
Applications of Systems Science to Understand and Manage Multiple Influences within Children’s Environmental Health in Least Developed Countries: A Causal Loop Diagram Approach



Abstract
1. Introduction
2. Methodology
2.1. Literature Review
2.2. Causal Loop Diagram Principles
- reinforcing—a dengue fever epidemic where the number of infected mosquitos drives up the number of infected humans, which in turn increases the number of infected mosquitos;
- balancing—where sweating is initiated in response to heat to regulate human body temperature.
- reinforcing—denoted by a +, in which an increase in a variable causes an increase in the variable it influences and vice versa, or e.g., internal air pollution increases respiratory disease;
- opposing—denoted by a −, when an increase in a variable causes a decrease in the variable it influences and vice versa, e.g., a clean water supply decreases WASH-related disease [28].
2.3. Table and Causal Loop Diagram Creation
- variables that it directly influences;
- variables that it is directly influenced by.
3. Results
3.1. Child Mortality and Morbidity in LDCs
3.2. Exclusions from CLD Scope
3.3. Influencing Linkages
- Variables are described in the shortest form possible, e.g., vehicles means number of vehicles, family size means number of people in the biological family, and clean water means the availability of a clean water supply;
- Polarities of links are shown, e.g., open defaecation increases WASH-related disease;
- Each endogenous variable influences other variables in the tables and is in turn influenced by other variables. As an example, WASH-related disease is the variable in the first row of Table 2. It appears as an influencer (reinforcing or positive) of malnutrition/stunting in the second row of Table 2 and is shown as being influenced by open defaecation in Table 3;
- The relationship between the variable and the links appearing in the “influenced by” column is summarised in the table text with supporting references. Relationships for items in the influences column are summarised when they appear in the variable column, usually in another table;
3.3.1. Health Outcomes
3.3.2. Environmental Domain
- LDCs contribute only 0.5% of the annual carbon dioxide emissions that are driving climate change, producing 0.17 million kt of a global annual total of 34 m kt [57]. Climate change impacts are specific to individual countries and regions, but all LDCs are vulnerable to the effects of climate change, manifested in rising temperatures, changing landscapes, and increased magnitude and frequency of natural disasters [52]. Climate change has thus been treated as an exogenous variable, influencing but not being influenced by the other variables in the CLD [22].
- Remoteness is part of the economic vulnerability index for LDCs, calculated as an indicator of distance from world markets [59], and is a structural obstacle to the development of adequate infrastructure. Whilst an LDC can improve its infrastructure and services, it cannot change its geographical remoteness, which is thus an exogenous variable.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Influenced by | +/− | Influences | +/− | Source |
|---|---|---|---|---|---|
| Improved water supply—delivered through water services infrastructure. Poverty prevents community-based improvement of water supplies when not provided by the state. Disasters affect water supply by damaging infrastructure and by flooding, which leads to contamination of both natural and improved water supplies. | Infrastructure Poverty Disasters | + − − | Clean water Hygiene | + + | [3,18,52,54,60] |
| Clean water—In urban/peri-urban areas, polluted watercourses are the only water source for many. Clean water is depleted through open defaecation and pollution of natural resources through activities such as logging or mining. In rural areas, clean water may be available from natural sources such as springs but may be too far from dwellings to be easily accessible. | Improved water supply Open defaecation Natural resource depletion/pollution Disasters | + − − − | WASH-related disease | − | [3,18,52,54,60] |
| Improved sanitation—is generally dependent on an improved water supply and adequate investment in infrastructure to build and maintain it. Poverty prevents community-based sanitation improvements. Overcrowding in urban/peri-urban settings acts against sufficient improved sanitation. | Improved water supply Infrastructure Poverty Overcrowding | + + − − | Open defaecation | − | [3,18,41,54,61,62] |
| Open defaecation—is the norm for up to 70% of people in some LDCs, both in rural and peri-urban settings. In addition to providing access to adequate sanitation, behaviour change, influenced by education, is required to effect optimal use of sanitation and to overcome cultural norms and/or taboos. | Improved sanitation Cultural norms | − + | Clean water Vectors WASH-related disease | − + + | [3,18,41,54,61,62] |
| Vectors—open waste dumps, pooled surface waters, and open faeces in LDCs attract insects and rodents, especially in overcrowded settings. Climate change-related temperature rise increases vector breeding sites. | Open defaecation Household waste management Climate change * | + − + | Vector-borne disease | + | [51,63,64] |
