
Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019)


Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
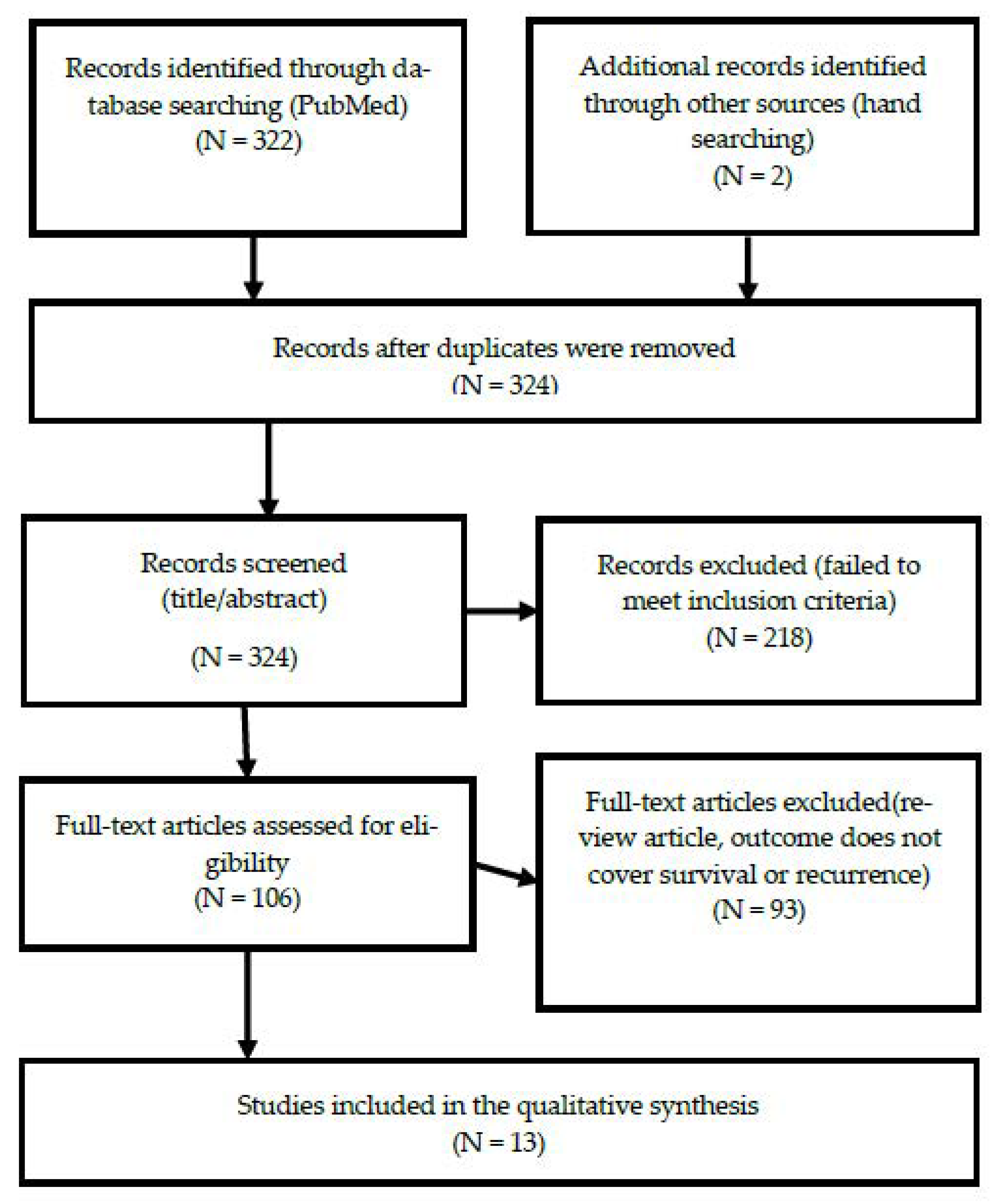
2.2. Searching and Screening
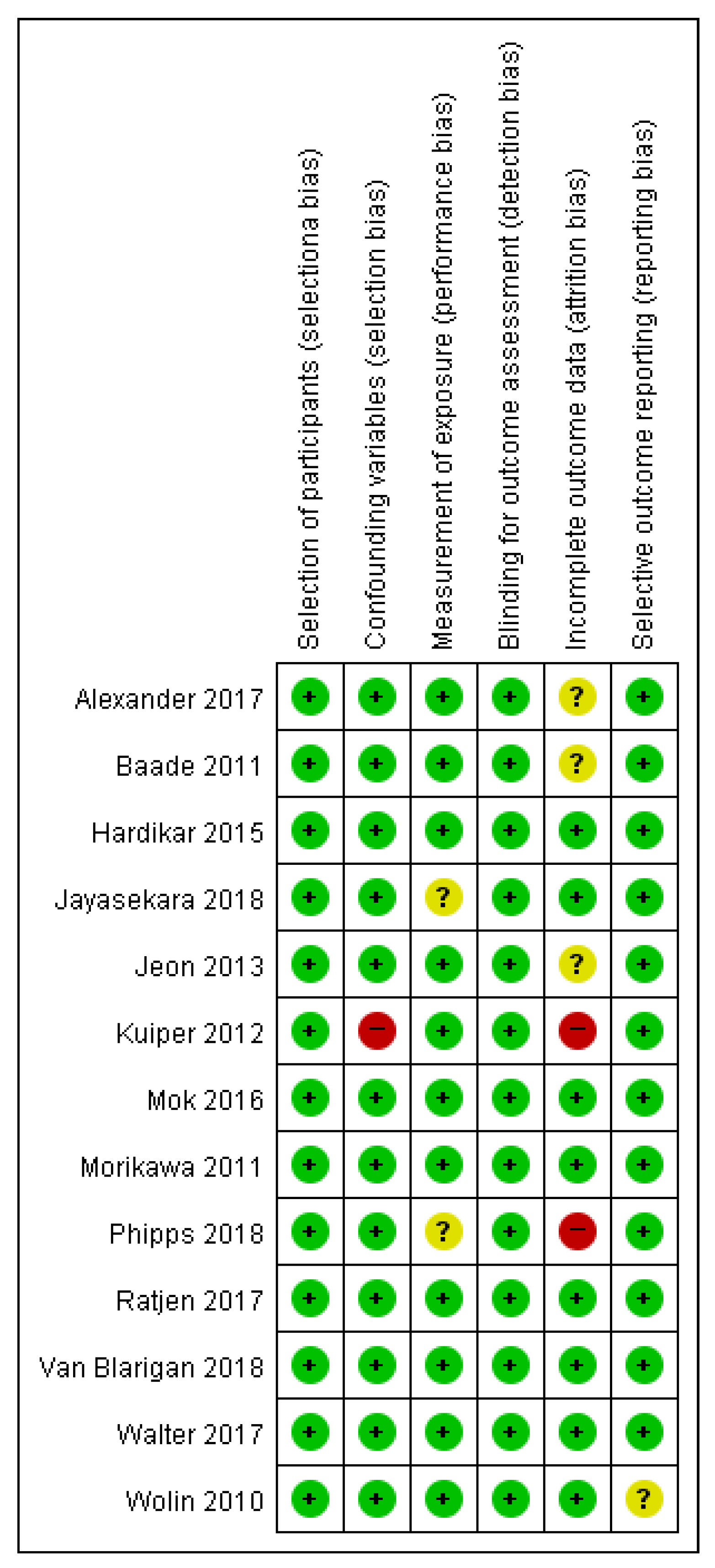
2.3. Assessment of Methodological Quality
2.4. Data Extraction
3. Results
3.1. General Characteristics of the Studies
3.2. Levels of Physical Activity
3.3. The Effect of Levels of Physical Activity on the Prognosis of Colorectal Cancer Patients
3.3.1. Recurrence and Disease-Free Survival
3.3.2. Disease-Specific Mortality
3.3.3. Disease-Specific Survival
3.3.4. Overall Survival
3.3.5. All-Cause Mortality
3.4. Recommended Level of Physical Activity to Improve the Prognosis of Colorectal Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Force, U.S.P.S.T.; Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W., Jr.; Garcia, F.A.R.; Gillman, M.W.; Harper, D.M.; Kemper, A.R.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 2564–2575. [Google Scholar] [CrossRef]
- Joseph, D.A.; King, J.B.; Dowling, N.F.; Thomas, C.C.; Richardson, L.C. Vital Signs: Colorectal Cancer Screening Test Use—United States, 2018. Mmwr. Morb. Mortal. Wkly. Rep. 2020, 69, 253–259. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef]
- Araghi, M.; Soerjomataram, I.; Jenkins, M.; Brierley, J.; Morris, E.; Bray, F.; Arnold, M. Global trends in colorectal cancer mortality: Projections to the year 2035. Int. J. Cancer 2019, 144, 2992–3000. [Google Scholar] [CrossRef] [PubMed]
- Ratjen, I.; Schafmayer, C.; di Giuseppe, R.; Waniek, S.; Plachta-Danielzik, S.; Koch, M.; Burmeister, G.; Nothlings, U.; Hampe, J.; Schlesinger, S.; et al. Postdiagnostic physical activity, sleep duration, and TV watching and all-cause mortality among long-term colorectal cancer survivors: A prospective cohort study. BMC Cancer 2017, 17, 701. [Google Scholar] [CrossRef] [PubMed]
- Eaglehouse, Y.L.; Koh, W.-P.; Wang, R.; Aizhen, J.; Yuan, J.-M.; Butler, L.M. Physical activity, sedentary time, and risk of colorectal cancer: The Singapore Chinese Health Study. Eur. J. Cancer Prev. 2017, 26, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. In US Department of Health and Human Services. 2008. Available online: https://health.gov/sites/default/files/2019-09/paguide.pdf (accessed on 1 December 2020).
