
Spatial Effects of Environmental Pollution on Healthcare Services: Evidence from China


Abstract
1. Introduction
- (1)
- This study aims to explore the spatial characteristics and distributions of different pollutants and of the utilization of healthcare services in China to provide proper guidance on spatial policies for the government.
- (2)
- Spatial econometric models were applied in this study to assess the spill-over effects of different pollutants on healthcare service utilization, that is, to identify the relationship between pollution in the local region and healthcare service utilization in geographically or economically adjacent provinces.
- (3)
- Inpatient and outpatient services are two different services used by different groups of people. In this study, we explored the direction and magnitude of the effects of environmental pollution on inpatient and outpatient services.
2. Materials and Methods
2.1. Data Source
2.2. Variables
2.2.1. Dependent Variables: Outpatient and Inpatient Care Services
2.2.2. Independent Variables: Environmental Pollution
2.2.3. Control Variables
2.3. Methods
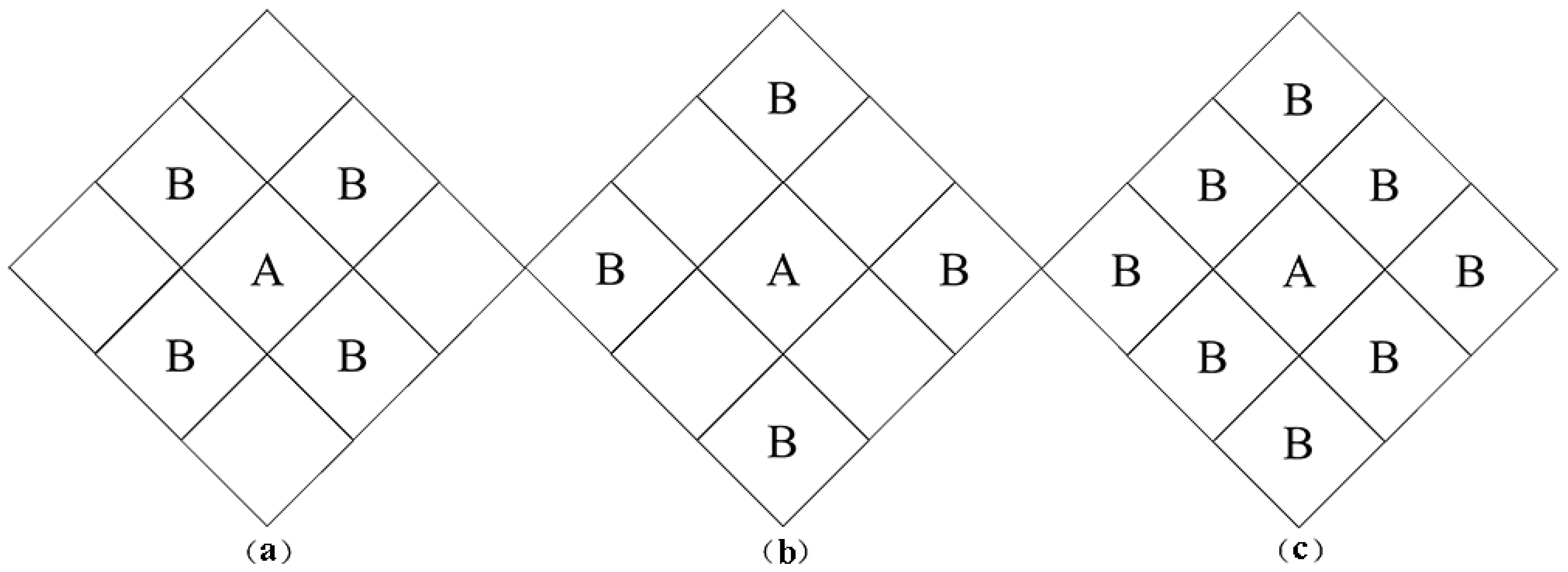
2.3.1. Spatial Autocorrelation Test
2.3.2. Spatial Econometric Model
2.4. Software