| Overcrowding—mostly in urban/peri-urban areas. Unsafe surroundings are often associated with a poor quality built environment and slum dwellings with insecure structures. Culture in some LDCs requires extended family to house migrating relatives, which increases overcrowding. | Poverty Urban migration Cultural norms | + + + | Injury Respiratory disease Skin diseases | + + + | [18,39,49] |
| Internal air pollution (IAP)—caused by biomass cooking and lighting fuel, including wood and kerosene. Second-hand smoking and AAP that enters the home also contribute to IAP. | Biomass cooking Second-hand smoke AAP | + + + | Respiratory disease Ambient air pollution | + + | [3,18,65] |
| Second-hand smoke—smoking is an established part of the culture in many LDCs. | Cultural norms | + | IAP | + | [3,18,65] |
| Ambient air pollution (AAP) and vehicle pollution—in urban environments with concentrated populations, open burning of waste as well as vehicle traffic contribute to AAP. IAP becomes AAP. LDCs rarely have effective pollution controls and are likely to import ageing vehicles that no longer comply with richer countries’ stricter emission standards. Poorly surfaced roads create dust pollution. Rising temperatures due to climate change increase AAP. | IAP Outdoor waste burning Vehicle pollution Climate change * | + + + + | Respiratory disease | + | [18,34,65,66] |
| Household waste management—is often inadequate in LDCs, particularly in urban areas, due to lack of infrastructure and funding, leading to household and other waste burning. | Infrastructure | + | Vectors Outdoor waste burning | − − | [67] |
| Natural resource depletion and pollution—is caused by increased population pressure, overexploiting resources beyond their sustainable limits (e.g., harvesting wood for fuel), and poor waste management. Pollution compromises natural water supplies. | Population Cooking with biomass fuel | + − | Deforestation/desertification Adequate child nutrition Clean water | + − − | [68,69] |
| Deforestation/desertification—is caused by natural resource depletion and accelerated by climate change. | Climate change * | + | [68,69] | ||
| Natural disasters—are increasing in frequency and magnitude. Many LDCs are in disaster-prone areas and do not have resources to mitigate the effects of natural disasters due to both inadequate infrastructure and inadequate disaster response resources | Climate change * | + | Injury Vectors Clean water Urban migration | + + − + | [70,71] |
3.3.3. Social Domain
| Variable | Influenced by | +/− | Influences | +/− | Source |
|---|---|---|---|---|---|
| Child education—is reduced by poor health and malnutrition and exposure to biomass fuel, which affect cognitive ability. It is impaired by poverty and by the expectations and priorities of the child’s carers, who may prioritise work or care of younger children over a child’s education, particularly for females. In rural areas, a lack of electricity and low access to schools reduce study opportunities. | Poverty Adult education Child morbidity/malnutrition Electricity | − + − + | Adult educational attainment | + | [45,73,74,75] |
| Adult educational attainment—adult education levels are improved as better educated children grow into adults. | Child education | + | Malnutrition/stunting Family size Hygiene | − − + | [59,76] |
| Cultural norms—cultural norms and behaviours that affect many influencers of children’s environmental health (CEH) are influenced by education levels. Examples are the inverse relationship between adult female education level and family size and cooking with biomass fuel, an established tradition in most LDCs. Similarly, open defaecation in rural settlements is associated with privacy and comfort in many LDCs, and a move to improved sanitation can only be made with both infrastructure in place and a change of cultural norms. | Adult educational attainment | − | Family size Adequate child nutrition Open defaecation Cooking with biomass fuel Second-hand smoke Overcrowding/unsafe surroundings | − − + + + + | [76,77] |
| Family planning availability—LDCs have both low contraceptive use (39%) and a high unmet need for family planning (22%). Poverty is associated with a lack of access to modern family planning services, whereas living in urban areas is associated with better access. | Poverty Urban migration | + − | Family size | − | [78] |
| Family size—cultural norms and expectations, reinforced by the requirement for children to support their parents, keep birth rates high, particularly in rural areas where the cost of raising a child is low and access to modern family planning services is limited or non-existent. | Family planning availability Cultural norms | − + | Population Adequate child nutrition | + − | [78,79] |
| Hygiene—handwashing and hygienic food preparation require an improved water supply close to the home. The definition of a basic water supply is up to 30 min round trip, which is not conducive to hygienic habits. Adult education, both general and WASH specific, is a prerequisite for the establishment of hygiene in families/communities. | Improved water supply Soap Adult educational attainment | + + + | WASH-related disease | − | [60] |
3.3.4. Economic Domain
| Variable | Influenced by | +/− | Influences | +/− | Source |
|---|---|---|---|---|---|
