
Promoting Mental Health and Well-Being among Adolescent Young Carers in Europe: A Randomized Controlled Trial Protocol

 ,
,  and
and
Abstract
1. Introduction
2. Original Study Protocol Methods
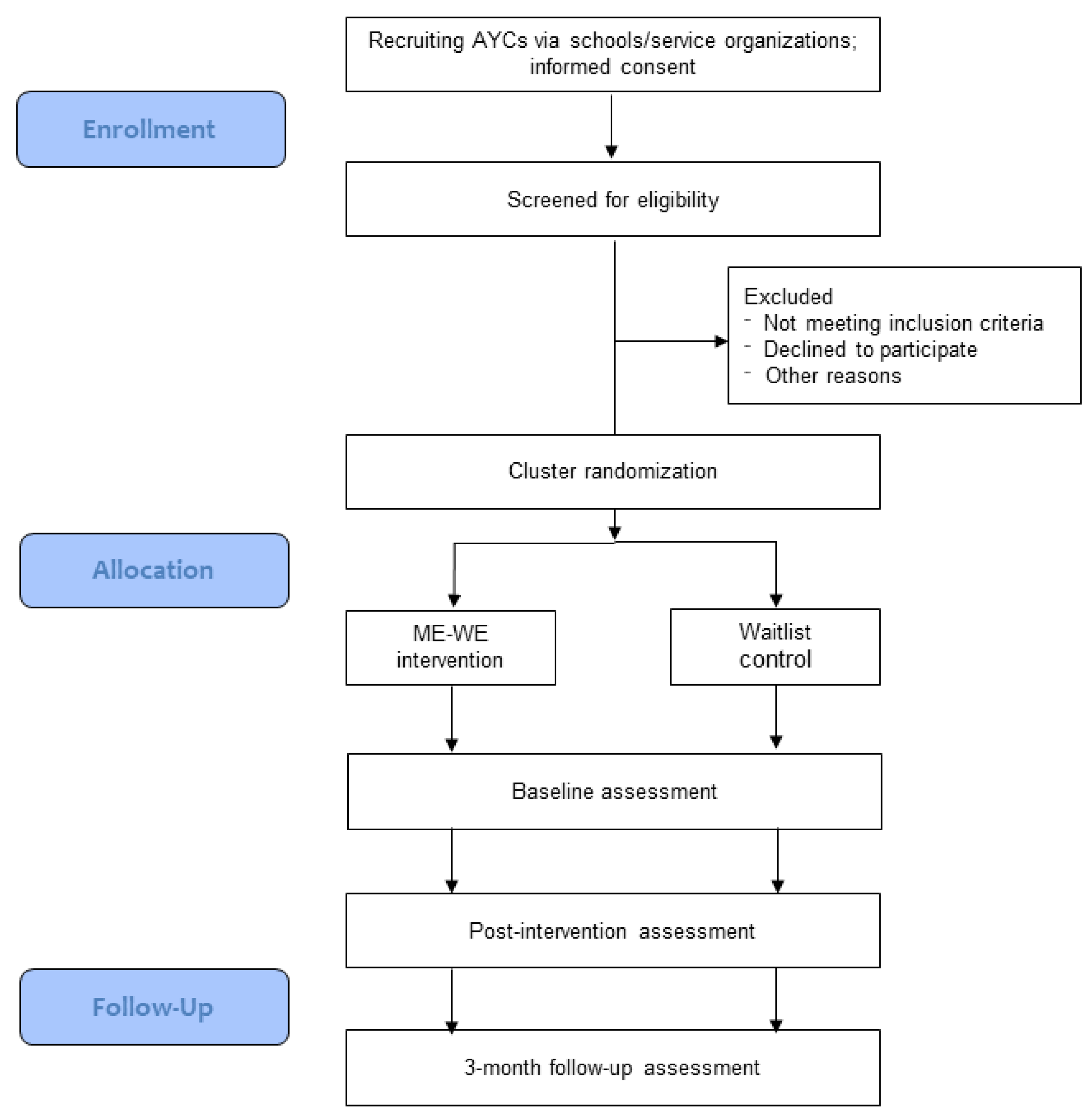
2.1. Study Design
2.2. Participants
2.2.1. Recruitment
2.2.2. Inclusion and Exclusion Criteria
2.3. Intervention
Intervention Fidelity
2.4. Control
2.5. Outcome Measures
2.5.1. Primary Outcomes
2.5.2. Secondary Outcomes
2.5.3. Control Variables
2.5.4. Post-Intervention Self-Assessment
2.5.5. Process Evaluation Outcomes
2.6. Piloting of the ME-WE Intervention and Assessment Questionnaires
2.7. Sample Size Calculation
2.8. Statistical Analyses
2.9. Ethics Approval
3. COVID-19-Related Amendments to Study Protocol Methods
3.1. Study Design Amendments
3.2. Participants
Recruitment Amendments
3.3. Intervention Amendments
3.4. Outcome Measures Amendments
3.4.1. COVID-19-Related Control Variables
3.4.2. Evaluation of Online Delivery of the ME-WE Intervention
3.5. Sample Size Calculation Amendments
3.6. Statistical Analyses Amendments
3.7. Ethics Approval of Amendments
4. Trial Status
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Session | Content |
|---|---|
| Session 1. Getting to know each other and intervention presentation. | Welcome, introduction of facilitators and participants; establishing program engagement and group rules. Introduction to DNA-V model and overview of the intervention; collecting participants’ expectations. Exercises: “DNA-V model description” 1, “Dropping the anchor”. |
| Session 2. The Advisor: dealing with annoying thoughts. | Introduction to the concept of annoying thoughts and the futility of trying to control them; learning to have a different, healthier relationship with these thoughts: letting them go in and out without being trapped in them; learning not to identify oneself with Advisor’s statements; introduction to the concept of mindfulness and first practice. Introduction to the online environment of the ME-WE app. 2 Exercises: “Draw and give a name to your Advisor” 3, “Give the Advisor a microphone” 1, “Normalize the Advisor—The GPS metaphor”1, “Going to extremes” 1, “Balloon breathing” 4. Home activity: “Watching for the Advisor” 1. |
| Session 3. The Noticer: being in connection with our feelings. | Identifying and getting in touch with our emotions, the body and the physical signals that come from the world around us, and understanding the importance of connecting with the present moment; developing understanding about the futility of trying to control unwanted feelings; learning to acknowledge feelings and allow them to be there; introduction to and practice on the AND acronym (Aware, Name, Describe). Exercises: “Rediscovering the wisdom of our feelings”, “Feeling with the body—Practicing AND” 1, “Seaweed goes with the ocean” 1. |
| Session 4. The Discoverer: growing and thriving. | Identifying challenging situations, encouraging the enlargement of the behavioral repertoire to make life bigger, richer, and more vital, or to refocus energy on better listening to what is important and taking committed action towards values; identifying personal strengths. Exercises: “Tracking workability of old behaviors” 1, “Strength spotting card sort” 1, “One moment meditation” 4. Home activity: “Using the Discoverer to discover values” 1. |
| Session 5. Values: connecting to meaning and vitality. | Introduction to values, and recognition of the important role they play on one’s life; learning to be free to listen to values and decide on actions; becoming aware of what is important in life, identifying values and goals, and committing to take action to live in line with them by developing an action plan. Exercises: “What values are” 4, “Values card sort” 1, “My valued journey” 1, “Mindfulness and music” 4. Home activity: “My valued journey”1. |