3. Spatial Distribution and Spatial Autocorrelation Analysis
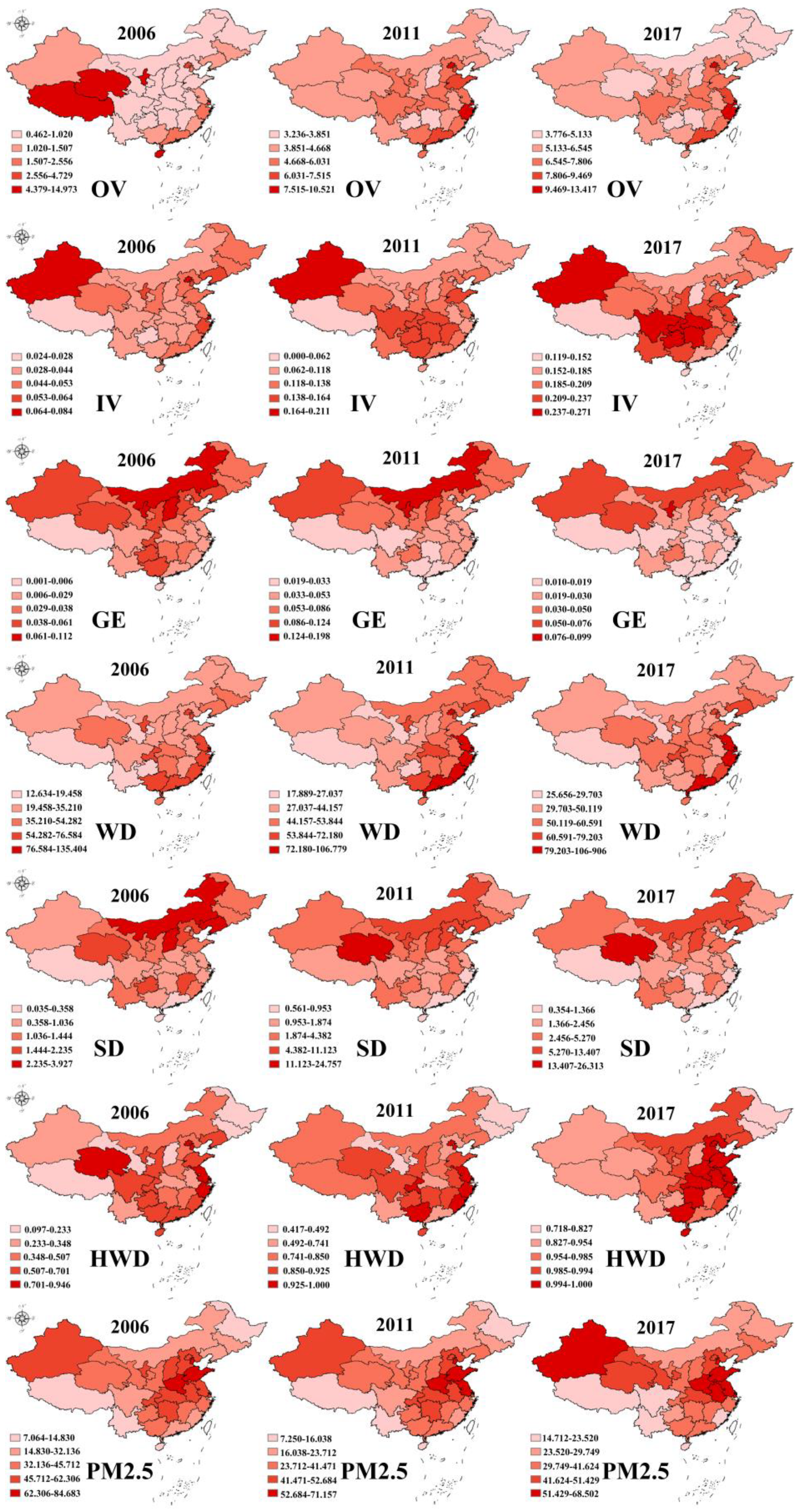
3.1. Descriptive Analysis
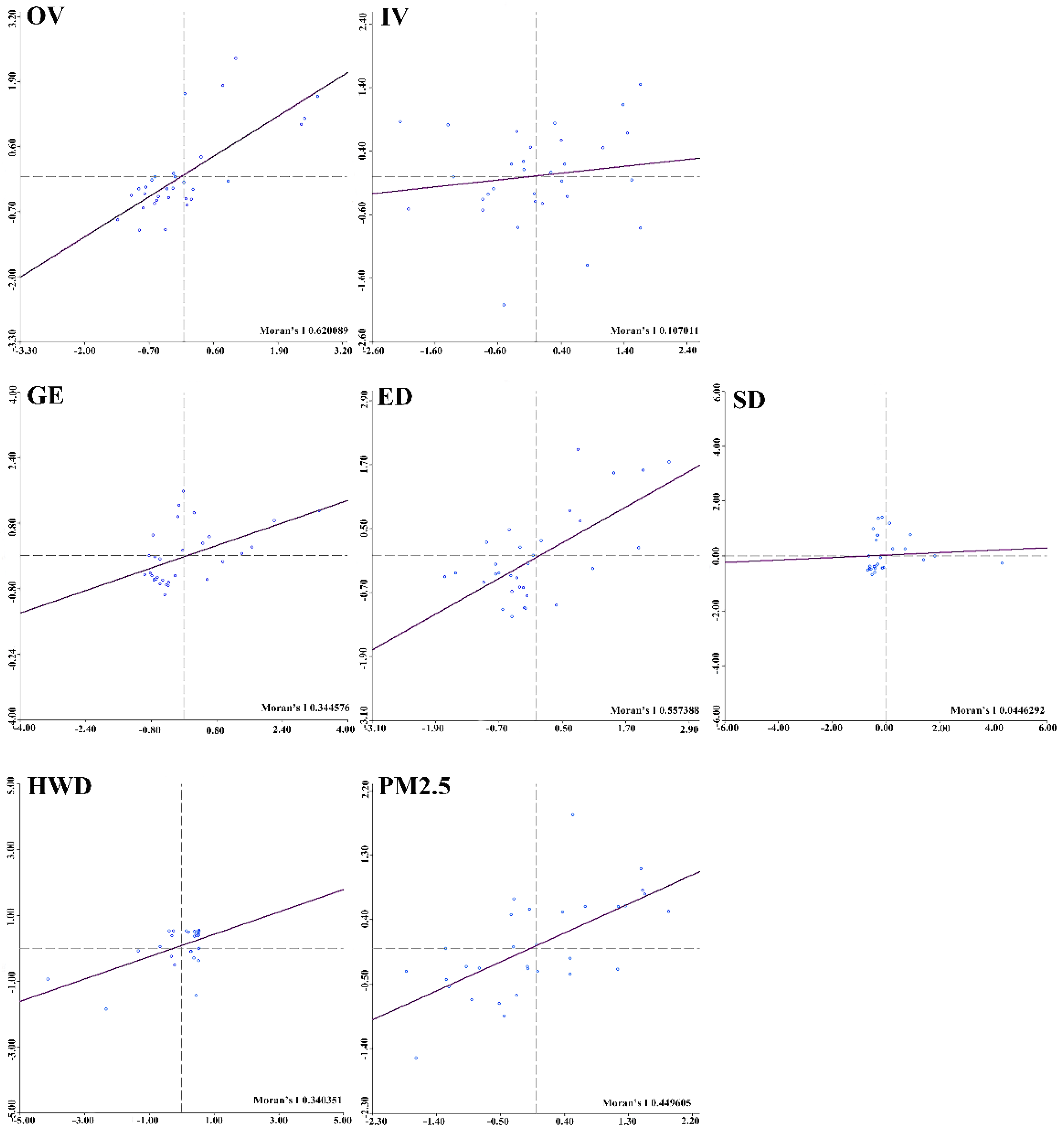
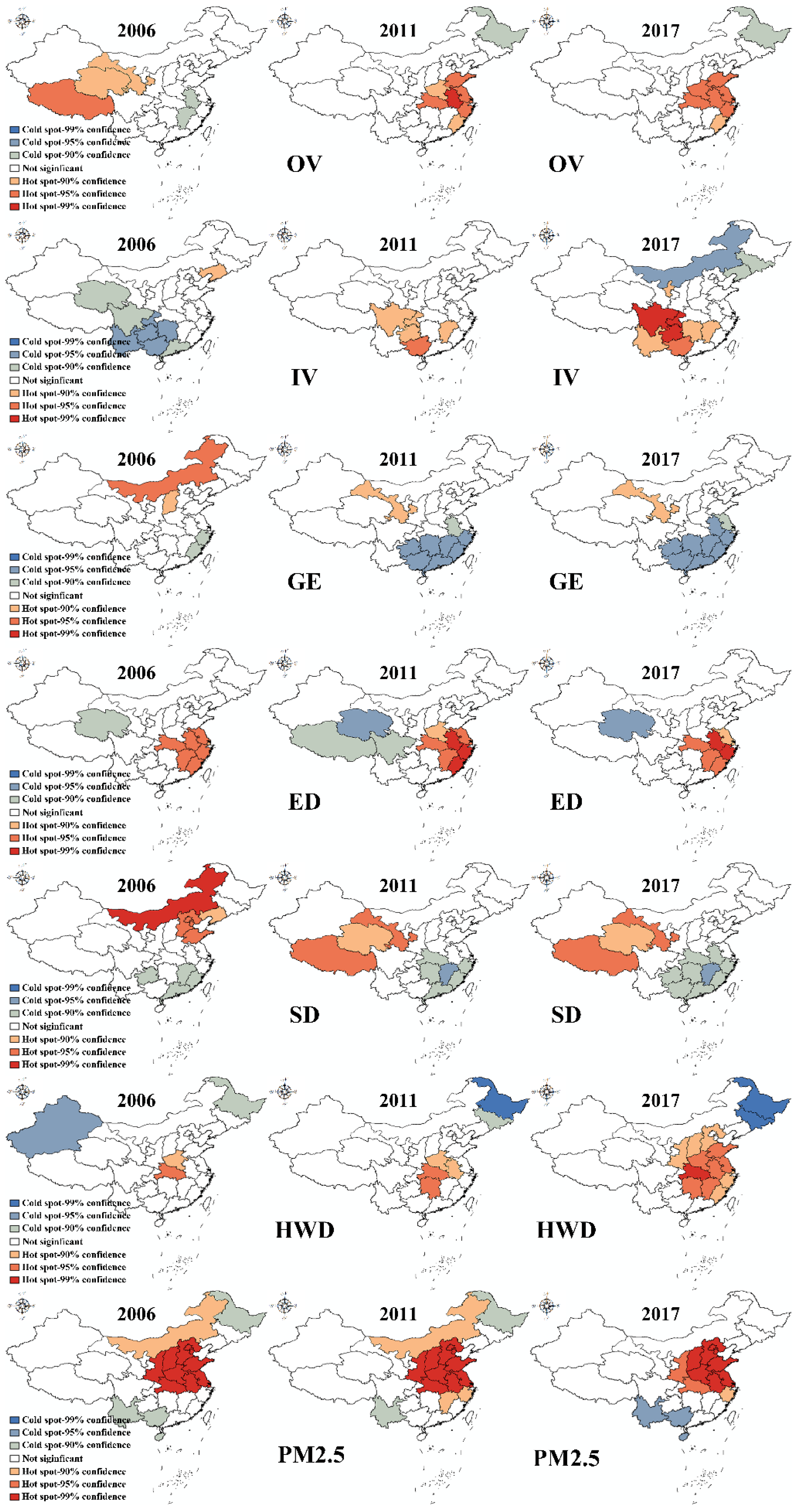
3.2. Spatial Autocorrelation Analysis
4. Empirical Analysis and Discussion
4.1. Empirical Results of Spatial Panel Models
4.2. Decomposition of Direct and Spill-Over Effects
5. Conclusions
- (1)
- The utilization of healthcare services and environmental pollution were not randomly distributed in China. There were distinct spatial cluster characteristics according to the global Moran’s I analysis. Healthcare services were affected not only by environmental factors but also by the pollution of geographically and economically related regions.
- (2)
- Environmental pollution could pose a threat to the health of humans. Regardless of whether the pollution is from the local region or another related province, the empirical analysis indicates that the growth of pollutants could contribute to the increase in outpatient and inpatient visits. For example, with every 1% increase in gas emissions in the local region, outpatient visits grow 0.350% in that specific region.
- (3)
- Environmental pollution exhibited spill-over effects on healthcare services. Local pollution can cause an increase in healthcare services in the same region, while pollution in other geographically or economically related regions could also affect healthcare services in the local region. Naturally, some forms of pollution, such as air pollution, can spread towards other places. Effluent discharge from upstream flows downstream. Economically related regions normally develop industries at the same pace, which may lead to similar contamination situations.
- (4)
- Specifically, pollution showed different degrees of influence on healthcare services, which means that the impact of environmental pollution on the number of outpatient visits is greater than its impact on that of inpatient visits. Almost all relationships between pollution and outpatient visits were significant, while there was no significant relationship between pollution and inpatient visits. Normally, outpatient services are for emergencies or diseases with mild symptoms, while inpatient services are aimed at diseases with serious symptoms or those requiring surgery. Although environmental pollution could cause diseases with either mild or severe symptoms, it is difficult to distinguish these factors from other determinants of disease.