- Petersen, K.E.N.; Johnsen, N.F.; Olsen, A.; Albieri, V.; Olsen, L.K.H.; Dragsted, L.O.; Overvad, K.; Tjonneland, A.; Egeberg, R. The combined impact of adherence to five lifestyle factors on all-cause, cancer and cardiovascular mortality: A prospective cohort study among Danish men and women. Br. J. Nutr. 2015, 113, 849–858. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef]
- Mok, Y.; Jeon, C.; Lee, G.J.; Jee, S.H. Physical Activity Level and Colorectal Cancer Mortality. Asia Pac. J. Public Health 2016, 28, 638–647. [Google Scholar] [CrossRef]
- Kuiper, J.G.; Phipps, A.I.; Neuhouser, M.L.; Chlebowski, R.T.; Thomson, C.A.; Irwin, M.L.; Lane, D.S.; Wactawski-Wende, J.; Hou, L.; Jackson, R.D.; et al. Recreational physical activity, body mass index, and survival in women with colorectal cancer. Cancer Causes Control. 2012, 23, 1939–1948. [Google Scholar] [CrossRef] [PubMed]
- Walter, V.; Jansen, L.; Knebel, P.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Physical activity and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2017, 140, 1985–1997. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; Berrington de Gonzalez, A.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Santos, T.; Martins, J.; Matos, M.G.D.; Valeiro, M.G. The association between physical activity and chronic diseases in European adults. Eur. J. Sport Sci. 2018, 18, 140–149. [Google Scholar] [CrossRef]
- Hardikar, S.; Newcomb, P.A.; Campbell, P.T.; Win, A.K.; Lindor, N.M.; Buchanan, D.D.; Makar, K.W.; Jenkins, M.A.; Potter, J.D.; Phipps, A.I. Prediagnostic physical activity and colorectal cancer survival: Overall and stratified by tumor characteristics. Cancer Epidemiol. Biomark Prev. 2015, 24, 1130–1137. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Park, J.; Kim, J.H.; Lee, H.J.; Park, S.J.; Hong, S.P.; Cheon, J.H.; Kim, W.H.; Park, J.S.; Jeon, J.Y.; Kim, T.I. The Effects of Physical Activity and Body Fat Mass on Colorectal Polyp Recurrence in Patients with Previous Colorectal Cancer. Cancer Prev. Res. 2017, 10, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef]
- Park, J.; Lee, Y.; Seo, H.; Jang, B.; Son, H.; Kim, S.; Shin, S.; Hahn, S. Risk of bias assessment tool for non-randomized studies (RoBANS): Development and validation of a new instrument. In Proceedings of the 19th Cochrane Colloquium, Madrid, Spain, 19–22 October 2011; pp. 19–22. [Google Scholar]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.; Allardice, G.M.; Moug, S.J.; Morrison, D.S. A retrospective cohort study of the influence of lifestyle factors on the survival of patients undergoing surgery for colorectal cancer. Colorectal. Dis. 2017, 19, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Patel, A.V.; Campbell, P.T.; Jacobs, E.J.; McCullough, M.L.; Colditz, G.A.; Gapstur, S.M. Change in physical activity and colon cancer incidence and mortality. Cancer Epidemiol. Biomark Prev. 2010, 19, 3000–3004. [Google Scholar] [CrossRef]
- Baade, P.D.; Meng, X.; Youl, P.H.; Aitken, J.F.; Dunn, J.; Chambers, S.K. The impact of body mass index and physical activity on mortality among patients with colorectal cancer in Queensland, Australia. Cancer Epidemiol. Biomark Prev. 2011, 20, 1410–1420. [Google Scholar] [CrossRef]
- Morikawa, T.; Kuchiba, A.; Yamauchi, M.; Meyerhardt, J.A.; Shima, K.; Nosho, K.; Chan, A.T.; Giovannucci, E.; Fuchs, C.S.; Ogino, S. Association of CTNNB1 (beta-catenin) alterations, body mass index, and physical activity with survival in patients with colorectal cancer. JAMA 2011, 305, 1685–1694. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Sato, K.; Niedzwiecki, D.; Ye, X.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Impact of physical activity after cancer diagnosis on survival in patients with recurrent colon cancer: Findings from CALGB 89803/Alliance. Clin. Colorectal. Cancer 2013, 12, 233–238. [Google Scholar] [CrossRef]