| Session 6. Developing a flexible self-view and self-compassion. | Developing a flexible self-view by experiencing oneself as a changing, evolving human, and weakening dysfunctional self-concepts; practicing loving-kindness toward oneself and self-compassion by learning to forgive oneself and working on guilt and self-criticism. Exercises: “Strengthening my self-view” 1, “Becoming a friend to yourself” 1, “Compassionate letter” 4, “3 min breathing space”3, “A gentle action”. Home activity: “A gentle action”. |
| Session 7. Building strong social networks. | Identifying what is important in a relationship and especially in a caring one; building strong social networks by becoming aware of people who can support and can be contacted in case of need; developing perspective-taking skills; recognition of the group as a resource. Exercises: “Circles of connection” 1, “Social DNA-V”, “Our group in a ball of yarn”, “My hand”. |
| Session 8. Follow-up. | Reflecting on how participants feel and what has changed in their lives; reviewing what has been experienced and reinforcing skills learned through the intervention; collecting feedback about the intervention. Exercises: “Booster exercise” 1, “The island of the self”. |
References
- Becker, S. Young carers. In The Blackwell Encyclopedia of Social Work, 3rd ed.; Davies, M., Ed.; Blackwell: Oxford, UK, 2000; p. 378. [Google Scholar]
- Metzing-Blau, S.; Schnepp, W. Young carers in Germany: To live on as normal as possible—A grounded theory study. BMC Nurs. 2008, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Leu, A.; Frech, M.; Wepf, H.; Sempik, J.; Joseph, S.; Helbling, L.; Moser, U.; Becker, S.; Jung, C. Counting Young Carers in Switzerland—A Study of Prevalence. Child. Soc. 2019, 33, 53–67. [Google Scholar] [CrossRef]
- Aldridge, J. Where are we now? Twenty-five years of research, policy and practice on young carers. Crit. Soc. Policy 2017, 38, 155–165. [Google Scholar] [CrossRef]
- Brimblecombe, N.; Knapp, M.; King, D.; Stevens, M.; Farias, J.C. The high cost of unpaid care by young people:health and economic impacts of providing unpaid care. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Järkestig-Berggren, U.; Bergman, A.-S.; Eriksson, M.; Priebe, G. Young carers in Sweden—A pilot study of care activities, view of caring, and psychological well-being. Child Fam. Soc. Work. 2018, 24, 292–300. [Google Scholar] [CrossRef]
- Kallander, E.K.; Weimand, B.; Ruud, T.; Becker, S.; Van Roy, B.; Hanssen-Bauer, K. Outcomes for children who care for a parent with a severe illness or substance abuse. Child Youth Serv. 2018, 39, 228–249. [Google Scholar] [CrossRef]
- Nagl-Cupal, M.; Daniel, M.; Koller, M.M.; Mayer, H. Prevalence and effects of caregiving on children. J. Adv. Nurs. 2014, 70, 2314–2325. [Google Scholar] [CrossRef]
- Roling, M.; Falkson, S.; Hellmers, C.; Metzing, S. Early caregiving experiences and the impact on transition into adulthood and further life: A literature review. Scand. J. Caring Sci. 2019, 34, 539–551. [Google Scholar] [CrossRef]
- Cohen, C.; Greene, J.; Toyinbo, P.; Siskowsky, R.N. Impact of family caregiving by youth on their psychological well-being: A latent trait analysis. J. Behav. Health Serv. Res. 2012, 39, 245–256. [Google Scholar] [CrossRef]
- Orel, N.A.; Dupuy, P.; Wright, J. Auxiliary caregivers: The perception of grandchildren within multigenerational caregiving environments. J. Intergener. Relatsh. 2004, 2, 67–92. [Google Scholar] [CrossRef]
- Kim-Cohen, J.; Caspi, A.; Moffitt, T.E.; Harrington, H.; Milne, B.J.; Poulton, R. Prior juvenile diagnoses in adults with mental disorder: Developmental follow-back of a prospective-longitudinal cohort. Arch. Gen. Psychiatry 2003, 60, 709–717. [Google Scholar] [CrossRef]
