
The Paternal Experience of Fear of Childbirth: An Integrative Review

Abstract
1. Introduction
1.1. Fear of Childbirth and the Request for Caesarean Section
1.2. Rational for Undertaking This Review
2. Methods
2.1. Design
2.2. Search Strategy
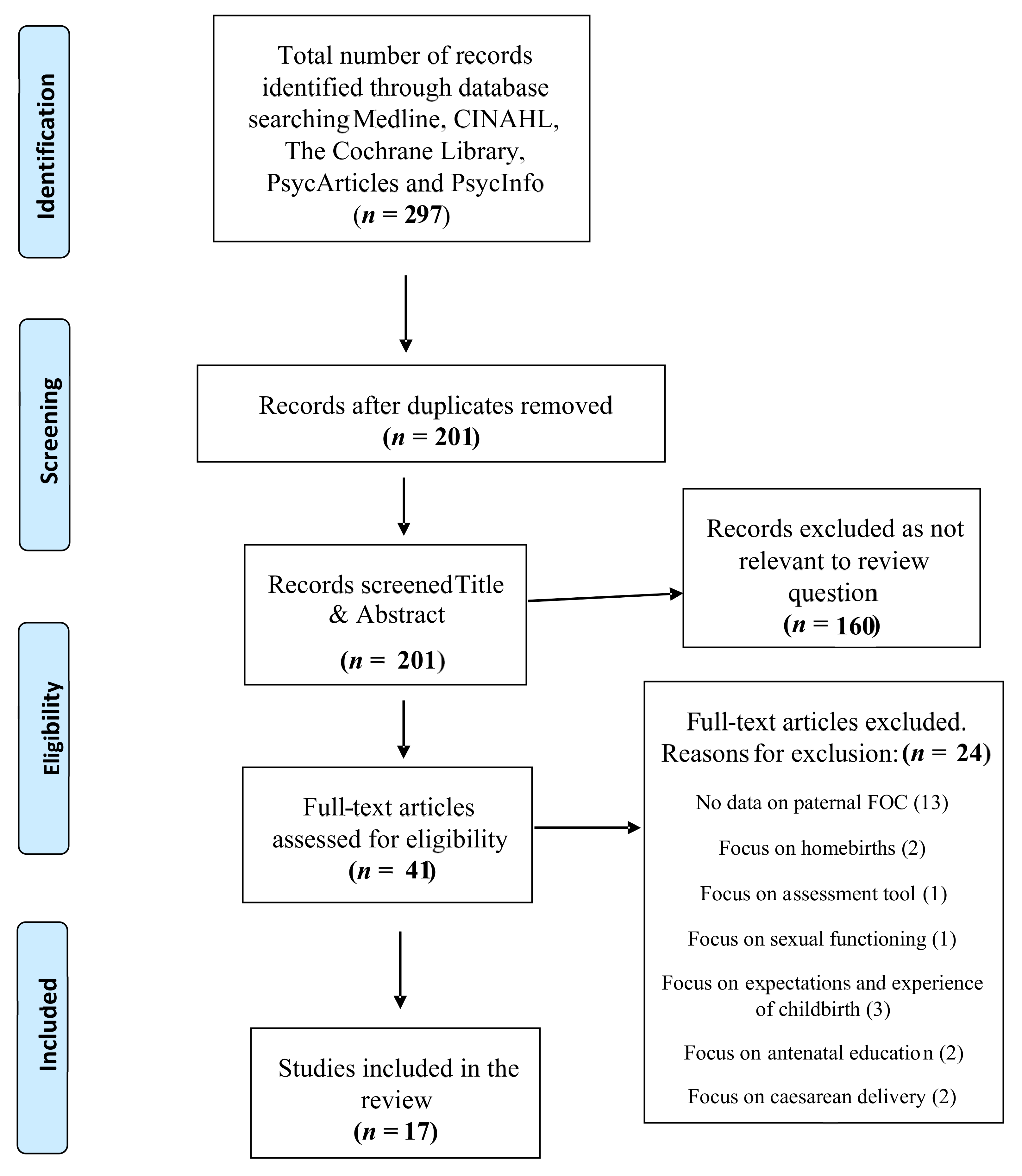
2.3. Search Results
2.4. Critical Appraisal
2.5. Data Extraction, Reduction and Analysis
3. Results
3.1. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
| Author(s), Year, Title, Country | Study Design and Setting | Sample Size and Strategy | Data Collection Methods | Analytical Approach | Findings | Strengths/ Limitations | Quality Appraisal Including CCAT Score |
|---|---|---|---|---|---|---|---|
| Bergström et al. (2013) [13] Fear of childbirth in expectant fathers, subsequent childbirth experience and impact of antenatal education: sub analysis of results from a randomised controlled trial. Sweden. | Quantitative sub analysis of results from a randomised controlled trial (RCT). Of the 83 men identified as having FOC, 39 were randomised to psych prophylaxis childbirth preparation training. The remaining 44 men received standard antenatal preparation without such training. 15 antenatal clinics in Sweden. | Convenience sample of 762 men, of whom 83 (10.9%) were identified as a subsample suffering from FOC based on the data from the W-DEQ. | The W-DEQ, the Cambridge Worry Scale (2 of 16 items excluded and 1 item altered for use in men). | Secondary statistical analysis from a RCT investigating two models of antenatal education. Chi-square tests, t-tests presented as means and standard deviations (SD). | Men with antenatal fear of childbirth more often experienced childbirth as frightening (OR 4.68, 95% CI) and reported feeling unprepared for childbirth (OR 4.04; 95% CI 2.08–7.84) compared with men without fear. Participants in the psych prophylaxis group had a lower risk of experiencing childbirth as frightening compared with those receiving standard antenatal preparation (OR 0.30: 95% CI 0.10–0.95). | The W-DEQ piloted for use in men prior to use and 8 of the 33 items were excluded since they were deemed irrelevant to men. Cut-off value of >60 set on the adapted W-DEQ. Further testing of the validity and reliability of the instrument for use in men is warranted. Secondary analysis of data from a trial originally designed for other hypotheses. | CCAT score 31/40 (77%). Validity of the W-DEQ tool tested through piloting. Conflict of interest and relationship between researchers and participants not addressed. |
| Chalmers and Meyer (1996) [47] What men say about pregnancy, birth and parenthood. South Africa. | Quantitative study (methodological design not identified). One public hospital and one private hospital. | Convenience sample of 150 first-time fathers split into three groups of 50. Participants were recruited equally between the two hospital settings. | Fathers in each group were asked to complete one questionnaire on their perception of their partners’ pregnancy (response rate 92%, n = 46), or their experience of antenatal education (response rate 72%, n = 36), or their experience of the birth (response rate 66%, n = 33). A follow-up questionnaire about parenthood experience was requested of all participants, with a response rate of 49.6% (n = 57). | Descriptive statistics. | The most significant fears experienced by men during pregnancy were the fear of abnormality in the baby (71%), not being at the birth (47.8%), partner experiencing pain (43.5%), and partner or baby dying (41.3%). 30.4% of men reported feeling more anxious than before pregnancy, more emotional (13.4%) and more irritable (8.7%). The most important source of emotional support for men was their partner (63.9%). | Methodological and data analysis approaches not identified. Cultural bias identified. Screening tools not used to assess FOC. Participants recruited from both the public and private hospital to represent both health care systems but no comparative results reported between the two hospitals. | CCAT score 19/40 (47%). Methodological design not explicit. Sample bias identified. Reports that questionnaires were pilot tested but no details provided of pilot. |
| Eriksson et al. (2005) [11] Experiential factors associated with childbirth-related fear in Swedish women and men: A population based study. Sweden. | Quantitative cross-sectional survey. Swedish hospital setting. | A convenience sample of 558 women and 552 men. Response rate (n = 410, 73% women) and (n = 329, 59% men). Participants identified via health records of their infants at primary health care centres. | Questionnaire, pilot tested for face validity. | Descriptive statistics including means and standard deviations. | 13% of the men were assessed as having intense fear of childbirth, 29% moderate fear. 98% of men with intense fear and 92% with mild/moderate fear felt afraid that their child would not be born healthy. Men with intense fear were more often 40 years of age or older. 56% of men with intense fear did not disclose their fear as they did not want to worry their partner. 49% with intense fear felt it best to keep the fear to themselves. | Lower response rate among male participants. Questionnaire was pilot tested in 10 men and 10 women, with minor adjustments made prior to use in study. | CCAT score 31/40 (77%). Possible response bias identified due to lack of information on non-responding male participants. Retrospective design may have introduced recall bias. Conflict of interest not reported. |