| Poverty—low economic development leads to limited individual economic opportunity in LDCs. This is reinforced by low levels of education and large family sizes, which drain resources and increase the family income needed to live above the poverty line. Illness and premature death, with their origins in childhood morbidity, deprive families of their breadwinners or require discretionary but often non-existent health expenditure. Rural poverty drives urban migration, which also reinforces poverty due to higher food and living costs and inadequate infrastructure, particularly in informal settlements. | Economic development Adult morbidity/premature mortality Adult educational attainment Urban migration Family size | − + − + − | Urban migration/overcrowding Adequate child nutrition Lack of access to clean fuel Improved sanitation/soap | + − + − | [54,82,83] |
| Economic development—influenced by the remoteness that characterises LDCs and by adult health outcomes. There are many other influences outside the scope of this study that could form an economics-focused causal loop diagram (CLD). | Remoteness * Adult morbidity/premature mortality | − − | Poverty Infrastructure/electricity | − + | [56,58,59] |
| Adequate child nutrition—has different influencers in urban and rural settings. Living below the poverty line does not in itself deny children access to sufficient nutrition as long as natural resources can support food production or hunting/fishing. Large family sizes make consistent availability of food more difficult, particularly in urban areas where a subsistence lifestyle cannot be practised. In some LDCs, cultural practices mean that food priority is not given to children. | Poverty Family size Natural resource depletion/pollution Adult education Cultural norms | − − − + − | Malnutrition/stunting | − | [44,45,77,83,84] |
| Soap—food takes priority over soap when there are limited financial resources. | Poverty | − | Hygiene | + | [18] |
| Urban migration—LDCs are less urbanised than their more developed counterparts, with an average of 70% of their populations living in rural settings, but their urbanisation rates are higher than global averages as rural poverty and climate change drives families to cities, often to live in urban or peri-urban informal settlements with poor infrastructure. | Poverty Climate change * | + + | Overcrowding Poverty Family planning availability Family size | + + + − | [9,79,85] |
| Infrastructure/electricity—which includes transport, WASH, and health facilities, is caused by low funding and compounded by the remoteness of many LDCs. Infrastructure is easily damaged by disasters, which are increasing as the impacts of climate change worsen. Population growth does not affect the absolute level of infrastructure and electricity investment but does influence its per capita availability. Small-scale solar electricity is still economically out of reach of many people in LDCs. | Economic development Remoteness * Population growth | + − − | Health services/clean fuel/improved water Household waste management | + + | [70,86] |
| Health services—many rural children in LDCs can only reach health facilities on a planned trip, if at all, leaving them vulnerable in emergency situations. Rural health facilities are short of qualified personnel, essential supplies, and medicines and may have no electricity, compromising the cold chain. Urban resources are stretched by growing populations. Items such as mosquito nets are in short supply. | Infrastructure Remoteness * | + − | Child morbidity/mortality | − | [7,81] |
| Clean fuel—rural poor cannot afford clean alternatives to biomass fuels such as wood, which they can collect for free but at great personal costs in time and distance travelled. Alternatives are unavailable if there is no electricity or distribution infrastructure. | Poverty Infrastructure/electricity | − + | Cooking with biomass fuel | − | [6,7] |
| Cooking with biomass fuel—cultural as well as financial barriers must also be overcome to change behaviours to move towards clean cooking methods. | Clean fuel Cultural norms | − + | IAP | + | [18,87] |
| Vehicles—as poverty reduces, vehicle numbers, particularly in urban areas, grow. | Poverty | − | Vehicle emissions | + | [4,7,88] |
3.4. Overall Causal Loop Diagram
3.5. Analysis of Causal Loops
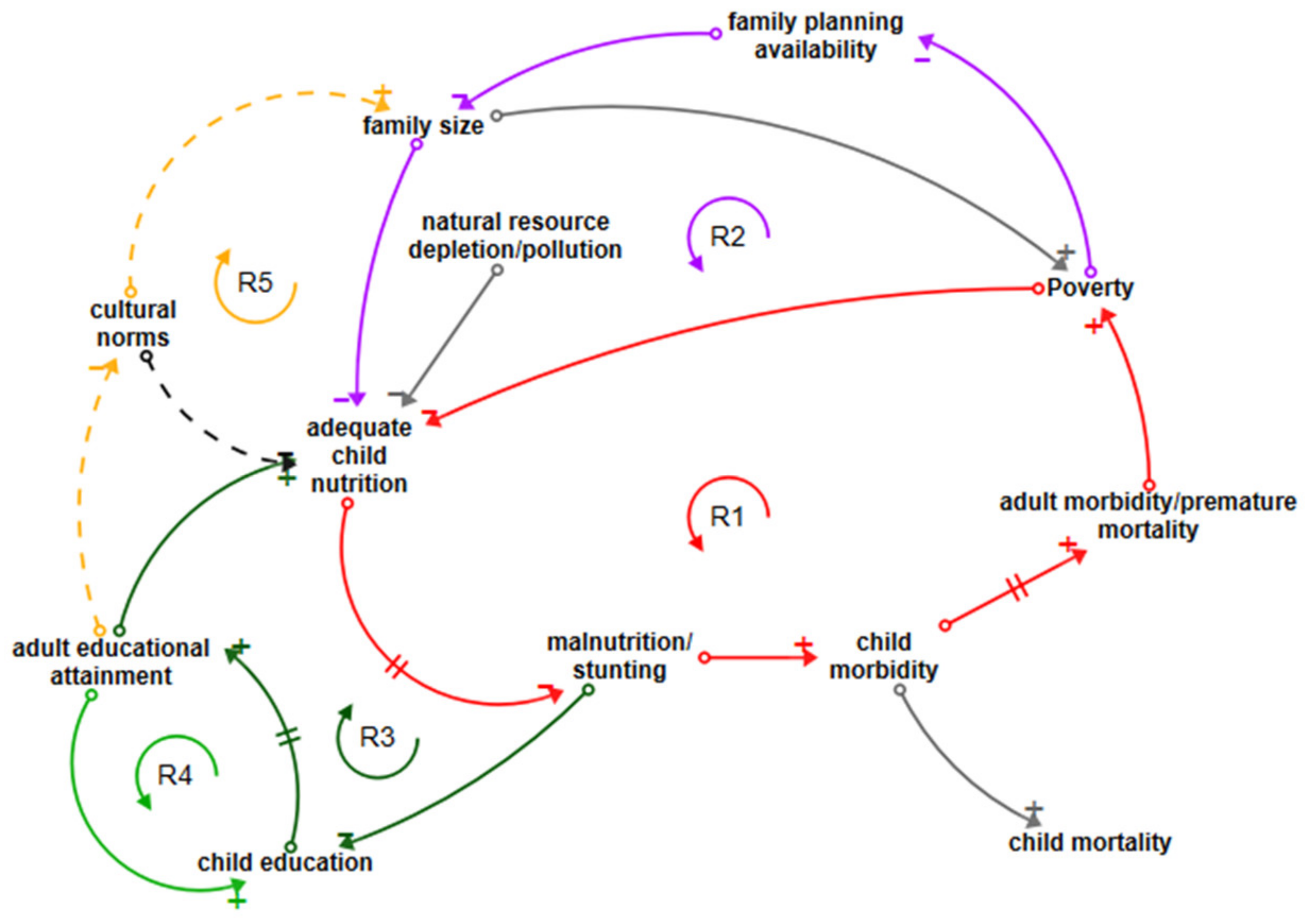
3.5.1. Nutritional Deficiency Loops
3.5.2. WASH-Related Disease Loops
3.5.3. Air Pollution-Related Disease Loops
3.5.4. Vector-Related Disease and Skin Disease Loops
3.5.5. Neonatal Disease Loops
3.5.6. Population Growth Loops
3.6. Leverage Points
4. Discussion
4.1. Application of the CLD
4.2. Potential Application for Systems Science in CEH
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Claudio, L. The impact of poverty, disparity and injustice on Children’s Environmental Health. In Textbook of Children’s Environmental Health; Landrigan, P., Etzel, R., Eds.; Oxford University Press: Oxford, UK, 2014; pp. 528–536. ISBN 978-019-992-957-3. [Google Scholar]
- WPRO. Human Health and Climate Change in Pacific Island Countries; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- WHO. Don’t Pollute My Future! The Impact of the Environment on Children’s Health; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- UNICEF. The Challenges of Climate Change: Children on the Front Line; UNICEF Office of Research: Florence, Italy, 2014. [Google Scholar]
- UNCTAD. Least Developed Countries. Available online: https://unctad.org/topic/least-developed-countries (accessed on 25 January 2021).
