Associations between Community Cohesion and Subjective Wellbeing of the Elderly in Guangzhou, China—A Cross-Sectional Study Based on the Structural Equation Model



Abstract
1. Introduction
1.1. Conceptualization and Dimensions of Community Cohesion
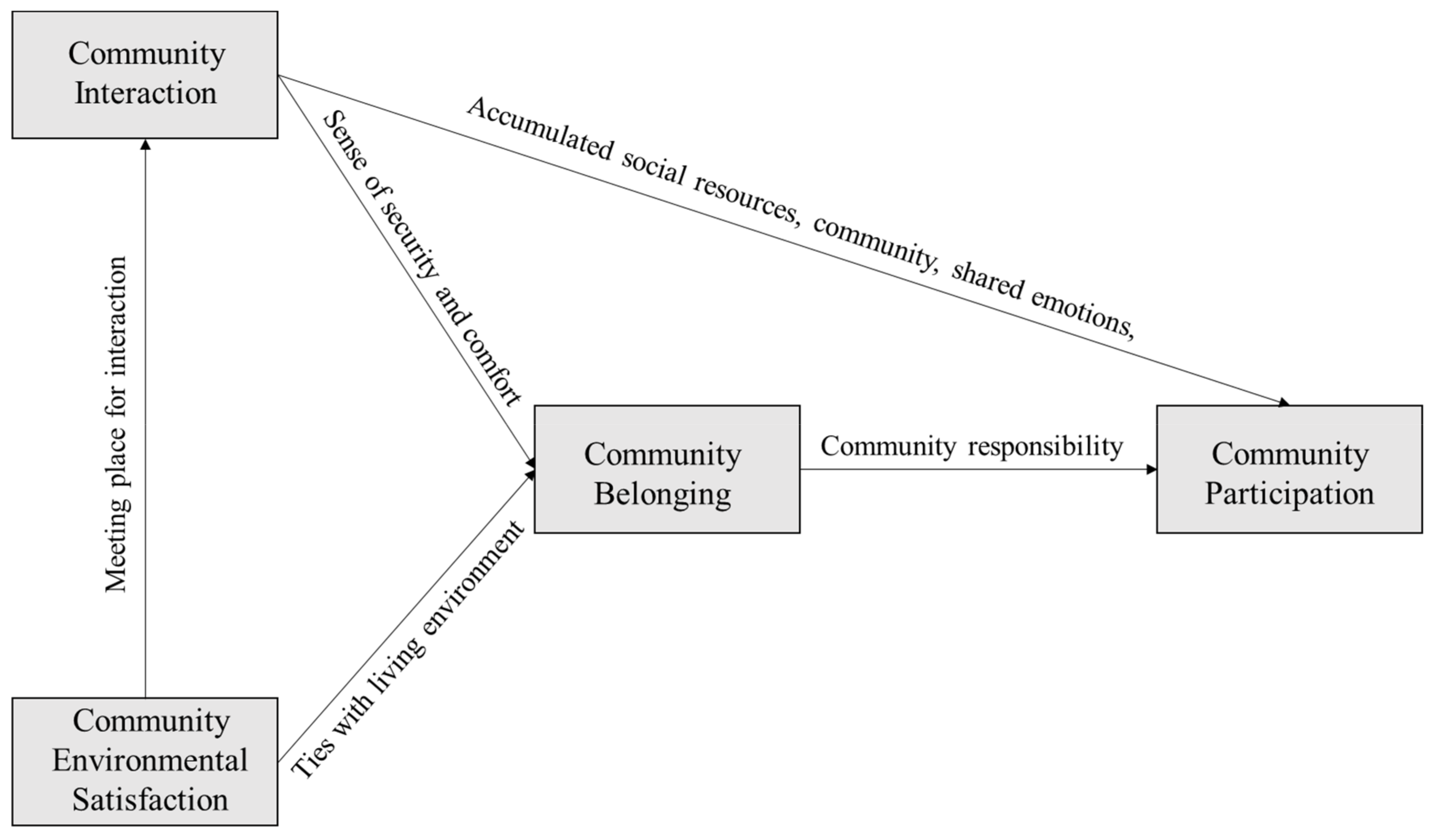
1.2. Interrelationship between Four Dimensions of Community Cohesion
1.3. Relationship between Community Cohesion and Individuals’ Subjective Wellbeing
1.4. Research Gap and Study Goal
2. Materials and Methods
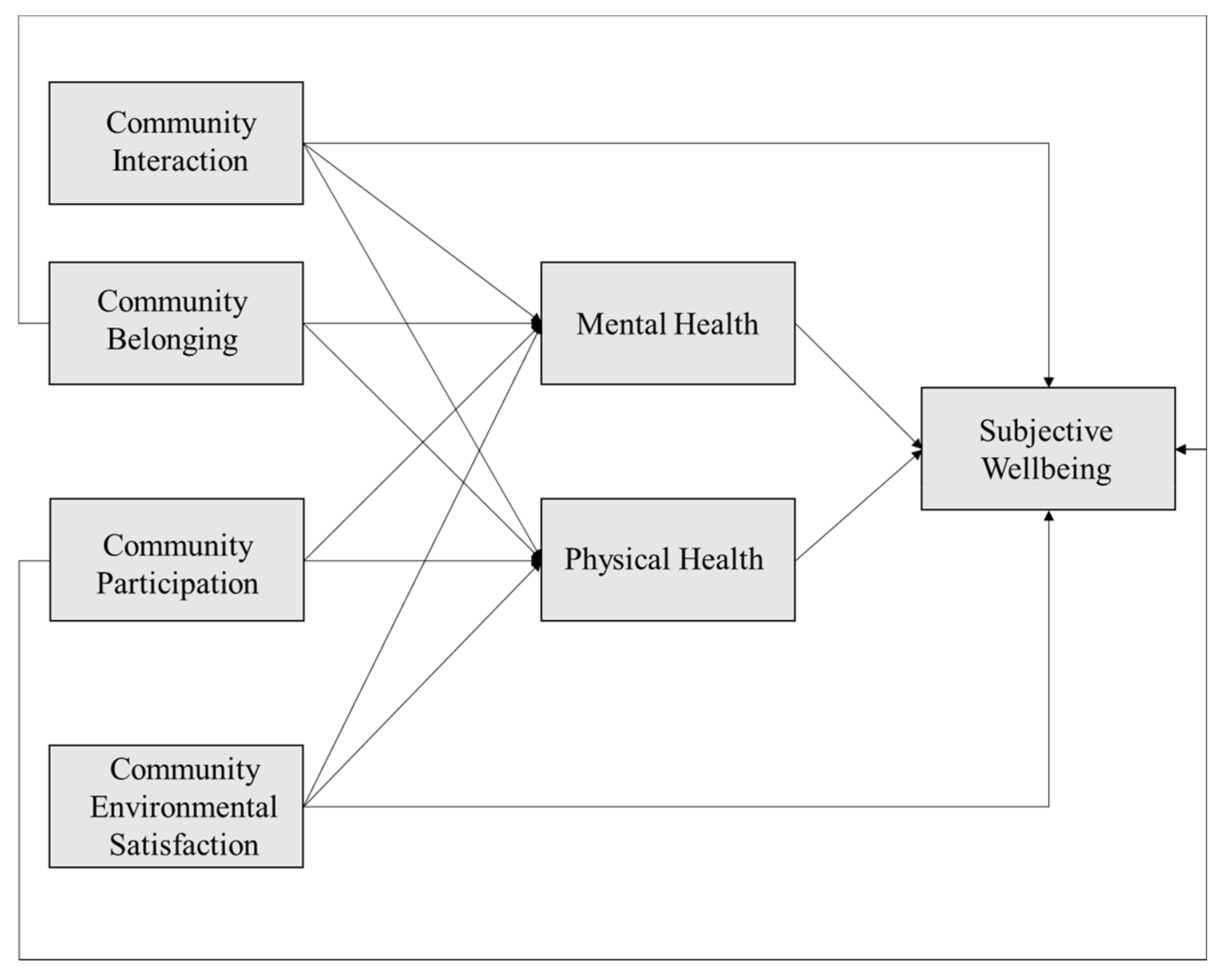
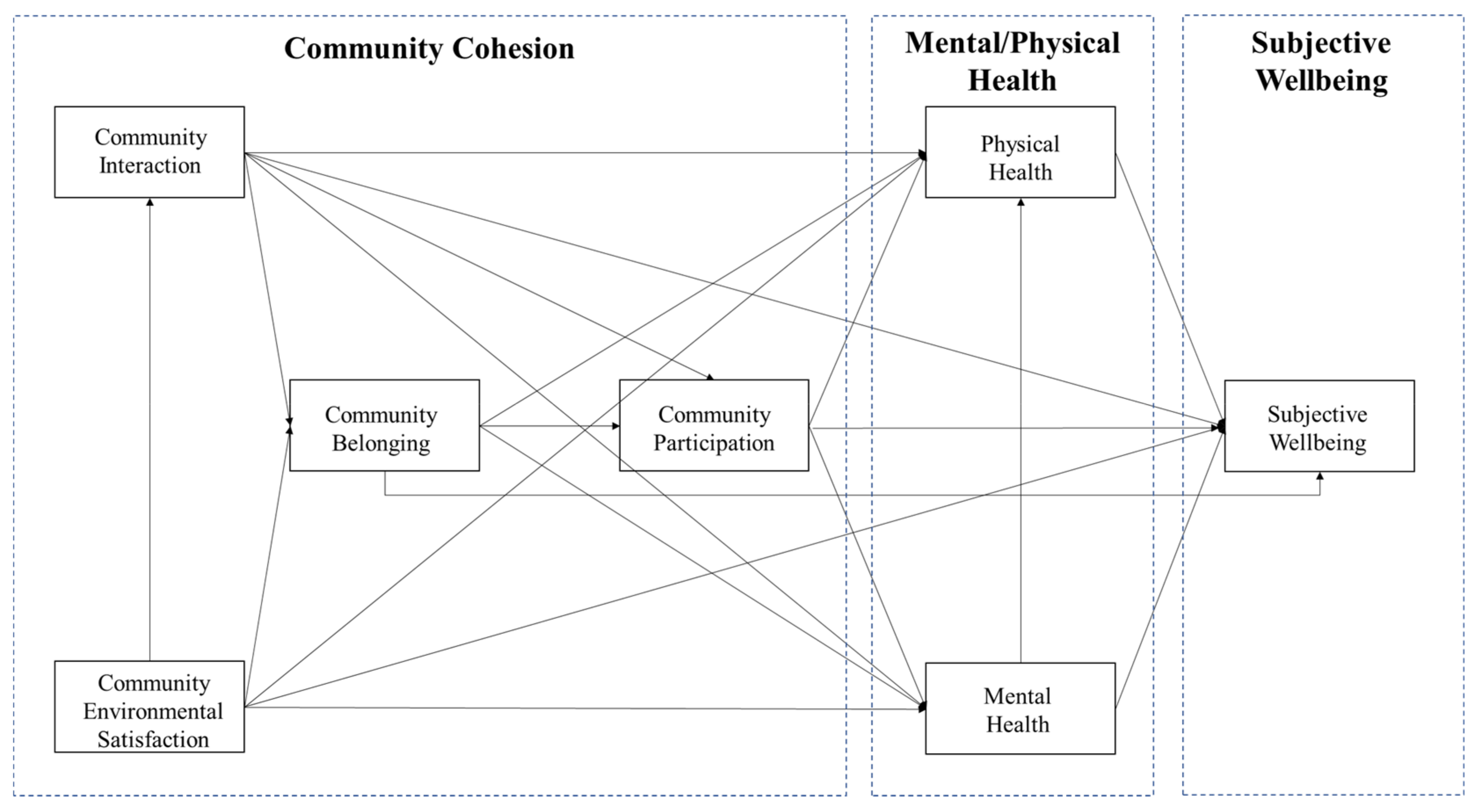
2.1. Hypotheses and Conceptual Model
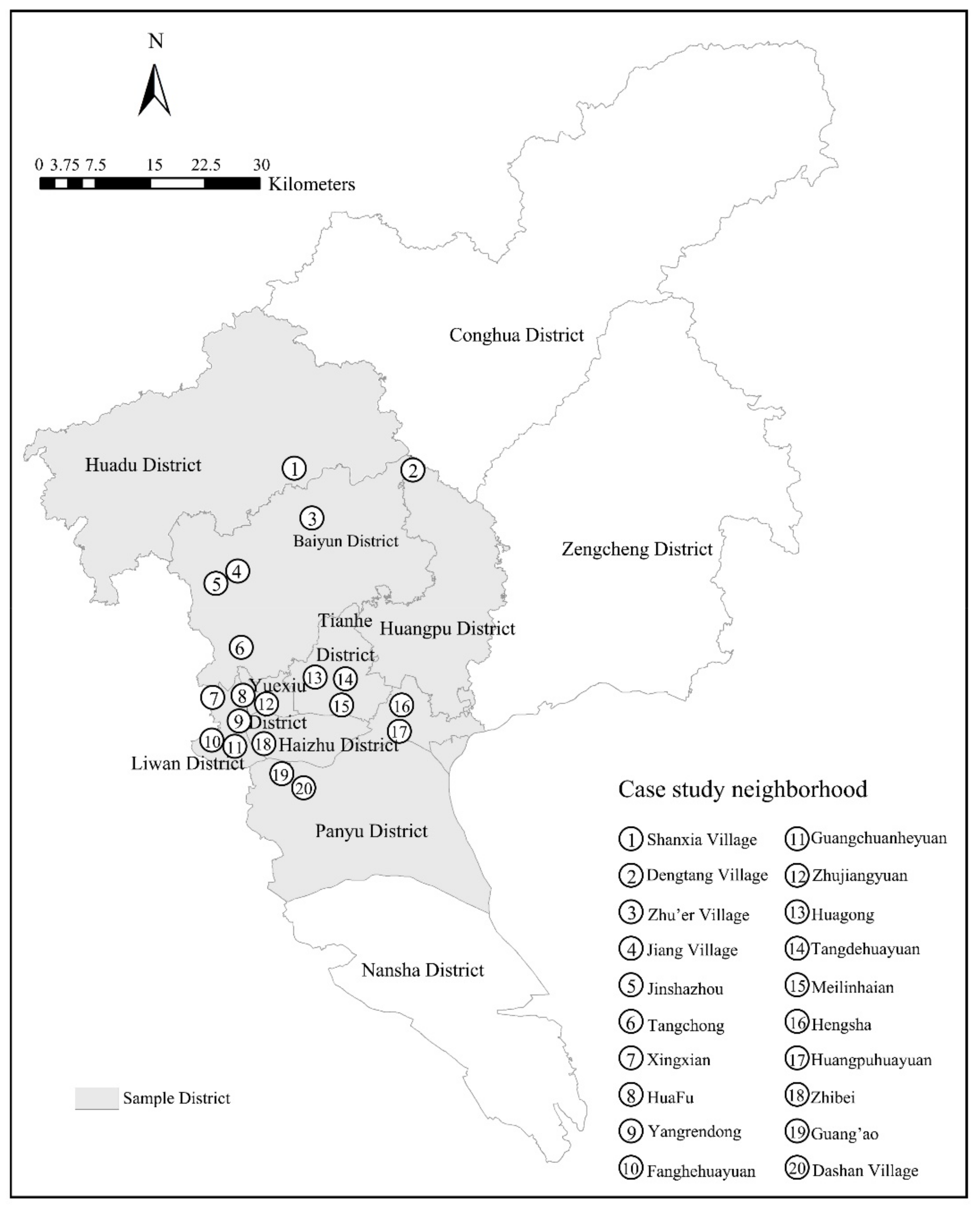
2.2. Study Design, Area and Participants
2.3. Measurement
2.4. Analysis Method
2.5. High and Low SESI Communities Classification
3. Results
3.1. Descriptive Statistics
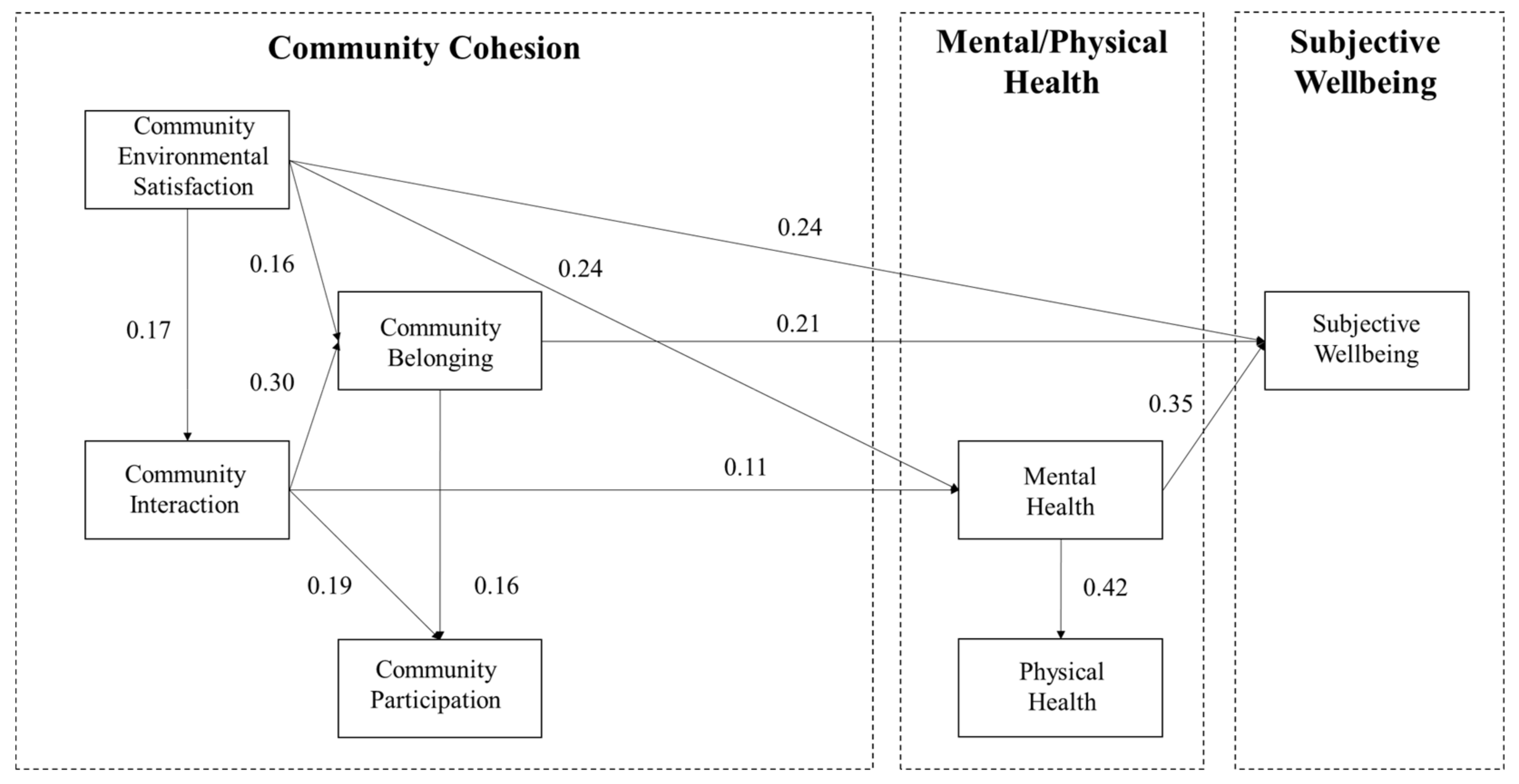
3.2. Model Fit and Results
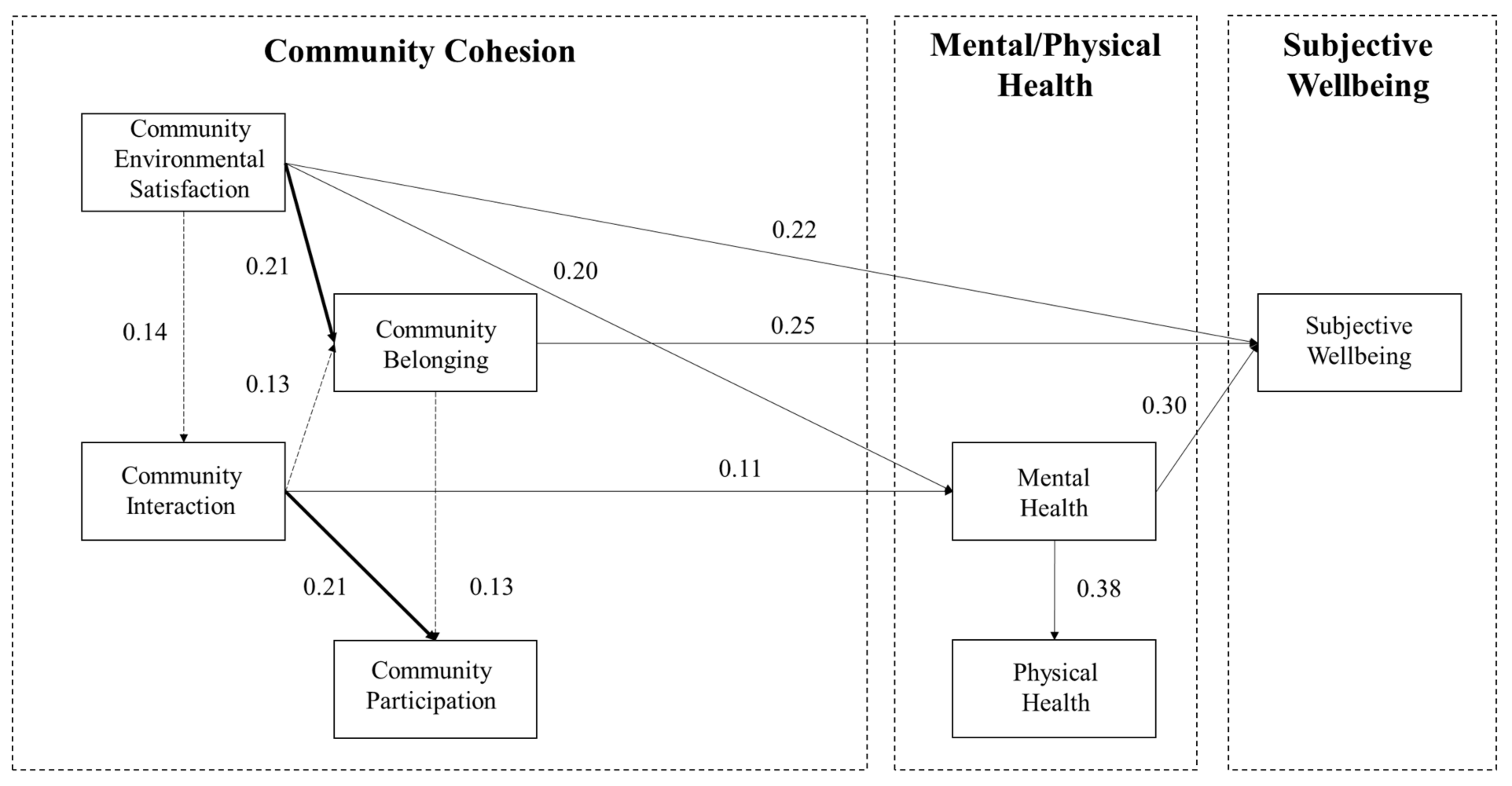
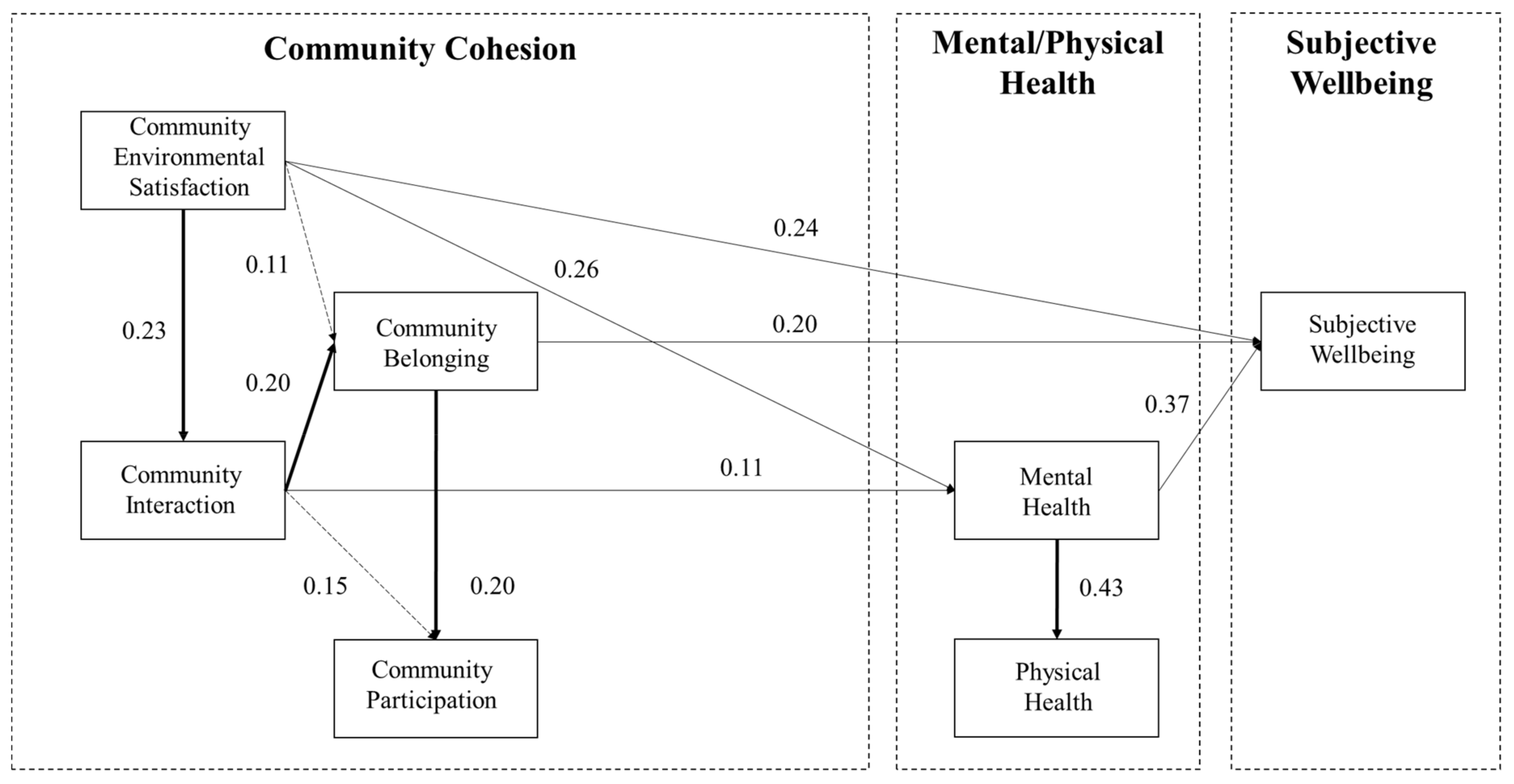
3.3. Multigroup Analysis
4. Discussion
4.1. Interrelationship between Four Dimensions of Community Cohesion
4.2. Association between Community Cohesion and the Elderly’s Health Status
4.3. Association between Community Cohesion and Subjective Wellbeing of the Elderly
4.4. Association Linkages between High- and Low-SESI Communities
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs. Population Division (2017); United Nations Department of Economic and Social Affairs: New York, NY, USA, 2017; ISBN 9789211515510. [Google Scholar]
- World Health Organization. China Country Assessment Report on Ageing and Health; World Health Organization Press: Geneva, Switzerland, 2015; ISBN 9789241509312. [Google Scholar]
- Zhang, Y. The Growth Rate of the Total Population Slows Down and the Level of Urbanization Continues to Rise (National Bureau of Statistics, in Chinese). Available online: http://www.stats.gov.cn/tjsj/zxfb/202001/t20200119_1723767.html (accessed on 27 July 2020).
- Beard, J.R.; Blaney, S.; Cerda, M.; Frye, V.; Lovasi, G.S.; Ompad, D.; Rundle, A.; Vlahov, D. Neighborhood characteristics and disability in older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, 252–257. [Google Scholar] [CrossRef]
- Encel, S.; Kaye, M.; Zdenkowski, G. Keeping in Touch: Older People Living Alone: A Discussion Paper; Consultative Committee on Ageing: Sydney, Australia, 1996.
- Colic-Peisker, V.; Robertson, S. Social change and community cohesion: An ethnographic study of two Melbourne suburbs. Ethn. Racial Stud. 2013, 38, 75–91. [Google Scholar] [CrossRef]
