
Prevalence of Sexual Abuse in Adults with Intellectual Disability: Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search and Selection Strategy
2.2. Inclusion and Exclusion Criteria
- (a)
- Characteristics of participants. Studies were included if they were conducted on or included adults (18+) with Intellectual and/or Developmental Disabilities (ID/DD) as defined by the ICD [3], DSM [4], or the AAIDD [6]. Participants must have experienced sexual abuse; this ranges from verbal harassment or unwanted sexual advances to forced penetration, and an array of types of coercion, from social pressure and intimidation to physical force. Behaviors such as exposing the genitals or looking at or touching certain parts of a victim’s body or requiring the victim to perform sexual acts are defined as sexual abuse. Several characteristics must apply to the victim: (1) he/she withholds the consent, or (2) is unable to give informed consent to, or is not developmentally prepared, or (3) the victim is unduly pressured due to the relationship (e.g., familial), the use of force, a weapon, or threats. Studies were included if they referred to adult samples, and if samples were over 10 subjects.
- (b)
- Characteristics of intervention, factor, or exposure. Studies were included if they reported data of sexual abuse.
- (c)
- Characteristics of comparison or control. For the meta-analysis, studies were included if they used control groups with intellectual disability who were not victims of sexual abuse. They also were included if they used comparison groups from the general population consisting of participants without intellectual disability who were victims of sexual abuse.
- (d)
- Characteristics of outcome. Studies reported prevalence of sexual abuse on population (total, females, and males) with intellectual disability.
2.3. Quality Assessment
3. Results
3.1. Qualitative Synthesis
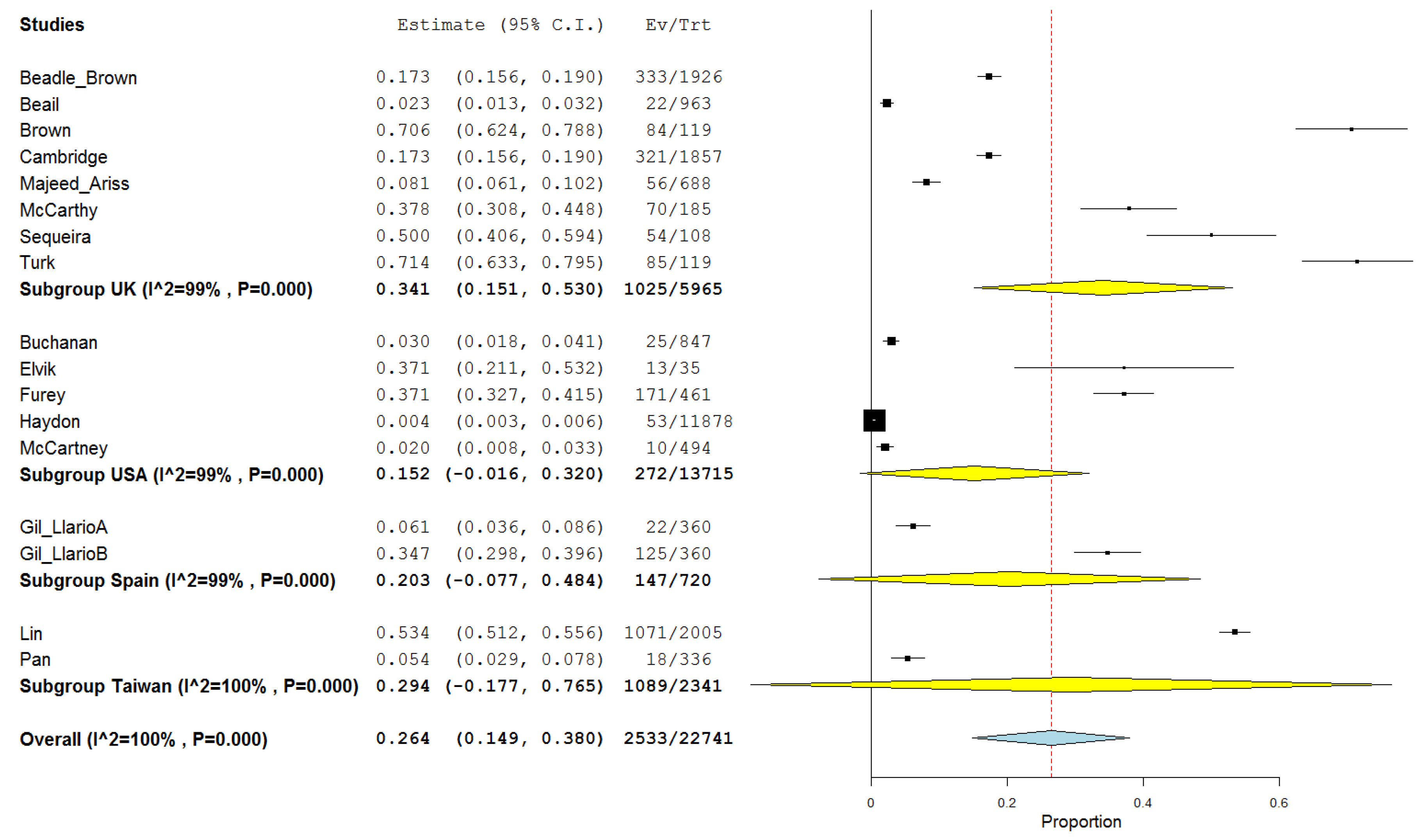
3.2. Quantitative Synthesis (Meta-Analysis)
3.3. Prevalence of Sexual Abuse in Adults with Intellectual Disability
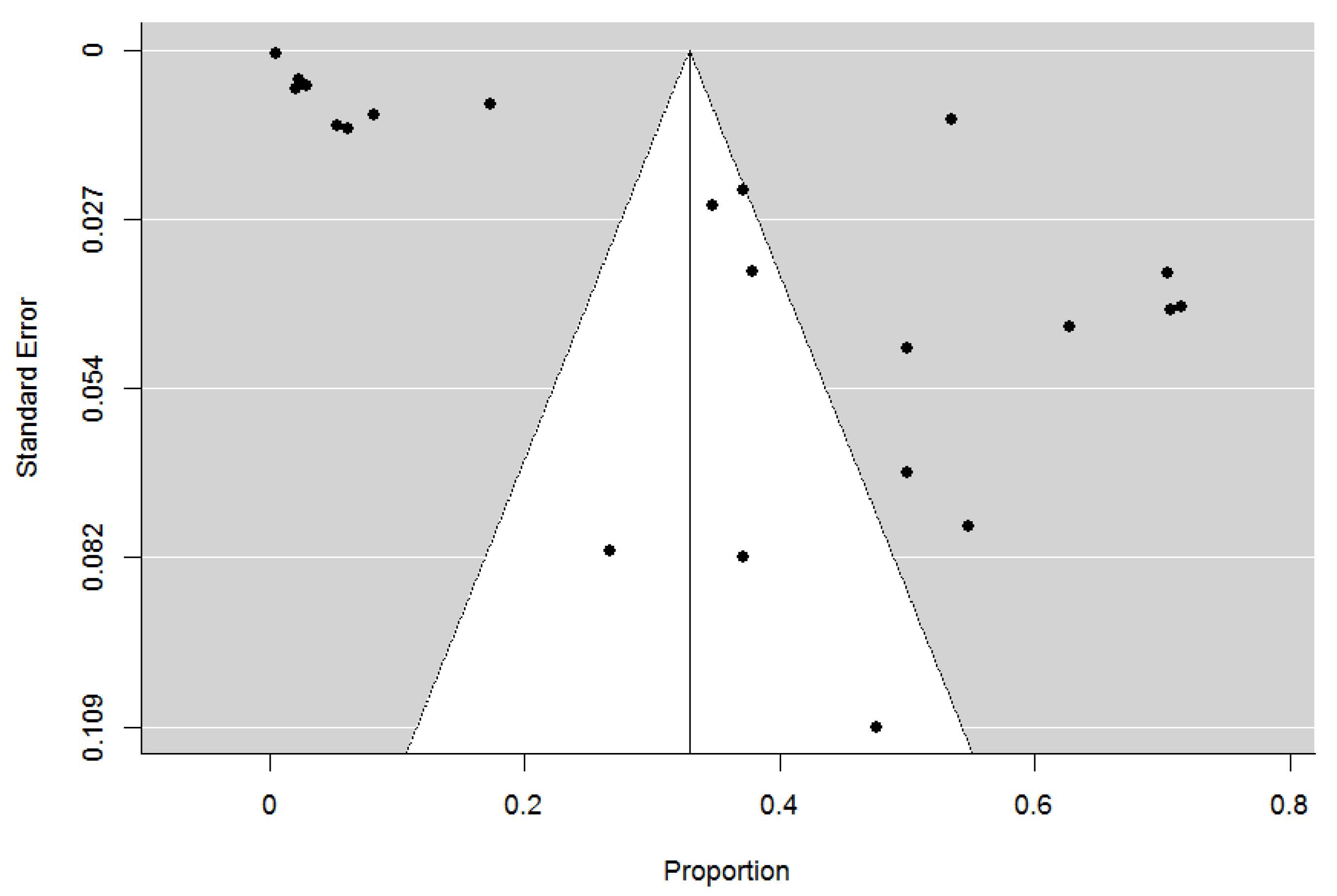
3.4. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | C1 | Study (1) | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 | C11 | C12 | C13 | C14 | Quality Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aker [28] | 2020 | Yes | Cross-Sectional | Yes | Yes | Yes | Yes | No | CD | CD | Yes | No | Yes | No | No | CD | Fair |
| Allington [29] | 2009 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | CD | Yes | Yes | No | No | CD | CD | CD | Fair |
| Beadle-Brown [30] | 2010 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| Beail [31] | 1995 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| Brown [32] | 1994 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| Buchanan [33] | 1991 | Yes | Cross-Sectional | Yes | No | Yes | Yes | Yes | CD | Yes | Yes | No | CD | CD | CD | CD | Fair |
| Cambridge [34] | 2011 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| Dickman [35] | 2005 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| Dunne [36] | 1990 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| ELvik [37] | 1990 | Yes | Cross-Sectional | Yes | No | Yes | Yes | Yes | CD | Yes | Yes | No | CD | CD | CD | CD | Fair |
| Furey [38] | 1994 | CD | Cross-Sectional | Yes | Yes | Yes | Yes | No | CD | Yes | CD | No | CD | No | No | CD | Fair |
