
Communication Experiences in Primary Healthcare with Refugees and Asylum Seekers: A Literature Review and Narrative Synthesis

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
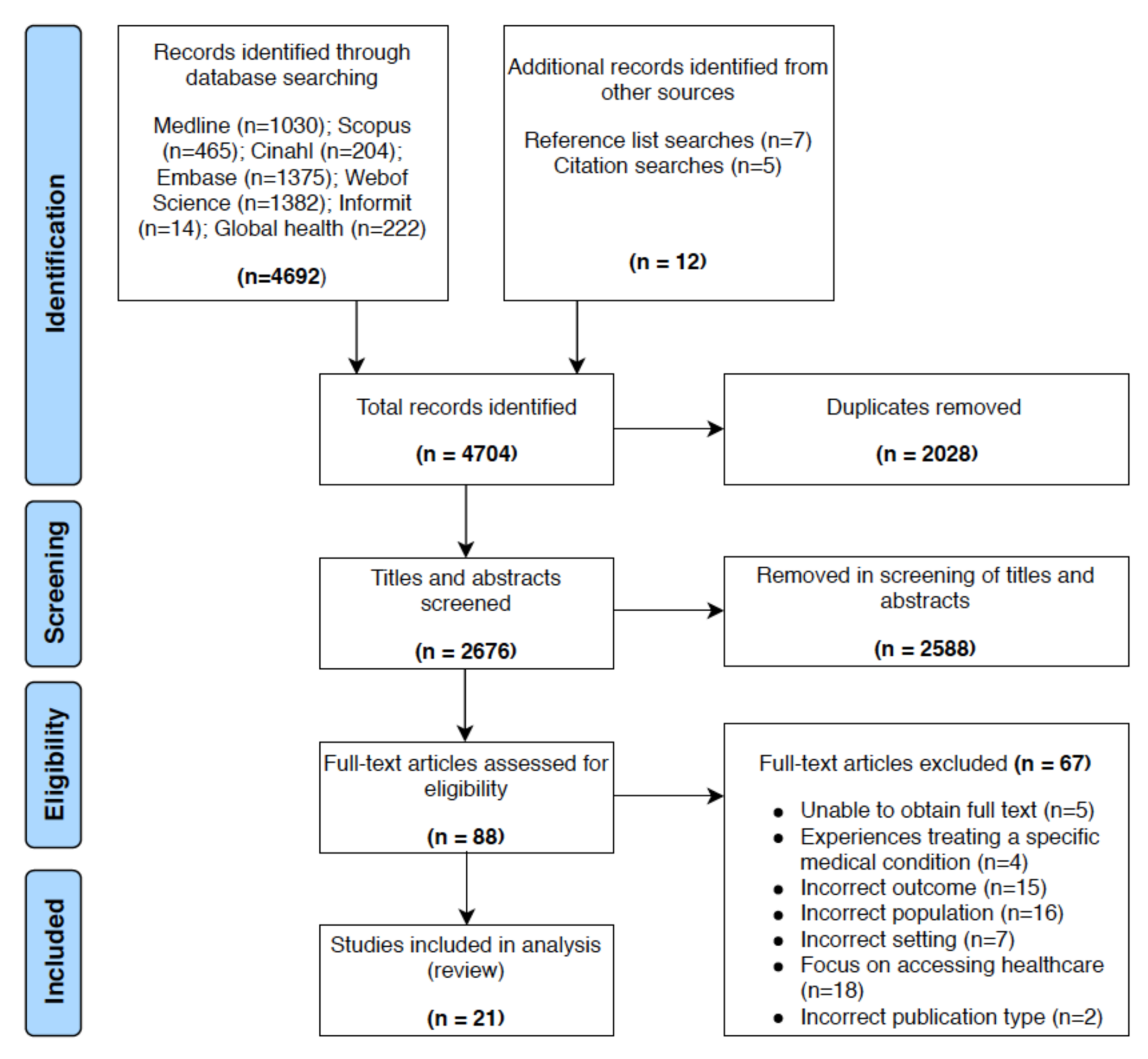
2.1. Search Strategy
2.2. Selection Criteria
2.2.1. Population
2.2.2. Study Design
2.3. Data Extraction and Quality Assessment
2.4. Data Analysis and Synthesis
3. Results
3.1. Linguistic Barriers
3.1.1. Qualitative Studies
“The times that I have needed it they have been–appointments have been booked well in advance. How do you book an interpreter when someone rings up at lunchtime and sees you two hours later for something that is minor or insignificant?”—HCP [34]
“Sometimes it is okay, but in the majority of the cases it is better with the authorized interpreters since they are more familiar with the medical terminology. So it is always a poorer consultation. It is typically the family being used and I feel they shouldn’t be there at all”—HCP [33]
“Sometimes you will see a client who does not want to work with an interpreter, especially in small communities there are limited numbers of interpreters from that community. The client may know the interpreter or know people who know the interpreter and they will worry about confidentiality. That causes a lot of embarrassment for women…”—HCP [38]
“When you get a translator and the translator doesn’t really get you the translation in details. Some of them just talk and talk and then when it comes to the translator, he can’t put the words the [right] way...”—patient [24]
“Inevitably there were misunderstandings during her GP consultations and, on one occasion, her son who had diarrhoea was prescribed medication for constipation...”—patient [35]
3.1.2. Quantitative Studies
3.2. Clinician Cues
“When you sit with a doctor and you hear kind words, that has an influence on your nerves, on your body. You start feeling better, healthier, than when the doctor is angry.”—patient [27]