- Wellman, B. Community: From neighborhood to network. Commun. ACM 2005, 48, 53–55. [Google Scholar] [CrossRef]
- Guest, A.M.; Wierzbicki, S.K. Social ties at the neighborhood level: Two decades of GSS evidence. Urban Aff. Rev. 1999, 35, 92–111. [Google Scholar] [CrossRef]
- Skjaeveland, O.; Gärling, T.; Maeland, J.G.; Skjæveland, O.; Mæland, J.G. A multidimensional measure of neighboring. Am. J. Community Psychol. 1996, 24, 413–435. [Google Scholar] [CrossRef]
- Richardson, J. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Bourdieu, P., Ed.; Greenwood Press: Westport, CT, USA, 1986; pp. 241–258. [Google Scholar]
- Putnam, R.D.; Leonardi, R. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993. [Google Scholar]
- Portes, A. Social capital: Its origins and applications in modern sociology. Annu. Rev. Sociol. 1998, 24, 1–24. [Google Scholar] [CrossRef]
- Ferragina, E. The socio-economic determinants of social capital and the mediating effect of history: Making Democracy Work revisited. Int. J. Comp. Sociol. 2013, 54, 48–73. [Google Scholar] [CrossRef]
- Ferragina, E. The welfare state and social capital in Europe: Reassessing a complex relationship. Int. J. Comp. Sociol. 2017, 58, 55–90. [Google Scholar] [CrossRef]
- Coleman, J.S. Social Capital in the creation of human capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Kearns, A.; Forrest, R. Social cohesion and multilevel urban governance. Urban Stud. 2000, 37, 995–1017. [Google Scholar] [CrossRef]
- Dekker, K.; Bolt, G. Social Cohesion in post-war estates in the Netherlands: Differences between socioeconomic and ethnic groups. Ned. Geogr. Stud. 2006, 42, 59–81. [Google Scholar] [CrossRef]
- Forrest, R.; Kearns, A. Social cohesion, social capital and the neighbourhood. Urban Stud. 2001, 38, 2125–2143. [Google Scholar] [CrossRef]
- Van Beckhoven, E.; Van Kempen, R. Towards more social cohesion in large post-second world war housing estates? A case study in Utrecht, the Netherlands1. Hous. Stud. 2006, 21, 477–500. [Google Scholar] [CrossRef]
- Smith, R.A. Measuring neighborhood cohesion: A review and some suggestions. Hum. Ecol. 1975, 3, 143–160. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, F.; Liu, Y.; Li, Z. Changing neighbourhood cohesion under the impact of urban redevelopment: A case study of Guangzhou, China. Urban Geogr. 2017, 38, 266–290. [Google Scholar] [CrossRef]
- Dekker, K. Social capital, neighbourhood attachment and participation in distressed urban areas. A case study in the Hague and Utrecht, the Netherlands. Hous. Stud. 2007, 22, 355–379. [Google Scholar] [CrossRef]