| Furey [39] | 1994 | Yes | Case-control | Yes | Yes | Yes | Yes | Yes | CD | Yes | CD | Yes | CD | CD | Fair | ||
| Furey [40] | 1994 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | CD | No | Fair |
| Gil-Llario [41] | 2018 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| Gil-Llario [42] | 2019 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | CD | CD | Yes | No | Yes | No | No | CD | Fair |
| Haydon [43] | 2011 | Yes | Cross-Sectional | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| Lewin [44] | 2007 | Yes | Cross-Sectional | Yes | No | Yes | Yes | Yes | CD | Yes | Yes | No | Yes | CD | CD | CD | Fair |
| Lin [45] | 2009 | Yes | Cross-Sectional | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| Majeed-Ariss [46] | 2020 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| McCabe [47] | 1994 | Yes | Case-control | Yes | No | Yes | Yes | Yes | CD | Yes | CD | CD | CD | CD | Fair | ||
| McCarthy [48] | 1997 | CD | Cross-Sectional | Yes | Yes | Yes | No | No | CD | Yes | Yes | No | Yes | No | No | CD | Fair |
| McCartney [49] | 1998 | Yes | Cross-Sectional | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| McCormack [50] | 2005 | Yes | Case-control | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| Pan [51] | 2007 | Yes | Case-control | Yes | Yes | Yes | No | No | CD | CD | Yes | No | Yes | No | No | CD | Fair |
| Sequeira [52] | 2003 | Yes | Case-control | Yes | Yes | Yes | Yes | Yes | CD | Yes | CD | Yes | CD | CD | Fair | ||
| Shabalala [53] | 2011 | Yes | Case-control | Yes | Yes | Yes | Yes | Yes | CD | Yes | CD | Yes | CD | CD | Fair | ||
| Sobsey [54] | 1991 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | CD | CD | Yes | No | Yes | No | No | CD | Fair |
| Stoffelen [55] | 2013 | Yes | Cross-Sectional | Yes | CD | Yes | No | Yes | Yes | No | Yes | No | Yes | No | No | No | Fair |
| Turk [56] | 1993 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | No | No | CD | Fair |
| Vadysinghe [57] | 2017 | Yes | Cross-Sectional | Yes | Yes | Yes | No | No | Yes | CD | Yes | No | Yes | No | No | CD | Fair |
| First Author | Year | Period of Publication | Context | Country | ID Abused | Total Sample | Women ID Abused | Tot Women | Men ID Abused | Tot Men | Age | Severity ID | Abuser | Informer |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beadle-Brown [30] | 2010 | 3 | non-clinical | UK | 333 | 1926 | NA | NA | NA | NA | 38.9 | moderate | Several | NA |
| Beail [31] | 1995 | 2 | non-clinical | UK | 22 | 963 | 3 | 963 | 3 | NA | 29.5 | mild | Home | other |
| Brown [32] | 1994 | 1 | non-clinical | UK | 84 | 119 | 87 | 119 | 23 | 31 | 31 | moderate | Several | user |
| Buchanan [33] | 1991 | 1 | non-clinical | USA | 25 | 847 | 12 | 847 | 11 | NA | 28 | moderate | Institution | other |
| Cambridge [34] | 2011 | 3 | non-clinical | UK | 321 | 1857 | 116 | 6148 | 100 | NA | 34.02 | moderate | Institution | other |
| Elvik [37] | 1990 | 1 | non-clinical | USA | 13 | 35 | 5 | 35 | NA | NA | 24 | profound | Institution | other |
| Furey [38] | 1994 | 1 | clinical | USA | 171 | 461 | 123 | 461 | 46 | 46 | 30 | moderate | Institution | user |
| Gil-Llario [41] | 2018 | 3 | non-clinical | Spain | 22 | 360 | 2 | 360 | 5 | 180 | NA | moderate | Service | other |
| Gil-Llario [42] | 2019 | 3 | non-clinical | Spain | 125 | 360 | 35 | 360 | 53 | 180 | 50 | moderate | Service | both |