- Alonso, J.A.; Luiza Cortez, A.; Klasen, S. LDC and Other Country Groupings: How Useful Are Current Approaches to Classify Countries in a More Heterogeneous Developing World? UN Department of Economic and Social Affairs: New York, NY, USA, 2014. [Google Scholar]
- UNCTAD. The Least Developed Countries Report 2020 Productive Capacities for the New Decade; United Nations Publications: New York, NY, USA, 2020; ISBN 978-921-112-998-4. [Google Scholar]
- UNPD. World Population Prospects–Population Division–United Nations. Available online: https://population.un.org/wpp (accessed on 25 January 2021).
- United Nations; IOM. Climate Change and Migration in Vulnerable Countries a Snapshot of Least Developed Countries, Landlocked Developing Countries and Small Island Developing States; International Organization for Migration: Geneva, Switzerland, 2019. [Google Scholar]
- UNCF. Levels and Trends in Child Mortality; United Nations Children’s Fund: New York, NY, USA, 2019. [Google Scholar]
- Buka, I.; Brennan, L.; Tarrabain, J.; Aghazadeh, S.; Drisse, M.N.B. Need for global core competencies in Child Health and the Environment: A Canadian perspective. J. Epidemiol. Community Health 2020. [Google Scholar] [CrossRef]
- English, K.; Lau, C.; Jagals, P. The Unique Vulnerabilities of Children to Environmental Hazards BT–Early-Life Environmental Exposure and Disease: Facts and Perspectives; Xia, Y., Ed.; Springer: Singapore, 2020; pp. 103–112. ISBN 978-981-15-3797-4. [Google Scholar]
- Gluckman, P.D.; Hanson, M.A.; Spencer, H.G.; Bateson, P. Environmental influences during development and their later consequences for health and disease: Implications for the interpretation of empirical studies. Proc. R. Soc. B Biol. Sci. 2005, 272, 671–677. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of In Utero and Early-Life Conditions on Adult Health and Disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef]
- Sly, J.L.; Carpenter, D.O. Special vulnerability of children to environmental exposures. Rev. Environ. Health 2012, 27, 151–157. [Google Scholar] [CrossRef]
- Risk, O.; Tun, H.; Manikam, L.; Lakhanpaul, M. Early Life Social and Economic Adversities on Health–Early-Life Environmental Exposure and Disease: Facts and Perspectives; Xia, Y., Ed.; Springer: Singapore, 2020; pp. 181–194. ISBN 978-981-15-3797-4. [Google Scholar]
- Landrigan, P.J.; Etzel, R.A. Textbook of Children’s Environmental Health; Oxford University Press: Oxford, UK, 2014; ISBN 9780199929573. [Google Scholar]
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- United Nations Environment Programme. Healthy Environment, Healthy People; UNEP: Nairobi, Kenya, 2016. [Google Scholar]
- Sterman, J. System dynamics at sixty: The path forward. Syst. Dyn. Rev. 2018, 34, 5–47. [Google Scholar] [CrossRef]
- Darabi, N.; Hosseinichimeh, N. System Dynamics Modeling in Health and Medicine: A Systematic Literature Review. Syst. Dyn. Rev. 2020, 36, 29–73. [Google Scholar] [CrossRef]
- Maani, K.; Cavana, R.Y. Systems Thinking, System Dynamics: Managing Change and Complexity, 2nd ed.; Prentice Hall: Auckland, NZ, USA, 2007. [Google Scholar]
- Rosenthal, J.; Arku, R.E.; Baumgartner, J.; Brown, J.; Clasen, T.; Eisenberg, J.N.S.; Hovmand, P.; Jagger, P.; Luke, D.A.; Quinn, A.; et al. Systems Science Approaches for Global Environmental Health Research: Enhancing Intervention Design and Implementation for Household Air Pollution (HAP) and Water, Sanitation, and Hygiene (WASH) Programs. Environ. Health Perspect. 2020, 128, 105001. [Google Scholar] [CrossRef] [PubMed]
- Currie, D.J.; Smith, C.; Jagals, P. The application of system dynamics modelling to environmental health decision-making and policy—A scoping review. BMC Public Health 2018, 18, 402. [Google Scholar] [CrossRef]
- Luke, D.A.; Stamatakis, K.A. Systems Science Methods in Public Health: Dynamics, Networks, and Agents. Annu. Rev. Public Health 2012, 33, 357–376. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.W.; de Rosa, C.; Howze, E.H.; Baldwin, G.T. Understanding Wicked Problems: A Key to Advancing Environmental Health Promotion. Health Educ. Behav. 2004, 31, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Garrity, E. Using Systems Thinking to Understand and Enlarge Mental Models: Helping the Transition to a Sustainable World. Systems 2018, 6, 15. [Google Scholar] [CrossRef]
- Sterman, J.D. Business Dynamics: Systems Thinking and Modeling for a Complex World; Irwin/McGraw-Hill: Boston, MA, USA, 2000; ISBN 0072311355. [Google Scholar]
- UN. The Future We Want. A/RES/66/288. 2012. Available online: undocs.org/en/A/RES/67/97 (accessed on 25 January 2021).