- Hidalgo, M.; Hernández, B. Place attachment: Conceptual and empirical questions. J. Environ. Psychol. 2001, 21, 273–281. [Google Scholar] [CrossRef]
- Relph, E.C. Place and Placelessness; Pion Limited: London, UK, 1976. [Google Scholar]
- Williams, A.; Kitchen, P.; DeMiglio, L.; Eyles, J.; Newbold, B.; Streiner, D. Sense of place in Hamilton, Ontario: Empirical results of a neighborhood-based survey. Urban Geogr. 2010, 31, 905–931. [Google Scholar] [CrossRef]
- Brown, B.; Perkins, D.D.; Brown, G. Place attachment in a revitalizing neighborhood: Individual and block levels of analysis. J. Environ. Psychol. 2003, 23, 259–271. [Google Scholar] [CrossRef]
- Raymond, C.M.; Brown, G.; Weber, D. The measurement of place attachment: Personal, community, and environmental connections. J. Environ. Psychol. 2010, 30, 422–434. [Google Scholar] [CrossRef]
- Scannell, L.; Gifford, R. Defining place attachment: A tripartite organizing framework. J. Environ. Psychol. 2010, 30, 1–10. [Google Scholar] [CrossRef]
- Fu, Q.; Lin, N. The weaknesses of civic territorial organizations: Civic engagement and homeowners associations in urban China. Int. J. Urban Reg. Res. 2013, 38, 2309–2327. [Google Scholar] [CrossRef]
- Zhu, Y. Toward community engagement: Can the built environment help? Grassroots participation and communal space in Chinese urban communities. Habitat Int. 2015, 46, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.; Gale, C.R.; Parsons, S.; Kuh, D. Neighbourhood cohesion and mental wellbeing among older adults: A mixed methods approach. Soc. Sci. Med. 2014, 107, 44–51. [Google Scholar] [CrossRef]
- Helliwell, J.F.; Putnam, R.D. The social context of well–being. Philos. Trans. R. Soc. B Biol. Sci. 2004, 359, 1435–1446. [Google Scholar] [CrossRef]
- Okun, M.A.; Stock, W.A.; Haring, M.J.; Witter, R.A. The social activity/subjective well-being relation: A quantitative synthesis. Res. Aging 1984, 6, 45–65. [Google Scholar] [CrossRef]
- Adams, K.B.; Leibbrandt, S.; Moon, H. A critical review of the literature on social and leisure activity and wellbeing in later life. Ageing Soc. 2011, 31, 683–712. [Google Scholar] [CrossRef]
- Berry, H.L.; Welsh, J.A. Social capital and health in Australia: An overview from the household, income and labour dynamics in Australia survey. Soc. Sci. Med. 2010, 70, 588–596. [Google Scholar] [CrossRef]
- Hays, R.A.; Kogl, A.M. neighborhood attachment, social capital building, and political participation: A case study of low- and moderate-income residents of Waterloo, Iowa. J. Urban Aff. 2007, 29, 181–205. [Google Scholar] [CrossRef]
