3.3. Assessment of the Degree of Inequality in Community Care Resource Distribution
The geographical accessibility assessment could provide a fair distribution in a policy allocating community care resources [
16,
17,
18,
20,
22,
23,
24,
33,
35,
44,
45,
53]. This study proposed three analytical optimal solutions for the optimization of supply capacity allocation and applied measures of inequality to assess the geographical accessibility of community care resources. In
Table 5, geographical accessibility scores were calculated using four methods before optimization (method M0) and after optimization (methods M1–M3) to assess the degree of inequality present in the distribution of community care resources.
A comparison of the first six statistics listed in
Table 3 indicate that the scores generated by method M3 have the highest median and the lowest standard deviation and range. This indicates that if the resource allocation was carried out according to method M3 (after optimization), the distribution of geographic accessibility scores would have a more uniform trend than that obtained through method M0 (before optimization).
The last three inequality indicators listed in
Table 5 show that the three analytic solutions (methods M1–M3) are fairer than those before optimization (method M0). For example, the |Median−Mean| indicator is 0.365 before optimization (method M0), and after optimization, for method M1 it is 0.212, for method M2 it is 0.044, and for method M3 it is 0.050. In the indicator of the Gini coefficient, method M0 (before optimization) produced the highest value (0.670), and method M3 (after optimization) produced the lowest value (0.006). This indicates that if resource allocation before optimization is conducted according to method M0, the degree of inequality in the accessible rate of service point resources is the highest, while methods M1, M2, and M3 can improve equity in the accessibility of resources after the optimization of capacity allocation, among which M3 can reduce the degree of inequality to the greatest extent. The MSE value for method M0 was as high as 1.651, and in contrast, the value for method M3 was 0.015. This indicates that a resource allocation method that follows method M3 will minimize the accessibility disparities in community care resources available to populations at demand in different villages.
In