| Eriksson et al. (2006) [4] Content of childbirth-related fear in Swedish women and men- analysis of an open-ended question. Sweden. | Quantitative Cross-sectional survey, retrospective design. Hospital setting in Northern Sweden. | A random sample of 558 mothers and 552 fathers. Response rate to questionnaire (n = 410, 75%) mothers and (n = 329 60%) fathers. Of the respondents with experience of childbirth-related fear (n = 308, 94%) mothers and (n = 194, 82%) fathers answered the open-ended question. Participants identified via health records of their infants at primary health care centres. | Self-rated questionnaire. Use of both fixed and open-ended questions. | Open-ended question analysed using content analysis. Chi-square tests were used to report proportional differences between participants with intense and mild–moderate FOC. | Predominant fears of fathers included the health and life of the baby (79%), injury to the child during birth (41%), the health and life of the woman (49%), the woman being injured during labour (45%). | Questionnaire was answered 1.5 years after the birth (retrospective design). The time delay may have altered recall of the birth event and/or specific details. Participants did not consent to have their details taken from health records. Open-ended questions enabled parents to describe their fears in their own words, giving a deeper insight. Content analysis coded by all three researchers. | CCAT score 28/40 (70%). Recall bias. |
| Eriksson et al. (2007) [40] Men’s experience of intense fear related to childbirth investigated in a Swedish qualitative study. Sweden. | Qualitative study, grounded theory design Interviews conducted in a setting of the participants’ choice. | Sample of 22 men. Sampling strategy not identified. Participants were identified as having FOC through participation in a previous survey. | Interviews guided by open-ended questions and a permissive strategy. | Similarity- difference grounded theory approach (Strauss and Corbin, 1990). | Content of childbirth fear was primarily described as being related to the health and life of their partner and child, obstetric staff competence/behaviour and their own capabilities /reactions. The manifestation of fear was often described as a mental occupation. Some of the strategies that participants used to deal with their fear was an attempt to increase their sense of control and diminish the emotion of fear. | All 3 authors participated individually and collectively in coding and characterisation of data and in establishing meaning and content, which added to the confirmability and reliability of reporting. Validity of original survey tool for assessing childbirth fear among participants unclear. | CCAT score 32/40 (80%). Fathers’ interviews were conducted between two and three years after their child’s birth, which may have introduced a recall bias. |
| Etheridge and Slade (2017) [9] “Nothing’s actually happened to me.”: the experience of fathers who found childbirth traumatic. U.K. | Mixed-methods study. | A volunteer sample of 11 fathers. Participants recruited via advert on the Birth Trauma Association Website, in a newsletter and on two internet forums. | The Impact of Event Scale (IES) questionnaire and semi- structured telephone interviews. | Thematic analysis using template analysis. | 10 of the 11 men (90%) described fears that their partner or baby would die. The pain of the woman and her suffering had a direct effect on the man and his distress mirrored hers. 7 fathers (63%) referred to “trying to keep it together” and be strong for their partner. Preoccupation and rumination was a feature for some men in the weeks, months and even years after the birth. | Reliability and validity of IES reported. Two men had received previous treatment for depression. Variations in length of time since birth ranged from 2 months to 6 years, which may introduce recall bias. | CCAT score 32/40 (80%). Participant’s right to withdraw reported. Volunteer bias. Suitability of sampling method or sample size not reported. |