- Taylor, M. Community participation in the real world: Opportunities and pitfalls in new governance spaces. Urban Stud. 2007, 44, 297–317. [Google Scholar] [CrossRef]
- Sooman, A.; MacIntyre, S. Health and perceptions of the local environment in socially contrasting neighbourhoods in glasgow. Health Place 1995, 1, 15–26. [Google Scholar] [CrossRef]
- Bures, R.M. Childhood residential stability and health at midlife. Am. J. Public Health 2003, 93, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Ambrey, C. Urban greenspace, physical activity and wellbeing: The moderating role of perceptions of neighbourhood affability and incivility. Land Use Policy 2016, 57, 638–644. [Google Scholar] [CrossRef]
- Ballas, D.; Tranmer, M. Happy people or happy places? A multilevel modeling approach to the analysis of happiness and well-being. Int. Reg. Sci. Rev. 2012, 35, 70–102. [Google Scholar] [CrossRef]
- Ettema, D.F.; Smajic, I. Walking, places and wellbeing. Geogr. J. 2015, 181, 102–109. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Schulz, A.J.; Israel, B.A.; Zenk, S.N.; Parker, E.A.; Lichtenstein, R.; Shellman-Weir, S.; Klem, A.B.L. Psychosocial stress and social support as mediators of relationships between income, length of residence and depressive symptoms among African American women on Detroit’s eastside. Soc. Sci. Med. 2006, 62, 510–522. [Google Scholar] [CrossRef]
- Wight, R.G.; Botticello, A.L.; Aneshensel, C.S. Socioeconomic context, social support, and adolescent mental health: A multilevel investigation. J. Youth Adolesc. 2006, 35, 115–126. [Google Scholar] [CrossRef]
- Chung, H. The protective function of neighborhood social ties on psychological health. Am. J. Health Behav. 2011, 35, 785–796. [Google Scholar] [CrossRef]
- Green, G.; Gilbertson, J.; Grimsley, M.F. Fear of crime and health in residential tower blocks. A case study in Liverpool, UK. Eur. J. Public Health 2002, 12, 10–15. [Google Scholar] [CrossRef]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social capital and health: A review of prospective multilevel studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef]
- Fone, D.L.; Dunstan, F.; Lloyd, K.; Williams, G.; Watkins, J.; Palmer, S. Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. Int. J. Epidemiol. 2007, 36, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, J.; Drukker, M.; Gunther, N.; Feron, F.; van Os, J. Children’s mental health service use, neighbourhood socioeconomic deprivation, and social capital. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Lindström, M.; Hanson, B.S.; Östergren, P.-O. Socioeconomic differences in leisure-time physical activity: The role of social participation and social capital in shaping health related behaviour. Soc. Sci. Med. 2001, 52, 441–451. [Google Scholar] [CrossRef]