“We don’t have anybody here. It is very important that the doctor is friendly.”—patient [28]
“I did not give him the medical file, because he was not interested. My expectation was somebody who will be open to me, like doctors in Africa.”—patient [26]
“That generalizing attitude is what still makes me angry.”—patient [26]
“To show that you are interested in the person, not only in the disease; to show that you want to know something about the context. Sometimes it is difficult to find time for it in a busy practice, but I see it is a worthwhile investment…”—HCP [27]
3.3. Cultural Understanding
“Give her a woman translator, so that she can be open to tell all the problems”—patient [24]
“Religion sometimes says it is good for you to have [a] female doctor if you are female”—patient [24]
“They have a different culture, so their cultural perception of symptoms and what they mean... trying to interpret the difference between a bloated abdomen and a painful abdomen, just becomes an impossible task...”—HCP [25]
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Declarations
Consent for Publication
Availability of Data and Materials
Abbreviations
Appendix A. Search Terms Used For Database Searches
- 1.
- Pop
- or.
- Asylum seek$
- or.
- (forced migrant$)
- or.
- (involuntary migrant$)
- or.
- Migrant$
- 2.
- AND
- or.
- Nurs$
- or.
- (General practi$)
- or.
- (community health centr$)
- or.
- (community clinic$)
- 3.
- AND
- or.
- Languag$
- or.
- Translat$
- or.
- Perception$
- or.
- Experienc$
- or.
- Attitude$
- or.
- View$
- or.
- Facilitat$
- or.
- Barrier$
- or.
- Challenge$
- or.
- Interact$
References
- UNHCR. Global Trends. Forced Displacement in 2018; UNHCR: Geneva, Switzerland, 2018; Available online: https://www.unhcr.org/globaltrends2018/ (accessed on 6 August 2019).
- UNHCR. Convention and Protocol Relating to the Status of Refugees; UNHCR: Geneva, Switzerland, 2010; Available online: https://www.unhcr.org/protection/basic/3b66c2aa10/convention-protocol-relating-status-refugees.html (accessed on 29 March 2019).