| Greer et al. (2014) [41] ‘Fear of childbirth’ and ways of coping for pregnant women and their partners during the birthing process: a salutogenic analysis. Northern Ireland. | Qualitative study (methodological underpinning not reported). Some of the interviews were conducted in the hospital setting and others in the participant’s homes. | A purposive sample of 19 women and 19 men. | In-depth semi- structured interviews. | Thematic content analysis. | Participants were fearful that their partner would be unable to cope with and be traumatised by the pain of childbirth and that their partner’s postnatal mental health would be affected. Participants felt labour and birth posed considerable risks to the physical health of the mother and baby. Some of the participants feared that their baby was too big to be born vaginally. | Study participants all attended the same health care setting (consultant-led hospital), which may have impacted the heterogeneity of sample. Confidentiality, privacy and informed written consent all considered. | CCAT score 26/40 (65%). No demographic details of participants reported but available through visiting a website. Dependability and rigor of data analysis method not reported. Conflict of interest not reported. |
| Hildingsson (2014a) [14] Swedish couples’ attitudes towards birth, childbirth fear and birth preferences and relation to mode of birth- A longitudinal cohort study. Sweden. | Quantitative Longitudinal cohort study. Three hospital settings Mid-North Sweden. | A convenience sample of 1074 pregnant women and their partners. | Two questionnaires—first one administered mid-pregnancy and the second two months after the birth. | Descriptive and inferential statistics (chi-square and t-tests) and multinomial regression analysis. | 15% of women and 5% of men had childbirth fear. Birth preferences and fear were strongly associated with mode of birth. Men rated women’s health and wellbeing higher while women prioritised the baby’s health. | Not all dimensions of FOC were covered within the questionnaire as overall purpose was to explore various components including early parenthood. A validated tool to screen for FOC was not utilised. | CCAT score 31/40 (77%). Confounding variables reported. Suitability of sample size was not discussed. |
| Hildingsson et al. (2014b) [43] Childbirth fear in Swedish fathers is associated with parental stress as well as poor physical and mental health. Sweden. | Longitudinal regional survey. Three hospital settings Mid-North Sweden. | A convenience sample of 1047 expectant fathers. 59% (n = 620) of fathers completed all three questionnaires. | Three questionnaires—first delivered in late pregnancy, second at two months postpartum and third one year postpartum. The Fear of Birth Scale (FOCS), self-reported physical and mental health assessment, and the Swedish Parental Stress Questionnaire (SPSQ). | Descriptive statistics. Crude and adjusted odds ratios (OR) with a 95% confidence interval (CI) were calculated between fathers who scored higher fear of birth and those who scored lower fear of birth. | Childbirth-related fear was present in 13.6% of fathers as assessed using the FOCS. Respondents with scores of >50 in the FOCS were identified as those with greater fear. These fathers were more likely to rate their physical (OR 1.8; CI 95% 1.2–2.8) and mental health (OR 3.0; 1.8–5.1) as poor compared to fathers without FOC. Fearful fathers were more likely to perceive difficulties in pregnancy (OR 2.1; 1.4–3.0) forthcoming birth (OR 4.3; 2.9–6.3) and parenthood (OR 1.4; 0.9–2.0) than fathers without FOC. Higher levels of self-rated stress were also present in men with FOC at 12 months postpartum. | Limited to Swedish-speaking fathers only. Large sample size but a high level of non-responders (41%) for final stage. Convenience sample may cause volunteer bias. | CCAT score 28/40 (70%). Reliability and validity of the FOCS and cut-off point of >50 highlighted. Confidentiality and researcher’s relationship with participants not reported. |
| Hildingsson et al. (2014c) [45] Childbirth fear in expectant fathers: Findings from a regional Swedish cohort study. Sweden. | Regional cohort study, part of a prospective longitudinal cohort study. Three hospital settings Mid-North Sweden. | A convenience sample of 1414 expectant fathers. Response rate (n = 1047, 74%). | Self-reported questionnaire using a five-point Likert scale and the FOCS. | Statistical analysis using crude and adjusted odds ratios with a 95% CI, logistic regression analysis. | 13.6% of expectant fathers were identified as having FOC through assessment using the FOCS. Scores of >50 were used as a cut-off point to identify those with FOC. Fathers reporting FOC were more likely born in a country outside Sweden (OR 2.8; 1.3–6.1) be first-time fathers (OR 1.8; 1.2–2.6), prefer a caesarean birth (OR 2.1; 1.7–4.1) and have more frequent childbirth-related thoughts in mid-pregnancy (OR 1.9; 1.1–2.0). Men with FOC were also less likely to agree with the statement that giving birth is a natural process. | Reliability and validity of the FOCS for use in men not reported. Fairly large sample size across three hospital settings. | CCAT score 30/40 (75%). Validity of cut-off point for the FOCS >50 not determined in male population. Low response rate. |