- Kahn, E.B.; Ramsey, L.T.; Brownson, R.C.; Heath, G.W.; Howze, E.H.; Powell, K.E.; Stone, E.J.; Rajab, M.W.; Corso, P. The effectiveness of interventions to increase physical activity: A systematic review. Am. J. Prev. Med. 2002, 22, 73–107. [Google Scholar] [CrossRef]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S. Social environment and physical activity: A review of concepts and evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef]
- Keyes, C.L. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef]
- Keyes, C.L. The nexus of cardiovascular disease and depression revisited: The complete mental health perspective and the moderating role of age and gender. Aging Ment. Health 2004, 8, 266–274. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Chronic physical conditions and aging: Is mental health a potential protective factor? Ageing Int. 2005, 30, 88–104. [Google Scholar] [CrossRef]
- Okun, M.A.; Stock, W.A.; Haring, M.J.; Witter, R.A. Health and subjective well-being: A meta-analyis. Int. J. Aging Hum. Dev. 1984, 19, 111–132. [Google Scholar] [CrossRef]
- Seligman, M.E.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Brian, B.; Goldman, M.; Kernis, M.H. Role of authenticity in healthy psychological functioning and subjective. Ann. Am. Psychother. Assoc. 2001, 5, 18–20. [Google Scholar]
- Satin, J.R.; Linden, W.; Phillips, M.J. Depression as a predictor of disease progression and mortality in cancer patients: A meta-analysis. Cancer 2009, 115, 5349–5361. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, S.S. Association between major depressive episodes in patients with chronic kidney disease and initiation of dialysis, hospitalization, or death. JAMA J. Am. Med. Assoc. 2010, 303, 1946–1953. [Google Scholar] [CrossRef]
- Meijer, A.; Conradi, H.J.; Bos, E.H.; Thombs, B.D.; van Melle, J.P.; de Jonge, P. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: A meta-analysis of 25 years of research. Gen. Hosp. Psychiatry 2011, 33, 203–216. [Google Scholar] [CrossRef]
- Zhang, Q. Community social network and subjective well-being of the aged people. Ph.D. Thesis, Shandong University, Jinan, China, 28 April 2016. (In Chinese). [Google Scholar]
- Ferragina, E. Social Capital and equality: Tocqueville’s legacy. Available online: https://www.econstor.eu/bitstream/10419/95420/1/609878379.pdf (accessed on 22 January 2021).