- Santini, S.; Socci, M.; D’Amen, B.; Di Rosa, M.; Casu, G.; Hlebec, V.; Lewis, F.; Leu, A.; Hoefman, R.; Brolin, R.; et al. Positive and Negative Impacts of Caring among Adolescents Caring for Grandparents. Results from an Online Survey in Six European Countries and Implications for Future Research, Policy and Practice. Int. J. Environ. Res. Public Health 2020, 17, 6593. [Google Scholar] [CrossRef]
- Msc, E.K.K.; Weimand, B.M.; Hanssen-Bauer, K.; Van Roy, B.; Ruud, T.; Hanssen-Bauer, K. Factors associated with quality of life for children affected by parental illness or substance abuse. Scand. J. Caring Sci. 2020. [Google Scholar] [CrossRef]
- Haugland, B.S.M.; Hysing, M.; Sivertsen, B. The Burden of Care: A National Survey on the Prevalence, Demographic Characteristics and Health Problems among Young Adult Carers Attending Higher Education in Norway. Front. Psychol. 2020, 10, 2859. [Google Scholar] [CrossRef]
- Douglas, F.; Ejebu, O.Z.; Garcia, A.; MacKenzie, F.; Whybrow, S.; McKenzie, L.; Ludbrook, A.; Dowler, E. The Nature and Extent of Food Poverty in Scotland; NHS Health Scotland: Glasgow, UK, 2015. [Google Scholar]
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; E Symonds, M.; Miraghajani, M. Food insecurity and mental health: A systematic review and meta-analysis. Public Health Nutr. 2020, 23, 1778–1790. [Google Scholar] [CrossRef]
- Hamilton, M.G.; Adamson, E. Bounded agency in young carers’ life-course stage domains and transitions. J. Youth Stud. 2013, 16, 101–117. [Google Scholar] [CrossRef]
- Hamilton, M.; Cass, B. Capturing the centrality of age and life-course stage in the provision of unpaid care. J. Sociol. 2016, 53, 79–93. [Google Scholar] [CrossRef]
- Lloyd, K. Happiness and Well-Being of Young Carers: Extent, Nature and Correlates of Caring Among 10 and 11 Year Old School Children. J. Happiness Stud. 2013, 14, 67–80. [Google Scholar] [CrossRef]
- Hamilton, M.; Redmond, G. Are Young Carers Less Engaged in School than Non-Carers? Evidence from a Representative Australian Study. Child Indic. Res. 2019, 13, 33–49. [Google Scholar] [CrossRef]
- Kavanaugh, M.S. Children and Adolescents Providing Care to a Parent with Huntington’s Disease: Disease Symptoms, Caregiving Tasks and Young Carer Well-Being. Child Youth Care Forum 2014, 43, 675–690. [Google Scholar] [CrossRef]
- Lakman, Y.; Chalmers, H.; Sexton, C. Young carers’ educational experiences and support: A roadmap for the development of school policies to foster their academic success. Alta. J. Educ. Res. 2017, 63, 63–74. [Google Scholar]
- Bolas, H.; Van Wersch, A.; Flynn, D. The well-being of young people who care for a dependent relative: An interpretative phenomenological analysis. Psychol. Health 2007, 22, 829–850. [Google Scholar] [CrossRef]
- Kaiser, S.; Schulze, G.C. Between Inclusion and Participation: Young Carers Who Are Absent from School. J. Cogn. Educ. Psychol. 2015, 14, 314–328. [Google Scholar] [CrossRef]
- Hall, M.; Sikes, P. ‘It’s just limboland’: Parental dementia and young people’s life courses. Sociol. Rev. 2020, 68, 242–259. [Google Scholar] [CrossRef]
- Gough, G.; Gulliford, A. Resilience amongst young carers: Investigating protective factors and benefit-finding as perceived by young carers. Educ. Psychol. Pr. 2020, 36, 149–169. [Google Scholar] [CrossRef]
- Matzka, M.; Nagl-Cupal, M. Psychosocial resources contributing to resilience in Austrian young carers—A study using photo novella. Res. Nurs. Health 2020, 43, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Becker, F. Service Needs and Delivery Following the Onset of Caring amongst Children and Young Adults: Evidence Based Review; Report; Commission for Rural Communities: Cheltenham, UK, 2008; Available online: http://sro.sussex.ac.uk/id/eprint/77425/ (accessed on 29 January 2021).