| Hunter et al. (2011) [16] Satisfaction and use of spiritually based mantram interventions for child-birth related fears in couples. U.S.A. | Mixed-methods design. Experimental and interviews. Urban military medical centre. | A convenience sample of 20 pregnant women and 9 male partners. Randomly assigned into intervention or control group. Control group: childbirth course only. Intervention group: childbirth course and mantram program. | The W-DEQ, the Client Satisfaction Questionnaire and six-month follow up via telephone interview. | Descriptive statistics and inferential statistics (t tests, chi-square and Cramer’s V statistics). | Males’ W-DEQ scores ranged from 73 to 96. No significant difference in FOC between intervention and control group. There was not sufficient evidence to confirm that mantram repetition is beneficial for managing FOC due to small sample size and incomplete data from questionnaires. Eight respondents in the intervention group (Women (n = 5) and men (n = 3)) completed a satisfaction questionnaire. 75% reported high satisfaction and 25% medium satisfaction. There was no breakdown of these percentages by sex. | The majority of participants were active duty military or military dependants, which may reduce generalisability. Convenience sample may lead to volunteer bias. Poor enrolment rate of 20% (of 134 potential participants) resulted in small sample size. No fathers completed the six-month follow-up interview. Uneven distribution of ethnicity. | CCAT score 28/40 (70%). Sampling bias identified. Construct validity was performed for use of the W-DEQ by means of correlation with other questionnaire scales. |
| Kannenberg et al. (2016) [46] Treatment-associated anxiety among pregnant women and their partners: What is the influence of sex, parity, age and education? Germany. | Quantitative cross-sectional survey. Women’s hospital setting, Germany. | A sample of 259 pregnant women and 183 male partners. Sampling strategy not identified. | State-Trait Anxiety Inventory (STAI) and self-assessment questionnaire. | Statistics ANOVA and t-tests. | Fathers did not report reduced scores for FOC with second or subsequent children as was found for women. Fear of foetal malformation was found to be more anxiety provoking in parents with higher levels of education. Fear for the unborn child’s health was the most prominent fear. Anxiety rose in both men and women as gestational age increased. | Reliability and validity of questionnaires used not reported. Methods to ensure participant’s confidentiality not reported. Conflict of interest reported. | CCAT score 24/40 (60%). Study participants consisted of couples attending hospital care who are at higher risk of obstetric complication than those who attend practice gynaecologists or midwifery care in this health setting. Thus results may not be fully representative. |
| Schytt and Hildingsson (2011) [48] Physical and emotional self-rated health among Swedish women and men during pregnancy and the first year of parenthood. Sweden. | Quantitative longitudinal study. Three hospital settings Mid-North Sweden. | Sample of 1506 women and 1414 male partners. Response rate: 80% (n= 1212) women and 78% (n= 1105) men completed the first questionnaire, 50% (n= 763) women and 46% (n = 655) men completed the final questionnaire. | A total of 4 questionnaires—Q1: completed in the second trimester, Q2: in the third trimester, Q3: two months postpartum and Q4: one year postpartum. | Statistical analysis (Friedman’s test, Wilcoxon signed rank test). | 30% of men with childbirth-related fears rated poor physical self-rated health and 27% poor emotional self-rated health in late pregnancy. With poor physical self-rated health among 42% and poor emotional self-rated health in 37% one year after birth. Poor emotional self-rated health was associated with having children previously, childbirth-related fear, pronounced emotional changes during pregnancy and perceived stress when facing the forthcoming parenthood. | Reliability and validity of questionnaire assessing childbirth-related fears not reported. Ethical approval and any conflict of interest not reported. | CCAT score 27/40 (67%). High attrition rates. Participation was limited to those with mastery of the Swedish language. |
| Schytt and Bergström (2014) [17] First-time fathers’ expectation and experience of childbirth in relation to age. Sweden. | Secondary data analysis from a randomised control trial. 15 antenatal clinics across Sweden. | Of the 1064 trial participants, 777 first-time fathers who completed the follow-up questionnaire were included. Divided into three groups: young men <27 years (n = 188), men of average age 28–33 years (n = 389) and men of advanced age >34 years (n = 200). | Two questionnaires—first completed in mid-pregnancy the second at follow-up 3 months postpartum. The W-DEQ was used to measure fearful expectations. Single-item questions on worry were retrieved from the Cambridge Worry Scale. | Statistical analysis (X2-tests, t-tests, multivariable logistic regression analysis). | 29% of the advanced aged men reported mixed or negative feelings compared with 27% average age and 17% young age (p = <0.05). Fearful expectations were most pronounced in the older cohort of men. The total sum score on the W-DEQ for men in the advanced age category was 43.3 (SD 16.9), compared with 42.9 (SD 13.5) in men of average age and 38.7 (SD 15.7) in the youngest age category. | The W-DEQ piloted for use in expectant fathers and validity of scale reported. Large sample size. | CCAT score 32/40 (80%). Sample bias may exist as participants took part in a trial on antenatal education and may not be representative of population. Confounding variables reported. |