- Stuck, A.E.; Iliffe, S. Comprehensive geriatric assessment for older adults. BMJ 2011, 343, d6799. [Google Scholar] [CrossRef]
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017, 9, CD006211. [Google Scholar] [CrossRef]
- Muthén, B.O. Latent variable modeling in heterogeneous populations. Psychometrika 1989, 54, 557–585. [Google Scholar] [CrossRef]
- Ullman, J.B.; Bentler, P.M. Structural equation modeling. In Handbook of Psychology, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Wu, Y.-T.; Prina, A.M.; Jones, A.; Barnes, L.E.; Matthews, F.E.; Brayne, C.E.; Cfas, M. Land use mix and five-year mortality in later life: Results from the cognitive function and ageing study. Health Place 2016, 38, 54–60. [Google Scholar] [CrossRef]
- Lin, J.; Zhou, Y.; Yuan, Y.; Liu, Y. Neighborhood effects on residents’ health and its difference: Structural equation model analysis based on 28 communities in Guangzhou. Mod. Urban Res. 2020, 9–17. [Google Scholar]
- Haiyan, J.; Rongbo, X.; Chunshan, Z. The comsumption’s social differentiation and supply’s strategies of Guangzhou central district’s public parks. Planners 2010, 26, 66–72. [Google Scholar]
- Zhou, Y.; Yuan, Y.; Chen, Y.; Lai, S. Association pathways between neighborhood greenspaces and the physical and mental health of older adults—A cross-sectional study in Guangzhou, China. Front. Public Health 2020, 8, 551453. [Google Scholar] [CrossRef]
- Suchocka, M.; Jankowski, P.; Błaszczyk, M. perception of urban trees by Polish tree professionals vs. nonprofessionals. Sustainability 2019, 11, 211. [Google Scholar] [CrossRef]
- Błaszczyk, M.; Suchocka, M.; Gawłowska, A.; Kimic, K.; Kaszuba, K. Warsaw parks as recreational places: Needs and preferences of the elderly users. In Proceedings of the Public Recreation and Landscape Protection—with Sense Hand in Hand, Křtiny, Czech Republic, 13–15 May 2019; pp. 481–486. [Google Scholar]
- Błaszczyk, M.; Suchocka, M.; Wojnowska-Heciak, M.; Muszyńska, M. Quality of urban parks in the perception of city residents with mobility difficulties. PeerJ 2020, 8, e10570. [Google Scholar] [CrossRef]
- Blokland, T. Unravelling three of a kind: Cohesion, community and solidarity. Neth. J. Soc. Sci. 2000, 36, 56–70. [Google Scholar]
- Abada, T.; Hou, F.; Ram, B. Racially mixed neighborhoods, perceived neighborhood social cohesion, and adolescent health in Canada. Soc. Sci. Med. 2007, 65, 2004–2017. [Google Scholar] [CrossRef] [PubMed]
- Robinette, J.W.; Charles, S.T.; Mogle, J.A.; Almeida, D.M. Neighborhood cohesion and daily well-being: Results from a diary study. Soc. Sci. Med. 2013, 96, 174–182. [Google Scholar] [CrossRef]
- Row, A.T.; Jacobs, J. The death and life of great american cities. Yale Law J. 1962, 71, 1597. [Google Scholar] [CrossRef]
- Gu, R.; Song, H.; Li, J. Investigation and correlation analysis of social support and mental health in community-dwelling elderly people. Chinese Gen. Pract. 2019, 22, 570–574. (In Chinese) [Google Scholar]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- Wang, J.; Yang, X. The influence of social interaction on the mental health of the elderly: The mediation effect of aging attitude: Relationship between childhood trauma and depressive symptoms among resident physicians: Mediating effect of resilience. In Proceedings of the 21st National Psychological Academic Conference, Beijing, China, 2–4 November 2018; pp. 1369–1370. (In Chinese). [Google Scholar]
- Xiao, Y.; Miao, S.; Sarkar, C.; Geng, H.; Lu, Y. Exploring the impacts of housing condition on migrants’ mental health in Nanxiang, Shanghai: A structural equation modelling approach. Int. J. Environ. Res. Public Health 2018, 15, 225. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.-L.; Liu, T.-B.; Chan, S.S.; Jin, D.; Hu, C.-Y.; Dai, J.; Chiu, H.F.K. Prevalence and correlates of major depressive disorder among rural-to-urban migrant workers in Shenzhen, China. J. Affect. Disord. 2015, 183, 1–9. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.; Saegert, S. Residential density, social overload, and social withdrawal. Hum. Ecol. 1978, 6, 253–272. [Google Scholar] [CrossRef]
- Lavin, T.; Higgins, C.; Metcalfe, O.; Jordan, A. Health Impacts of the Built Environment: A Review; Institute of Public Health in Ireland: Belfast, UK, 2006; ISBN 9780954231668. [Google Scholar]
- Ottosson, J.; Grahn, P. Measures of restoration in geriatric care residences: The influence of nature on elderly people’s power of concentration, blood pressure and pulse rate. J. Hous. Elder. 2005, 19, 227–256. [Google Scholar] [CrossRef]
- Rothstein, B. Social capital in the social democratic welfare state. Polit. Soc. 2001, 29, 207–241. [Google Scholar] [CrossRef]
- Rugel, E.J.; Carpiano, R.M.; Henderson, S.B.; Brauer, M. Exposure to natural space, sense of community belonging, and adverse mental health outcomes across an urban region. Environ. Res. 2019, 171, 365–377. [Google Scholar] [CrossRef]
- Jakubec, S.L.; Olfert, M.; Choi, L.L.S.; Dawe, N.; Sheehan, D. Understanding belonging and community connection for seniors living in the suburbs. Urban Plan. 2019, 4, 43–52. [Google Scholar] [CrossRef]
- Frank, L.D.; Andresen, M.A.; Schmid, T.L. Obesity relationships with community design, physical activity, and time spent in cars. Am. J. Prev. Med. 2004, 27, 87–96. [Google Scholar] [CrossRef]
- Kligerman, M.; Sallis, J.F.; Ryan, S.; Frank, L.D.; Nader, P.R. Association of neighborhood design and recreation environment variables with physical activity and body mass index in adolescents. Am. J. Health Promot. 2007, 21, 274–277. [Google Scholar] [CrossRef]
- Grafova, I.B. Overweight children: Assessing the contribution of the built environment. Prev. Med. 2008, 47, 304–308. [Google Scholar] [CrossRef]
- Storgaard, R.L.; Hansen, H.S.; Aadahl, M.; Glümer, C. Association between neighbourhood green space and sedentary leisure time in a Danish population. Scand. J. Public Health 2013, 41, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Althoff, T.; Sosič, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Hale, C.J.; Hannum, J.W.; Espelage, D.L. Social support and physical health: The importance of belonging. J. Am. Coll. Health 2010, 53, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Satariano, W.A.; Guralnik, J.M.; Jackson, R.J.; Marottoli, R.A.; Phelan, E.A.; Prohaska, T.R. Mobility and Aging: New directions for public health action. Am. J. Public Health 2012, 102, 1508–1515. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Prevalence and most common causes of disability among adults—United States, 2005. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 421–426. [Google Scholar]
- Liu, Y.; Tao, L.; Zhang, J.; Liu, J.; Li, H.; Liu, X.; Luo, Y.; Zhang, J.; Wang, W.; Guo, X. Impact of commuting mode on obesity among a working population in Beijing, China: Adjusting for air pollution. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3959–3968. [Google Scholar] [CrossRef]