- Jayasekara, H.; English, D.R.; Haydon, A.; Hodge, A.M.; Lynch, B.M.; Rosty, C.; Williamson, E.J.; Clendenning, M.; Southey, M.C.; Jenkins, M.A.; et al. Associations of alcohol intake, smoking, physical activity and obesity with survival following colorectal cancer diagnosis by stage, anatomic site and tumor molecular subtype. Int. J. Cancer 2018, 142, 238–250. [Google Scholar] [CrossRef]
- Van Blarigan, E.L.; Fuchs, C.S.; Niedzwiecki, D.; Zhang, S.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Association of Survival With Adherence to the American Cancer Society Nutrition and Physical Activity Guidelines for Cancer Survivors After Colon Cancer Diagnosis: The CALGB 89803/Alliance Trial. JAMA Oncol. 2018, 4, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Phipps, A.I.; Shi, Q.; Zemla, T.J.; Dotan, E.; Gill, S.; Goldberg, R.M.; Hardikar, S.; Jahagirdar, B.; Limburg, P.J.; Newcomb, P.A.; et al. Physical Activity and Outcomes in Patients with Stage III Colon Cancer: A Correlative Analysis of Phase III Trial NCCTG N0147 (Alliance). Cancer Epidemiol. Biomark Prev. 2018, 27, 696–703. [Google Scholar] [CrossRef]
- De Rezende, L.F.; Rabacow, F.M.; Viscondi, J.Y.; Luiz Odo, C.; Matsudo, V.K.; Lee, I.M. Effect of physical inactivity on major noncommunicable diseases and life expectancy in Brazil. J. Phys. Act. Health 2015, 12, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Oruc, Z.; Kaplan, M.A. Effect of exercise on colorectal cancer prevention and treatment. World J. Gastrointest Oncol. 2019, 11, 348–366. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.P.; Awasthi, R.; Sweet, S.N.; Minnella, E.M.; Bergdahl, A.; Santa Mina, D.; Carli, F.; Scheede-Bergdahl, C. Four-week prehabilitation program is sufficient to modify exercise behaviors and improve preoperative functional walking capacity in patients with colorectal cancer. Support. Care Cancer 2017, 25, 33–40. [Google Scholar] [CrossRef]
- Young, J.; Badgery-Parker, T.; Dobbins, T.; Jorgensen, M.; Gibbs, P.; Faragher, I.; Jones, I.; Currow, D. Comparison of ECOG/WHO performance status and ASA score as a measure of functional status. J. Pain Symptom Manag. 2015, 49, 258–264. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Robert-McComb, J.J.; Carnero, E.Á.; Iglesias-Gutiérrez, E. Estimating Energy Requirements. Active Female 2014, 411–449. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Rogers, L.Q.; Alfano, C.M.; Thomson, C.A.; Courneya, K.S.; Meyerhardt, J.A.; Stout, N.L.; Kvale, E.; Ganzer, H.; Ligibel, J.A. Practical clinical interventions for diet, physical activity, and weight control in cancer survivors. Ca Cancer J. Clin. 2015, 65, 167–189. [Google Scholar] [CrossRef]
- Craft, L.L.; Vaniterson, E.H.; Helenowski, I.B.; Rademaker, A.W.; Courneya, K.S. Exercise effects on depressive symptoms in cancer survivors: A systematic review and meta-analysis. Cancer Epidemiol. Biomark Prev. 2012, 21, 3–19. [Google Scholar] [CrossRef]
- Stene, G.B.; Helbostad, J.L.; Balstad, T.R.; Riphagen, I.I.; Kaasa, S.; Oldervoll, L.M. Effect of physical exercise on muscle mass and strength in cancer patients during treatment--a systematic review. Crit. Rev. Oncol. Hematol. 2013, 88, 573–593. [Google Scholar] [CrossRef] [PubMed]
- Hojman, P.; Gehl, J.; Christensen, J.F.; Pedersen, B.K. Molecular Mechanisms Linking Exercise to Cancer Prevention and Treatment. Cell Metab. 2018, 27, 10–21. [Google Scholar] [CrossRef]
- Ferrer, R.A.; Huedo-Medina, T.B.; Johnson, B.T.; Ryan, S.; Pescatello, L.S. Exercise interventions for cancer survivors: A meta-analysis of quality of life outcomes. Ann. Behav. Med. 2011, 41, 32–47. [Google Scholar] [CrossRef]
- Lynch, B.M.; Cerin, E.; Owen, N.; Hawkes, A.L.; Aitken, J.F. Prospective relationships of physical activity with quality of life among colorectal cancer survivors. J. Clin. Oncol. 2008, 26, 4480–4487. [Google Scholar] [CrossRef] [PubMed]