- Milosevic, D.; Cheng, I.-H.; Smith, M.M. The NSW Refugee Health Service: Improving refugee access to primary care. Aust. Fam. Physician 2012, 41, 147. [Google Scholar]
- Yelland, J.; Riggs, E.; Wahidi, S.; Fouladi, F.; Casey, S.; Szwarc, J. How do Australian maternity and early childhood health services identify and respond to the settlement experience and social context of refugee background families? BMC Pregnancy Childbirth 2014, 14, 348. [Google Scholar] [CrossRef]
- Eckstein, B. Primary care for refugees. Am. Fam. Physician 2011, 83, 429–436. [Google Scholar]
- Harris, M.F. Integration of refugees into routine primary care in NSW, Australia. Public Health Res. Pract. 2018, 28, e2811802. [Google Scholar] [CrossRef]
- Cheng, I.-H.; Drillich, A.; Schattner, P. Refugee experiences of general practice in countries of resettlement: A literature review. Br. J. Gen. Pract. 2015, 65, e171–e176. [Google Scholar] [CrossRef]
- Starfield, B. Primary Care: Balancing Health Needs, Services, and Technology; Oxford University Press: Oxford, MS, USA, 1998. [Google Scholar]
- Robertshaw, L.; Dhesi, S.; Jones, L.L. Challenges and facilitators for health professionals providing primary healthcare for refugees and asylum seekers in high-income countries: A systematic review and thematic synthesis of qualitative research. BMJ Open 2017, 7, e015981. [Google Scholar] [CrossRef]
- Simpson, M.; Buckman, R.; Stewart, M.; Maguire, P.; Lipkin, M.; Novack, D. Doctor-patient communication: The Toronto consensus statement. BMJ Br. Med. J. 1991, 303, 1385. [Google Scholar] [CrossRef]
- Mercer, S.W.; Neumann, M.; Wirtz, M.; Fitzpatrick, B.; Vojt, G. General practitioner empathy, patient enablement, and patient-reported outcomes in primary care in an area of high socio-economic deprivation in Scotland—A pilot prospective study using structural equation modeling. Patient Educ. Couns. 2008, 73, 240–245. [Google Scholar] [CrossRef]
- Ong, L.M.L.; De Haes, J.C.J.M.; Hoos, A.M.; Lammes, F.B. Doctor-patient communication: A review of the literature. Soc. Sci. Med. 1995, 40, 903–918. [Google Scholar] [CrossRef]
- Brandenberger, J.; Tylleskär, T.; Sontag, K.; Peterhans, B.; Ritz, N. A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries—The 3C model. BMC Public Health 2019, 19, 755. [Google Scholar] [CrossRef]
- Wanzer, M.B.; Booth-Butterfield, M.; Gruber, K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Commun. 2004, 16, 363–384. [Google Scholar] [CrossRef]
- Korsch, B.M.; Gozzi, E.K.; Francis, V. Gaps in doctor-patient communication: I. Doctor-patient interaction and patient satisfaction. Pediatrics 1968, 42, 855–871. [Google Scholar]
- King, A.; Hoppe, R.B. “Best practice” for patient-centered communication: A narrative review. J. Grad. Med. Educ. 2013, 5, 385–393. [Google Scholar] [CrossRef]
- UN. United Nations Regional Groups of Member States 2014; UN: 2014. Available online: http://www.un.org/depts/DGACM/RegionalGroups.shtml (accessed on 6 August 2019).
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2011; Volume 5. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M. Guidance on the conduct of narrative synthesis in systematic reviews. A Product from ESRC methods Program Version 1. Comput. Sci. 2006, 1. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Hacker, K.; Anies, M.; Folb, B.L.; Zallman, L. Barriers to health care for undocumented immigrants: A literature review. Risk Manag. Healthc. Policy 2015, 8, 175–183. [Google Scholar] [CrossRef]
- Institute TJB. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews. The Joanna Briggs Institute Critical Appraisal tools. 2017. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 12 June 2019).