| Haydon [43] | 2011 | 3 | non-clinical | USA | 53 | 11878 | 33 | 53 | 20 | 5428 | NA | mild | Several | both |
| Lewin [44] | 2007 | 2 | non-clinical | Sweden | 23 | 42 | 6 | 7 | 1 | 10 | 50 | moderate | Institution | other |
| Lin [45] | 2009 | 3 | non-clinical | Taiwan | 1071 | 2005 | 0 | 2005 | NA | NA | NA | NA | Several | both |
| Majeed-Ariss [46] | 2020 | 3 | non-clinical | UK | 56 | 688 | 50 | 679 | 6 | 56 | 21.5 | mild | Several | other |
| McCabe [47] | 1997 | 2 | non-clinical | Australia | 8 | 30 | 0 | 30 | NA | 12 | 25.2 | mild | Home | user |
| McCarthy [48] | 1998 | 2 | non-clinical | UK | 70 | 185 | 43 | 185 | 30 | 120 | NA | mild | Institution | user |
| McCartney [49] | 2005 | 2 | non-clinical | USA | 10 | 494 | 6 | 494 | 6 | 296 | NA | profound | Institution | other |
| McCormack [50] | 2007 | 2 | non-clinical | Ireland | 74 | 118 | 39 | 118 | NA | NA | NA | severe | Service | user |
| Pan [51] | 2003 | 2 | non-clinical | Taiwan | 18 | 336 | 10 | 336 | 8 | 190 | NA | mild | Several | user |
| Sequeira [52] | 1991 | 1 | non-clinical | UK | 54 | 108 | 36 | 108 | 18 | 18 | 29.4 | mild | Institution | both |
| Shabalala [53] | 2013 | 3 | non-clinical | South Africa | 27 | 54 | 24 | 54 | 3 | 3 | 18 | mild | Several | both |
| Sobsey [54] | 1993 | 1 | non-clinical | Canada | 114 | 162 | 93 | 162 | NA | 30 | 19.2 | severe | Several | other |
| Stoffelen [55] | 2017 | 3 | non-clinical | The Netherlands | 10 | 21 | 0 | 21 | 10 | 19 | 40.5 | mild | Several | user |
| Turk [56] | 1993 | 1 | non-clinical | UK | 85 | 119 | 62 | 119 | 23 | 31 | 29 | moderate | Several | other |
| Vadysinghe [57] | 2017 | 3 | clinical | Sri Lanka | NA | NA | 74 | 82 | 8 | 82 | 28.3 | mild | Home | NA |
References
- UN General Assembly. Convention on the Rights of Persons with Disabilities: Resolution/Adopted by the General Assembly; 24 January 2007, A/RES/61/106; UN General Assembly: New York, NY, USA, 2007; Available online: https://www.refworld.org/docid/45f973632.html (accessed on 5 February 2021).
- Navas, P.; Gómez, L.E.; Verdugo, M.Á.; Schalock, R.L. Derechos de las personas con discapacidad intelectual: Implicaciones de la convención de naciones unidas. Siglo Cero 2012, 32, 7–28. [Google Scholar]
- World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11); WHO: Geneva, Switzerland, 2018. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013; p. 5. [Google Scholar]
- World Health Organization (WHO). International Classification of Functioning, Disability, and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- AAIDD Ad Hoc Committee on Terminology and Classification. Intellectual Disability: Definition, Classification, and Systems of Support, 11th ed.; AAIDD: Washington, DC, USA, 2010. [Google Scholar]
- Smit, M.J.; Scheffers, M.; Emck, C.; Van Busschbach, J.T.; Beek, P.J. Clinical characteristics of individuals with intellectual disability who have experienced sexual abuse. An overview of the literature. Res. Dev. Disabil. 2019, 95, 103513. [Google Scholar] [CrossRef] [PubMed]
- Fenwick, A. Sexual abuse in adults with learning disabilities. Br. J. Learn. Disabil. 1994, 22, 53–56. [Google Scholar] [CrossRef]
- Fisher, M.H.; Baird, J.V.; Currey, A.D.; Hodapp, R.M. Victimisation and social vulnerability of adults with intellectual disability: A review of research extending beyond wilson and brewer. Aust. Psychol. 2016, 51, 114–127. [Google Scholar] [CrossRef]