- (5)
- This finding was related to the control variables. Different age groups were associated with different healthcare services. Children aged 0–14 tended to receive outpatient services, while elderly people were more likely to receive inpatient services. This may be explained by the disease spectrum across different age groups. In addition, demographic factors showed distinct spill-over effects, and the high need for healthcare services in some places could lead to a decrease in the provision of healthcare services in geographically and economically close regions.
- (6)
- The lasting finding was associated with economic development, in some extent, the relationship between economic growth and health with environmental pollution as mediator variable was still unclear. In this study, per capita GDP was included in as independent variable, and the positive association was found towards this variable. The reason behind this was the attraction of rich regions which owned better medical services. However, economic development may cause environmental pollution and changes of healthcare services. This study was unable to state that relationship. There were two main opinions about this relationship in research world: “economic growth-heavy environmental pollution-bad health-heavy healthcare needs”, “economic growth- transformation of industries-better environment-less healthcare needs”. The first change improves healthcare needs in local regions, while the other changes that in other regions. To sum up, the relationship between economic growth and health with environmental pollution as mediator variable was complicated and this study failed to prove it.
- (1)
- At the governmental level, authorities from all levels should not only participate in the formulation and implementation of basic environmental protection policies but also enhance their cooperation with other authorities. On the one hand, the management of health and environmental protection belong to different administrative divisions in China, so authorities in all divisions should work together to address this problem. On the other hand, environmental pollution showed spill-over effects, so regional and national cooperation should be considered.
- (2)
- From the perspective of a company or industrial organization that may cause pollution, apart from obeying the basic requirements issued by the government, the relevant companies should pay more attention to the location of their spill-over effects. Most importantly, the location of factories should be distant from residential areas and the community. In addition, all factories should obtain information on their pollutants and the damage caused thereby, as well as on the areas affected by that damage. This could help effective and fast measures be implemented when an emergency occurs.
- (3)
- From the perspective of communities and citizens, it is vital to learn and understand the damage caused by environmental pollution and to take measures towards alleviating this problem. Specifically, it would be better for communities and citizens to have access to information about surrounding factories and their possible pollutants in order to take necessary precautions against those pollutants. In addition, citizens who live in unpolluted areas should try to avoid staying in places with heavy pollution for a long time, such as mining areas, waste incineration areas, and regions with contaminated water.
- (1)
- Limitations
- (2)
- Strengths
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, L.; Fu, H. China’s health care system reform: Progress and prospects. Int. J. Health Plan. Manag. 2017, 32, 240–253. [Google Scholar] [CrossRef]
- Abbafati, C.; Machado, D.B.; Cislaghi, B.; Salman, O.M.; Karanikolos, M.; McKee, M.; Abbas, K.M.; Brady, O.J.; Larson, H.J.; Trias-Llimós, S. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar]
- WHO. Unicef Progress on Sanitation and Drinking Water 2013 Update; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- WHO. Safely Managed Drinking Water; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- WHO; UNICEF. Progress on Sanitation and Drinking Water: 2015 Update and MDG Assessment; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- IQAir. World Air Quality Report; WHO Press: Geneva, Switzerland, 2019. [Google Scholar]
- Apte, J.S.; Brauer, M.; Cohen, A.J.; Ezzati, M.; Pope, C.A. Ambient PM2.5 reduces global and regional life expectancy. Environ. Sci. Technol. Lett. 2018, 5, 546–551. [Google Scholar] [CrossRef]
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.-B.H.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef]