- McGibbon, M. The experiences of young carers in Northern Ireland: Negotiating pathways to a positive sense of self-identity—Narratives of resilience, risk and identity. In Narrating Childhood with Children and Young People; Moran, L., Reilly, K., Brady, B., Eds.; Palgrave Macmillan: Cham, Switzerland, 2020; pp. 63–86. [Google Scholar]
- Głąbska, D.; Guzek, D.; Groele, B.; Gutkowska, K. Fruit and vegetables intake in adolescents and mental health: A systematic review. Rocz. Państw. Zakł. Hig. 2020, 71, 15–25. [Google Scholar] [CrossRef]
- Mohanty, I.; Niyonsenga, T. A longitudinal analysis of mental and general health status of informal carers in Australia. BMC Public Health 2019, 19, 1436. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, L.C.; Shochet, I.M.; Smith, C.L.; Wurfl, A. A qualitative evaluation of an innovative resilience-building camp for young carers. Child Fam. Soc. Work 2017, 22, 700–710. [Google Scholar] [CrossRef]
- Acton, J.; Carter, B. The Impact of Immersive Outdoor Activities in Local Woodlands on Young Carers Emotional Literacy and Well-Being. Compr. Child Adolesc. Nurs. 2016, 39, 94–106. [Google Scholar] [CrossRef]
- Assaf, R.R.; Der Springe, J.A.; Siskowski, C.; Ludwig, D.A.; Mathew, M.S.; Belkowitz, J. Participation Rates and Perceptions of Caregiving Youth Providing Home Health Care. J. Community Health 2016, 41, 326–333. [Google Scholar] [CrossRef]
- Gettings, S.; Franco, F.; Santosh, P.J. Facilitating support groups for siblings of children with neurodevelopmental disorders using audio-conferencing: A longitudinal feasibility study. Child Adolesc. Psychiatry Ment. Health 2015, 9, 1–15. [Google Scholar] [CrossRef]
- Schlarmann, J.G.; Metzing, S.; Schoppmann, S.; Schnepp, W. Germany’s First Young Carers Project’s Impact on the Children: Relieving the Entire Family. A Qualitative Evaluation. Open Nurs. J. 2011, 5, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Heyman, A.; Heyman, B. ‘The sooner you can change their life course the better’: The time-framing of risks in relationship to being a young carer. Health Risk Soc. 2013, 15, 561–579. [Google Scholar] [CrossRef]
- Purcal, C.; Hamilton, M.; Thomson, C.; Cass, B. From Assistance to Prevention: Categorizing Young Carer Support Services in Australia, and International Implications. Soc. Policy Adm. 2011, 46, 788–806. [Google Scholar] [CrossRef]
- Stamatopoulos, V. Supporting young carers: A qualitative review of young carer services in Canada. Int. J. Adolesc. Youth 2014, 21, 178–194. [Google Scholar] [CrossRef]
- Fraser, E.; Pakenham, K.I. Evaluation of a Resilience-Based Intervention for Children of Parents with Mental Illness. Aust. N. Zealand J. Psychiatry 2008, 42, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- Dray, J.; Bowman, J.; Campbell, E.; Freund, M.; Wolfenden, L.; Hodder, R.K.; McElwaine, K.; Tremain, D.; Bartlem, K.; Bailey, J.; et al. Systematic Review of Universal Resilience-Focused Interventions Targeting Child and Adolescent Mental Health in the School Setting. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 813–824. [Google Scholar] [CrossRef]
- Merry, S.N.; E Hetrick, S.; Cox, G.R.; Brudevold-Iversen, T.; Bir, J.J.; McDowell, H. Cochrane Review: Psychological and educational interventions for preventing depression in children and adolescents. Evid. Based Child Health A Cochrane Rev. J. 2012, 7, 1409–1685. [Google Scholar] [CrossRef]
- Taylor, R.D.; Oberle, E.; Durlak, J.A.; Weissberg, R.P. Promoting Positive Youth Development Through School-Based Social and Emotional Learning Interventions: A Meta-Analysis of Follow-Up Effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef]
- Manwell, L.A.; Barbic, S.P.; Roberts, K.; Durisko, Z.; Lee, C.; Ware, E.; McKenzie, K. What is mental health? Evidence towards a new definition from a mixed methods multidisciplinary international survey. BMJ Open 2015, 5, e007079. [Google Scholar] [CrossRef]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef]
- Gilmore, K.J.; Meersand, P. Normal Child and Adolescent Development: A Psychodynamic Primer; American Psychiatric Publishing: Washington, DC, USA, 2014; pp. 203–248. [Google Scholar]
- Ogden, T.; Hagen, K.A. Adolescent Mental Health: Prevention and Intervention, 2nd ed.; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Hayes, L.; Ciarrochi, J. The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Positive Connections; New Harbinger Publications: Oakland, CA, USA, 2015. [Google Scholar]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford: New York, NY, USA, 1999. [Google Scholar]
- Ernst, M.M.; Mellon, M.W. Acceptance and commitment therapy (ACT) to foster resilience in pediatric chronic illness. In Child and Adolescent Resilience within Medical Contexts; DeMichelis, C., Ferrari, M., Eds.; Springer: Cham, Switzerland, 2016; pp. 193–207. [Google Scholar]