- Chave-Cox, R.S. Forensic examination of the mentally disabled sexual abuse complainant. J. Forensic Leg. Med. 2014, 25, 71. [Google Scholar] [CrossRef] [PubMed]
- Fogden, B.C.; Thomas, S.D.M.; Daffern, M.; Ogloff, J.R.P. Crime and victimisation in people with intellectual disability: A case linkage study. BMC Psychiatry 2016, 16, 170. [Google Scholar] [CrossRef]
- McGilloway, C.; Smith, D.; Galvin, R. Barriers faced by adults with intellectual disabilities who experience sexual assault: A systematic review and meta-synthesis. J. Appl. Res. Intellect. Disabil. 2020, 33, 51–66. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A. Incidence of sexual crime committed against learning disabled adults: A review of two key studies and discussion of implications for practitioners and managers of services. J. Learn. Disabil. Nurs. Heal. Soc. Care 1997, 1, 90–95. [Google Scholar] [CrossRef]
- Byrne, G. Prevalence and psychological sequelae of sexual abuse among individuals with an intellectual disability: A review of the recent literature. J. Intellect. Disabil. 2018, 22, 294–310. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; McCann, E. Sexuality issues and the voices of adults with intellectual disabilities: A systematic review of the literature. Res. Dev. Disabil. 2018, 74, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Medina-Rico, M.; López-Ramos, H.; Quiñonez, A. Sexuality in people with intellectual disability: Review of literature. Sex. Disabil. 2018, 36, 231–248. [Google Scholar] [CrossRef]
- Marsland, D.; Oakes, P.; White, C. Abuse in care? The identification of early indicators of the abuse of people with learning disabilities in residential settings. J. Adult Prot. 2007, 9, 6–20. [Google Scholar] [CrossRef]
- White, C.; Holland, E.; Marsland, D.; Oakes, P. The identification of environments and cultures that promote the abuse of people with intellectual disabilities: A review of the literature. J. Appl. Res. Intellect. Disabil. 2003, 16, 1–9. [Google Scholar] [CrossRef]
- Curry, M.A.; Hassouneh-Phillips, D.; Johnston-Silverberg, A. Abuse of women with disabilities. Violence Against Women 2001, 7, 60–79. [Google Scholar] [CrossRef]
- McCarthy, M. Sexual violence against women with learning disabilities. Fem. Psychol. 1998, 8, 544–551. [Google Scholar] [CrossRef]
- Laffaye, C.; Kennedy, C.; Stein, M.B. Post-traumatic stress disorder and health-related quality of life in female victims of intimate partner violence. Violence Vict. 2003, 18, 227–238. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.; Hunt, S.; Milne-Skillman, K. ‘I know it was every week, but I can’t be sure if it was every day”: Domestic violence and women with learning disabilities. J. Appl. Res. Intellect. Disabil. 2016, 30, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Bryen, D.N.; Carey, A.; Frantz, B. Ending the silence: Adults who use augmentative communication and their experiences as victims of crimes. Augment. Altern. Commun. 2003, 19, 125–134. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, 1–25. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Åker, T.H.; Johnson, M.S. Sexual abuse and violence against people with intellectual disability and physical impairments: Characteristics of police-investigated cases in a Norwegian national sample. J. Appl. Res. Intellect. Disabil. 2019, 33, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Allington, C.L.J. Sexual abuse within services for people with learning disabilities. J. Br. Inst. Ment. Handicap. (APEX) 2009, 20, 59–63. [Google Scholar] [CrossRef]