- Bourdrel, T.; Bind, M.A.; Béjot, Y.; Morel, O.; Argacha, J.F. Cardiovascular effects of air pollution. Arch. Cardiovasc. Dis. 2017, 110, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Williams, J.S.; Kowal, P.; Negin, J.; Snodgrass, J.J.; Yawson, A.; Minicuci, N.; Thiele, L.; Phaswana-Mafuya, N.; Biritwum, R.B. Universal health coverage in emerging economies: Findings on health care utilization by older adults in China, Ghana, India, Mexico, the Russian Federation, and South Africa. Glob. Health Action 2014, 7, 25314. [Google Scholar]
- Song, C.; He, J.; Wu, L.; Jin, T.; Chen, X.; Li, R.; Ren, P.; Zhang, L.; Mao, H. Health burden attributable to ambient PM2.5 in China. Environ. Pollut. 2017, 223, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Du, J.; Zhang, W. Spatial-temporal effects of PM 2.5 on health burden: Evidence from China. Int. J. Environ. Res. Public Health 2019, 16, 4695. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, Z. Industrial water pollution, water environment treatment, and health risks in China. Environ. Pollut. 2016, 218, 358–365. [Google Scholar] [CrossRef]
- Yang, Q.; Li, Z.; Lu, X.; Duan, Q.; Huang, L.; Bi, J. A review of soil heavy metal pollution from industrial and agricultural regions in China: Pollution and risk assessment. Sci. Total Environ. 2018, 642, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Ghorani-Azam, A.; Riahi-Zanjani, B.; Balali-Mood, M. Effects of air pollution on human health and practical measures for prevention in Iran. J. Res. Med. Sci. 2016, 21, 65. [Google Scholar] [PubMed]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Fuller, R.; Fisher, S.; Suk, W.A.; Sly, P.; Chiles, T.C.; Bose-O’Reilly, S. Pollution and children’s health. Sci. Total Environ. 2019, 650, 2389–2394. [Google Scholar] [CrossRef]
- Rodríguez-Tapia, L.; Morales-Novelo, J.A. Bacterial pollution in river waters and gastrointestinal diseases. Int. J. Environ. Res. Public Health 2017, 14, 479. [Google Scholar] [CrossRef]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public Health 2020, 8, 14. [Google Scholar]
- Patrick, D.L. Health and environmental effects of air pollution. Health Environ. Eff. Air Pollut. Health 2016, 1, 1–3. [Google Scholar]
- Mao, Y.; Yang, D.; He, J.; Krasna, M.J. Epidemiology of lung cancer. Surg. Oncol. Clin. North Am. 2016, 25, 439–445. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; De Matteis, S.; Jung, S.H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A. Air pollution and noncommunicable diseases: A review by the forum of international respiratory societies’ environmental committee, part 2: Air pollution and organ systems. Chest 2019, 155, 409–416. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, B. Air pollution and healthcare expenditure: Implication for the benefit of air pollution control in China. Environ. Int. 2018, 120, 443–455. [Google Scholar]
- Taj, T.; Malmqvist, E.; Stroh, E.; Åström, D.O.; Jakobsson, K.; Oudin, A. Short-term associations between air pollution concentrations and respiratory health—Comparing primary health care visits, hospital admissions, and emergency department visits in a multi-municipality study. Int. J. Environ. Res. Public Health 2017, 14, 587. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.; Fu, Q.; Zhang, L.; Lyu, D.; Mao, G.; Wu, L.; Xu, P.; Wang, Z.; Pan, X.; Chen, Z. Acute effects of air pollution on respiratory disease mortalities and outpatients in Southeastern China. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Zhong, T.; Li, H.; Xu, J.; Ye, X.; Mu, Z.; Lu, Y.; Mashaghi, A.; Zhou, Y.; Tan, M. Ambient air pollution, weather changes, and outpatient visits for allergic conjunctivitis: A retrospective registry study. Sci. Rep. 2016, 6, 23858. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Messier, K.P.; Gani, S.; Brauer, M.; Kirchstetter, T.W.; Lunden, M.M.; Marshall, J.D.; Portier, C.J.; Vermeulen, R.C.H.; Hamburg, S.P. High-resolution air pollution mapping with google street view cars: Exploiting big data. Environ. Sci. Technol. 2017, 51, 6999–7008. [Google Scholar] [CrossRef]
- Chen, Z.; Kahn, M.E.; Liu, Y.; Wang, Z. The consequences of spatially differentiated water pollution regulation in China. J. Environ. Econ. Manag. 2018, 88, 468–485. [Google Scholar] [CrossRef]
- Wang, X.B.; Yan, X.; Li, X.Y.; Ji, H.J. Environmental risks for application of phosphogysum in agricultural soils in China. Sci. Agric. Sin. 2019, 2, 293–311. [Google Scholar]
- Yang, J.; Jit, M.; Leung, K.S.; Zheng, Y.-M.; Feng, L.-Z.; Wang, L.-P.; Lau, E.H.Y.; Wu, J.T.; Yu, H.-J. The economic burden of influenza-associated outpatient visits and hospitalizations in China: A retrospective survey. Infect. Dis. Poverty 2015, 4, 44. [Google Scholar] [CrossRef]
- Li, J.; Wang, P.; Kong, X.; Liang, H.; Zhang, X.; Shi, L. Patient satisfaction between primary care providers and hospitals: A cross-sectional survey in Jilin province, China. Int. J. Qual. Health Care 2016, 28, 346–354. [Google Scholar] [CrossRef]
