 2021; 18(6):3082. https://doi.org/10.3390/ijerph18063082
Chicago/Turabian StyleAlvial, Ximena, Alejandra Rojas, Raúl Carrasco, Claudia Durán, and Christian Fernández-Campusano. 2021. "Overuse of Health Care in the Emergency Services in Chile" International Journal of Environmental Research and Public Health 18, no. 6: 3082. https://doi.org/10.3390/ijerph18063082
APA StyleAlvial, X., Rojas, A., Carrasco, R., Durán, C., & Fernández-Campusano, C. (2021). Overuse of Health Care in the Emergency Services in Chile. International Journal of Environmental Research and Public Health, 18(6), 3082. https://doi.org/10.3390/ijerph18063082