- Adair, R.; Nwaneri, M.O.; Barnes, N. Health care access for Somali refugees: Views of patients, doctors, nurses. Am. J. Health Behav. 1999, 23, 286–292. [Google Scholar] [CrossRef]
- Carroll, J.; Epstein, R.; Fiscella, K.; Gipson, T.; Volpe, E.; Jean-Pierre, P. Caring for Somali women: Implications for clinician-patient communication. Patient Educ. Couns. 2007, 66, 337–345. [Google Scholar] [CrossRef]
- Farley, R.; Askew, D.; Kay, M. Caring for refugees in general practice: Perspectives from the coalface. Aust. J. Prim. Health 2014, 20, 85–91. [Google Scholar] [CrossRef]
- Feldmann, C.T.; Bensing, J.M.; De Ruijter, A.; Boeije, H.R. Somali Refugees’ Experiences with their General Practitioners: Frames of Reference and Critical Episodes. Int. J. Migr. Health Soc. Care 2006, 2, 28–40. [Google Scholar] [CrossRef]
- Feldmann, C.T.; Bensing, J.M.; De Ruijter, A. Worries are the mother of many diseases: General practitioners and refugees in the Netherlands on stress, being ill and prejudice. Patient Educ. Couns. 2007, 65, 369–380. [Google Scholar] [CrossRef]
- Feldmann, C.T.; Bensing, J.M.; De Ruijter, A.; Boeije, H.R. Afghan refugees and their general practitioners in The Netherlands: To trust or not to trust? Sociol. Health Illn. 2007, 29, 515–535. [Google Scholar] [CrossRef]
- Feldmann, T. What do refugees and general practitioners say about medically unexplained physical symptoms? Medical errors undermine trust in the GP. Huisarts Wet. 2007, 50, 381–384. [Google Scholar]
- Grut, L.; Tingvold, L.; Hauff, E. General practitioners’ experiences with refugee patients: A qualitative study. Tidsskr. Nor. Laegeforen. 2006, 126, 1318–1320. [Google Scholar]
- Gurnah, K.; Khoshnood, K.; Bradley, E.; Yuan, C. Lost in translation: Reproductive health care experiences of Somali Bantu women in Hartford, Connecticut. J. Midwifery Womens Health 2011, 56, 340–346. [Google Scholar] [CrossRef]
- Harris, M.; Zwar, N. Refugee health. Aust. Fam. Physician 2005, 34, 825–829. [Google Scholar]
- Jensen, N.K.; Norredam, M.; Priebe, S.; Krasnik, A. How do general practitioners experience providing care to refugees with mental health problems? A qualitative study from Denmark. BMC Fam. Pract. 2013, 14, 1–9. [Google Scholar] [CrossRef]
- Johnson, D.R.; Ziersch, A.M.; Burgess, T. I don’t think general practice should be the front line: Experiences of general practitioners working with refugees in South Australia. Aust. N. Z. Health Policy 2008, 5, 20. [Google Scholar] [CrossRef]
- MacFarlane, A.; Dzebisova, Z.; Karapish, D.; Kovacevic, B.; Ogbebor, F.; Okonkwo, E. Arranging and negotiating the use of informal interpreters in general practice consultations: Experiences of refugees and asylum seekers in the west of Ireland. Soc. Sci. Med. 2009, 69, 210–214. [Google Scholar] [CrossRef]
- MacFarlane, A.; Glynn, L.G.; Mosinkie, P.I.; Murphy, A.W. Responses to language barriers in consultations with refugees and asylum seekers: A telephone survey of Irish general practitioners. BMC Fam. Pract. 2008, 9, 6. [Google Scholar] [CrossRef]
- Manchikanti, P.; Cheng, I.H.; Advocat, J.; Russell, G. Acceptability of general practice services for Afghan refugees in south-eastern Melbourne. Aust. J. Prim. Health 2017, 23, 87–91. [Google Scholar] [CrossRef]
- Mengesha, Z.B.; Perz, J.; Dune, T.; Ussher, J. Talking about sexual and reproductive health through interpreters: The experiences of health care professionals consulting refugee and migrant women. Sex. Reprod. Healthc. 2018, 16, 199–205. [Google Scholar] [CrossRef]
- O’Donnell, C.A.; Higgins, M.; Chauhan, R.; Mullen, K. Asylum seekers’ expectations of and trust in general practice: A qualitative study. Br. J. Gen. Pract. 2008, 58, e1–e11. [Google Scholar] [CrossRef]
- O’Donnell, C.A.; Higgins, M.; Chauhan, R.; Mullen, K. “They think we’re OK and we know we’re not”. A qualitative study of asylum seekers’ access, knowledge and views to health care in the UK. BMC Health Serv. Res. 2007, 7, 75. [Google Scholar] [CrossRef]
- Pottie, K. Misinterpretation: Language proficiency, recent immigrants, and global health disparities. Can. Fam. Physician 2007, 53, 1899–1901. [Google Scholar]
- Svenberg, K.; Skott, C.; Lepp, M. Ambiguous expectations and reduced confidence: Experience of somali refugees encountering Swedish health care. J. Refug. Stud. 2011, 24, 690–705. [Google Scholar] [CrossRef]
- Karliner, L.S.; Jacobs, E.A.; Chen, A.H.; Mutha, S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv. Res. 2007, 42, 727–754. [Google Scholar] [CrossRef]