- Erlangga, D.; Ali, S.; Bloor, K. The impact of public health insurance on healthcare utilisation in Indonesia: Evidence from panel data. Int. J. Public Health 2019, 64, 603–613. [Google Scholar] [CrossRef]
- Li, Y.R.; Xiao, C.C.; Li, J.; Tang, J.; Geng, X.Y.; Cui, L.J.; Zhai, J.X. Association between air pollution and upper respiratory tract infection in hospital outpatients aged 0–14 years in Hefei, China: A time series study. Public Health 2018, 156, 92–100. [Google Scholar] [CrossRef]
- Carey, I.M.; Atkinson, R.W.; Kent, A.J.; Van Staa, T.; Cook, D.G.; Anderson, H.R. Mortality associations with long-term exposure to outdoor air pollution in a national English cohort. Am. J. Respir. Crit. Care Med. 2013, 187, 1226–1233. [Google Scholar] [CrossRef]
- Austin, G.; Yu, K. Characteristics of wastewater. In Constructed Wetlands and Sustainable Development; Routledge & CRC Press: New York, NY, USA, 2018. [Google Scholar]
- Khan, D.; Kumar, A.; Samadder, S.R. Impact of socioeconomic status on municipal solid waste generation rate. Waste Manag. 2016, 49, 15–25. [Google Scholar] [CrossRef]
- Wilson, S.R.; Patrick, M.; Pierce, A. Statistics Reference Online; Wiley StatsRef: Hoboken, NJ, USA, 2014. [Google Scholar]
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Getis, A.; Ord, J.K. The analysis of spatial association by use of distance statistics. Geogr. Anal. 2010, 24, 189–206. [Google Scholar] [CrossRef]
- Ord, J.K.; Getis, A. Local spatial autocorrelation statistics: Distributional issues and an application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Gaile, G.L.; Willmott, C. Spatial Statistics and Models; Springer Science & Business Media: Berlin, Germany, 1984. [Google Scholar]
- Schuenemeyer, J.H.; Clark, W.A.V.; Hosking, P.L. Statistical methods for geographers. J. Am. Stat. Assoc. 1988, 83, 575. [Google Scholar]
- Getis, A.; Aldstadt, J. Constructing the spatial weights matrix using a local statistic. Geogr. Anal. 2004, 36, 90–104. [Google Scholar] [CrossRef]
- Conley, T.G. GMM estimation with cross sectional dependence. J. Econom. 1999, 92, 1–45. [Google Scholar] [CrossRef]
- Das, M.; Ghosh, S.K. A cost-efficient approach for measuring Moran’s index of spatial autocorrelation in geostationary satellite data. In Proceedings of the International Geoscience and Remote Sensing Symposium (IGARSS), Beijing, China, 10–15 July 2016. [Google Scholar]
- Li, L.; Zhou, Y.; Jin, F. Spatial autocorrelation analysis of total fertility rate based on different spatial weight matrices. J. Geomatics 2015, 5, 62–64. [Google Scholar]
- Elhorst, J.P. Specification and estimation of spatial panel data models. Int. Reg. Sci. Rev. 2003, 26, 244–268. [Google Scholar]
- Horne, B.D.; Joy, E.A.; Hofmann, M.G.; Gesteland, P.H.; Cannon, J.B.; Lefler, J.S.; Blagev, D.P.; Kent Korgenski, E.; Torosyan, N.; Hansen, G.I. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am. J. Respir. Crit. Care Med. 2018, 198, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A. Particulate matter air pollution and cardiovascular disease. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Soto-Martinez, M.E. Strategies to minimize the effects of air pollution on respiratory health. Pediatr. Pulmonol. 2019, 48, 996–999. [Google Scholar]
- Mhimbira, F.A.; Cuevas, L.E.; Dacombe, R.; Mkopi, A.; Sinclair, D. Interventions to increase tuberculosis case detection at primary healthcare or community-level services. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Research Subjects | Years | Data Resources |
|---|---|---|---|
| Outpatient visits | 31 provinces | 2006–2017 | CHSY, CHFPSY |
| Inpatient visits | 31 provinces | 2006–2017 | CHSY, CHFPSY |
| Water pollution | 31 provinces | 2006–2017 | CSY |
| Air pollution | 31 provinces | 2006–2017 | CSY |
| solid wastes | 31 provinces | 2006–2017 | CSY |
| PM2.5 concentrations | 31 provinces | 2006–2017 | CSY |
| Domestic waste disposal | 31 provinces | 2006–2017 | CSY |
| Per capita GDP | 31 provinces | 2006–2017 | CSY |
| Urban population | 31 provinces | 2006–2017 | CSY |
| Population aged 0–14 | 31 provinces | 2006–2017 | CSY |
| Population aged above 65 | 31 provinces | 2006–2017 | CSY |
| Education level | 31 provinces | 2006–2017 | CSY |
| Variable Type | Variable Name | Measurement | Code | Description |
|---|---|---|---|---|
| Dependent variable | Medical care | Outpatient visits per capita | OV | Number of the outpatient visits divided by the population |
| Inpatient visits per capital | IV | Number of the inpatient visits divided by the population | ||
| Independent variables | Environmental pollution | Effluent discharge | ED | Amount of effluent discharge divided by the population |