| Shibli-Kometiani and Brown (2012) [1] Fathers’ experiences accompanying labour and birth. Israel. | A phenomenological qualitative study. Interviews took place in participants’ own home. | A purposive sample of 8 fathers. Suitable participants were identified through the labour ward register. | Semi-structured interviews. | Colaizzi (1978) framework for data analysis. | Every participant expressed significant levels of fear, anxiety and helplessness as labour progressed. They feared their partners and baby might die. As their distress increased, they became passive and less supportive. A knowledge deficit about labour served to increase their anxiety. | Couples the researcher had cared for personally were excluded to reduce bias. Management of data, confidentiality, written consent and participants’ right to withdraw were reported. Sample representative of the cultural diversity of the region. Small sample size. Screening tools not used to assess FOC. | CCAT score 26/40 (65%). Limited discussion and interpretation of results within context of current knowledge. Rigor of chosen analytical method not reported. No statement of ethical approval. |
| Somers-Smith (1998) [42] A place for the partner? Expectations and experiences of support during childbirth. U.K. | A qualitative study using an ethnographic approach Two consultant-led maternity units in Hampshire, U.K. | A purposive sample of 13 couples; response rate 61% (n = 8 couples). | Two semi-structured interviews—first conducted six weeks before the birth and second approx. twelve weeks after the birth. | Thematic analysis guided by Miles and Huberman (1994). | One fear voiced was the possibility of their partner dying. Other fears men expressed were the possibility of fainting, panicking and if they would be able ‘to keep it together’. The men mostly kept their fears to themselves. One father relied on cues from the midwife to minimise his anxiety during the labour. | Small sample with refusal rate of 39%. No participants from lower social economic groups and limited ethnic diversity among participants. Screening tools not used to assess FOC. | CCAT score 28/40 (70%). Exclusion criteria not reported. Relationship between the researcher and participants not reported. Conflict of interest not reported. |
| Szeverényi et al. (1998) [44] Contents of childbirth-related fear among couples wishing the partner’s presence at delivery. Hungary. | Cross-sectional survey. Distributed at self-referred antenatal parent craft preparation course. | Convenience sample of 216 couples. | Questionnaire designed by Ringler (1985) included 49 items for women and 52 items for men. | Analytical approach not identified. Statistical summary of results presented in tables. | Approx. 80% of couples had fears relating to childbirth. 13% of men had a strong fear and 11% a very strong fear of caesarean delivery. 15.7% of men were very afraid that their wife could die and 5.6% quite afraid. 14.8% were very afraid their baby may be stillborn and 11.1% quite afraid. | First study of its kind in Hungary. Only partners who attended the 3 parent craft preparation courses were permitted to attend the birth of the baby. 100% of couples completed the questionnaire. Potential response bias and lack of generalisability may be present due to the couples being self-referred. Screening tools not used to assess FOC. | CCAT 19/40 (47%). Poorly described methodology. Validity and reliability of questionnaire reported using analysis of variance. Suitability of sample size and exclusion criteria not reported. Ethical approval not reported. |
3.2. Focus of Fear
3.2.1. The Health and Life of the Baby
3.2.2. The Health and Life of the Partner
3.2.3. Reactions and Behaviour
3.3. Impact on Health and Wellbeing
3.3.1. Mental Health
3.3.2. Physical Health
3.3.3. Coping Mechanisms and Avoidance
3.4. A Private Burden
3.4.1. Gender Constructs
3.4.2. Non-Disclosure
3.4.3. Giving Support
3.4.4. Receiving Support
4. Discussion
4.1. Paternal PMH and Childbirth Fears
4.2. Overcoming Barriers and Screening
4.3. Self-Efficacy and Antenatal Education
5. Recommendations for Future Research
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Shibli-Kometiani, M.; Brown, A. Fathers’ experiences accompanying labour and birth. Br. J. Midwifery 2012, 20, 339–344. [Google Scholar] [CrossRef]
- Darwin, Z.; Galdas, P.; Hinchliff, S.; Littlewood, E.; Mcmillan, D.; Mcgowan, L.; Gilbody, S. Fathers’ Views and Experiences of Their Own Mental Health during Pregnancy and the First Postnatal Year: A Qualitative Interview Study of Men Participating in the UK Born and Bred in Yorkshire (BaBY) Cohort. 2017. Available online: http://eprints.whiterose.ac.uk/109125/13/art%253A10.1186%252Fs12884-017-1229-4.pdf (accessed on 14 November 2019).