- Flint, E.; Cummins, S. Active commuting and obesity in mid-life: Cross-sectional, observational evidence from UK Biobank. Lancet Diabetes Endocrinol. 2016, 4, 420–435. [Google Scholar] [CrossRef]
- Bell, S.L.; Phoenix, C.; Lovell, R.; Wheeler, B.W. Green space, health and wellbeing: Making space for individual agency. Health. Place 2014, 30, 287–292. [Google Scholar] [CrossRef]
- Spinney, J.E.; Scott, D.M.; Newbold, K.B. Transport mobility benefits and quality of life: A time-use perspective of elderly Canadians. Transp. Policy 2009, 16, 1–11. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; De Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; de Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef]
- Thompson, C.W.; Roe, J.J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef]
- Carrus, G.; Scopelliti, M.; Lafortezza, R.; Colangelo, G.; Ferrini, F.; Salbitano, F.; Agrimi, M.; Portoghesi, L.; Semenzato, P.; Sanesi, G. Go greener, feel better? The positive effects of biodiversity on the well-being of individuals visiting urban and peri-urban green areas. Landsc. Urban Plan. 2015, 134, 221–228. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, J. Social participation and subjective well-being among retirees in China. Soc. Indic. Res. 2015, 123, 143–160. [Google Scholar] [CrossRef]
- Shulin, L.; Zhou, Y.; Yuan, Y. Comparative research on characteristics and formation mechanism of megacity’s urban and rural aging communities—Based on taipingtongjin community and Huangshatang Village in Guangzhou. Mod. Urban Res. 2019, 03, 15–22. (In Chinese) [Google Scholar]
- Nowok, B.; Van Ham, M.; Findlay, A.M.; Gayle, V. Does Migration Make You Happy? A longitudinal study of internal migration and subjective well-being. Environ. Plan. A Econ. Space 2013, 45, 986–1002. [Google Scholar] [CrossRef]
- Bradburn, N.M. The Structure of Psychological Well-Being; Aldine Publishing Company: Chicago, IL, USA, 1969; ISBN 9780202250298. [Google Scholar]
- Yakovlev, P.A.; Leguizamon, S. Ignorance is not bliss: On the role of education in subjective well-being. J. Socio Econ. 2012, 41, 806–815. [Google Scholar] [CrossRef]
- Campbell, A. Subjective measures of well-being. Am. Psychol. 1976, 31, 117–124. [Google Scholar] [CrossRef]
- Hu, F. Homeownership and subjective wellbeing in urban China: Does owning a house make you happier? Soc. Indic. Res. 2013, 110, 951–971. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Adler, N.E.; Marmot, M.G. Subjective social status: Its determinants and its association with measures of ill-health in the Whitehall II study. Soc. Sci. Med. 2003, 56, 1321–1333. [Google Scholar] [CrossRef]
- Kenny, C. Does development make you happy? subjective wellbeing and economic growth in developing countries. Soc. Indic. Res. 2005, 73, 199–219. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, F.; Wu, F.; Liu, Y.; Li, Z. The subjective wellbeing of migrants in Guangzhou, China: The impacts of the social and physical environment. Cities 2017, 60, 333–342. [Google Scholar] [CrossRef]
- Tang, D.; Lin, Z.; Chen, F. Moving beyond living arrangements: The role of family and friendship ties in promoting mental health for urban and rural older adults in China. Aging Ment. Health 2020, 24, 1523–1532. [Google Scholar] [CrossRef]
- Fukuyama, F. Trust: The Social Virtues and the Creation of Prosperity; Free Press: New York, NY, USA, 1995. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Proportion/Mean (Standard Deviation) |
|---|---|
| Population characteristics (total population = 969) | |
| Gender (%) | |
| Male | 43.0% |
| Female | 57.0% |
| Registered residence status | |
| Local registered resident | 69.0% |
| Nonlocal registered resident | 31.0% |
| Highest education level | |
| Elementary school diploma and below | 41.4% |
| Junior high school diploma | 28.0% |
| Senior high school diploma | 23.8% |
| College degree | 4.1% |
| Bachelor’s degree | 2.6% |
| Post-graduate degree and above | 0.1% |
| Average Age | 70 |
| Individual estimate monthly income | 4531.8 |
| Household per capita monthly income | 2970.2 |
| Housing property rights | |
| Self-owned housing | 63.6% |
| Children’s housing | 12.9% |
| Rental housing | 23.5% |
| Community cohesion | |
| Community interaction: “I think that I know many people in the community” (1–5) | 3.72 (0.971) |
| Community belonging: “I belong to this community” (1–5) | 4.04 (0.882) |
| Community participation: “How often did you participate in community activities in the past 12 months?” (1–5) | 1.73 (0.733) |
| Average community environmental satisfaction (1–5) | 3.98 (0.614) |
| Transportation satisfaction (1–5) | 4.16 (0.726) |
| Shopping satisfaction (1–5) | 4.16 (0.700) |
| Medical satisfaction (1–5) | 3.98 (0.856) |
| Housekeeping maintenance satisfaction (1–5) | 3.87 (0.823) |
| Service and payment satisfaction (1–5) | 3.98 (0.798) |
| Environmental sanitation satisfaction (1–5) | 3.77 (0.993) |
| Public security satisfaction (1–5) | 3.97 (0.831) |
| Greenery satisfaction (1–5) | 3.94 (0.834) |
| Subjective wellbeing | |
| “I think I am happy.” | 4.05 (0.821) |
| Potential Mediators | |
| Physical Health (1–5) | 3.41 (0.892) |
| Feels hard to do heavy exercise activities (such as running, playing, lifting weights, etc.) (1–5) | 2.84 (1.220) |
| Feels hard to do moderate exercise activities (such as lifting tables, cleaning rooms, doing gymnastics, etc.) (1–5) | 3.36 (1.176) |
| Feels hard to climb the stairs (1–5) | 3.17 (1.229) |
| Feels hard to bend and kneel (1–5) | 3.30 (1.209) |
| Feels hard to walk for about 20 min (1–5) | 3.670(1.236) |
| Feels hard to bathe and dress yourself (1–5) | 4.000 (0.924) |
| Has your body been in pain (such as headache, chest tightness, nausea, etc.) in the past four weeks? (1–5) | 3.37 (1.236) |
| Has the physical pain affected your work and housework in the past for weeks? (1–5) | 3.545 (1.180) |
| Mental Health (1–5) | 3.95 (0.766) |
| I feel calm (1–5) | 4.05 (0.800) |
| I feel good and happy (1–5) | 4.02 (0.873) |
| I can concentrate on the things that I am doing (1–5) | 3.99(0.850) |
| I don’t feel stressed (1–5) | 3.88 (1.039) |
| I am not nervous (1–5) | 3.95 (0.931) |
| I don’t feel downcast and nothing can cheer me up (1–5) | 3.94 (0.921) |
| I feel energetic (1–5) | 3.80 (0.931) |
| Association between | Community Environmental Satisfaction | Community Interaction | Community Belonging | Community Participation | Mental Health | Physical Health |
|---|---|---|---|---|---|---|
| Community interaction | 0.171 *** | — | — | — | — | — |
| Community belonging | 0.162 *** | 0.300 *** | — | — | — | — |
| Community participation | — | 0.186 *** | 0.156 *** | — | — | — |
| Mental health | 0.239 *** | 0.111 *** | — | — | — | — |
| Physical health | — | — | — | — | 0.417 *** | — |
| Subjective wellbeing | 0.235 *** | — | 0.213 *** | — | 0.346 *** | — |