| Waste gas emission | GE | Amount of gas emission divided by the population | ||
| Solid discharge | SD | Amount of solid discharge divided by the population | ||
| Average PM2.5 concentration | PM2.5 | The average values of PM2.5 concentrations in the form of the natural logarithm | ||
| Household waste disposal (%) | HWD | The ratio of household waste disposal | ||
| Control variables | Socioeconomic conditions | Gross domestic product per capita | GDP | Real gross domestic product divided by the population |
| Demographic conditions | Total population | TP | The total population of all counties | |
| The proportion of the urban population (%) | PUP | A total population divided by urban population | ||
| The proportion of the population aged 0–14 | 0–14 | A total population divided by population aged 0–14 | ||
| The proportion of the population aged above 65 | Above 65 | A total population divided by population aged above 65 | ||
| The proportion of the population with a higher education level | HD | A total population divided by population with an associate degree or higher |
| Variable | Obs 1 | Mean | Std. Dev. 2 | Min. 3 | Max. 4 | Units |
|---|---|---|---|---|---|---|
| OV 5 | 372 | 7.76 | 11.68 | 0.17 | 87.06 | Times/population |
| IV | 372 | 0.19 | 0.27 | 0.19 | 14.733 | Times/population |
| ED | 372 | 83.32 | 128.21 | 1.16 | 1078.45 | Amount/population |
| GE | 372 | 0.06 | 0.10 | 0.00 | 0.89 | Amount/population |
| PM2.5 | 372 | 3.58 | 0.51 | 1.94 | 4.44 | μg/m3 |
| SD | 372 | 4.04 | 7.35 | 0.02 | 68.79 | Amount/population |
| HWD | 372 | 0.80 | 0.20 | 0.10 | 1.00 | % |
| GDP | 372 | 10.42 | 0.60 | 8.66 | 11.77 | Yuan |
| TP | 372 | 17.22 | 1.35 | 12.61 | 21.24 | Person |
| PUP | 372 | 0.53 | 0.14 | 0.23 | 0.90 | % |
| 0–14 | 372 | 0.17 | 0.04 | 0.07 | 0.27 | % |
| 65 | 372 | 0.09 | 0.02 | 0.04 | 0.14 | % |
| HD | 372 | 0.12 | 0.07 | 0.00 | 0.47 | % |
| Year | Effluent Discharge | Waste Gas Emission | Solid Discharge | PM2.5 Concentration | Household Waste Disposal |
|---|---|---|---|---|---|
| 2006 | 0.198 | 0.235 *,1,2 | 0.277 ** | 0.499 *** | 0.110 |
| 2007 | 0.196 | 0.237 * | 0.264 * | 0.504 *** | 0.277 ** |
| 2008 | 0.201 * | 0.215 * | 0.277 ** | 0.456 *** | 0.365 *** |
| 2009 | 0.208 * | 0.205 * | 0.288 ** | 0.453 *** | 0.316 ** |
| 2010 | 0.245 * | 0.171 | 0.244 * | 0.425 *** | 0.206 * |
| 2011 | 0.236 * | 0.240 * | 0.236 * | 0.498 *** | 0.080 |
| 2012 | 0.252 * | 0.221 * | 0.226 * | 0.446 *** | 0.188 |
| 2013 | 0.270 * | 0.168 | 0.218 * | 0.498 *** | 0.216 * |
| 2014 | 0.246 * | 0.242 * | 0.261 ** | 0.416 *** | 0.271 ** |
| 2015 | 0.234 * | 0.269 * | 0.281 * | 0.492 *** | 0.264 ** |
| 2016 | 0.257 * | 0.148 | 0.247 * | 0.507 *** | 0.208 * |
| 2017 | 0.269 * | 0.088 | 0.281 ** | 0.452 *** | 0.279 ** |
| Variable | Ln (OV) 2 | Ln (IV) | ||||
|---|---|---|---|---|---|---|
| Matrix One | Matrix Two | Matrix Three | Matrix One | Matrix Two | Matrix Three | |
| Ln (GE) | 0.195 * 1,3 (2.14) | 0.137 (1.71) | 0.350 *** (3.93) | 0.017 (0.61) | 0.041 (1.39) | −0.041 (−1.52) |
| Ln (ED) | 0.575 *** (5.12) | 0.775 *** (9.87) | 0.373 ** (2.63) | 0.114 ** (2.90) | 0.036 (0.77) | 0.027 (0.62) |
| Ln (SD) | 0.126 * (2.13) | 0.132 ** (2.33) | −0.013 (−0.21) | −0.007 (−0.34) | −0.020 (−1.01) | 0.013 (0.70) |
| Ln (PM2.5) | −0.004 (0.330) | −0.002 (−0.73) | −0.001 (−0.15) | 0.003 (1.50) | −0.002 (−1.03) | −0.001 (−0.64) |
| HWD | 0.005 ** (2.75) | 0.003 * (1.90) | 0.005 * (2.50) | 0.001 ** (2.61) | 0.002 *** (3.78) | 0.001 * (2.13) |
| Ln (TP) | 0.652 *** (5.21) | 0.257 *** (3.44) | 0.788 *** (4.72) | 0.868 *** (14.08) | −0.004 (−0.14) | 1.017 *** (17.89) |
| PUP | 2.007 ** (2.80) | 1.614 ** (2.34) | 3.862 *** (3.51) | 0.891 ** (2.75) | 1.176 *** (3.36) | 0.851 ** (2.71) |
| 0–14 | 3.160 * (1.99) | 3.436 * (2.18) | 4.505 * (2.46) | 1.023 * (1.97) | 0.588 (1.01) | 1.021 (1.76) |
| Above 65 | 0.103 (0.04) | 4.766 * (2.08) | 4.646 (1.82) | 3.154 *** (4.04) | 1.408 (1.81) | 3.263 *** (4.31) |
| Ln (GDP) | −0.202 (−1.20) | 0.452 ** (3.02) | 0.091 (−1.55) | 0.263 *** (3.82) | 0.559 *** (9.44) | 0.448 *** (6.55) |
| HD | −1.047 (−1.21) | −0.868 (−1.06) | 1.683 (−1.55) | 0.048 (0.16) | 0.524 (1.57) | −0.179 (−0.54) |
| W × Ln (GE) | 0.251 (1.79) | −0.051 (−0.30) | 0.146 (0.98) | −0.057 (−1.49) | −0.115 * (−2.21) | −0.042 (−0.93) |
| W × Ln (ED) | 0.229 (1.64) | 0.888 *** (4.16) | 0.207 (0.69) | 0.037 (0.60) | 0.085 (0.53) | −0.029 (−0.29) |
| W × Ln (SD) | 0.050 (0.49) | −0.223 (−0.88) | 0.005 (0.03) | −0.024 (−0.76) | 0.053 (0.61) | 0.136 ** (2.72) |
| W × (PM2.5) | 0.006 (0.99) | 0.014 (1.68) | −0.005 (−0.66) | 0.006 * (2.25) | 0.003 (1.14) | 0.000 (0.08) |
| W × HWD | −0.005 (−1.25) | −0.013 * (−1.92) | −0.031 *** (−5.21) | −0.000 (−0.22) | −0.005 * (−1.99) | −0.001 (−0.76) |