- Hanson, S.; Hunter, L.P.; Bormann, J.R.; Sobo, E.J. Paternal Fears of Childbirth: A Literature Review. J. Perinat. Educ. 2009, 18, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, C.; Westman, G.; Hamberg, K. Content of Childbirth-Related Fear in Swedish Women and Men-Analysis of an Open-Ended Question. J. Midwifery Women’s Health 2006, 51, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Leach, L.; Poyser, C.; Cooklin, A.; Giallo, R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: A systematic review. J. Affect. Disord. 2016, 190, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Philpott, L.F.; Leahy-Warren, P.; FitzGerald, S.; Savage, E. Stress in fathers in the perinatal period: A systematic review. Midwifery 2017, 55, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Saxbe, D.; Horton, K.T.; Tsai, A.B. The Birth Experiences Questionnaire: A brief measure assessing psychosocial dimensions of childbirth. J. Fam. Psychol. 2018, 32, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Bastos, M.H.; Furuta, M.; Small, R.; McKenzie-McHarg, K.; Bick, D. Debriefing interventions for the prevention of psychological trauma in women following childbirth. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Etheridge, J.; Slade, P.P. “Nothing’s actually happened to me.”: The experiences of fathers who found childbirth traumatic. BMC Pregnancy Childbirth 2017, 17, 1–15. [Google Scholar] [CrossRef]
- Paulson, J.F.; Bazemore, S.D. Prenatal and postpartum depression in fathers and its association with maternal depression: A meta-analysis. J. Am. Med. Assoc. 2010, 303, 1961–1969. [Google Scholar] [CrossRef]
- Eriksson, C.; Westman, G.; Hamberg, K. Experiential factors associated with childbirth-related fear in Swedish women and men: A population-based study. J. Psychosom. Obstet. Gynecol. 2005, 26, 63–72. [Google Scholar] [CrossRef]
- Ganapathy, T. Tokophobia among First Time Expectant Fathers. J. Depress. Anxiety 2015. [Google Scholar] [CrossRef]
- Bergström, M.; Rudman, A.; Waldenström, U.; Kieler, H. Fear of childbirth in expectant fathers, subsequent childbirth experience and impact of antenatal education: Sub analysis of results from a randomised control trial. Acta Obstet. Gynecol. Scand. 2013, 92, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Hildingsson, I. Swedish couples’ attitudes towards birth, childbirth fear and birth preferences and relation to mode of birth- A longitudinal cohort study. Sex. Reprod. Healthc. 2014, 5, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Wijma, K.; Wijma, B.; Zar, M. Psychometric aspects of the W-DEQ; a new questionnaire for the measurement of fear of childbirth. J. Psychosom. Obstet. Gynecol. 1998, 19, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Hunter, L.; Bormann, J.; Belding, W.; Sobo, E.J.; Axman, L.; Reseter, B.K.; Hanson, S.; Anderson, V.M. Satisfaction and use of a spiritually based mantram intervention for childbirth-related fears in couples. Appl. Nurs. Res. 2011, 24, 138–146. [Google Scholar] [CrossRef]
- Schytt, E.; Bergström, M. First-time fathers’ expectations and experiences of childbirth in relation to age. Midwifery 2014, 30, 82–88. [Google Scholar] [CrossRef]
- Nilsson, C.; Hessman, E.; Sjöblom, H.; Dencker, A.; Jangsten, E.; Mollberg, M.; Patel, H.; Sparud-Lundin, C.; Wigert, H.; Begley, C. Definitions, measurements and prevalence of fear of childbirth: A systematic review. BMC Pregnancy Childbirth 2018, 18, 28. [Google Scholar]
- Demšar, K.; Svetina, M.; Verdenik, I.; Tul, N.; Blickstein, I.; Globevnik Velikonja, V. Tokophobia (fear of childbirth): Prevalence and risk factors. J. Perinat. Med. 2018, 46, 51–154. [Google Scholar] [CrossRef]
- Betrán, A.P.; Ye, J.; Moller, A.B.; Zhang, J.; Gülmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar]
- Saisto, T.; Salmela-Aro, K.; Nurmi, J.E.; Halmesmäki, E. Psychosocial characteristics of women and their partners fearing vaginal childbirth. Int. J. Obstet. Gynaecol. 2003, 108, 492–498. [Google Scholar] [CrossRef]
- Gao, Y.; Tang, Y.; Tong, M.; Du, Y.; Chen, Q. Does attendance of a prenatal education course reduce rates of caesarean section on maternal request? A questionnaire study in a tertiary women hospital in Shanghai, China. BMJ Open 2019, 9, e029437. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Recommendations Non-Clinical Interventions to Reduce Unnecessary Caesarean Sections; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Serçekuş, P.; Cetisli, N.E.; Hatice Inci, F. Birth preferences by nulliparous women and their partners in Turkey. Sex. Reprod. Healthc. 2015, 6, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Scollato, A.; Lampasona, R. Tokophobia: When fear of childbirth prevails. Mediterr. J. Clin. Psychol. 2013, 1. [Google Scholar] [CrossRef]
