Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults




Abstract
1. Introduction
2. Materials and Methods
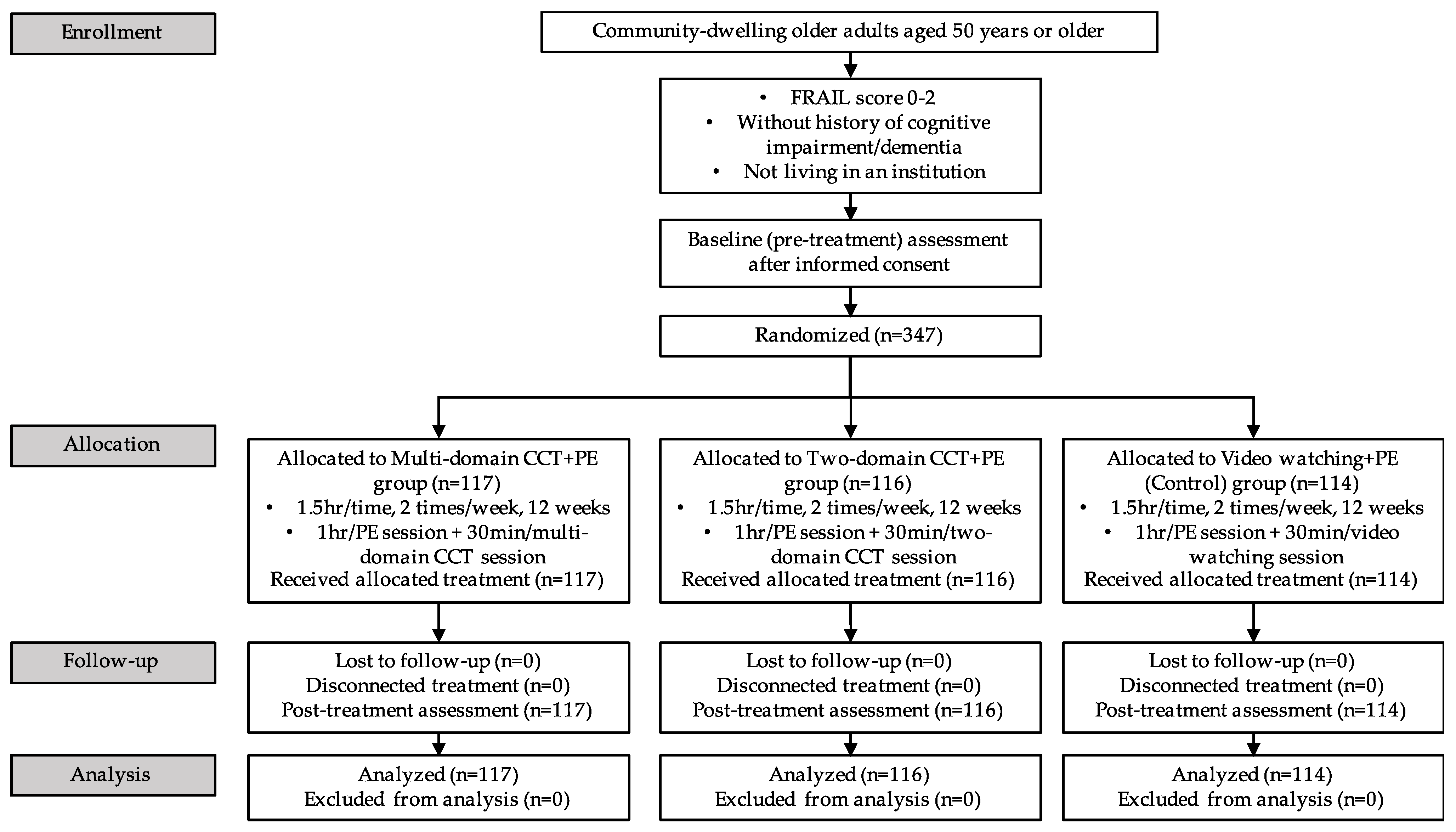
2.1. Study Design
2.2. Participants
2.3. Baseline Assessment and Randomization
2.4. Intervention
2.4.1. The Multi-Domain CCT + PE Group
2.4.2. The Two-Domain CCT + PE Group
2.4.3. Video Watching + PE (Control) Group
2.5. Outcome Measures
2.5.1. Frailty
2.5.2. Cognitive Function
2.5.3. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asakawa, T.; Koyano, W.; Ando, T.; Shibata, H. Effects of functional decline on quality of life among the Japanese elderly. Int. J. Aging Hum. Dev. 2000, 50, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.W.; Wang, X.; Ma, Q.; Sun, H.P.; Xu, Y.; Wang, P. Cognitive dysfunction and health-related quality of life among older Chinese. Sci. Rep. 2015, 5, 1–8. [Google Scholar] [CrossRef]
- Launer, L.J. The epidemiologic study of dementia: A life-long quest? Neurobiol. Aging 2005, 26, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Storandt, M.; Grant, E.A.; Miller, J.P.; Morris, J.C. Longitudinal course and neuropathologic outcomes in original vs revised MCI and in pre-MCI. Neurology 2006, 67, 467–473. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Report on Ageing and Health 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- WHO. Governments Commit to Advancements in Dementia Research and Care; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- WHO. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Chou, C.H.; Hwang, C.L.; Wu, Y.T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.H.M.; Van Berckel, B.N.M.; Scheltens, P.; Scherder, E.J.A.; Van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Sanders, L.M.J.; Hortobágyi, T.; la Bastide-van Gemert, S.; van der Zee, E.A.; van Heuvelen, M.J.G. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Kramer, A.F.; Erickson, K.I.; Scalf, P.; McAuley, E.; Cohen, N.J.; Webb, A.; Jerome, G.J.; Marquez, D.X.; Elavsky, S. Cardiovascular fitness, cortical plasticity, and aging. PNAS 2004, 101, 3316–3321. [Google Scholar] [CrossRef]