- Purvis, B.; Mao, Y.; Robinson, D. Three pillars of sustainability: In search of conceptual origins. Sustain. Sci. 2019, 14, 681–695. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network Global Burden of Disease Study 2019 Results. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 25 January 2021).
- Werner, A.K.; Vink, S.; Watt, K.; Jagals, P. Environmental health impacts of unconventional natural gas development: A review of the current strength of evidence. Sci. Total Environ. 2015, 505, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- UN. Global Indicator Framework for the Sustainable Development Goals and Targets of the 2030 Agenda for Sustainable Development. A/RES/71/313. 2017. Available online: undocs.org/en/A/RES/71/313 (accessed on 25 January 2021).
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Balde, A.B.; Bertollini, R.; O’Reilly, S.B.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Pullan, R.L.; Smith, J.L.; Jasrasaria, R.; Brooker, S.J. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit. Vectors 2014, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.; Kamath, A. Neglected tropical diseases in sub-Saharan Africa: Review of their prevalence, distribution, and disease burden. PLoS Negl. Trop. Dis. 2009, 3, e412. [Google Scholar] [CrossRef]
- Kline, K.; McCarthy, J.S.; Pearson, M.; Loukas, A.; Hotez, P.J. Neglected tropical diseases of Oceania: Review of their prevalence, distribution, and opportunities for control. PLoS Negl. Trop. Dis. 2013, 7, e1755. [Google Scholar] [CrossRef] [PubMed]
- Karimkhani, C.; Colombara, D.V.; Drucker, A.M.; Norton, S.A.; Hay, R.; Engelman, D.; Steer, A.; Whitfeld, M.; Naghavi, M.; Dellavalle, R.P. The global burden of scabies: A cross-sectional analysis from the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1247–1254. [Google Scholar] [CrossRef]
- Romani, L.; Whitfeld, M.J.; Koroivueta, J.; Kama, M.; Wand, H.; Tikoduadua, L.; Tuicakau, M.; Koroi, A.; Ritova, R.; Andrews, R.; et al. The Epidemiology of Scabies and Impetigo in Relation to Demographic and Residential Characteristics: Baseline Findings from the Skin Health Intervention Fiji Trial. Am. J. Trop. Med. Hyg. 2017, 97, 845–850. [Google Scholar] [CrossRef]
- Mills, J.E.; Cumming, O. The Impact of Water, Sanitation and Hygiene on Key Health and Social Outcomes: Review of Evidence, Sanitation and Hygiene Applied Research for Equity; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M.; Curtis, V.; de France, J.; et al. Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014. [Google Scholar] [CrossRef]
- Ziegelbauer, K.; Speich, B.; Mäusezahl, D.; Bos, R.; Keiser, J.; Utzinger, J. Effect of sanitation on soil-transmitted helminth infection: Systematic review and meta-analysis. PLoS Med. 2012, 9, e1001162. [Google Scholar] [CrossRef]
- Groome, M.J.; Parashar, U.D. Understanding the full clinical spectrum of childhood diarrhoea in low-income and middle-income countries. Lancet Glob. Health 2019, 7, e534–e535. [Google Scholar] [CrossRef]
- Eckhardt, C. Micronutrient Malnutrition, Obesity, and Chronic Disease in Countries Undergoing the Nutrition Transition: Potential Links and Program/Policy Implications; IFPRI: Washington DC, USA, 2006. [Google Scholar]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Babatola, S.S. Global burden of diseases attributable to air pollution. J. Public Health Afr. 2018, 9, 813. [Google Scholar] [CrossRef] [PubMed]
- Tong, S. Air pollution and disease burden. Lancet Planet. Health 2019, 3, e49–e50. [Google Scholar] [CrossRef]
- Mengersen, K.; Morawska, L.; Wang, H.; Murphy, N.; Tayphasavanh, F.; Darasavong, K.; Holmes, N. The effect of housing characteristics and occupant activities on the respiratory health of women and children in Lao PDR. Sci. Total Environ. 2011, 409, 1378–1384. [Google Scholar] [CrossRef]
- Wardlaw, T.; Johansson, E.; Hodge, M. Pneumonia, the Forgotten Killer of Children; WHO/UNICEF: Geneva, Switzerland, 2006; p. 40. [Google Scholar]
- WHO. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Hosangadi, D. The Global Rise of Dengue Infections; John Hopkins Center for Health Security: Baltimore, MD, USA, 2019; Available online: https://www.outbreakobservatory.org/outbreakthursday-1/3/21/2019/the-global-rise-of-dengue-infections.2019 (accessed on 25 January 2021).