- Beadle-Brown, J.; Mansell, J.; Cambridge, P.; Milne, A.; Whelton, B. Adult protection of people with intellectual disabilities: Incidence, nature and responses. J. Appl. Res. Intellect. Disabil. 2010, 23, 573–584. [Google Scholar] [CrossRef]
- Beail, N.; Warden, S. Sexual abuse of adults with learning disabilities. J. Intellect. Disabil. Res. 1995, 39, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.; Turk, V. Sexual abuse in adulthood: Ongoing risks for people with learning disabilities. Child Abus. Rev. 1994, 3, 26–35. [Google Scholar] [CrossRef]
- Buchanan, A.; Wilkins, R. Sexual abuse of the mentally handicapped: Difficulties in establishing prevalence. Psychiatr. Bull. 1991, 15, 601–605. [Google Scholar] [CrossRef]
- Cambridge, P.; Beadle-Brown, J.; Milne, A.; Mansell, J.; Whelton, B. Patterns of risk in adult protection referrals for sexual abuse and people with intellectual disability. J. Appl. Res. Intellect. Disabil. 2011, 24, 118–132. [Google Scholar] [CrossRef]
- Dickman, B.J.; Roux, A.J. Complainants with learning disabilities in sexual abuse cases: A 10-year review of a psycho-legal project in Cape Town, South Africa. Br. J. Learn. Disabil. 2005, 33, 138–144. [Google Scholar] [CrossRef]
- Dunne, T.P.; Power, A. Sexual abuse and mental handicap: Preliminary findings of a community-based study. Ment. Handicap. Res. 2010, 3, 111–125. [Google Scholar] [CrossRef]
- Elvik, S.L.; Berkowitz, C.D.; Nicholas, E.; Lipman, J.L.; Inkelis, S.H. Sexual abuse in the developmentally disabled: Dilemmas of diagnosis. Child Abus. Negl. 1990, 14, 497–502. [Google Scholar] [CrossRef]
- Furey, E.M. Sexual abuse of adults with mental retardation: Who and where. Ment. Retard. 1994, 32, 173–180. [Google Scholar] [PubMed]
- Furey, E.M.; Granfield, J.M.; Karan, O.C. Sexual abuse and neglect of adults with mental retardation: A comparison of victim characteristics. Behav. Interv. 1994, 9, 75–86. [Google Scholar] [CrossRef]
- Furey, E.M.; Niesen, J.J. Sexual abuse of adults with mental retardation by other consumers. Sex. Disabil. 1994, 12, 285–295. [Google Scholar] [CrossRef]
- Gil-Llario, M.D.; Morell-Mengual, V.; Ballester-Arnal, R.; Díaz-Rodríguez, I. The experience of sexuality in adults with intellectual disability. J. Intellect. Disabil. Res. 2017, 62, 72–80. [Google Scholar] [CrossRef]
- Gil-Llario, M.D.; Morell-Mengual, V.; Díaz-Rodríguez, I.; Ballester-Arnal, R. Prevalence and sequelae of self-reported and other-reported sexual abuse in adults with intellectual disability. J. Intellect. Disabil. Res. 2018, 63, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Haydon, A.A.; McRee, A.-L.; Halpern, C.T. Unwanted sex among young adults in the United States. J. Interpers. Violence 2011, 26, 3476–3493. [Google Scholar] [CrossRef] [PubMed]
- Lewin, B. Who cares about disabled victims of crime? Barriers and facilitators for redress. J. Policy Pr. Intellect. Disabil. 2007, 4, 170–176. [Google Scholar] [CrossRef]
- Lin, L.-P.; Yen, C.-F.; Kuo, F.-Y.; Wu, J.-L.; Lin, J.-D. Sexual assault of people with disabilities: Results of a 2002–2007 National Report in Taiwan. Res. Dev. Disabil. 2009, 30, 969–975. [Google Scholar] [CrossRef]