- Willis, S.L.; Tennstedt, S.L.; Marsiske, M.; Ball, K.; Elias, J.; Koepke, K.M.; Morris, J.N.; Rebok, G.W.; Unverzagt, F.W.; Stoddard, A.M. Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA 2006, 296, 2805–2814. [Google Scholar] [CrossRef]
- Rebok, G.W.; Ball, K.; Guey, L.T.; Jones, R.N.; Kim, H.Y.; King, J.W.; Marsiske, M.; Morris, J.N.; Tennstedt, S.L.; Unverzagt, F.W. Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J. Am. Geriatr. Soc. 2014, 62, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Flnkel, S.I.; Yesavage, J.A. Learning mnemonics: A preliminary evaluation of a computer-aided instruction package for the elderly. Exp. Aging Res. 1989, 15, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Dustman, R.E.; Emmerson, R.Y.; Steinhaus, L.A.; Shearer, D.E.; Dustman, T.J. The effects of videogame playing on neuropsychological performance of elderly individuals. J. Gerontol. 1992, 47, P168–P171. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.; Cajko, L.; Oosterbroek, M.; Michielsen, M.; Van Houten, O.; Salverda, F. Video games and the elderly. Soc. Behav. Pers. 1997, 25, 345–352. [Google Scholar] [CrossRef]
- Ball, K.; Berch, D.B.; Helmers, K.F.; Jobe, J.B.; Leveck, M.D.; Marsiske, M.; Morris, J.N.; Rebok, G.W.; Smith, D.M.; Tennstedt, S.L. Effects of cognitive training interventions with older adults: A randomized controlled trial. JAMA 2002, 288, 2271–2281. [Google Scholar] [CrossRef] [PubMed]
- Günther, V.K.; Schäfer, P.; Holzner, B.J.; Kemmler, G.W. Long-term improvements in cognitive performance through computer-assisted cognitive training: A pilot study in a residential home for older people. Aging Ment. Health 2003, 7, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Jimison, H.; Pavel, M.; Le, T. Home-based cognitive monitoring using embedded measures of verbal fluency in a computer word game. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, Canada; pp. 3312–3315.