- Kassebaum, N.; Kyu, H.H.; Zoeckler, L.; Olsen, H.E.; Thomas, K.; Pinho, C.; Bhutta, Z.A.; Dandona, L.; Ferrari, A.; Ghiwot, T.T.; et al. Child and adolescent health from 1990 to 2015: Findings from the global burden of diseases, injuries, and risk factors 2015 study. JAMA Pediatr. 2017, 171, 573–592. [Google Scholar]
- Landrigan, P.J.; Sly, J.L.; Ruchirawat, M.; Silva, E.R.; Huo, X.; Diaz-Barriga, F.; Zar, H.J.; King, M.; Ha, E.H.; Asante, K.A.; et al. Health Consequences of Environmental Exposures: Changing Global Patterns of Exposure and Disease. Ann. Glob. Health 2016, 82, 10–19. [Google Scholar] [CrossRef]
- Lilford, R.J.; Oyebode, O.; Satterthwaite, D.; Melendez-Torres, G.J.; Chen, Y.-F.; Mberu, B.; Watson, S.I.; Sartori, J.; Ndugwa, R.; Caiaffa, W.; et al. Improving the health and welfare of people who live in slums. Lancet 2016, 389, 559–570. [Google Scholar] [CrossRef]
- Risnes, K.R.; Vatten, L.J.; Baker, J.L.; Jameson, K.; Sovio, U.; Kajantie, E.; Osler, M.; Morley, R.; Jokela, M.; Painter, R.C.; et al. Birthweight and mortality in adulthood: A systematic review and meta-analysis. Int. J. Epidemiol. 2011, 40, 647–661. [Google Scholar] [CrossRef]
- WorldBank. World Development Indicators (WDI)|Data Catalog. Available online: https://datacatalog.worldbank.org/dataset/world-development-indicators (accessed on 25 January 2021).
- Mcgovern, M.E.; Krishna, A.; Aguayo, V.M.; Subramanian, S.V. A review of the evidence linking child stunting to economic outcomes. Int. J. Epidemiol. 2017, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Johnson Rucker, C.; Schoeni Robert, F.; Johnson, R.; Schoeni, R. The Influence of Early-Life Events on Human Capital, Health Status, and Labor Market Outcomes over the Life Course. BE J. Econ. Anal Policy 2011, 11, 2521. [Google Scholar] [CrossRef] [PubMed]
- UN. LDC Identification Criteria & Indicators|Department of Economic and Social Affairs. Available online: https://www.un.org/development/desa/dpad/least-developed-country-category/ldc-criteria.html (accessed on 25 January 2021).
- WHO; UNICEF. Drinking Water Services JMP Ladder. Available online: https://washdata.org/monitoring/drinking-water (accessed on 25 January 2021).
- WorldBank. World Bank DataBank–Sustainable Development Goals (SDGs). 2018. Available online: http://databank.worldbank.org/data/reports.aspx?source=sustainable-development-goals-(sdgs) (accessed on 25 January 2021).
- WHO; UNICEF. SanitationJMP Ladder. Available online: https://washdata.org/monitoring/sanitation (accessed on 25 January 2021).
- Bueno-Marí, R.; Jiménez-Peydró, R. Global change and human vulnerability to vector-borne diseases. Front. Physiol. 2013, 4, 158. [Google Scholar] [CrossRef] [PubMed]
- WHO. Entomology and Vector Control. Available online: https://www.who.int/malaria/areas/vector_control/en/ (accessed on 25 January 2021).
- Muyanja, D.; Allen, J.G.; Vallarino, J.; Valeri, L.; Kakuhikire, B.; Bangsberg, D.R.; Christiani, D.C.; Tsai, A.C.; Lai, P.S. Kerosene lighting contributes to household air pollution in rural Uganda. Indoor Air 2017, 27, 1022–1029. [Google Scholar] [CrossRef]
- WHO. Burden of disease from Ambient Air Pollution for 2012; WHO: Geneva, Switzerland, 2014; pp. 2012–2014. [Google Scholar] [CrossRef]
- Tvedten, I.; Candiracci, S. “Flooding our eyes with rubbish”: Urban waste management in Maputo, Mozambique. Environ. Urban. 2018, 30, 631–646. [Google Scholar] [CrossRef]
- Aswani, S.; Vaccaro, I.; Abernethy, K.; Albert, S.; de Pablo, J.F. Can Perceptions of Environmental and Climate Change in Island Communities Assist in Adaptation Planning Locally? Environ. Manag. 2015, 56, 1487–1501. [Google Scholar] [CrossRef]
- Wenger, A.S.; Atkinson, S.; Santini, T.; Falinski, K.; Hutley, N.; Albert, S.; Horning, N.; Watson, J.E.M.; Mumby, P.J.; Jupiter, S.D. Predicting the impact of logging activities on soil erosion and water quality in steep, forested tropical islands. Environ. Res. Lett. 2018, 13, 44035. [Google Scholar] [CrossRef]
- Kuruppu, N.; Willie, R. Barriers to reducing climate enhanced disaster risks in least developed country-small islands through anticipatory adaptation. Weather Clim. Extrem. 2015, 7, 72–83. [Google Scholar] [CrossRef]
- Diwakar, V.; Lovell, E.; Opitz-Stapleton, S.; Shepherd, A.; Twigg, J. Child Poverty, Disasters and Climate Change Investigating Relationships and Implications Over the Life Course of Children. ODI. 2019. Available online: https://www.odi.org/publications/11281-child-poverty-disasters-and-climate-change-investigating-relationships-and-implications-over-life (accessed on 25 January 2021).