- Majeed-Ariss, R.; Rodriguez, P.M.; White, C. The disproportionately high prevalence of learning disabilities amongst adults attending Saint Marys Sexual Assault Referral Centre. J. Appl. Res. Intellect. Disabil. 2020, 33, 595–603. [Google Scholar] [CrossRef] [PubMed]
- McCabe, M.P.; Cummins, R.A.; Reid, S.B. An empirical study of the sexual abuse of people with intellectual disability. Sex. Disabil. 1994, 12, 297–306. [Google Scholar] [CrossRef]
- McCarthy, M.; Thompson, D. A prevalence study of sexual abuse of adults with intellectual disabilities referred for sex education. J. Appl. Res. Intellect. Disabil. 1997, 10, 105–124. [Google Scholar] [CrossRef]
- McCartney, J.R.; Campbell, A.V. Confirmed abuse cases in public residential facilities for persons with mental retardation: A multi-state study. Ment. Retard. 1998, 36, 465–473. [Google Scholar] [CrossRef]
- McCormack, B.; Kavanagh, D.; Caffrey, S.; Power, A. Investigating sexual abuse: Findings of a 15-year longitudinal study. J. Appl. Res. Intellect. Disabil. 2005, 18, 217–227. [Google Scholar] [CrossRef]
- Pan, S.-M. Prevalence of sexual abuse of people with intellectual disabilities in Taiwan. Intellect. Dev. Disabil. 2007, 45, 373–379. [Google Scholar] [CrossRef]
- Sequeira, H.; Howlin, P.; Hollins, S. Psychological disturbance associated with sexual abuse in people with learning disabilities. Br. J. Psychiatry 2003, 183, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Shabalala, N.; Jasson, A. PTSD symptoms in intellectually disabled victims of sexual assault. South Afr. J. Psychol. 2011, 41, 424–436. [Google Scholar] [CrossRef]
- Sobsey, D.; Doe, T. Patterns of sexual abuse and assault. Sex. Disabil. 1991, 9, 243–259. [Google Scholar] [CrossRef]
- Stoffelen, J.; Kok, G.; Hospers, H.; Curfs, L.M.G. Homosexuality among people with a mild intellectual disability: An explorative study on the lived experiences of homosexual people in the Netherlands with a mild intellectual disability. J. Intellect. Disabil. Res. 2012, 57, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Turk, V.; Brown, H. The sexual abuse of adults with learning disabilites: Results of a two year incidence survey. Ment. Handicap. Res. 2010, 6, 193–216. [Google Scholar] [CrossRef]
- Vadysinghe, A.; Dassanayaka, P.; Sivasubramanium, M.; Senasinghe, D.; Samaranayake, A.; Wickramasinghe, W.; Samaranayaka, A. A study on sexual violence inflicted on individuals with intellectual developmental disorder. Disabil. Heal. J. 2017, 10, 451–454. [Google Scholar] [CrossRef]
- Wallace, B.C.; Dahabreh Issa, J.; Trikalinos Thomas, A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the gap between methodologists and end-users: R as a computational back-end. J. Stat. Softw. 2012, 49, 5. [Google Scholar] [CrossRef]
- Jamovi Project jamovi, Version 0.9, Computer Software. 2018. Available online: https://www.jamovi.org (accessed on 18 September 2018).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Lipsey, M.; Wilson, D. Practical Meta-Analysis; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- De Sola, H.; Dueñas, M.; Salazar, A.; Ortega-Jiménez, P.; Failde, I. Prevalence of therapeutic use of opioids in chronic non-cancer pain patients and associated factors: A systematic review and meta-analysis. Front. Pharmacol. 2020, 11, 564412. [Google Scholar] [CrossRef] [PubMed]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Becker, B.J.; Aloe, A.M. Model-based Meta-analysis And Related Approaches. In He Handbook of Research Synthesis And Meta-Analysis, 3rd ed.; Copper, T.H., Hedges, L.V., Valentine, J.C., Eds.; Russell Sage Foundation: New York, NY, USA, 2019; pp. 339–363. [Google Scholar]