- Kueider, A.M.; Parisi, J.M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.F.; Flatt, J.D.; Fu, B.; Butters, M.A.; Chang, C.C.H.; Ganguli, M. Interactive video gaming compared with health education in older adults with mild cognitive impairment: A feasibility study. Int. J. Geriatr. Psychiatry 2014, 29, 890–898. [Google Scholar] [CrossRef]
- Harvey, P.D.; McGurk, S.R.; Mahncke, H.; Wykes, T. Controversies in computerized cognitive training. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 907–915. [Google Scholar] [CrossRef]
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized cognitive training in cognitively healthy older adults: A systematic review and meta-analysis of effect modifiers. PLoS Med. 2014, 11, e1001756. [Google Scholar] [CrossRef]
- Hill, N.T.M.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized cognitive training in older adults with mild cognitive impairment or dementia: A systematic review and meta-analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.F.; Huntley, J.; Bhome, R.; Holmes, B.; Cahill, J.; Gould, R.L.; Wang, H.L.; Yu, X.; Howard, R. Effect of computerised cognitive training on cognitive outcomes in mild cognitive impairment: A systematic review and meta-analysis. BMJ Open 2019, 9, e027062. [Google Scholar] [CrossRef] [PubMed]
- Kalbe, E.; Roheger, M.; Paluszak, K.; Meyer, J.; Becker, J.; Fink, G.R.; Kukolja, J.; Rahn, A.; Szabados, F.; Wirth, B. Effects of a cognitive training with and without additional physical activity in healthy older adults: A follow-up 1 year after a randomized controlled trial. Front. Aging Neurosci. 2018, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Lee, S.; Lee, S.; Jung, S.; Makino, K.; Harada, K.; Harada, K.; Shinkai, Y.; Chiba, I.; Shimada, H. The effect of a multicomponent intervention to promote community activity on cognitive function in older adults with mild cognitive impairment: A randomized controlled trial. Complement. Ther. Med. 2019, 42, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Kempermann, G.; Fabel, K.; Ehninger, D.; Babu, H.; Leal-Galicia, P.; Garthe, A.; Wolf, S. Why and how physical activity promotes experience-induced brain plasticity. Front. Neurosci. 2010, 4, 189. [Google Scholar] [CrossRef] [PubMed]
- Fabel, K.; Wolf, S.; Ehninger, D.; Babu, H.; Galicia, P.; Kempermann, G. Additive effects of physical exercise and environmental enrichment on adult hippocampal neurogenesis in mice. Front. Neurosci. 2009, 3, 2. [Google Scholar] [CrossRef]
- Shatil, E. Does combined cognitive training and physical activity training enhance cognitive abilities more than either alone? A four-condition randomized controlled trial among healthy older adults. Front. Aging Neurosci. 2013, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Verdile, G.; Sohrabi, H.; Campbell, A.; Putland, E.; Cheetham, C.; Dhaliwal, S.; Weinborn, M.; Maruff, P.; Darby, D. A combination of physical activity and computerized brain training improves verbal memory and increases cerebral glucose metabolism in the elderly. Transl. Psychiatry 2014, 4, e487. [Google Scholar] [CrossRef]