- Waugh, C.E.; Thompson, R.J.; Gotlib, I.H. Flexible emotional responsiveness in trait resilience. Emotion 2011, 11, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Bjorgvinsdottir, K.; Halldorsdottir, S. Silent, invisible and unacknowledged: Experiences of young caregivers of single parents diagnosed with multiple sclerosis. Scand. J. Caring Sci. 2014, 28, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.; Ding, D. A meta-analysis of the efficacy of acceptance and commitment therapy for children. J. Context. Behav. Sci. 2020, 15, 225–234. [Google Scholar] [CrossRef]
- Halliburton, A.E.; Cooper, L.D. Applications and adaptations of Acceptance and Commitment Therapy (ACT) for adolescents. J. Context. Behav. Sci. 2015, 4, 1–11. [Google Scholar] [CrossRef]
- Kallapiran, K.; Koo, S.; Kirubakaran, R.; Hancock, K. Review: Effectiveness of mindfulness in improving mental health symptoms of children and adolescents: A meta-analysis. Child Adolesc. Ment. Health 2015, 20, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Swain, J.; Hancock, K.; Dixon, A.; Bowman, J. Acceptance and Commitment Therapy for children: A systematic review of intervention studies. J. Context. Behav. Sci. 2015, 4, 73–85. [Google Scholar] [CrossRef]
- Hayes, L.; Boyd, C.P.; Sewell, J. Acceptance and Commitment Therapy for the Treatment of Adolescent Depression: A Pilot Study in a Psychiatric Outpatient Setting. Mindfulness 2011, 2, 86–94. [Google Scholar] [CrossRef]
- Livheim, F.; Hayes, L.; Ghaderi, A.; Magnusdottir, T.; Högfeldt, A.; Rowse, J.; Turner, S.; Hayes, S.C.; Tengström, A. The effectiveness of acceptance and commitment therapy for adolescent mental health: Swedish and Australian pilot outcomes. J. Child Fam. Stud. 2015, 24, 1016–1030. [Google Scholar] [CrossRef]
- Marino, F.; Crimi, I.; Carrozza, C.; Failla, C.; Sfrazzetto, S.T.; Chilà, P.; Bianco, M.; Arnao, A.A.; Tartarisco, G.; Cavallaro, A.; et al. A Novel Third Wave Contextual Approach of Positive Behavior Support in School for Adolescent at High Psychosocial Risk: Rationale, Feasibility, and First Pilot Outcomes. Front. Psychol. 2019, 10, 2635. [Google Scholar] [CrossRef]
- Fayers, P.M.; Jordhùy, M.S.; Kaasa, S. Cluster-randomized trials. Palliat. Med. 2002, 16, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jeriíc, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Hanson, E.; Magnusson, L.; Sennemark, M.E. Blended Learning Networks Supported by Information and Communication Technology: An Intervention for Knowledge Transformation Within Family Care of Older People. Gerontologist 2011, 51, 561–570. [Google Scholar] [CrossRef]
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self-Identity 2003, 2, 85–101. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P.; Carlbring, P.; Riper, H.; Hedman, E. Guided Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: A systematic review and meta-analysis. World Psychiatry 2014, 13, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Carlbring, P.; Andersson, G.; Cuijpers, P.; Riper, H.; Hedman-Lagerlöf, E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn. Behav. Ther. 2018, 47, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Individuals Who Have Basic or Above Basic Overall Digital Skills by Sex. Available online: https://ec.europa.eu/eurostat/databrowser/view/tepsr_sp410/default/table?lang=en (accessed on 4 December 2020).
- Clay, D.; Connors, C.; Day, N.; Gkiza, M.; Aldridge, J. The Lives of Young Carers in England; Qualitative Report to Department for Education; Department for Education: London, UK, 2016. [Google Scholar]
- DNA-V—The Youth Model of Acceptance, Mindfulness, and Positive Psychology. Available online: https://www.praxiscet.com/events/dna-v/ (accessed on 4 December 2020).
- Harkness, J.A.; Schoua-Glusberg, A. Questionnaires in translation. ZUMA-Nachr. Spezial. 1998, 3, 87–127. [Google Scholar]
- Greco, L.A.; Lambert, W.; Baer, R.A. Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychol. Assess. 2008, 20, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, M.; Ristallo, A.; Oppo, A.; Pergolizzi, F.; Presti, G.; Moderato, P. Ragazzi in lotta con emozioni e pensieri: La validazione della versione italiana dellʼAvoidance and Fusion Questionnaire for Youth (I-AFQ-Y). Psicoter. Cogn. Comport. 2017, 23, 141–162. [Google Scholar]
- Muris, P.; Meesters, C.; Herings, A.; Jansen, M.; Vossen, C.; Kersten, P. Inflexible Youngsters: Psychological and Psychopathological Correlates of the Avoidance and Fusion Questionnaire for Youths in Nonclinical Dutch Adolescents. Mindfulness 2017, 8, 1381–1392. [Google Scholar] [CrossRef] [PubMed]
- Cederberg, J.T.; Weineland, S.; Dahl, J.; Ljungman, G. A preliminary validation of the Swedish short version of the Avoidance and Fusion Questionnaire for Youth (AFQ-Y8) for children and adolescents with cancer. J. Context. Behav. Sci. 2018, 10, 103–107. [Google Scholar] [CrossRef]
- Livheim, F.; Tengström, A.; Bond, F.W.; Andersson, G.; Dahl, J.; Rosendahl, I. Psychometric properties of the Avoidance and Fusion Questionnaire for Youth: A psychological measure of psychological inflexibility in youth. J. Contextual Behav. Sci. 2016, 5, 103–110. [Google Scholar] [CrossRef]