- Barnett, E.; Casper, M. A Definition of “Social Environment”. AmJPH 2001, 91, 465. [Google Scholar]
- Victora, C.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef]
- Leipziger, D.; Fay, M.; Wodon, Q.; Yepes, T. Achieving the Millennium Development Goals: The Role of Infrastructure; Policy Research Working Papers. World Bank eLibrary. Available online: https://elibrary.worldbank.org/doi/abs/10.1596/1813-9450-3163 (accessed on 25 January 2021).
- Munroe, R.L.; Gauvain, M. Exposure to open-fire cooking and cognitive performance in children. Int. J. Environ. Health Res. 2012, 22, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Nguyen, M. Shedding light on maternal education and child health in developing countries. World Dev. 2020, 133, 105005. [Google Scholar] [CrossRef]
- Ajao, K.O.; Ojofeitimi, E.O.; Adebayo, A.A.; Fatusi, A.O.; Afolabi, O.T. Influence of family size, household food security status, and child care practices on the nutritional status of under-five children in Ile-Ife, Nigeria. Afr. J. Reprod. Health 2010, 14, 117–126. [Google Scholar]
- Rana, M.J.; Goli, S. Tracing long-term trajectories of contraceptive practice across 185 countries. PLoS ONE 2018, 13, e0205927. [Google Scholar] [CrossRef]
- Vollset, S.E.; Goren, E.; Yuan, C.-W.; Cao, J.; Smith, A.E.; Hsiao, T.; Bisignano, C.; Azhar, G.S.; Castro, E.; Chalek, J.; et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: A forecasting analysis for the Global Burden of Disease Study. Lancet 2020. [Google Scholar] [CrossRef]
- Graham, J.P.; Kaur, M.; Jeuland, M.A. Access to environmental health assets across wealth strata: Evidence from 41 low- and middle-income countries. PLoS ONE 2018, 13, e0207339. [Google Scholar] [CrossRef] [PubMed]
- Markandya, A.; Wilkinson, P. Electricity generation and health. Lancet 2007, 370, 979–990. [Google Scholar] [CrossRef]
- Pérez-Moreno, S.; Blanco-Arana, M.C.; Bárcena-Martín, E. Economic cycles and child mortality: A cross-national study of the least developed countries. Econ. Hum. Biol. 2016, 22, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Padmadas, S.; Falkingham, J. Is Rapid Urbanisation Exacerbating Wealth-Related Urban Inequalities in Child Nutritional Status? Evidence from Least Developed Countries. Eur. J. Dev. Res. 2018, 30, 630–651. [Google Scholar] [CrossRef]
- Chatterjee, P. Tackling social determinants to reduce child malnutrition. Lancet Child Adolesc. Health 2019, 3, 140–141. [Google Scholar] [CrossRef]
- Warner, K.; Hamza, M.; Oliver-Smith, A.; Renaud, F.; Julca, A. Climate change, environmental degradation and migration. Nat. Hazards 2010, 55, 689–715. [Google Scholar] [CrossRef]
- Chan, H.-Y.; Sopian, K. Renewable Energy in Developing Countries: Local Development and Techno-Economic Aspects; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Austin, K.F.; Mejia, M.T. Household air pollution as a silent killer: Women’s status and solid fuel use in developing nations. Popul. Environ. 2017, 39, 1–25. [Google Scholar] [CrossRef]
- Hoque, A.; Mohiuddin, M.; Su, Z. Effects of Industrial Operations on Socio-Environmental and Public Health Degradation: Evidence from a Least Developing Country (LDC). Sustainability 2018, 10, 3948. [Google Scholar] [CrossRef]
- Burden of Disease IHME Viz Hub. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 25 January 2021).
- Hovmand, P.S. Community Based System Dynamics; Springer: New York, NY, USA, 2014. [Google Scholar]
- Powell, B.J.; Beidas, R.S.; Lewis, C.C.; Aarons, G.A.; McMillen, J.C.; Proctor, E.K.; Mandell, D.S. Methods to Improve the Selection and Tailoring of Implementation Strategies. J. Behav. Health Serv. Res. 2015, 44, 177–194. [Google Scholar] [CrossRef] [PubMed]
- UN. World Mortality 2017: Data Booklet. Available online: https://www.un.org/development/desa/pd/ (accessed on 25 January 2021).