- Brisset, C.; Leanza, Y.; Laforest, K. Working with interpreters in health care: A systematic review and meta-ethnography of qualitative studies. Patient Educ. Couns. 2013, 91, 131–140. [Google Scholar] [CrossRef]
- White, J.; Plompen, T.; Osadnik, C.; Tao, L.; Micallef, E.; Haines, T. The experience of interpreter access and language discordant clinical encounters in Australian health care: A mixed methods exploration. Int. J. Equity Health 2018, 17, 151. [Google Scholar] [CrossRef]
- Vaughn, L.M.; Jacquez, F.; Bakar, R.C. Cultural health attributions, beliefs, and practices: Effects on healthcare and medical education. Open Med. Educ. J. 2009, 2. [Google Scholar] [CrossRef]
- Street, R.L., Jr.; Makoul, G.; Arora, N.K.; Epstein, R.M. How does communication heal? Pathways linking clinician–patient communication to health outcomes. Patient Educ. Couns. 2009, 74, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.M.; Franks, P.; Fiscella, K.; Shields, C.G.; Meldrum, S.C.; Kravitz, R.L. Measuring patient-centered communication in patient–physician consultations: Theoretical and practical issues. Soc. Sci. Med. 2005, 61, 1516–1528. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.M.; Franks, P.; Shields, C.G.; Meldrum, S.C.; Miller, K.N.; Campbell, T.L. Patient-centered communication and diagnostic testing. Ann. Fam. Med. 2005, 3, 415–421. [Google Scholar] [CrossRef]
- Suphanchaimat, R.; Kantamaturapoj, K.; Putthasri, W.; Prakongsai, P. Challenges in the provision of healthcare services for migrants: A systematic review through providers’ lens. BMC Health Serv. Res. 2015, 15, 390. [Google Scholar] [CrossRef]
- Scheppers, E.; Van Dongen, E.; Dekker, J.; Geertzen, J.; Dekker, J. Potential barriers to the use of health services among ethnic minorities: A review. Fam. Pract. 2006, 23, 325–348. [Google Scholar] [CrossRef]
- Wensing, M.; Jung, H.P.; Mainz, J.; Olesen, F.; Grol, R. A systematic review of the literature on patient priorities for general practice care. Part 1: Description of the research domain. Soc. Sci. Med. 1998, 47, 1573–1588. [Google Scholar] [CrossRef]
- Little, J.M. Humanistic medicine or values-based medicine… what’s in a name? Med. J. Aust. 2002, 177, 319–321. [Google Scholar] [CrossRef]
- Pellegrino, E.D. Humanism and the Physician; University of Tennessee: Knoxville, TN, USA, 1979. [Google Scholar]
- Rider, E.A.; Gilligan, M.C.; Osterberg, L.G.; Litzelman, D.K.; Plews-Ogan, M.; Weil, A.B. Healthcare at the Crossroads: The Need to Shape an Organizational Culture of Humanistic Teaching and Practice. J. Gen. Intern. Med. 2018, 33, 1092–1099. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country | Population (Service Users) | Setting (Service Provider/Setting) | Number | Data Collection Method | Analysis Methodology | Quality Score |
|---|---|---|---|---|---|---|---|---|
| Adair et al. [23] | 1999 | United States of America | Refugees (Somali) | Primary care clinic—both doctors and nurses | 38 patients, 6 nurses, 32 doctors | Refugees—semi-structured telephone interviews Medical professional-survey questions | Quantitative analysis | 8 |
| Carroll et al. [24] | 2007 | United States of America | Refugee women (Somali) | Primary care provider | 34 refugees | Refugees—in depth interviews | Grounded theory | 9 |
| Farley et al. [25] | 2014 | Australia | Newly arrived refugees | General Practitioners, nurses, admin staff | 20 GPs b, 5 nurse, 11 admin staff | HCP c—focus groups and semi-structured interview | Inductive thematic analysis | 9 |
| Feldmann et al. [26] | 2006 | Netherlands | Refugees (Somali) | General Practitioners | 36 refugees | Refugees—in depth interviews | Thematic analysis | 7 |
| Feldmann et al. [27] | 2007 | Netherlands | Refugees (Afghan/Somali) | General Practitioners | 66 Refugees, 24 GPs | Refugees—in depth interviews GPs—semi structured interviews | Thematic analysis | 7 |
| Feldmann et al. [28] | 2007 | Netherlands | Refugees (Afghan) | General Practitioners | 30 refugees | Refugees—in depth interviews | Thematic analysis | 7 |
| Feldmann et al. [29] | 2007 | Netherlands | Refugees (Afghan/Somali) | General Practitioners | 24 GPs | Interviews (refugees and GPs) | General narrative | 6 |
| Grut et al. [30] | 2006 | Norway | Refugees | General Practitioners | 12 GPs | GP—interviews | Narrative synthesis | 6 |
| Gurnah et al. [31] | 2011 | United States of America | Refugee women (Somali Bantu) | Reproductive health service | 14 refugees | Refugee—interviews, focus group and semi-structured survey | Thematic analysis | 8 |
| Harris [6] | 2018 | Australia | Refugees | General Practice | n/a a | n/a | Opinion article | 6 |