| Association Type | Community Environmental Satisfaction | Community Interaction | Community Belonging | Community Participation | Mental Health | Physical Health | |
|---|---|---|---|---|---|---|---|
| Community interaction | Overall association | 0.171 | — | — | — | — | — |
| Direct association | 0.171 | — | — | — | — | — | |
| Indirect association | 0.000 | — | — | — | — | — | |
| Community belonging | Overall association | 0.214 | 0.300 | — | — | — | — |
| Direct association | 0.162 | 0.300 | — | — | — | — | |
| Indirect association | 0.052 | 0.000 | — | — | — | — | |
| Community participation | Overall association | 0.065 | 0.233 | 0.156 | — | — | — |
| Direct association | 0.000 | 0.186 | 0.156 | — | — | — | |
| Indirect association | 0.065 | 0.047 | 0.000 | — | — | — | |
| Mental health | Overall association | 0.258 | 0.111 | — | — | — | — |
| Direct association | 0.239 | 0.111 | — | — | — | — | |
| Indirect association | 0.019 | 0.000 | — | — | — | — | |
| Physical health | Overall association | 0.107 | 0.046 | — | — | 0.417 | — |
| Direct association | 0.000 | 0.000 | — | — | 0.417 | — | |
| Indirect association | 0.107 | 0.046 | — | — | 0.000 | ||
| Subjective wellbeing | Overall association | 0.370 | 0.102 | 0.213 | — | 0.346 | — |
| Direct association | 0.235 | 0.000 | 0.213 | — | 0.346 | — | |
| Direct association | 0.135 | 0.102 | 0.000 | — | 0.000 | — |
| Variables | High-SESI Aging Communities (Percentage/Mean) | Low-SESI Aging Communities (Percentage/Mean) |
|---|---|---|
| Registered residence status (hukou) | ||
| Local registered resident | 75.0% | 62.7% |
| Nonlocal registered resident | 25.0% | 38.3% |
| Highest education level | ||
| Elementary school diploma and below | 30.3% | 56.6% |
| Junior high school diploma | 30.7% | 24.3% |
| Senior high school diploma | 29.8% | 15.7% |
| College degree | 5.7% | 2.0% |
| Bachelor’s degree | 3.4% | 1.5% |
| Post-graduate degree and above | 0.2% | 0.0% |
| Individual estimate monthly income | 5740.8 | 2869.4 |
| Household per capita monthly income | 3514.0 | 2222.5 |
| Housing property rights | ||
| Self-owned housing | 69.7% | 55.1% |
| Children’s housing | 9.3% | 17.9% |
| Rental housing | 21.0% | 27.0% |
| Community cohesion | ||
| Community interaction: “I think that I know many people in the community” (1–5) | 3.50 | 3.76 |
| Community belonging: “I belong to this community” (1–5) | 4.02 | 4.06 |
| Community participation: “How often did you participate in community activities in the past 12 months?” (1–5) | 1.66 | 1.78 |
| Average Community environmental satisfaction (1–5) | 4.06 | 3.87 |
| Transportation satisfaction (1–5) | 4.22 | 4.07 |
| Shopping satisfaction (1–5) | 4.18 | 4.13 |
| Medical satisfaction (1–5) | 4.06 | 3.87 |
| Housekeeping maintenance satisfaction (1–5) | 4.00 | 3.70 |
| Service and payment satisfaction (1–5) | 4.04 | 3.90 |
| Environmental sanitation satisfaction (1–5) | 3.85 | 3.66 |
| Public security satisfaction (1–5) | 4.09 | 3.80 |
| Greenery satisfaction (1–5) | 4.04 | 3.80 |
| Association Type | Community Type | Community Environmental Satisfaction | Community Interaction | Community Belonging | Community Participation | Mental Health | Physical Health | |
|---|---|---|---|---|---|---|---|---|
| Community interaction | Overall association | High-SESI | 0.143 | — | — | — | — | — |
| Low-SESI | 0.227 | — | — | — | — | — | ||
| Direct association | High-SESI | 0.143 | — | — | — | — | — | |
| Low-SESI | 0.227 | — | — | — | — | — | ||
| Indirect association | High-SESI | 0.000 | — | — | — | — | — | |
| Low-SESI | 0.000 | — | — | — | — | — | ||
| Community belonging | Overall association | High-SESI | 0.254 | 0.297 | — | — | — | — |
| Low-SESI | 0.181 | 0.305 | — | — | — | — | ||
| Direct association | High-SESI | 0.212 | 0.297 | — | — | — | — | |
| Low-SESI | 0.112 | 0.305 | — | — | — | — | ||
| Indirect association | High-SESI | 0.042 | 0.000 | — | — | — | — | |
| Low-SESI | 0.069 | 0.000 | — | — | — | — | ||
| Community participation | Overall association | High-SESI | 0.064 | 0.251 | 0.132 | — | — | — |
| Low-SESI | 0.069 | 0.208 | 0.199 | — | — | — | ||
| Direct association | High-SESI | 0.000 | 0.212 | 0.132 | — | — | — | |
| Low-SESI | 0.000 | 0.147 | 0.199 | — | — | — | ||
| Indirect association | High-SESI | 0.064 | 0.039 | 0.000 | — | — | — | |
| Low-SESI | 0.069 | 0.061 | 0.000 | — | — | — | ||
| Mental health | Overall association | High-SESI | 0.218 | 0.113 | — | — | — | — |
| Low-SESI | 0.280 | 0.108 | — | — | — | — | ||
| Direct association | High-SESI | 0.201 | 0.113 | — | — | — | — | |
| Low-SESI | 0.255 | 0.108 | — | — | — | — | ||
| Indirect association | High-SESI | 0.017 | 0.000 | — | — | — | — | |
| Low-SESI | 0.025 | 0.000 | — | — | — | — | ||
| Physical health | Overall association | High-SESI | 0.082 | 0.043 | — | — | 0.379 | — |
| Low-SESI | 0.122 | 0.047 | — | — | 0.435 | — | ||
| Direct association | High-SESI | 0.000 | 0.000 | — | — | 0.379 | — | |
| Low-SESI | 0.000 | 0.000 | — | — | 0.435 | — | ||
| Indirect association | High-SESI | 0.082 | 0.043 | — | — | 0.000 | ||
| Low-SESI | 0.122 | 0.047 | — | — | 0.000 | |||
| Subjective wellbeing | Overall association | High-SESI | 0.347 | 0.107 | 0.246 | — | 0.302 | — |
| Low-SESI | 0.378 | 0.102 | 0.203 | — | 0.369 | — | ||
| Direct association | High-SESI | 0.218 | 0.000 | 0.246 | — | 0.302 | — | |
| Low-SESI | 0.238 | 0.000 | 0.203 | — | 0.369 | — | ||
| Direct association | High-SESI | 0.129 | 0.107 | 0.000 | — | 0.000 | — | |
| Low-SESI | 0.140 | 0.102 | 0.000 | — | 0.000 | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, S.; Zhou, Y.; Yuan, Y. Associations between Community Cohesion and Subjective Wellbeing of the Elderly in Guangzhou, China—A Cross-Sectional Study Based on the Structural Equation Model. Int. J. Environ. Res. Public Health 2021, 18, 953. https://doi.org/10.3390/ijerph18030953
Lai S, Zhou Y, Yuan Y. Associations between Community Cohesion and Subjective Wellbeing of the Elderly in Guangzhou, China—A Cross-Sectional Study Based on the Structural Equation Model. International Journal of Environmental Research and Public Health. 2021; 18(3):953. https://doi.org/10.3390/ijerph18030953
Chicago/Turabian StyleLai, Shulin, Yuquan Zhou, and Yuan Yuan. 2021. "Associations between Community Cohesion and Subjective Wellbeing of the Elderly in Guangzhou, China—A Cross-Sectional Study Based on the Structural Equation Model" International Journal of Environmental Research and Public Health 18, no. 3: 953. https://doi.org/10.3390/ijerph18030953
APA StyleLai, S., Zhou, Y., & Yuan, Y. (2021). Associations between Community Cohesion and Subjective Wellbeing of the Elderly in Guangzhou, China—A Cross-Sectional Study Based on the Structural Equation Model. International Journal of Environmental Research and Public Health, 18(3), 953. https://doi.org/10.3390/ijerph18030953