| Child Mortality Disease Group | U15 1 Deaths Rank | U15 Deaths % | U5 2 Deaths Rank | U5 Deaths % | Child Morbidity Disease Group | U15 YLD 3 Rank | U15 YLD % | U5 YLD Rank | U5 YLD % |
|---|---|---|---|---|---|---|---|---|---|
| Neonatal disorders | 1 | 28.7 | 1 | 31.6 | Nutritional | 1 | 26.6 | 1 | 35.0 |
| Enteric disease | 2 | 15.1 | 3 | 14.5 | Skin/subcutaneous diseases | 2 | 9.9 | 4 | 8.4 |
| Respiratory disease | 3 | 14.7 | 2 | 15.2 | Other NCDs | 3 | 9.8 | 2 | 12.0 |
| NTDs 4 and malaria | 4 | 10.2 | 4 | 10.1 | Mental disorders | 4 | 9.6 | 8 | 3.2 |
| Other infectious diseases | 5 | 9.0 | 5 | 8.7 | NTDs and malaria | 5 | 9.0 | 5 | 8.1 |
| Other NCDs | 6 | 8.3 | 6 | 8.6 | Respiratory disease | 6 | 6.7 | 7 | 6.5 |
| HIV/AIDS | 7 | 3.0 | 7 | 2.7 | Neonatal disorders | 7 | 6.3 | 3 | 9.3 |
| Unintentional injuries/transport injuries | 8 | 4.2 | 9 | 2.9 | Neurological disorders | 8 | 5.8 | 9 | 2.9 |
| Nutritional | 9 | 2.4 | 8 | 2.5 | Enteric disease | 9 | 4.3 | 6 | 6.7 |
| Neoplasms | 10 | 1.1 | 10 | 0.7 | Sense organ diseases | 10 | 3.0 | - | - |
| Other infectious diseases | - | - | 10 | 2.8 |
| Variable | Influenced by | +/− | Influences | +/− | Source |
|---|---|---|---|---|---|
| Water, sanitation and hygiene (WASH)-related disease—includes enteric diseases of which diarrhoea is the most prevalent, parasitic NTDs including hookworm and schistosomiasis, all of which have strong causal links with polluted water, open defaecation, and inadequate hygiene. Helminth infections also increase the risk of diarrhoeal disease. Skin diseases, e.g., scabies, yaws are strongly associated with inadequate hygiene measures and overcrowding. | Clean water Open defaecation Hygiene Overcrowding | − + − + | Malnutrition/stunting Child morbidity/mortality | + + | [3,18,34,35,36,37,38,39,40,41,42] |
| Malnutrition/stunting—is the biggest contributor to YLD in LDCs. The effects of a lack of nutritious food are compounded by acute and chronic diarrhoeal disease and helminth infections. A lack of micronutrients in childhood can also predispose to obesity in later life, increasing the risk of NCDs. | Adequate child nutrition WASH-related disease | − + | Child morbidity/mortality Child education | + − + | [3,18,43,44,45] |
| Respiratory disease—is caused by both internal air pollution (IAP) and ambient air pollution (AAP) exposure in LDCs. Rural exposure is primarily through IAP whilst urban/peri-urban exposure is to both IAP 1 and AAP 2. Overcrowding increases transmission of infectious respiratory diseases such as TB. | Internal air pollution (IAP) Ambient air pollution (AAP) Overcrowding | + + + | Child morbidity/mortality | + | [3,18,34,46,47,48,49] |
| Vector-borne disease—such as malaria, which is the fourth largest contributor to child mortality. Dengue fever is a growing threat in urban areas. Other vector-borne diseases include chikungunya fever, Zika virus, Chagas disease, and leishmaniasis. Infection cycles are perpetuated by mosquitos as well as flies, which use faeces in their breeding cycles. | Vectors | + | Child morbidity/mortality | + | [3,4,18,50,51] |
| Childhood injury including traffic injuries—is a risk of unsafe surroundings. Whilst injury is perceived mainly as a problem of an unsafe built environment, remoteness from health resources worsens the prognosis after injury. | Overcrowding Unsafe surroundings | + + | Child morbidity/mortality | + | [52,53,54] |
| Child morbidity/mortality—is increased by inadequate access to health services. In all LDCs, shortages of health personnel, infrastructure, pharmaceutical supplies, and medical equipment are a limitation; in rural and remote areas, these are exacerbated by the need to travel long distances with minimal transport infrastructure. Maternal poor health leads to suboptimal birth outcomes such as fetal growth restriction, low birthweight, and suboptimal breastfeeding. | Disease group mortality/morbidity Health services Maternal health | + − − | Adult morbidity/premature mortality | + | [1,7] |
| Maternal health—Female childhood malnutrition, insufficient nutrition for pregnant women and mothers in some LDCs, large families, and inability to plan and space families all contribute to poor maternal health. | Malnutrition/stunting Family size | − − | Child morbidity/mortality | + | [45,55] |
| Adult morbidity/premature mortality—is a direct result of chronic adult illness with its roots in childhood, reducing lifespan (average 63 in LDCs versus global lifespan of 73) and lifetime economic contribution in LDCs. | Child morbidity | + | Poverty | + | [56,57,58] |
| Neonatal disorders—lead to neonatal deaths and, for survivors, increased mortality risk and morbidity such as stunting, with subsequent adult mortality and morbidity implications. | Maternal health IAP | − + | Child morbidity/premature mortality | + | [18,45,55] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brereton, C.F.; Jagals, P. Applications of Systems Science to Understand and Manage Multiple Influences within Children’s Environmental Health in Least Developed Countries: A Causal Loop Diagram Approach. Int. J. Environ. Res. Public Health 2021, 18, 3010. https://doi.org/10.3390/ijerph18063010
Brereton CF, Jagals P. Applications of Systems Science to Understand and Manage Multiple Influences within Children’s Environmental Health in Least Developed Countries: A Causal Loop Diagram Approach. International Journal of Environmental Research and Public Health. 2021; 18(6):3010. https://doi.org/10.3390/ijerph18063010
Chicago/Turabian StyleBrereton, Claire F., and Paul Jagals. 2021. "Applications of Systems Science to Understand and Manage Multiple Influences within Children’s Environmental Health in Least Developed Countries: A Causal Loop Diagram Approach" International Journal of Environmental Research and Public Health 18, no. 6: 3010. https://doi.org/10.3390/ijerph18063010
APA StyleBrereton, C. F., & Jagals, P. (2021). Applications of Systems Science to Understand and Manage Multiple Influences within Children’s Environmental Health in Least Developed Countries: A Causal Loop Diagram Approach. International Journal of Environmental Research and Public Health, 18(6), 3010. https://doi.org/10.3390/ijerph18063010