- Tandu-Umba, B.; Dedetemo, D.K.; Mananga, G.L. Maternal Stress and Pregnancy Outcomes. Open J. Obstet. Gynecol. 2014. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Culhane, J.F.; Rauh, V.; Barve, S.S. Stress and Preterm Birth: Neuroendocrine, Immune/Inflammatory, and Vascular Mechanisms. Matern. Child Health J. 2001, 5, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.G.; Beattie, J.; Lau, R.; East, C.; Biro, M.A. Mindfulness and perinatal mental health: A systematic review. Women Birth 2016, 29, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Ramchandani, P.; Domoney, J.; Sethna, V.; Psychogiou, L.; Vlachos, H.; Murray, L. Do early father–infant interactions predict the onset of externalizing behaviours in young children? Findings from a longitudinal cohort study. J. Child Psychol. Psychiatry 2013, 54, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ayer, L.; Kohl, P.; Malsberger, R.; Burgette, L. The impact of fathers on maltreated youths’ mental health. Child. Youth Serv. Rev. 2016, 63, 16–20. [Google Scholar] [CrossRef]
- Fletcher, R.; Garfield, C.F.; Matthey, S. Fathers’ Perinatal Mental Health: Identifying Perinatal Depression and Anxiety: Evidence-Based Practice in Screening, Psychosocial Assessment, and Management; John Wiley & Sons: Chichester, UK, 2015. [Google Scholar]
- Philpott, L.F.; Savage, E.; FitzGerald, S.; Leahy-Warren, P. Anxiety in fathers in the perinatal period: A systematic review. Midwifery 2019, 76, 54–101. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Clarke, J. What is a systematic review? Evid. Based Nurs. 2011, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Bettany-Saltikov, J. How to Do a Systematic Literature Review in Nursing: A Step-by-Step Guide; Open University Press: Berkshire, UK, 2012. [Google Scholar]
- Crowe, M. Crowe Critical Appraisal Tool (CCAT) User Guide; Conchra House: Scotland, UK, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Clarke, V.; Braun, V. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. Psychologist 2013, 26, 120–123. [Google Scholar]
- Eriksson, C.; Salander, P.; Hamberg, K. Men’s experiences of intense fear related to childbirth investigated in a Swedish qualitative study. J. Men’s Health Gend. 2007, 4, 409–418. [Google Scholar] [CrossRef]
- Greer, J.; Lazenbatt, A.; Dunne, L. Fear of childbirth and ways of coping for pregnant women and their partners during the birthing process: A salutogenic analysis. Evid. Based Midwifery 2014, 12, 95–100. [Google Scholar]
- Somers-Smith, M.J. A place for the partner? Expectations and experiences of support during childbirth. Midwifery 1998, 15, 101–108. [Google Scholar] [CrossRef]
- Hildingsson, I.; Haines, H.; Johansson, M.; Rubertsson, C.; Fenwick, J. Childbirth fear in Swedish fathers is associated with parental stress as well as poor physical and mental health. Midwifery 2014, 30, 248–254. [Google Scholar] [CrossRef]
- Szeverényi, P.; Póka, R.; Hetey, M.; Török, Z. Contents of childbirth-related fear among couples wishing the partner’s presence at delivery. J. Psychosom. Obstet. Gynecol. 1998, 19, 38–43. [Google Scholar] [CrossRef]
- Hildingsson, I.; Johansson, M.; Fenwick, J.; Haines, H.; Rubertsson, C. Childbirth fear in expectant fathers: Findings from a regional Swedish cohort study. Midwifery 2014, 30, 242–247. [Google Scholar] [CrossRef]
- Kannenberg, K.; Weichert, J.; Rody, A.; Banz-Jansen, C. Treatment-Associated Anxiety among Pregnant Women and their Partners: What is the Influence of Sex, Parity and Education? Geburtshlife Frauenheilkd. 2016, 76, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, B.; Meyer, D. What men say about pregnancy, birth and parenthood. J. Psychosom. Obstet. Gynaecol. 1996, 17, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Schytt, E.; Hildingsson, I. Physical and emotional self-rated health among Swedish women and men during pregnancy and the first year of parenthood. Sex. Reprod. Healthc. 2011, 2, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Bergström, M.; Kieler, H.; Waldenström, U. Effects of natural childbirth preparation versus standard antenatal education on epidural rates, experience of childbirth and parental stress in mothers and fathers: A randomized controlled multicentre trial. BJOG 2009, 116, 1167–1176. [Google Scholar] [PubMed]
- Ruffell, B.; Smith, D.M.; Wittkowski, A. The Experiences of Male Partners of Women with Postnatal Mental Health Problems: A Systematic Review and Thematic Synthesis. J. Child Fam. Stud. 2019, 28, 2772–2790. [Google Scholar] [CrossRef]
- Poggi, L.; Goutaudier, N.; Séjourné, N.; Chabrol, H. When Fear of Childbirth is Pathological: The Fear Continuum. Matern. Child Health J. 2018, 22, 772–778. [Google Scholar]
- Aktar, E.; Qu, J.; Lawrence, P.J.; Tollenaar, M.S.; Elzinga, B.M.; Bögels, S.M. Foetal and Infant Outcomes in the Offspring of Parents with Perinatal Mental Disorders: Earliest Influences. Front. Psychiatry 2019. [Google Scholar] [CrossRef]
- Badaoui, A.; Kassm, S.A.; Naja, W. Fear and Anxiety Disorders Related to Childbirth: Epidemiological and Therapeutic Issues. Curr. Psychiatry Rep. 2019, 21, 27. [Google Scholar] [CrossRef]
- Higgins, A.; Carroll, M.; Downes, C.; Monahan, M.; Gill, A.; Madden, D.; McGoldrick, E.; Nagel, U. Perinatal Mental Health: An Exploration of Practices, Policies, Processes and Education Needs of Midwives and Nurses within Maternity and Primary Care Services in Ireland; Health Service Executive: Dublin, Ireland, 2017. [Google Scholar]
- Singley, D.B.; Edwards, L.M. Men’s perinatal mental health in the transition to fatherhood. Prof. Psychol. Res. Pract. 2015, 46, 309–316. [Google Scholar] [CrossRef]