- Allroggen, M.; Ohlert, J.; Rau, T.; Fegert, J.M. Sexual abuse prevalence rates of residents in institutional care settings compared with a population representative sample. Resid. Treat. Child. Youth 2018, 35, 286–296. [Google Scholar] [CrossRef]
- Mitra, M.; Mouradian, V.E.; Diamond, M. Sexual violence victimization against men with disabilities. Am. J. Prev. Med. 2011, 41, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Igualdad. Macroencuesta de Violencia Contra la Mujer 2019; Ministerio de Igualdad: Madrid, Spain, 2019. Available online: https://violenciagenero.igualdad.gob.es/violenciaEnCifras/macroencuesta2015/pdf/Macroencuesta_2019_estudio_investigacion.pdf (accessed on 2 July 2018).
- Murphy, G.H.; O’Callaghan, A.C.; Clare, I.C.H. The impact of alleged abuse on behaviour in adults with severe intellectual disabilities. J. Intellect. Disabil. Res. 2007, 51, 741–749. [Google Scholar] [CrossRef] [PubMed]




| First Author * | Year | Country | Context | Type of Study | Temporal Direction | Prevalence/ Incidence | Point/ Period | Length of Study |
|---|---|---|---|---|---|---|---|---|
| * Aker [28] | 2020 | Norway | clinical | Cross-sectional | Retrospective | PR | PE | 2 |
| * Allington [29] | 2009 | UK | clinical | Cross-sectional | Retrospective | PR | PO | |
| Beadle-Brown [30] | 2010 | UK | clinical | Longitudinal | Retrospective | PR | PE | 0.8 |
| Beail [31] | 1995 | UK | clinical | Cross-sectional | Retrospective | PR | PE | 4 |
| Brown [32] | 1994 | UK | clinical | Longitudinal | Retrospective | IN | PE | 3 |
| Buchanan [33] | 1991 | USA | clinical | Cross-sectional | Retrospective | PR | PO | |
| Cambridge [34] | 2011 | UK | clinical | Longitudinal | Retrospective | PR | PE | 5 |
| * Dickman [35] | 2005 | South Africa | clinical | Cross-sectional | Retrospective | PR | PE | 10 |
| * Dunne [36] | 1990 | Ireland | clinical | Cross-sectional | Retrospective | PR | PE | 3 |
| Elvik [37] | 1990 | USA | non-clinical | Cross-sectional | Retrospective | PR | PO | |
| Furey [38] | 1994 | USA | clinical | Cross-sectional | Retrospective | PR | PE | 5 |
| * Furey [39] | 1994 | USA | clinical | Case-control | Retrospective | PR | PE | 5 |
| * Furey [40] | 1994 | USA | clinical | Cross-sectional | Retrospective | PR | PE | 5 |
| Gil-Llario [41] | 2018 | Spain | non-clinical | Cross-sectional | Retrospective | PR | PO | |
| Gil-Llario [42] | 2019 | Spain | non-clinical | Cross-sectional | Retrospective | PR | PO | |
| Haydon [43] | 2011 | USA | non-clinical | Cross-sectional | Retrospective | PR | PE | 1 |
| Lewin [44] | 2007 | Sweden | clinical | Cross-sectional | Retrospective | PR | PO | |
| Lin [45] | 2009 | Taiwan | clinical | Longitudinal | Retrospective | PR/IN | PE | 6 |
| Majeed-Ariss [46] | 2020 | UK | clinical | Cross-sectional | Retrospective | PR | PE | 1 |
| McCabe [47] | 1994 | UK | non-clinical | Case-control | Retrospective | PR | PO | |
| McCarthy [48] | 1997 | USA | non-clinical | Cross-sectional | Retrospective | PR | PE | 5 |
| McCartney [49] | 1998 | Ireland | clinical | Cross-sectional | Retrospective | PR | PE | 2 |
| McCormack [50] | 2005 | Taiwan | clinical | Cross-sectional | Retrospective | PR | PO | 15 |