| Harris and Zwar [32] | 2005 | Australia | Refugees | General Practice | n/a | n/a | Opinion article | 6 |
| Jensen et al. [33] | 2013 | Denmark | Refugees | General Practitioners | 9 GPs | GP—semi structured interviews | Content analysis | 8 |
| Johnson et al. [34] | 2008 | Australia | Refugees | General Practitioners | 12 GPs | GP—semi structured interviews | Template analysis | 8 |
| MacFarlane et al. [35] | 2009 | Ireland | Refugees and asylum seekers | General Practitioners | 26 refugees | Refugees—semi-structured interviews | Thematic analysis | 9 |
| MacFarlane et al. [36] | 2008 | Ireland | Refugees and asylum seekers | General Practitioners | 56 GPs | GP—telephone survey | Quantitative analysis | 8 |
| Manchikanti et al. [37] | 2017 | Australia | Refugees (Afghan) | General Practice | 18 refugees | Refugees—in depth, semi-structured interviews | Thematic analysis | 8 |
| Mengesha et al. [38] | 2018 | Australia | Refugees | General Practitioners, nurses, midwife | 5 GPs, 8 nurses, 1 midwife | HCP—semi-structured interviews | Thematic analysis | 8 |
| O’Donnell et al. [39] | 2008 | Scotland (UK) | Asylum seekers | General Practice | 52 refugees | Asylum seekers—focus groups and semi-structured interview | Thematic analysis | 9 |
| O’Donnell et al. [40] | 2007 | Scotland (UK) | Asylum seekers | General Practice | 52 refugees | Asylum seekers—focus groups, one-on-one interviews or group interviews | Thematic analysis | 9 |
| Pottie [41] | 2007 | Canada | Refugees | Family physician | 1 refugee | Refugee—case report | 5 | |
| Svenberg et al. [42] | 2011 | Sweden | Refugees (Somali) | General Practice | 20 refugees | Refugee—interviews | hermeneutic approach | 7 |
| Author | Study Aims and Objectives | Outcomes Measures | Study Outcomes/Conclusions |
|---|---|---|---|
| Adair et al. [23] | To identify barriers to healthcare access perceived by a group of refugees from Somalia and by the doctors and nurses providing care for them. | Somali and HCPa responses to questions regarding transportation to clinic, payment for medical care, availability of interpreters and satisfaction with the level of communication achieved, comfort with being examined, and obtaining of medical care at multiple clinics. | Nurses and doctors who provide care for these patients and are quite familiar with their demographic characteristics but were inaccurate in predicting how they felt about access to care. |
| Carroll et al. [24] | To identify characteristics associated with favourable treatment in receipt of preventive healthcare services, from the perspective of resettled African refugee women. | African refugee women’s response to questions about positive and negative experiences with primary healthcare services, beliefs about respectful vs. disrespectful treatment, experiences of racism, prejudice or bias, and ideas about removing access barriers and improving healthcare services. | Qualities associated with a favorable healthcare experience included effective verbal and nonverbal communication, feeling valued and understood, availability of female interpreters and clinicians and sensitivity to privacy for gynecologic concerns. |
| Farley et al. [25] | To explore the experiences of general practices working within this new model, focusing on the barriers and enablers they continue to experience in providing care to refugees. | HCP responses to questions regarding barriers and enablers experienced when providing refugee healthcare and the resources providers felt would assist them in this task. | HCP working with refugees were enthusiastic and committed. The flexibility of the general practice setting enables providers to be innovative in their approach to caring for refugees. However, most practices continue to feel isolated as they search for solutions. |
| Feldmann et al. [28] | What are participants’ frames of reference, in respect of healthcare, and what is their definition of health? How did participants try to solve their health-related problems and what was their experience of the process? What personal and social resources were useful to them? How can we explain differences between participants’ experiences of healthcare and their interpretations of their experiences? | Refugee responses to questions regarding healthcare experiences, health-related problems and social and personal resources used in healthcare. | The elements that constituted positive and negative episodes and led to the development or undermining of trust were identified in the narratives. Negative experience tended to be interpreted as a sign of prejudice on the part of the HCP. |