- ten Brinke, L.F.; Best, J.R.; Chan, J.L.C.; Ghag, C.; Erickson, K.I.; Handy, T.C.; Liu-Ambrose, T. The effects of computerized cognitive training with and without physical exercise on cognitive function in older adults: An 8-week randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 755–763. [Google Scholar] [CrossRef]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J.; Morley, J.E. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J. Am. Geriatr. Soc. 2012, 60, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Yoo, H.J.; Park, S.Y.; Kim, S.W.; Choi, J.Y.; Yoon, S.J.; Kim, C.H.; Kim, K.I. The Korean version of the FRAIL scale: Clinical feasibility and validity of assessing the frailty status of Korean elderly. Korean J. Intern. Med. 2016, 31, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Miller, D.K.; Morley, J.E. A comparison of four frailty models. J. Am. Geriatr. Soc. 2014, 62, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Voss, V.B.; Cruz-Oliver, D.M.; Cummings-Vaughn, L.A.; Tumosa, N.; Grossberg, G.T.; Morley, J.E. The Rapid Cognitive Screen (RCS): A point-of-care screening for dementia and mild cognitive impairment. J. Nutr. Health Aging 2015, 19, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Kwok, I. Hong Kong List Learning Test: Manual and Preliminary Norm; Department of Psychological and Clinical Psychology Center: Hong Kong, 1999. [Google Scholar]
- Chan, A.S.; Shum, D.; Cheung, R.W.Y. Recent development of cognitive and neuropsychological assessment in Asian countries. Psychol. Assess. 2003, 15, 257–267. [Google Scholar] [CrossRef]
- Chan, A.S.; Kwok, I. Hong Kong List Learning Test; Chinese University of Hong Kong: Hong Kong, 2006. [Google Scholar]
- Mok, V.C.T.; Wong, A.; Yim, P.; Fu, M.; Lam, W.W.M.; Hui, A.C.; Yau, C.; Wong, K.S. The validity and reliability of chinese frontal assessment battery in evaluating executive dysfunction among Chinese patients with small subcortical infarct. Alzheimer Dis. Assoc. Disord. 2004, 18, 68–74. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621. [Google Scholar] [CrossRef]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef]
- Li, K.Z.H.; Roudaia, E.; Lussier, M.; Bherer, L.; Leroux, A.; McKinley, P.A. Benefits of cognitive dual-task training on balance performance in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 1344–1352. [Google Scholar] [CrossRef]
- Smith-Ray, R.L.; Hughes, S.L.; Prohaska, T.R.; Little, D.M.; Jurivich, D.A.; Hedeker, D. Impact of cognitive training on balance and gait in older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 357–366. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: A randomized controlled trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef]
- Fabel, K.; Fabel, K.; Tam, B.; Kaufer, D.; Baiker, A.; Simmons, N.; Kuo, C.J.; Palmer, T.D. VEGF is necessary for exercise-induced adult hippocampal neurogenesis. Eur. J. Neurosci. 2003, 18, 2803–2812. [Google Scholar] [CrossRef] [PubMed]
- Trejo, J.L.; Carro, E.; Torres-Alemán, I. Circulating insulin-like growth factor I mediates exercise-induced increases in the number of new neurons in the adult hippocampus. J. Neurosci. 2001, 21, 1628–1634. [Google Scholar] [CrossRef] [PubMed]