- Huusko, L.; Sjöberg, S.; Ekström, A.; Hertfelt Wahn, E.; Thorstensson, S. First-Time Fathers’ Experience of Support from Midwives in Maternity Clinics: An Interview Study. Nurs. Res. Pract. 2018, 7. [Google Scholar] [CrossRef]
- Chandler, S.; Field, P.A. ‘Becoming a father. First-time fathers’ experience of labor and delivery’. J. Nurse Midwifery 1997, 42, 17–24. [Google Scholar] [CrossRef]
- O’Brien, A.; Mcneil, K.; Fletcher, R.; Conrad, A.; Wilson, A.; Jones, D.; Chan, S. New Fathers’ Perinatal Depression and Anxiety-Treatment Options: An Integrative Review. Am. J. Men’s Health 2017, 11, 863–876. [Google Scholar]
- Williams, M. Assessing and managing paternal mental health issues. Nurs. Times 2017, 114, 26–29. [Google Scholar]
- Rouhe, H.; Salmela-Aro, K.; Toivanen, R.; Tokola, M.; Halmesmäki, E.; Ryding, E.; Saisto, T. Group psychoeducation with relaxation for severe fear of childbirth improves maternal adjustment and childbirth experience—A randomized controlled trial. J. Psychosom. Obstet. Gynecol. 2015, 36, 1–9. [Google Scholar] [CrossRef]
- Rondung, E.; Thomtén, J.; Sundin, O. Psychological perspectives on fear of childbirth. J. Anxiety Disord. 2016, 44, 80–91. [Google Scholar]
- Serçekuş, P.; Başkale, H. Effects of antenatal education on fear of childbirth, maternal self-efficacy and parental attachment. Midwifery 2016, 34, 166–172. [Google Scholar] [CrossRef]
- Erlandsson, K.; Häggström-Nordin, E. Prenatal Parental Education from the perspective of Fathers with Experience as Primary Caregiver Immediately Following Birth: A Phenomenographic Study. J. Perinat. Educ. 2010, 19, 19–28. [Google Scholar]
- Fenwick, J.; Bayes, S.; Johansson, M. A qualitative investigation into the pregnancy experiences and childbirth expectations of Australian fathers-to-be. Sex. Reprod. Healthc. 2012, 3, 3–9. [Google Scholar]
- Premberg, A.; Lundgren, I. Fathers’ Experiences of Childbirth Education. J. Perinat. Educ. 2006, 15, 21–28. [Google Scholar] [CrossRef]
- Kunjappy-Clifton, A. And father came too…a study exploring the role of first-time fathers during the birth process and to explore the meaning of the experience for these men: Part two. MIDRIS 2008, 18, 57–66. [Google Scholar]
- Persson, E.K.; Fridlund, B.; Kvist, L.J.; Dykes, A.K. Fathers’ sense of security during the first postnatal week—A qualitative interview study in Sweden. Midwifery 2012, 28, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Sponsler, W.; Weatherspoon, C.; Weatherspoon, D.; Campbell, D. Fear of Fatherhood. Int. J. Childbirth Educ. 2015, 30, 33–37. [Google Scholar]
- Hugill, K.; Harvey, M. Fatherhood in Midwifery and Neonatal Practice; Quay Books Division: London, UK, 2012. [Google Scholar]
- Longworth, H.L.; Kingdon, C.K. Fathers in the birth room: What are they expecting and experiencing? A phenomenological study. Midwifery 2011, 27, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Dellmann, T. The best moment of my life: A literature review of fathers’ experiences of childbirth. Aust. Midwifery J. 2004, 17, 20–26. [Google Scholar]
- Johansson, M.; Rådestad, I.; Rubertsson, C.; Karlström, A.; Hildingsson, I. Few fathers-to-be prefer caesarean section for the birth of their baby. Int. J. Obstet. Gynaecol. 2010, 117, 1–9. [Google Scholar] [CrossRef]
- Striebich, S.; Mattern, E.; Ayerle, G.M. Support for pregnant women identified with fear of childbirth (FOC)/tokophobia—A systematic review of approaches and interventions. Midwifery 2018, 61, 97–115. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef]



| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Quantitative, qualitative and mixed-methods studies. | Studies examining fathers with other co-morbidities or mental health diagnoses. |
| Studies relating to the experience of FOC * among fathers. Studies with data relating to FOC among fathers. Studies examining FOC among couples with extractable data relating to fathers. Studies among both first-time fathers and fathers with previous children. Studies published in English. | Studies relating to FOC where a diagnosis of foetal abnormality had been confirmed in pregnancy. Studies published in a language other than English. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moran, E.; Bradshaw, C.; Tuohy, T.; Noonan, M. The Paternal Experience of Fear of Childbirth: An Integrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1231. https://doi.org/10.3390/ijerph18031231
Moran E, Bradshaw C, Tuohy T, Noonan M. The Paternal Experience of Fear of Childbirth: An Integrative Review. International Journal of Environmental Research and Public Health. 2021; 18(3):1231. https://doi.org/10.3390/ijerph18031231
Chicago/Turabian StyleMoran, Emma, Carmel Bradshaw, Teresa Tuohy, and Maria Noonan. 2021. "The Paternal Experience of Fear of Childbirth: An Integrative Review" International Journal of Environmental Research and Public Health 18, no. 3: 1231. https://doi.org/10.3390/ijerph18031231
APA StyleMoran, E., Bradshaw, C., Tuohy, T., & Noonan, M. (2021). The Paternal Experience of Fear of Childbirth: An Integrative Review. International Journal of Environmental Research and Public Health, 18(3), 1231. https://doi.org/10.3390/ijerph18031231