- Fennell, C.; Barkley, J.E.; Lepp, A. The relationship between cell phone use, physical activity, and sedentary behavior in adults aged 18–80. Comput. Hum. Behav. 2019, 90, 53–59. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Luo, J. Wearable Technology Applications in Healthcare: A Literature Review. Online J. Nurs. Inform. 2019, 23, 8. [Google Scholar]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author (Year) | Purpose, Setting, Design | Data & Characteristics | Variables | Outcomes | Key Findings |
|---|---|---|---|---|---|
| Wolin, K. Y. (2010) | [Purpose] Analyzing the risk of colorectal cancer incidence and mortality according to the level of physical activity among adults [Setting] The United States Population-based [Design] Prospective, cohort study | [Data] CPS II Nutrition Cohort (American Cancer Society) [Duration] Total: 1982–2006 PA: 1982, 1992, 1997 Cancer Dx. and mortality: 1998–2006 [Cohort characteristics] Total: 158,253 Incident CRC: 1863 Death d/t CRC: 846 | [Physical activity] 1982: How much exercise do you get (work or play)? Low (none or slight) High (moderate or heavy) 1992: Cardiovascular exercise Walking, jogging, running, swimming, tennis, cycling, aerobics, dancing → MET < 17.5: low ≥ 17.5: high Increasing (low → high) Decreasing (high → low) | [PA (level)—CRC] - General None vs. 30 ≤ MET → HR: 0.72 (0.58–0.89) [PA (level & change)—DSM] Physical activity low (reference) Maintain high physical activity → HR: 0.81 (0.66–0.99) Decreased physical activity → HR: 0.91 (0.76–1.08) Increased physical activity → HR: 1.03 (0.74–1.45) (age-adjusted) | PA measurement after Dx (+) PA → DSM ↓ (+) PA → ACM ↓ (x) PA-Recur. ↓ (x) Compared to the low physical activity group, only the high physical activity maintenance group reduced their risk of colon cancer death |
| Baade, P. D. (2011) | [Purpose] Analyze the effect of physical activity and body mass index on the mortality rate of colorectal cancer patients [Setting] Queensland, Australia Population-based [Design] Prospective, cohort study | [Duration] Primary CRC patient Enrollment: 2003–2004 f/u: until 2008 (5 min, 12 min after Dx) [Cohort characteristics] Participants: 1825 Included CRC stage: 1, 2, 3 + unknown Excluded CRC stage 0, 4 (1.1%, 6.1%) mortality = 462 (25.3%) Mean dx. age: 67 (21–82) | [Physical activity] - The Active Australia Survey Sum of walking, moderate or vigorous PA time/overall 4 wks - PA level (Australia PA Guidelines) (1) sedentary: 0 min/wk (2) insufficiently active: 1–149 min/wk (3) sufficiently active: 150 ≤ min/wk → Kappa coefficient = 0.62 - PA change (five months, 12 months) (1) no change (2) increase 2 < h/wk (3) increase 2 ≤ h/wk | [PA (level)—ACM] 5 yrs mortality 25–28% ↓ [PA (change)—DSM] PA↑ DSM 32~36% ↓ (1) no change (reference) (2) increase 2 < h/wk [HR: 0.68 (0.48–0.97)] (3) increase 2 ≤ h/wk [HR: 0.64 (0.44–0.93)] [PA(change)—ACM] PA ↑ ASM 31% ↓ (1) sedentary (reference) (2) insufficiently active [HR: 0.72 (0.57–0.91)] (3) sufficiently active [HR: 0.69 (0.50–0.94)] | PA measurement after Dx (+) PA ↑ → DSM ↓ (+) PA ↑ → ACM ↓ (+) PA ↑ → Recur. ↓ (x) |
| Morikawa, T. (2011) | [Purpose] Determine the prognosis according to one’s body mass index (BMI) and post-diagnosis physical activity level in CTNNB1-activated colorectal cancer patients [Setting] The United States [Design] Prospective, cohort study | [Data] (1) The Nurses’ Health Study (since 1976) (2) The Health Professionals Follow-up Study (since 1986) [Duration] Until 30 June 2009 Treatment period: up until one year after diagnosis PA evaluation: one to four years after diagnosis [Cohort characteristics] CRC Stages: 1, 2, 3, 4, and 5 CRC patient: N = 955 | [Physical activity] (1) Aerobic exercises walking (at their usual pace), jogging, running, cycling, swimming laps, playing racket sports (2) Lower-intensity exercise (yoga, toning, stretching) and other vigorous activities → MET scoring Reference: 18 MET h/wk | [PA—DSM] Nuclear CTNNB1 (−), stage (1, 2, 3) → adjusted HR: 0.33 (0.13–0.81) Nuclear CTNNB1 (+) → N/S | PA measurement after Dx (+) PA ↑ → DSM ↓ (+) PA ↑ → ACM ↓ (x) PA↑→ Recur.↓(x) |