| Feldmann et al. [26] | Which frames of reference play a role in the development over time of an individual refugee’s relationship with the Dutch healthcare system, in particular with the GP? | Refugee responses to questions regarding healthcare in country of origin and healthcare in the Netherlands. | For a positive relationship to develop, based on trust, GPs need to invest in the relationship with individual refugees, and avoid actions based on prejudice. |
| Feldmann et al. [29] | What do refugees and general practitioner say about physically inexplicable somatic complaints? | GPs’ perspectives on medically unexplained physical symptoms presented by their refugee patients, strategies to address this and problems assisting refugee patients. | The personal attitude and communication skills of the practitioner appear to be central to building or undermining trust. |
| Feldmann et al. [27] | To confront the views of refugee patients and general practitioners in the Netherlands, focusing on medically unexplained physical symptoms. | Refugees’ perspectives on health, illness and mental worries, their expectations from doctors and problems dealing with Dutch doctors. GPs’ perspectives on medically unexplained physical symptoms presented by their refugee patients, strategies to address this and problems assisting refugee patients. | GPs need to invest in the relationship with individual refugees, and avoid actions based on prejudice. |
| Grut et al. [30] | What challenges do the regular GPs experience in meeting these patients (refugee backgrounds)? | GP responses to questions about the challenges about meeting patients from refugee backgrounds. | GPs need more guidance materials to adapt to cultural challenges of treating refugee patients. |
| Gurnah et al. [31] | Explore the reproductive health experiences of Somali Bantu women in Connecticut, to identify potential barriers to care experienced by marginalized populations. | Somali women’s response to questions regarding perceptions of barriers to reproductive healthcare. | There was a lack of cultural fluency between patients and provider. There is a need for developing cultural competency in health care delivery. |
| Harris and Zwar [32] | n/ac | n/a | Refugees and asylum seekers come to Australia with a range of health problems related to their experience both overseas and in Australia. These problems need to be addressed in general practice, as should preventive care, which is often overlooked. |
| Harris [6] | n/a | n/a | Need for more integrated health service provision for people from refugee backgrounds, based on trust and communication. |
| Jensen et al. [33] | To investigate how general practitioners experience providing care to refugees with mental health problems. | GP responses to questions regarding delivery of care to immigrants in general, and delivery of care to patients with different immigration status. | Findings suggest that the development of conversational models for general practitioners including points to be aware of in the treatment of refugee patients may serve as a support in the management of refugee patients in primary care. |
| Johnson et al. [34] | To document the existence and nature of challenges for GPs who do this work in South Australia. To explore the ways in which these challenges could be reduced. To discuss the policy implications of this in relation to optimising the initial healthcare for refugees | GP responses to questions regarding challenges in providing initial care to refugees, suggestions on how to reduce challenges and ways to optimise initial healthcare for refugees. | GPs in this study were under-resourced, at both an individual GP level as well as a structural level, to provide effective initial care for refugees. |
| MacFarlane et al. [35] | Exploration of the elements of that experience in terms of their access to informal interpreters, choices and trade-offs about who to ask and negotiations with general practitioners about their use. | Asylum seeker responses to questions around use of health services; barriers and facilitators to accessing care; use of secondary care services; experience of translators; and previous experience of healthcare in responders’ country of origin. | Overall, service users experience a tension between the value of having someone present to act as their interpreter and the burden of work and responsibility to manage the language barrier. |