| W × Ln (TP) | −0.684 *** (−5.37) | −0.226 ** (−2.82) | −0.795 *** (−4.74) | −0.870 *** (−14.11) | 0.008 (0.31) | −1.013 (−0.76) |
| W × PUP | −3.570 ** (−2.77) | −0.190 (−0.07) | −14.007 *** (−5.80) | −1.939 *** (−3.70) | −0.254 (−0.20) | −2.230 ** (−2.75) |
| W × 0–14 | 2.324 (0.94) | 2.131 (0.46) | −7.500 (−1.89) | −2.371 ** (−2.65) | −4.752 (−1.80) | −0.802 (−0.56) |
| W × Above 65 | −0.892 (−0.23) | −24.475 *** (−3.54) | −8.522 (−1.52) | −1.686 (−1.35) | −1.901 (−0.81) | −0.922 (−0.54) |
| W × Ln (GDP) | 0.890 *** (3.59) | 1.735 *** (5.16) | 2.179 *** (6.32) | 0.082 (0.84) | −0.315 (−1.49) | −0.044 (−0.39) |
| W × HD | 1.976 (1.21) | −1.109 (−0.32) | 7.338 ** (2.66) | −1.047 * (−2.11) | −2.098 (−1.85) | −1.613 * (−1.98) |
| 0.5356 *** | 0.699 *** | 0.4977 *** | 0.7454 *** | 0.8215 *** | 0.7493 *** | |
| LLR | −171.8192 | −139.5325 | −166.9149 | 291.9434 | 247.1688 | 270.2405 |
| R2 | 0.8225 | 0.8380 | 0.7712 | 0.9390 | 0.2128 | 0.9386 |
| Obs | 372 | 372 | 372 | 372 | 372 | 372 |
| Variable | Ln (OV) 2 | Ln (IV) | ||||
|---|---|---|---|---|---|---|
| Matrix One | Matrix Two | Matrix Three | Matrix One | Matrix Two | Matrix Three | |
| Ln (GE) | 0.167 (1.82) | 0.150 (1.77) | 0.350 ***,1,3 (3.81) | 0.004 (0.906) | 0.028 (0.83) | −0.057 (−1.89) |
| Ln (ED) | 0.583 *** (5.40) | 0.738 *** (9.13) | 0.363 ** (2.60) | 0.151 ** (3.09) | 0.051 (0.77) | 0.021 (0.40) |
| Ln (SD) | 0.127 * (2.05) | 0.161 * (2.41) | −0.010 (−0.15) | −0.016 (−0.70) | −0.013 (−0.49) | 0.048 * (1.92) |
| Ln (PM2.5) | −0.003 (−0.90) | −0.001 (−0.29) | −0.001 (−0.32) | 0.001 (0.83) | −0.001 (−0.83) | −0.001 (−0.69) |
| HWD | 0.005 * (2.45) | 0.002 (1.22) | 0.002 (1.05) | 0.002 * (2.47) | 0.001 (1.74) | 0.001 (1.52) |
| Ln (TP) | 0.595 *** (5.38) | 0.252 *** (3.61) | 0.751 *** (4.88) | 0.796 *** (14.54) | −0.003 (−0.12) | 0.963 *** (18.23) |
| PUP | 1.560 * (2.06) | 1.690 * (2.10) | 2.593 * (2.38) | 0.478 (1.29) | 1.304 *** (3.20) | 0.489 (1.37) |
| 0–14 | 3.858 * (2.56) | 3.929 * (2.55) | 3.885 * (2.00) | 0.502 (0.83) | −0.106 (−0.13) | 1.005 (1.31) |
| Above 65 | 0.114 (0.05) | 2.093 (1.32) | 4.179 (1.69) | 3.432 *** (4.23) | 1.305 (1.64) | 3.682 *** (4.43) |
| Ln (GDP) | 0.067 (0.43) | 0.313 * (2.06) | 0.328 (1.37) | 0.352 *** (5.49) | 0.585 *** (8.66) | 0.515 *** (6.47) |
| HD | −0.781 (−0.84) | −1.013 (−1.11) | −1.020 (−0.95) | −0.283 (−0.78) | 0.217 (0.52) | −0.591 (−1.51) |
| Variable | Ln (OV) 2 | Ln (IV) | ||||
|---|---|---|---|---|---|---|
| Matrix One | Matrix Two | Matrix Three | Matrix One | Matrix Two | Matrix Three | |
| Ln (GE) | 0.288 (1.17) | −0.516 (−0.93) | −0.064 (−0.24) | −0.162 (−1.36) | −0.460 (−1.46) | −0.279 (−1.76) |
| Ln (ED) | 0.156 (0.70) | −1.100 (−1.48) | −0.060 (−0.11) | 0.429 (1.85) | 0.556 (0.54) | −0.059 (−0.14) |
| Ln (SD) | −0.040 (−0.22) | −1.072 (−1.25) | 0.002 (0.01) | −0.108 (−1.15) | 0.193 (0.39) | 0.559 **,1,3 (2.66) |
| Ln (PM2.5) | 0.008 (−0.50) | 0.040 (1.41) | −0.009 (−0.66) | −0.014 (−1.10) | 0.010 (0.75) | −0.001 (−0.17) |
| HWD | −0.004 (−0.50) | −0.037 (−1.48) | −0.053 *** (−3.83) | 0.003 (0.68) | −0.022 (−1.33) | −0.001 (−0.09) |
| Ln (TP) | −0.663 *** (−5.54) | −0.132 (−1.05) | −0.767 *** (−4.83) | −0.801 *** (−13.85) | 0.036 (0.59) | −0.947 *** (−15.97) |
| PUP | −4.942 (−1.91) | 3.227 (0.760) | −22.985 *** (−5.23) | −4.592 ** (−2.56) | 4.064 (0.55) | −6.076 * (−2.13) |
| 0–14 | 7.582 (1.54) | 14.440 (0.82) | −10.111 (−1.31) | −6.135 * (−1.90) | −22.906 (−1.54) | 0.012 (0.00) |
| Above 65 | −1.702 (−0.25) | −9.276 ** (−2.57) | −12.119 (−1.20) | 2.408 (0.60) | −4.986 (−0.40) | 5.717 (0.87) |
| Ln (GDP) | 1.539 *** (−5.54) | 4.654 ** (3.15) | 4.179 *** (5.60) | 1.002 *** (3.96) | 0.854 (0.70) | 1.085 * (2.48) |
| HD | 2.784 (0.82) | −5.951 (−0.49) | 12.582 * (2.43) | −3.659 (−1.90) | −9.447 (−1.22) | −6.600 * (−1.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, N.; Mao, Y. Spatial Effects of Environmental Pollution on Healthcare Services: Evidence from China. Int. J. Environ. Res. Public Health 2021, 18, 1784. https://doi.org/10.3390/ijerph18041784
Zhang N, Mao Y. Spatial Effects of Environmental Pollution on Healthcare Services: Evidence from China. International Journal of Environmental Research and Public Health. 2021; 18(4):1784. https://doi.org/10.3390/ijerph18041784
Chicago/Turabian StyleZhang, Ning, and Ying Mao. 2021. "Spatial Effects of Environmental Pollution on Healthcare Services: Evidence from China" International Journal of Environmental Research and Public Health 18, no. 4: 1784. https://doi.org/10.3390/ijerph18041784
APA StyleZhang, N., & Mao, Y. (2021). Spatial Effects of Environmental Pollution on Healthcare Services: Evidence from China. International Journal of Environmental Research and Public Health, 18(4), 1784. https://doi.org/10.3390/ijerph18041784