| Jeon, J. (2013) | [Purpose] A study on the relationship between physical activity and survival period in patients with recurring colorectal cancer [Setting] The United States [Design] Prospective, cohort study | [Data] National Cancer Institute-sponsored Cancer and Leukemia Group B (CALGB) adjuvant therapy trial for stage III colon cancer [Duration] Enrollment: April 1999–May 2000 Stage 3 CRC pt. with recur. f/u until 9 November 2009. [Cohort characteristics] N = 237 | [Physical activity] Total MET h/wk low: < 3 middle: < 3.0–17.9 high: ≥ 18 | [PA(Level)—ACM] MET ≥ 18 Statistically significant difference (−) but mortality 29% ↓ [HR: 0.71 (0.46–1.11)] PA level ↑ → Mortality ↓ [trend p = 0.052] | PA measurement after Dx (+) → before recur. PA ↑ → DSM ↓ (x) PA ↑ → ACM ↓ (+) PA ↑ → Recur. ↓ (x) Physical activity affects the prognosis of recurrent patients. |
| Mok, Y. (2016) | [Purpose] Checking the correlation of CRC mortality according to the time and intensity of physical activity [Setting] South Korea Population-based [Design] Retrospective, cohort study | [Data] The Korean Metabolic Syndrome Mortality Study (KMSMS) 1994–2004 [Duration] f/u until 2014 [Cohort characteristics] N = 226,089 CRC death = 469 | [Physical activity]—Level MET (MET h/wk) none, < 17.5, ≥ 17.5 - Duration (total h/wk) non, 2, 2–3, 4 - Frequency (frequency/wk): none, 1–3, 4 - Type: Jogging, jumping rope, walking, climbing, calisthenics, swimming, yoga, aerobics, or golf → Exercise * hour * frequency per week → MET h/wk | [PA (level & change)—DSM] - Overall 17.5 MET hours/week CRC mortality [HR: 0.64 (0.45–0.91)] - MEN Regular PA—CRC death [HR: 0.75 (0.58–0.97)] | PA measurement after Dx (+) PA ↑ → DSM ↓ (+) PA ↑ → ACM ↓ (x) PA ↑ → Recur. ↓ (x) Increasing total hours and intensity resulted in a decrease in colon cancer risk, but was not related to women. |
| Alexander, D. (2017) | [Purpose] Analyzing the relationship between modifiable behavioral factors and survival of CRC patients [Setting] The NHS Greater Glasgow and Clyde area, UK [Design] Retrospective, cohort study | [Data] Scottish Cancer Registry, National Scottish Death Records [Duration] Enrollment: 1 January 2012 to 31 December 2012 f/u until: 30 June 2015 [Cohort characteristics] N = 181 Total duration of F/U 480 person-years Mean age: Male = 68.7 (±9.2) Female = 67.0 (±9.9) | [Physical activity] The ability to climb stairs (1) Climbs stairs without stopping (2) Climbs stairs with stopping, cannot climb stairs | [PA−ACM] Able to climb stairs without resting: reference Unable to climb stairs without resting [HR: 3.31 (1.13–9.66)] | PA measurement before Dx (+) PA ↑ → DSM ↓ (x) PA ↑ → ACM ↓ (+) PA↑Recur.↓(x) |
| Ratjen, I. (2017) | [Purpose] Effects of physical activity, sleep, and TV viewing on all causes of death among CRC survivors [Setting] Regional cancer registry, Northern Germany [Design] Prospective, cohort study | [Data] Regional cancer registry (23 hospitals) [Duration] Dx: 1993–2005 F/u start: PA assessment date F/u end: date of death, last vital status assessment [Cohort characteristics] final total N = 1376 All-cause death N = 200 (14.5%) mean f/u = Seven years | [Physical activity] - MET walking: 3.0, cycling: 6.0, sports: 6.0, gardening: 4.0, housework: 3.0, home repair: 4.5, stair climbing: 8.0 × h/wk - Sports, cycling, gardening (MET h/wk) 0, > 0–10, > 10–20, > 20 - Housework, home repair, climbing stairs, walking: 0–10, > 10–20, > 20–30, > 30 - Duration of watching TV ≤ 2, > 2- < 4, ≥ 4 h/day - Total PA Q1 (0–64.5), Q2 (> 64.5–99.7), Q3 (> 99.7–144.9), Q4 (> 144.9) | [PA−ACM] PA Level Q4 (vs. PA Q1) [HR: 0.53(0.36–0.80)] sports > 20 = HR: 0.34 (0.20–0.59) walking > 20 = HR: 0.65 (0.43–1.00) gardening > 20 = HR: 0.62 (0.42–0.91) [Watching TV−ACM] ≤ 2 h/day = reference ≥ 4 h/day = HR: 1.45 (1.02–2.06) | PA measurement after Dx (+) → 6 yr survivors PA → DSM ↓ (x) PA → ACM ↓ (+) PA Recur. ↓ (x) |