- Steiner, B.; Zurborg, S.; Hörster, H.; Fabel, K.; Kempermann, G. Differential 24 h responsiveness of Prox1–expressing precursor cells in adult hippocampal neurogenesis to physical activity, environmental enrichment, and kainic acid–induced seizures. Neuroscience 2008, 154, 521–529. [Google Scholar] [CrossRef]
- Maffei, L.; Picano, E.; Andreassi, M.G.; Angelucci, A.; Baldacci, F.; Baroncelli, L.; Begenisic, T.; Bellinvia, P.F.; Berardi, N.; Biagi, L. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar] [CrossRef]
- Leuner, B.; Mendolia-Loffredo, S.; Kozorovitskiy, Y.; Samburg, D.; Gould, E.; Shors, T.J. Learning enhances the survival of new neurons beyond the time when the hippocampus is required for memory. J. Neurosci. 2004, 24, 7477–7481. [Google Scholar] [CrossRef]
- Sahay, A.; Wilson, D.A.; Hen, R. Pattern separation: A common function for new neurons in hippocampus and olfactory bulb. Neuron 2011, 70, 582–588. [Google Scholar] [CrossRef]
- Aimone, J.B.; Deng, W.; Gage, F.H. Resolving new memories: A critical look at the dentate gyrus, adult neurogenesis, and pattern separation. Neuron 2011, 70, 589–596. [Google Scholar] [CrossRef]
- Shors, T.J.; Anderson, M.L.; Curlik Ii, D.M.; Nokia, M.S. Use it or lose it: How neurogenesis keeps the brain fit for learning. Behav. Brain Res. 2012, 227, 450–458. [Google Scholar] [CrossRef]
- Perini, R.; Bortoletto, M.; Capogrosso, M.; Fertonani, A.; Miniussi, C. Acute effects of aerobic exercise promote learning. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Formenti, D.; Cavaggioni, L.; Duca, M.; Trecroci, A.; Rapelli, M.; Alberti, G.; Komar, J.; Iodice, P. Acute effect of exercise on cognitive performance in middle-aged adults: Aerobic versus balance. J. Phys. Act. Health 2020, 17, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wu, W.; Feng, W.; Wang, J.; Chen, Y.; Shen, Y.; Li, Q.; Zhang, X.; Li, C. The effects of multi-domain versus single-domain cognitive training in non-demented older people: A randomized controlled trial. BMC Med. 2012, 10, 30. [Google Scholar] [CrossRef]


{kind=link}
| Name of Video Game | Game Details | Cognitive Domain Focus |
|---|---|---|
| 1. Forest of Memory | Remember the location of the cards with different symbols to train short-term memory | Memory |
| 2. Catch the Star | Remember the order of the stars that change in color to train memory and logical thinking | Memory |
| 3. Colored Light Bulbs | Remember the color of the light bulbs to train short-term memory | Memory |
| 4. Master of Oriental Stitch | Remember the pattern and color of embroidery and recognize differences to train short-term memory | Memory |
| 5. Conveyor Belt | Switch the conveyor sorter and collect items with a specific color to train multi-task handling capability | Attention |
| 6. Spot the Difference | Find the unique insect to train attention and capability to filter information | Attention |
| 7. Film Collector | Select the film with a specific color or pattern to train the immediate response to moving objects | Attention |
| 8. Honey Haunters | Identify the correct number over a short period of time continuously to train attention and capability to filter information | Attention |
| 9. Conquer the Ice | Look for the ice cubes with the answer to the calculation to train quick logical thinking | Executive functions |