| Pan [51] | 2007 | UK | non-clinical | Cross-sectional | Retrospective | PR | PO | |
| Sequeira [52] | 2003 | Sweden | clinical | Case-control | Retrospective | PR | PO | |
| Shabalala [53] | 2011 | South Africa | clinical | Case-control | Retrospective | PR | PO | |
| Sobsey [54] | 1991 | Canada | clinical | Cross-sectional | Retrospective | PR | PE | 2 |
| Stoffelen [55] | 2013 | The Netherlands | clinical | Cross-sectional | Retrospective | PR | PO | |
| Turk [56] | 1993 | UK | clinical | Cross-sectional | Retrospective | PR | PE | 3 |
| Vadysinghe [57] | 2017 | Sri Lanka | clinical | Cross-sectional | Retrospective | PR | PE | 5 |
| Subgroups | Studies | Pooled Prevalence (%) | SE | p | Hete I2(%) | Q | p |
|---|---|---|---|---|---|---|---|
| Several | 10 | 39.1 (21.1–57.1) | 0.092 | <0.001 | 100 | 3710.49 | <0.001 |
| Home | 2 | 13.1 (−10.6–36.9) | 0.121 | 0.278 | 89 | 9.09 | <0.003 |
| Institution | 7 | 28.1 (12.0–44.1) | 0.082 | <0.001 | 99 | 450.19 | <0.001 |
| Service | 3 | 34.3 (2.3–66.3) | 0.163 | 0.036 | 99 | 226.23 | <0.001 |
| Place | 22 | 32.7 (22.1–43.3) | 0.054 | <0.001 | 100 | 4767.23 | <0.001 |
| Professionals | 3 | 17.6 (−1.9–37.0) | 0.099 | 0.076 | 99 | 216.93 | <0.001 |
| Relatives | 2 | 36.2 (−30.5–100) | 0.340 | 0.287 | 100 | 353.80 | <0.001 |
| Peers | 6 | 42.7 (19.7–65.7) | 0.117 | <0.001 | 99 | 516.21 | <0.001 |
| Several | 7 | 25.4 (10.0–40.8) | 0.079 | 0.001 | 98 | 336.73 | <0.001 |
| nonspec | 4 | 39.2 (13.2–65.2) | 0.133 | 0.003 | 100 | 2356.46 | <0.001 |
| Abuser | 22 | 32.7 (22.1–43.3) | 0.054 | <0.001 | 100 | 4767.23 | <0.001 |
| Mild | 9 | 24.3 (10.2–38.4) | 0.072 | <0.001 | 98 | 381.07 | <0.001 |
| Moderate | 8 | 34.0 (14.7–53.4) | 0.099 | <0.001 | 99 | 849.21 | <0.001 |
| Severe | 2 | 67.0 (59.5–74.4) | 0.038 | <0.001 | 44 | 1.79 | 0.180 |
| Profound | 2 | 18.6 (−15.7–53.0) | 0.175 | 0.288 | 95 | 18.38 | <0.001 |
| Severity | 21 | 31.7 (20.7–42.7) | 0.056 | <0.001 | 99 | 2545.31 | <0.001 |
| User | 7 | 38.0 (20.1–55.8) | 0.091 | <0.001 | 99 | 403.47 | <0.001 |
| Other | 10 | 26.8 (9.0–44.6) | 0.091 | 0.003 | 99 | 917.27 | <0.001 |
| Both | 5 | 37.4 (17.9–56.9) | 0.100 | <0.001 | 100 | 2596.75 | <0.001 |
| Informant | 22 | 32.7 (22.1–43.3) | 0.054 | <0.001 | 100 | 4767.23 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomsa, R.; Gutu, S.; Cojocaru, D.; Gutiérrez-Bermejo, B.; Flores, N.; Jenaro, C. Prevalence of Sexual Abuse in Adults with Intellectual Disability: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 1980. https://doi.org/10.3390/ijerph18041980
Tomsa R, Gutu S, Cojocaru D, Gutiérrez-Bermejo B, Flores N, Jenaro C. Prevalence of Sexual Abuse in Adults with Intellectual Disability: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(4):1980. https://doi.org/10.3390/ijerph18041980
Chicago/Turabian StyleTomsa, Raluca, Smaranda Gutu, Daniel Cojocaru, Belén Gutiérrez-Bermejo, Noelia Flores, and Cristina Jenaro. 2021. "Prevalence of Sexual Abuse in Adults with Intellectual Disability: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 4: 1980. https://doi.org/10.3390/ijerph18041980
APA StyleTomsa, R., Gutu, S., Cojocaru, D., Gutiérrez-Bermejo, B., Flores, N., & Jenaro, C. (2021). Prevalence of Sexual Abuse in Adults with Intellectual Disability: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(4), 1980. https://doi.org/10.3390/ijerph18041980