| Walter, V. (2017) | [Purpose] To provide evidence for the relevance of physical activity before diagnosis of CRC on the prognosis after diagnosis [Setting] Southwest of Germany Population-based [Design] Prospective, cohort study | [Data] DACHS study (colorectal cancer: chances for prevention through screening)—population-based case-control study 2003~2010 CRC Dx. [Cohort characteristics] Over age 30 CRC Total: N = 3,121 Death: N = 868 CRC specific mortality = 635 Recurr. and meta = 623 mean f/u = 4.8 yrs | [Physical activity] Average physical activity (MET h/wk) Q1: 0.0–25.4 Q2: > 25.4–43.5 Q3: > 4.35–65.4 Q4: > 65.4 Recent physical activity (MET h/wk) Q1: 0.0–13.2 Q2: > 13.2–29.2 Q3: > 29.2–56.2 Q4: > 56.2 adjustment for occupational PA | [Lifetime PA−Survival] Overall Survival (−) CRC specific survival (−) Recurrence free survival (−) Disease-free survival (−) [Latest PA−Survival] PA ↑ Overall Survival ↑ (+) Q2 = HR: 0.81 (0.67–0.97) Q3 = HR: 0.64 (0.58–0.78), Q4 = HR: 0.75 (0.61–0.91) CRC specific survival (+) Q3 = HR: 0.66 (0.52–0.83) Disease-free Survival (+) Q3 = HR: 0.78 (0.65–0.93) | PA measurement after Dx (+) PA ↑ → DSM ↓ (+) PA ↑ → ACM ↓ (+) PA ↑ Recur. ↓ (−) Recent leisure activities have been associated with improved survival in non-metastatic CRC patients. |
| Jayasekara, H. (2018) | [Purpose] A study on the relationship between the lifestyle measured before diagnosis and the survival rate of CRC patients. [Setting] Melbourne, Australia [Design] Prospective, cohort study | [Data] Melbourne Collaborative Cohort Study Enrollment: 41,513 (1990–1994) [Cohort characteristics] Median age = 71 (44–87) CRC patient: N = 724 AJCC Excluding stage 4 | [Physical activity] - Physical activity score 0, 0–3.9, 4–5.9, 6 or more - Exercise Non-exercisers: vigorous and moderate physical activity (never) exercisers: any regular exercise (≥ 1 time per week) - Walking (last 6 mths) for recreation or exercise: Not Walking: never/wk Walking: 1 ↑/wk | [PA−Overall mortality] PA score (−) PA ox (−) Walking (−) [PA(level, exer.)−DSS/DSM] PA score (−) PA ox (−) Walking (−) → subgroup stage II DSM PA ox (+) [HR: 0.25 (0.10–0.60)] | PA measurement before Dx (+) PA ↑ → DSM ↓ (+) in stage 2 only PA ↑ → ACM ↓ (−) PA ↑ → Recur. ↓ (x) |
| Phipps, A. I. (2018) | [Purpose] A study on the relationship between survival and recurrence according to physical activity patterns using clinical trial data of adjuvant chemotherapy for stage III colon cancer [Setting] The United States, multicenter [Design] Prospective, cohort study | [Data] The North Central Cancer Treatment Group (NCCTG; now a part of the Alliance for Clinical Trials in Oncology) Multicenter phase III randomized trial [Duration] DFS: f/u 5 yrs OS: f/u 8 yrs Until 2014.12.3 [Cohort characteristics] Total (stage 3) = 1992 Deaths = 505 Recurrence = 541 | [Physical activity] * During a routine day: almost none/mild activity/moderate/heavy activity * Free time: - Never: about once a month/several times a month/several times a week/daily) - Moderate physical activity: golf, garden management, long walking, bowling - vigorous physical activity: jogging, racket sports, swimming, aerobics | [PA−Overall survival] Any free-time PA (+) PA > once/month (vs. ≤ once) [HR: 0.76 (0.63–0.93)] (vs. none) [HR: 0.73] Moderate-intensity ≥ 2/month (vs. ≤ once) [HR: 0.80 (0.66–0.96)] [PA−Disease-free survival] Any free-time (+) PA > once/month (vs. ≤ once) [HR: 0.82 (0.69–0.99)] (vs. none) [HR: 0.77] → Vigorous-intensity PA (−) | PA measurement after Dx (+) → before Tx PA ↑ → DSM ↓ (+) PA ↑ → ACM ↓ (+) PA ↑ Recur. ↓ (+) The prognostic effect of physical activity was better in non-smokers, T3, folfox monotherapy, and obese groups. |