| 10. From Small to Big | Select labels with different presentations of values in ascending order to train quick logical thinking | Executive functions |
| 11. Switch and Match | Pair the fish with same color but different pattern to train multiple condition handling capabilities | Executive functions |
| 12. Piet Mondrian Mansion | Determine the consistency of the color of light and literal meaning of word of the lift to that on the wall to train quick conversion thinking | Flexibility |
| 13. Color or Shape | Match the shape or color of moving signals to train quick conversion thinking | Flexibility |
| 14. Save the Daruma | Match the pattern to the blocks on the left and right to train quick conversion thinking | Flexibility |
| 15. Pairing Detective | Fit the totem pole to the empty slots on the wall to train sensitivity of visual space | Visuospatial |
| 16. Fixing Pixels | Identify the dominant color of the grids on the TV screen to train the ability to distinguish colors | Visuospatial |
| 17. Dance in the Rain | Select an umbrella with a specific color and shape to train sensitivity to multiple visual spaces | Visuospatial |
| Mean ± SD/n (%) | |||||
|---|---|---|---|---|---|
| Cognitive Intervention Group | |||||
| Variables | Total (n = 347) | Multi-Domain CCT + PE (n = 117) | Two-Domain CCT + PE (n = 116) | Video Watching + PE (Control) (n = 114) | p1 |
| Socio-demographics | |||||
| Age, years | 64.2 ± 6.4 | 64.7 ± 7.3 | 64.0 ± 6.3 | 64.0 ± 5.3 | 0.659 |
| Sex | 0.056 | ||||
| Men | 50 (14.4) | 12 (10.3) | 24 (20.7) | 14 (12.3) | |
| Women | 297 (85.6) | 105 (89.7) | 92 (79.3) | 100 (87.7) | |
| Marital | 0.977 | ||||
| Not married | 114 (32.9) | 38 (32.5) | 39 (33.6) | 37 (32.5) | |
| Married | 233 (67.1) | 79 (67.5) | 77 (66.4) | 77 (67.5) | |
| Educational level | 0.103 | ||||
| Secondary or below | 232 (66.9) | 74 (63.2) | 73 (62.9) | 85 (74.6) | |
| Post-secondary or above | 115 (33.1) | 43 (36.8) | 43 (37.1) | 29 (25.4) | |
| Living arrangement | 0.586 | ||||
| Living with others | 298 (85.9) | 103 (88.0) | 100 (86.2) | 95 (83.3) | |
| Living alone | 49 (14.1) | 14 (12.0) | 16 (13.8) | 19 (16.7) | |
| Frailty | |||||
| FRAIL, score | 0.9 ± 0.7 | 0.9 ± 0.7 | 0.9 ± 0.7 | 0.7 ± 0.7 | 0.056 |
| Cognitive function | |||||
| RCS, score | 7.1 ± 1.6 | 7.0 ± 1.7 | 7.2 ± 1.4 | 7.2 ± 1.6 | 0.472 |
| HKLLT-TL, score | 27.7 ± 7.0 | 27.2 ± 6.9 | 27.5 ± 7.3 | 28.6 ± 6.5 | 0.237 |
| HKLLT-DRT, score | 9.4 ± 3.5 | 9.2 ± 3.1 | 9.1 ± 3.6 | 9.9 ± 3.6 | 0.155 |
| FAB, score | 14.9 ± 2.4 | 14.5 ± 2.4 | 15.6 ± 2.1 | 14.7 ± 2.6 | 0.001 |
| Mean ± SD | Mean ± SD | Mean ± SD | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Multi-Domain CCT + PE (n = 117) | Two-Domain CCT + PE (n = 116) | Video Watching + PE (Control) (n = 114) | |||||||||||||
| Variables | Pre | Post | Diff | p1 | Pre | Post | Diff | p1 | p2 | Pre | Post | Diff | p1 | p3 | p4 |
| FRAIL | 0.9 ± 0.7 | 0.5 ± 0.7 | −0.4 ± 1.0 | <0.001 | 0.9 ± 0.7 | 0.5 ± 0.6 | −0.4 ± 0.8 | <0.001 | 0.794 | 0.7 ± 0.7 | 0.7 ± 0.8 | −0.1 ± 0.9 | 0.319 | 0.011 | 0.012 |
| RCS | 7.0 ± 1.7 | 7.6 ± 1.5 | 0.6 ± 2.0 | 0.002 | 7.2 ± 1.4 | 7.7 ± 1.7 | 0.5 ± 1.8 | 0.004 | 0.700 | 7.2 ± 1.6 | 7.5 ± 1.4 | 0.3 ± 2.0 | 0.124 | 0.455 | 0.390 |