| MacFarlane et al. [36] | Quantify the need for language assistance in general practice consultations and examine the experience of, and satisfaction with, methods of language assistance utilised. | GPb responses to questions regarding the need for language assistance, their knowledge and use of professional interpreters and use of informal interpreters | The need for language assistance in consultations with refugees and asylum seekers in Irish general practice is high. General practitioners rely on informal responses. |
| Manchikanti et al. [37] | To investigate the acceptability of general practitioner (GP) services and understand what aspects of acceptability are relevant for Afghan refugees. | Refugees responses to questions regarding access to primary healthcare. | The findings reinforce the importance of tailoring healthcare delivery to the evolving needs and healthcare expectations of newly arrived and established refugees, respectively. |
| Mengesha et al. [38] | To explore the healthcare professional (HCP) experiences of working with interpreters when consulting refugee and migrant women who are not proficient in English around sexual and reproductive health issues. | HCP responses to questions regarding their recent encounters with refugee and migrant women not proficient in English language in sexual and reproductive healthcare. | Communication barriers in the provision of sexual reproductive health services to refugee and migrant women may not be avoided despite the use of interpreters. |
| O’Donnell et al. [39] | How migrants’ previous knowledge and experience of healthcare influences their current expectations of healthcare in a system relying on clinical generalists performing a gatekeeping role. | Asylum seekers response to health services; barriers and facilitators to accessing care; use of secondary care services; experience of translators; and previous experience of health care in responders’ country of origin. | HCPs need to be aware that experience of different systems of care can have an impact on individuals’ expectations in a GP- led system. |
| O’Donnell et al. [40] | To identify the barriers and facilitators to accessing healthcare, both medical and dental, and to explore the healthcare needs and beliefs of asylum seekers. | Asylum seeker responses to discussion around health services; barriers and facilitators to accessing care; use of secondary care services; use of dental services; experience of translators; and previous experience of healthcare in their own country. | The findings highlight issues of access to timely health care and the role of interpreters within the consultation. In addition to understanding the role of GPs and the UK health system. |
| Pottie [41] | n/a | n/a | The quality of patient care is improved with the use of professional interpreters. |
| Svenberg et al. [42] | To explore Somali refugees’ experience of their encounters with Swedish healthcare. | Refugees’ responses to questions regarding their and their family’s experience with meeting Swedish healthcare. | Interpretation of the findings suggests unfulfilled expectations of the medical encounters, resulting in disappointment among the Somali informants. This entailed a lack of trust and feelings of rejection and, ultimately, decisions to seek private medical care abroad. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, P.; Bernays, S.; Dolan, H.; Muscat, D.M.; Trevena, L. Communication Experiences in Primary Healthcare with Refugees and Asylum Seekers: A Literature Review and Narrative Synthesis. Int. J. Environ. Res. Public Health 2021, 18, 1469. https://doi.org/10.3390/ijerph18041469
Patel P, Bernays S, Dolan H, Muscat DM, Trevena L. Communication Experiences in Primary Healthcare with Refugees and Asylum Seekers: A Literature Review and Narrative Synthesis. International Journal of Environmental Research and Public Health. 2021; 18(4):1469. https://doi.org/10.3390/ijerph18041469
Chicago/Turabian StylePatel, Pinika, Sarah Bernays, Hankiz Dolan, Danielle Marie Muscat, and Lyndal Trevena. 2021. "Communication Experiences in Primary Healthcare with Refugees and Asylum Seekers: A Literature Review and Narrative Synthesis" International Journal of Environmental Research and Public Health 18, no. 4: 1469. https://doi.org/10.3390/ijerph18041469
APA StylePatel, P., Bernays, S., Dolan, H., Muscat, D. M., & Trevena, L. (2021). Communication Experiences in Primary Healthcare with Refugees and Asylum Seekers: A Literature Review and Narrative Synthesis. International Journal of Environmental Research and Public Health, 18(4), 1469. https://doi.org/10.3390/ijerph18041469