- Greco, L.A.; Baer, R.A.; Smith, G.T. Assessing mindfulness in children and adolescents: Development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol. Assess. 2011, 23, 606–614. [Google Scholar] [CrossRef]
- Chiesi, F.; Dellagiulia, A.; Lionetti, F.; Bianchi, G.; Primi, C. Using Item Response Theory to Explore the Psychometric Properties of the Italian Version of the Child and Adolescent Mindfulness Measure (CAMM). Mindfulness 2016, 8, 351–360. [Google Scholar] [CrossRef]
- Ristallo, A.; Schweiger, M.; Oppo, A.; Pergolizzi, F.; Presti, G.; Moderato, P. Misurare la mindfulness in età evolutiva: Proprietà psicometriche e struttura fattoriale della versione italiana della Child and Adolescent Mindfulness Measure (I-CAMM). Psicoter. Cogn. Comport. 2016, 22, 297–315. [Google Scholar]
- Saggino, A.; Bartoccini, A.; Sergi, M.R.; Romanelli, R.; Macchia, A.; Tommasi, M. Assessing Mindfulness on Samples of Italian Children and Adolescents: The Validation of the Italian Version of the Child and Adolescent Mindfulness Measure. Mindfulness 2017, 8, 1364–1372. [Google Scholar] [CrossRef]
- De Bruin, E.I.; Zijlstra, B.J.H.; Bögels, S.M. The Meaning of Mindfulness in Children and Adolescents: Further Validation of the Child and Adolescent Mindfulness Measure (CAMM) in Two Independent Samples from The Netherlands. Mindfulness 2013, 5, 422–430. [Google Scholar] [CrossRef]
- Bluth, K.; Campo, R.A.; Pruteanu-Malinici, S.; Reams, A.; Mullarkey, M.; Broderick, P.C. A School-Based Mindfulness Pilot Study for Ethnically Diverse At-Risk Adolescents. Mindfulness 2016, 7, 90–104. [Google Scholar] [CrossRef]
- O’Dell, S.M.; Hosterman, S.J.; Hostutler, C.A.; Nordberg, C.; Klinger, T.; Petts, R.A.; Whitehead, M.R.; Faulkner, S.A.; Garcia, A.; Massura, C.A. Retrospective cohort study of a novel acceptance and commitment therapy group intervention for adolescents implemented in integrated primary care. J. Context. Behav. Sci. 2020, 16, 109–118. [Google Scholar] [CrossRef]
- Petts, R.A.; Duenas, J.A.; Gaynor, S.T. Acceptance and Commitment Therapy for adolescent depression: Application with a diverse and predominantly socioeconomically disadvantaged sample. J. Context. Behav. Sci. 2017, 6, 134–144. [Google Scholar] [CrossRef]
- Van Der Gucht, K.; Takano, K.; Van Broeck, N.; Raes, F. A Mindfulness-Based Intervention for Economically Disadvantaged People: Effects on Symptoms of Stress, Anxiety, and Depression and on Cognitive Reactivity and Overgeneralization. Mindfulness 2014, 6, 1042–1052. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.M.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, T.; Giles, M.; McLaughlin, M. Benefit finding and resilience in child caregivers. Br. J. Health Psychol. 2013, 19, 606–618. [Google Scholar] [CrossRef]
- Soer, R.; Dijkstra, M.W.M.C.S.; Bieleman, H.J.; Stewart, R.E.; Reneman, M.F.; Oosterveld, F.G.J.; Schreurs, K.M.G. Measurement properties and implications of the Brief Resilience Scale in healthy workers. J. Occup. Health 2019, 61, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Chmitorz, A.; Wenzel, M.; Stieglitz, R.-D.; Kunzler, A.; Bagusat, C.; Helmreich, I.; Gerlicher, A.; Kampa, M.; Kubiak, T.; Kalisch, R.; et al. Population-based validation of a German version of the Brief Resilience Scale. PLoS ONE 2018, 13, e0192761. [Google Scholar] [CrossRef]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Shannon, S.; Breslin, G.; Prentice, G.; Leavey, G. Testing the factor structure of the Warwick-Edinburgh Mental Well-Being Scale in adolescents: A bi-factor modelling methodology. Psychiatry Res. 2020, 293, 113393. [Google Scholar] [CrossRef]
- Gremigni, P.; Stewart-Brown, S. Una misura del benessere mentale: Validazione italiana della Warwick-Edinburgh Mental Well-Being Scale (WEMWBS). G. Ital. Psicol. 2011, 38, 485–508. [Google Scholar]
- Ikink, J.G.; Lamers, S.M.; Bolier, J.M. De Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) als Meetinstrument voor Mentaal Welbevinden in Nederland. Master’s Thesis, Universiteit Twente, Enschede, The Netherlands, 12 November 2012. [Google Scholar]
- Cilar, L.; Pajnkihar, M.; Štiglic, G. Validation of the Warwick-Edinburgh Mental Well-being Scale among nursing students in Slovenia. J. Nurs. Manag. 2020, 28, 1335–1346. [Google Scholar] [CrossRef]
- Haver, A.; Akerjordet, K.; Caputi, P.; Furunes, T.; Magee, C. Measuring mental well-being: A validation of the Short Warwick–Edinburgh Mental Well-Being Scale in Norwegian and Swedish. Scand. J. Public Health 2015, 43, 721–727. [Google Scholar] [CrossRef]
- Lang, G.; Bachinger, A. Validation of the German Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) in a community-based sample of adults in Austria: A bi-factor modelling approach. J. Public Health 2017, 25, 135–146. [Google Scholar] [CrossRef]
- Haugland, S.; Wold, B.; Stevenson, J.; Aaroe, L.E.; Woynarowska, B. Subjective health complaints in adolescence: A cross-national comparison of prevalence and dimensionality. Eur. J. Public Health 2001, 11, 4–10. [Google Scholar] [CrossRef]
- Health Behaviour in School-Aged Children (HBSC). Available online: http://www.hbsc.org/ (accessed on 29 January 2021).