| Van Blarigan, E. L. (2018) | [Purpose] Confirming whether following ACS guidelines improves the survival rate of colon cancer patients [Setting] The United States [Design] Prospective, cohort study | [Data] CALGB (Cancer and Leukemia Group B) 89803 Enrollment: 1999–2001 within 8 min after surgery. [Cohort characteristics] Enrolment: N = 992 Stage 3 colon cancer Recurrence = 335 Deaths = 299 Recurrence + deaths = 256/335 (86%) | [Physical activity] During and six months after chemotherapy MET: < 8.75; 8.75–17.4; ≥ 17.5 The average value is used after the survey on the 90th and 180th days | [PA−Overall survival] * 8.75–17.4 MET h/wk (vs. < 8.75) [HR: 0.64 (0.45–0.92)] : Median MET = 12.0 * ≥ 17.5 MET-h/wk (vs. < 8.75) [HR: 0.58 (0.42–0.81)]: Median MET = 32.2 | PA measurement after Dx (+) PA ↑ → DSM ↓ (−) PA ↑ → ACM ↓ (+) PA ↑ → Recur. ↓ (−) * Recommendation at least 8.75 MET h/wk 8.75 MET h/wk = moderate activity (brisk walking) 150 min/wk |
| Kuiper, J. G. (2012) | [Purpose] The effect of recreation and physical activity on mortality before and after diagnosis in female CRC patients [Setting] 40 centers in the United States [Design] Prospective, cohort study | [Data] The Women’s Health Initiative study (WHI) October 1993–December 1998 40 centers in the United States [Cohort characteristics] Enrollment = 1339 women | [Physical activity] * MET - Mild (3 MET): slow dancing, bowling, golf - Moderate (4 MET): biking, exercise machines, calisthenics, easy swimming, dancing - Strenuous (7 MET): aerobics, jogging, tennis, swimming laps - MET Level (MET h/wk) 0.0; > 0.0–2.9; 3.0–8.9; 9.0–17.; ≥ 18.0 | [PA−ACM] * Pre-diagnostic PA level ≥ 18.0 MET h/wk (vs. 0.0) [HR: 0.63 (0.42–0.96), p trend = 0.02] * Post-diagnostic PA level ≥ 18.0 MET h/wk (vs. 0.0) [HR: 0.41 (0.21–0.81); p trend = 0.005] [PA−DSM] * Pre-diagnostic PA level → 59% ↓ ≥ 18.0 MET h/wk (vs. 0.0) [HR: 0.68 (0.41–1.13), p trend = 0.08] * Post-diagnostic PA level → 71%↓ ≥ 18.0 MET h/wk (vs. 0.0) [HR: 0.29 (0.11–0.77); p trend = 0.02] | PA measurement before and after Dx (+) PA → DSM ↓ (+) PA → ACM ↓ (+) PA Recur ↓ (x) ≥ 9 MET h/week 32% ↓ DSM 37% ↓ ASM = moderate * 3 h/wk |
| Hardikar, S. (2015) | [Purpose] The effect of physical activity level before diagnosis on survival [Setting] Six study centers Seattle, United States [Design] Prospective, C ohort study | [Data] The population-based Seattle Colon Cancer Family Registry (S-CCFR) [Duration] f/u until December 2012 [Cohort characteristics] CRC pt. = 2706 not metastasis (excluding stage 4) | [Physical activity] - MET (+) MET h/wk < 3.5; 3.5 ≦ 8.75; 8.75 ≦ 17.5; 17.5 ≦ 35; ≧ 35 Cutoff—8.75 MET h/wk Moderate = 2.5 h Vigorous = 75 min | [PA−OS] < 3.5, Reference 3.5 ≦ 8.75, HR: 0.53 (0.39–0.72) 8.75 ≦ 17.5, HR: 0.64 (0.48–0.85) 17.5 ≦ 35, HR: 0.64 (0.47–0.85) ≧ 35, HR: 0.70 (0.52–0.96) [PA−DSS] < 3.5, Reference 3.5 ≦ 8.75, HR: 0.58 (0.39–0.86) 8.75 ≦ 17.5, HR: 0.56 (0.38–0.83) 17.5 ≦ 35, HR: 0.60 (0.40–0.88) ≧ 35, HR: 0.63 (0.42–0.95) | PA measurement before Dx (+) PA → DSM ↓ (+) PA → ACM ↓ (+) PA Recur. ↓ (x) PA beneficial effect - all molecular phenotypes of CRC (+) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.; Park, J. Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019). Int. J. Environ. Res. Public Health 2021, 18, 2896. https://doi.org/10.3390/ijerph18062896
Hong J, Park J. Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019). International Journal of Environmental Research and Public Health. 2021; 18(6):2896. https://doi.org/10.3390/ijerph18062896
Chicago/Turabian StyleHong, Jineui, and Jungmin Park. 2021. "Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019)" International Journal of Environmental Research and Public Health 18, no. 6: 2896. https://doi.org/10.3390/ijerph18062896
APA StyleHong, J., & Park, J. (2021). Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019). International Journal of Environmental Research and Public Health, 18(6), 2896. https://doi.org/10.3390/ijerph18062896