| HKLLT-TL | 27.2 ± 6.9 | 32.4 ± 6.6 | 5.2 ± 6.8 | <0.001 | 27.5 ± 7.3 | 33.4 ± 7.1 | 6.0 ± 5.9 | <0.001 | 0.375 | 28.6 ± 6.5 | 32.0 ± 7.3 | 3.4 ± 8.0 | <0.001 | 0.014 | 0.015 |
| HKLLT-DRT | 9.2 ± 3.1 | 10.9 ± 3.4 | 1.7 ± 3.4 | <0.001 | 9.1 ± 3.6 | 11.5 ± 3.4 | 2.4 ± 3.4 | <0.001 | 0.133 | 9.9 ± 3.6 | 11.1 ± 3.5 | 1.2 ± 3.8 | 0.001 | 0.038 | 0.027 |
| FAB^ | 14.5 ± 2.4 | 15.9 ± 2.3 | 1.4 ± 2.7 | <0.001 | 15.6 ± 2.1 | 16.5 ± 1.8 | 0.9 ± 2.2 | <0.001 | 0.162 | 14.7 ± 2.6 | 16.0 ± 2.1 | 1.3 ± 3.0 | <0.001 | 0.345 | 0.371 |
| Mean ± SD | Mean ± SD | Mean ± SD | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Multi-Domain CCT + PE (n = 41) | Two-Domain CCT + PE (n = 47) | Video Watching + PE (Control) (n = 47) | |||||||||||||
| Variables | Pre | Post | Diff | p1 | Pre | Post | Diff | p1 | p2 | Pre | Post | Diff | p1 | p3 | p4 |
| RCS ≥ 8 (n = 135) | |||||||||||||||
| FRAIL | 0.9 ± 0.8 | 0.4 ± 0.7 | −0.4 ± 1.0 | 0.015 | 0.9 ± 0.6 | 0.5 ± 0.7 | −0.4 ± 0.8 | 0.005 | 0.794 | 0.7 ± 0.7 | 0.6 ± 0.7 | −0.1 ± 0.8 | 0.390 | 0.230 | 0.228 |
| HKLLT-TL | 29.5 ± 6.6 | 33.9 ± 6.1 | 4.4 ± 6.6 | <0.001 | 28.8 ± 7.1 | 35.2 ± 6.3 | 6.3 ± 5.9 | <0.001 | 0.143 | 30.1 ± 6.0 | 33.7 ± 7.2 | 3.6 ± 7.9 | 0.003 | 0.137 | 0.161 |
| HKLLT-DRT | 10.4 ± 2.8 | 11.7 ± 3.1 | 1.3 ± 3.4 | 0.019 | 9.2 ± 3.7 | 12.4 ± 2.3 | 3.1 ± 3.1 | <0.001 | 0.009 | 10.7 ± 3.3 | 11.5 ± 3.6 | 0.7 ± 4.0 | 0.206 | 0.004 | 0.004 |
| FAB | 15.2 ± 2.0 | 16.4 ± 1.7 | 1.3 ± 2.5 | 0.003 | 15.7 ± 2.1 | 16.5 ± 1.8 | 0.8 ± 2.2 | 0.019 | 0.343 | 15.3 ± 2.4 | 16.2 ± 2.1 | 0.9 ± 2.8 | 0.031 | 0.647 | 0.762 |
| RCS < 8 (n = 212) | |||||||||||||||
| FRAIL | 1.0 ± 0.7 | 0.6 ± 0.7 | −0.4 ± 1.0 | <0.001 | 0.9 ± 0.7 | 0.5 ± 0.6 | −0.4 ± 0.8 | <0.001 | 0.916 | 0.8 ± 0.7 | 0.7 ± 0.8 | −0.1 ± 1.0 | 0.545 | 0.047 | 0.047 |
| HKLLT-TL | 25.9 ± 6.8 | 31.6 ± 6.7 | 5.7 ± 6.9 | <0.001 | 26.5 ± 7.4 | 32.3 ± 7.3 | 5.7 ± 6.0 | <0.001 | 0.979 | 27.6 ± 6.8 | 30.8 ± 7.2 | 3.2 ± 8.1 | 0.002 | 0.056 | 0.054 |
| HKLLT-DRT | 8.6 ± 3.1 | 10.5 ± 3.5 | 1.9 ± 3.5 | <0.001 | 9.0 ± 3.6 | 10.8 ± 3.9 | 1.9 ± 3.6 | <0.001 | 0.930 | 9.3 ± 3.7 | 10.8 ± 3.4 | 1.5 ± 3.7 | 0.002 | 0.728 | 0.671 |
| FAB ^ | 14.1 ± 2.5 | 15.6 ± 2.5 | 1.4 ± 2.9 | <0.001 | 15.5 ± 2.2 | 16.5 ± 1.8 | 1.0 ± 2.2 | <0.001 | 0.314 | 14.2 ± 2.7 | 15.9 ± 2.1 | 1.7 ± 3.2 | <0.001 | 0.365 | 0.264 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, R.; Leung, G.; Woo, J. Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1396. https://doi.org/10.3390/ijerph18041396
Yu R, Leung G, Woo J. Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(4):1396. https://doi.org/10.3390/ijerph18041396
Chicago/Turabian StyleYu, Ruby, Grace Leung, and Jean Woo. 2021. "Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults" International Journal of Environmental Research and Public Health 18, no. 4: 1396. https://doi.org/10.3390/ijerph18041396
APA StyleYu, R., Leung, G., & Woo, J. (2021). Randomized Controlled Trial on the Effects of a Combined Intervention of Computerized Cognitive Training Preceded by Physical Exercise for Improving Frailty Status and Cognitive Function in Older Adults. International Journal of Environmental Research and Public Health, 18(4), 1396. https://doi.org/10.3390/ijerph18041396