- Gariepy, G.; McKinnon, B.; Sentenac, M.; Elgar, F.J. Validity and Reliability of a Brief Symptom Checklist to Measure Psychological Health in School-Aged Children. Child Indic. Res. 2016, 9, 471–484. [Google Scholar] [CrossRef]
- Haugland, S.; Wold, B. Subjective health complaints in adolescence—Reliability and validity of survey methods. J. Adolesc. 2001, 24, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U. The KIDSCREEN Questionnaires. Quality of Life Questionnaires for Children and Adolescents; Pabst Science Publisher: Lengerich, Germany, 2006. [Google Scholar]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L.; et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: A short measure for children and adolescents’ well-being and health-related quality of life. Qual. Life Res. 2010, 19, 1487–1500. [Google Scholar] [CrossRef] [PubMed]
- Kuhne, F.; Krattenmacher, T.; Bergelt, C.; Ernst, J.C.; Flechtner, H.-H.; Führer, D.; Herzog, W.; Klitzing, K.V.; Romer, G.; Möller, B. Parental palliative cancer: Psychosocial adjustment and health-related quality of life in adolescents participating in a German family counselling service. BMC Palliat. Care 2012, 11, 21. [Google Scholar] [CrossRef]
- KIDSCREEN-10 Index. Available online: https://www.kidscreen.org/english/questionnaires/kidscreen-10-index/ (accessed on 29 January 2021).
- Joseph, S.; Becker, S.; Becker, F.; Regel, S. Assessment of caring and its effects in young people: Development of the Multidimensional Assessment of Caring Activities Checklist (MACA-YC18) and the Positive and Negative Outcomes of Caring Questionnaire (PANOC-YC20) for young carers. Child Care Health Dev. 2009, 35, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Sarason, I.G.; Sarason, B.R.; Shearin, E.N.; Pierce, G.R. A Brief Measure of Social Support: Practical and Theoretical Implications. J. Soc. Pers. Relatsh. 1987, 4, 497–510. [Google Scholar] [CrossRef]
- Nyklíček, I.; Vingerhoets, A. ‘Adaptive’ Psychosocial Factors in Relation to Home Blood Pressure: A Study in the General Population of Southern Netherlands. Int. J. Behav. Med. 2009, 16, 212–218. [Google Scholar] [CrossRef]
- Esposito, C.L.; Clum, G.A. Social support and problem-solving as moderators of the relationship between childhood abuse and suicidality: Applications to a delinquent population. J. Trauma. Stress 2002, 15, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Cox, S. Effects of Benefit Finding, Social Support and Caregiving on Youth Adjustment in a Parental Illness Context. J. Child Fam. Stud. 2018, 27, 2491–2506. [Google Scholar] [CrossRef]
- Joseph, S.; Becker, F.; Becker, S. Manual for Measures of Caring Activities and Outcomes for Children and Young People; The Princess Royal Trust for Carers: London, UK, 2009. [Google Scholar]
- Linnan, L.; Steckler, A. Process Evaluation for Public Health Interventions and Research; Jossey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Swain, J.; Hancock, K.; Hainsworth, C.; Bowman, J. Mechanisms of change: Exploratory outcomes from a randomised controlled trial of acceptance and commitment therapy for anxious adolescents. J. Context. Behav. Sci. 2015, 4, 56–67. [Google Scholar] [CrossRef]
- Daniel, W.W. Biostatistics: A foundation for Analysis in the Health Sciences, 7th ed.; Wiley: New York, NY, USA, 1999. [Google Scholar]
- Italian Institute of Statistics (ISTAT). La Conciliazione tra Lavoro e Famiglia Anno 2010; ISTAT: Rome, Italy, 2011; Available online: https://www.istat.it/it/archivio/48912 (accessed on 4 December 2020).
- Nordenfors, M.; Melander, C.; Daneback, K. Unga Omsorgsgivare i Sverige; Nationellt Kompetenscentrum Anhöriga: Kalmar, Sweden, 2014. [Google Scholar]
- De Roos, S.A.; De Boer, A.H.; Bot, S.M. Well-being and Need for Support of Adolescents with a Chronically Ill Family Member. J. Child Fam. Stud. 2016, 26, 405–415. [Google Scholar] [CrossRef]
- Joseph, S.; Kendall, C.; Toher, D.; Sempik, J.; Holland, J.; Becker, S.; Holland, J. Young carers in England: Findings from the 2018 BBC survey on the prevalence and nature of caring among young people. Child Care Health Dev. 2019, 45, 606–612. [Google Scholar] [CrossRef]
- Leu, A.; Becker, S. A cross-national and comparative classification of in-country awareness and policy responses to ‘young carers’. J. Youth Stud. 2016, 20, 750–762. [Google Scholar] [CrossRef]
- Montori, V.M.; Guyatt, G.H. Intention-to-treat principle. Can. Med Assoc. J. 2001, 165, 1339–1341. [Google Scholar]
- Dreyhaupt, J.; Mayer, B.; Keis, O.; Öchsner, W.; Muche, R. Cluster-randomized Studies in Educational Research: Principles and Methodological Aspects. GMS J. Med Educ. 2017, 34, 34. [Google Scholar]
- Field, A.P.; Wilcox, R.R. Robust statistical methods: A primer for clinical psychology and experimental psychopathology researchers. Behav. Res. Ther. 2017, 98, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Schreier, M. Qualitative content analysis. In The SAGE Handbook of Qualitative Data Analysis; Flick, U., Ed.; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2014; pp. 170–183. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Regulation, G.D.P. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Off. J. Eur. Union 2016, 59, 294. [Google Scholar]
- Beane, J.D.; Dedhia, P.H.; Ejaz, A.; Contreras, C.M.; Cloyd, J.M.; Tsung, A.; Pawlik, T.M. Conducting Clinical Trials in the Time of a Pandemic. Ann. Surg. 2020, 272, 219. [Google Scholar] [CrossRef] [PubMed]
- Clay, R.A. Conducting Research During the COVID-19 Pandemic: Advice from Psychological Researchers on Protecting Participants, Animals and Research Plans. Available online: https://www.apa.org/news/apa/2020/03/conducting-research-covid-19 (accessed on 4 December 2020).
- Nearchou, F.; Flinn, C.; Niland, R.; Subramaniam, S.S.; Hennessy, E. Exploring the Impact of COVID-19 on Mental Health Outcomes in Children and Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8479. [Google Scholar] [CrossRef]
- Schulz, K.F.; The CONSORT Group; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef]
- Nosek, B.A.; Beck, E.D.; Campbell, L.; Flake, J.K.; Hardwicke, T.E.; Mellor, D.T.; Veer, A.E.V.T.; Vazire, S. Preregistration Is Hard, and Worthwhile. Trends Cogn. Sci. 2019, 23, 815–818. [Google Scholar] [CrossRef] [PubMed]
- van’t Veer, A.E.; Giner-Sorolla, R. Pre-registration in social psychology—A discussion and suggested template. J. Exp. Soc. Psychol. 2016, 67, 2–12. [Google Scholar] [CrossRef]
- Grist, R.; Porter, J.; Stallard, P. Mental Health Mobile Apps for Preadolescents and Adolescents: A Systematic Review. J. Med Internet Res. 2017, 19, e176. [Google Scholar] [CrossRef]
- Patterson, P.; Pearce, A.; Slawitschka, E. The initial development of an instrument to assess the psychosocial needs and unmet needs of young people who have a parent with cancer: Piloting the offspring cancer needs instrument (OCNI). Support. Care Cancer 2010, 19, 1165–1174. [Google Scholar] [CrossRef]
- Turner, J.R. Designing clinical trials. In New Drug Development; Springer: New York, NY, USA, 2010; pp. 47–67. [Google Scholar]
- Chen, M.; Zheng, H.; Li, J.; Huang, D.; Chen, Q.; Fang, J. Non-pharmacological treatments for adult patients with functional constipation: A systematic review protocol. BMJ Open 2014, 4, e004982. [Google Scholar] [CrossRef] [PubMed]
- Gold, C.; Erkkilä, J. Authors’ reply to “Refurbishing the masked RCT design for psychological interventions”. Br. J. Psychiatry 2011, 199, 515–516. [Google Scholar] [CrossRef]
- Shifren, K.; Chong, A. Health-Related Behaviors: A Study Among Former Young Caregivers. J. Adult Dev. 2012, 19, 111–121. [Google Scholar] [CrossRef]
- Tatangelo, G.; McCabe, M.; MacLeod, A.; You, E. “I just don’t focus on my needs.” The unmet health needs of partner and offspring caregivers of people with dementia: A qualitative study. Int. J. Nurs. Stud. 2018, 77, 8–14. [Google Scholar] [CrossRef]
- Johnson, R.B.; Onwuegbuzie, A.J. Mixed Methods Research: A Research Paradigm Whose Time Has Come. Educ. Res. 2004, 33, 14–26. [Google Scholar] [CrossRef]
- Phillips, D.; Paul, G.; Fahy, M.; Dowling-Hetherington, L.; Kroll, T.; Moloney, B.; Duffy, C.; Fealy, G.; Lafferty, A. The invisible workforce during the COVID-19 pandemic: Family carers at the frontline. HRB Open Res. 2020, 3, 24. [Google Scholar] [CrossRef] [PubMed]
- Carers Trust. My Future, My Feelings, My Family: How Coronavirus is Affecting Young Carers and Young Adult Carers, and what They Want You to do Next; Report; Carers Trust: London, UK, 2020; Available online: https://carers.org/downloads/what-we-do-section/my-future-my-feelings-my-family.pdf (accessed on 26 January 2021).
- Carers Trust Scotland. 2020 Vision: Hear Me, See Me, Support Me and Don’t Forget Me; Report; Carers Trust Scotland: Glasgow, UK, 2020; Available online: https://carers.org/downloads/scotland-pdfs/2020-vision.pdf (accessed on 26 January 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casu, G.; Hlebec, V.; Boccaletti, L.; Bolko, I.; Manattini, A.; Hanson, E. Promoting Mental Health and Well-Being among Adolescent Young Carers in Europe: A Randomized Controlled Trial Protocol. Int. J. Environ. Res. Public Health 2021, 18, 2045. https://doi.org/10.3390/ijerph18042045
Casu G, Hlebec V, Boccaletti L, Bolko I, Manattini A, Hanson E. Promoting Mental Health and Well-Being among Adolescent Young Carers in Europe: A Randomized Controlled Trial Protocol. International Journal of Environmental Research and Public Health. 2021; 18(4):2045. https://doi.org/10.3390/ijerph18042045
Chicago/Turabian StyleCasu, Giulia, Valentina Hlebec, Licia Boccaletti, Irena Bolko, Alessandra Manattini, and Elizabeth Hanson. 2021. "Promoting Mental Health and Well-Being among Adolescent Young Carers in Europe: A Randomized Controlled Trial Protocol" International Journal of Environmental Research and Public Health 18, no. 4: 2045. https://doi.org/10.3390/ijerph18042045
APA StyleCasu, G., Hlebec, V., Boccaletti, L., Bolko, I., Manattini, A., & Hanson, E. (2021). Promoting Mental Health and Well-Being among Adolescent Young Carers in Europe: A Randomized Controlled Trial Protocol. International Journal of Environmental Research and Public Health, 18(4), 2045. https://doi.org/10.3390/ijerph18042045