Table 6, the quintile method is used to compare geographical accessibility scores obtained through the four assessment methods, revealing improvements in resource allocation equity. Within the Q5 and Q95 class intervals, the dispersions of resource distribution disparity are presented. The distribution area for method M0 was the largest, and method M3 had the lowest disparity. For Q25, Q50, and Q75, method M3 rendered the same value of 0.617. This indicates that if resource allocation assessment is carried out according to method M3, over 75% of the population at demand will have consistent accessibility and achieve the maximum equity target.
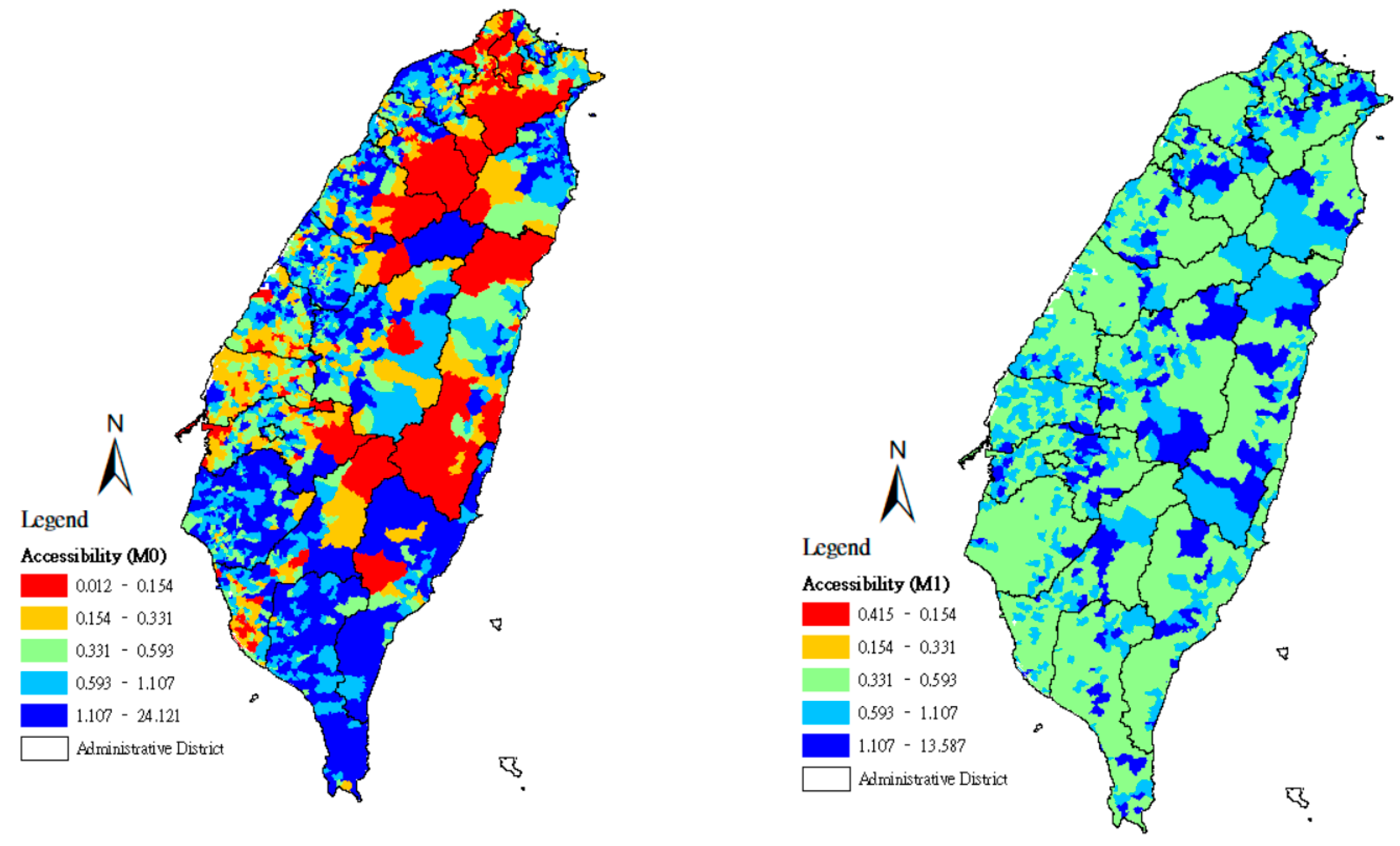
Using the quintile method, the geographical accessibility scores found in methods M0–M3 were divided according to a 20% class interval, and the spatial distributions of the accessibility scores of community care points were set using maps. From the lowest accessibility scores to the highest, the maps were marked with the colors red (0–20%), orange (21–40%), green (41–60%), light blue (61–80%), and deep blue (81–100%).
Figure 1 displays the map results for methods M0 and M1, where the lower-accessibility areas are scattered across eastern Taiwan and the mountainous zones of central Taiwan. The calculation of method M0 evaluates how the populations at demand in each county/city of Taiwan reach community care stations along the shortest routes, especially when the service points are distributed across metropolitan areas and districts with convenient transportation. In this case, the service point accessibility score of the population at demand in that county/city is higher.
Figure 1 also shows that in the assessment by method M0, the inequality in resource allocation between counties/cities is considerably high. Lower-accessibility areas are mainly scattered across the two northern municipalities (Taipei City and New Taipei City). In method M1, for each service point
j, the maximum value for distance is adopted as an approximate representation of the distances between
j and the locations at demand
i, which rely on its services, allowing the maximum value of resource optimization capacity
to be derived. Here,
Figure 1 exhibits the map result for method M1. That is, lower-accessibility areas disappear, and the most widely distributed areas are the moderate-accessibility areas, with high-accessibility areas only appearing in certain areas. Although the red and yellow areas determined by method M1 are significantly smaller than those of method M0, the three inequality indicators remain relatively large (
Table 5).
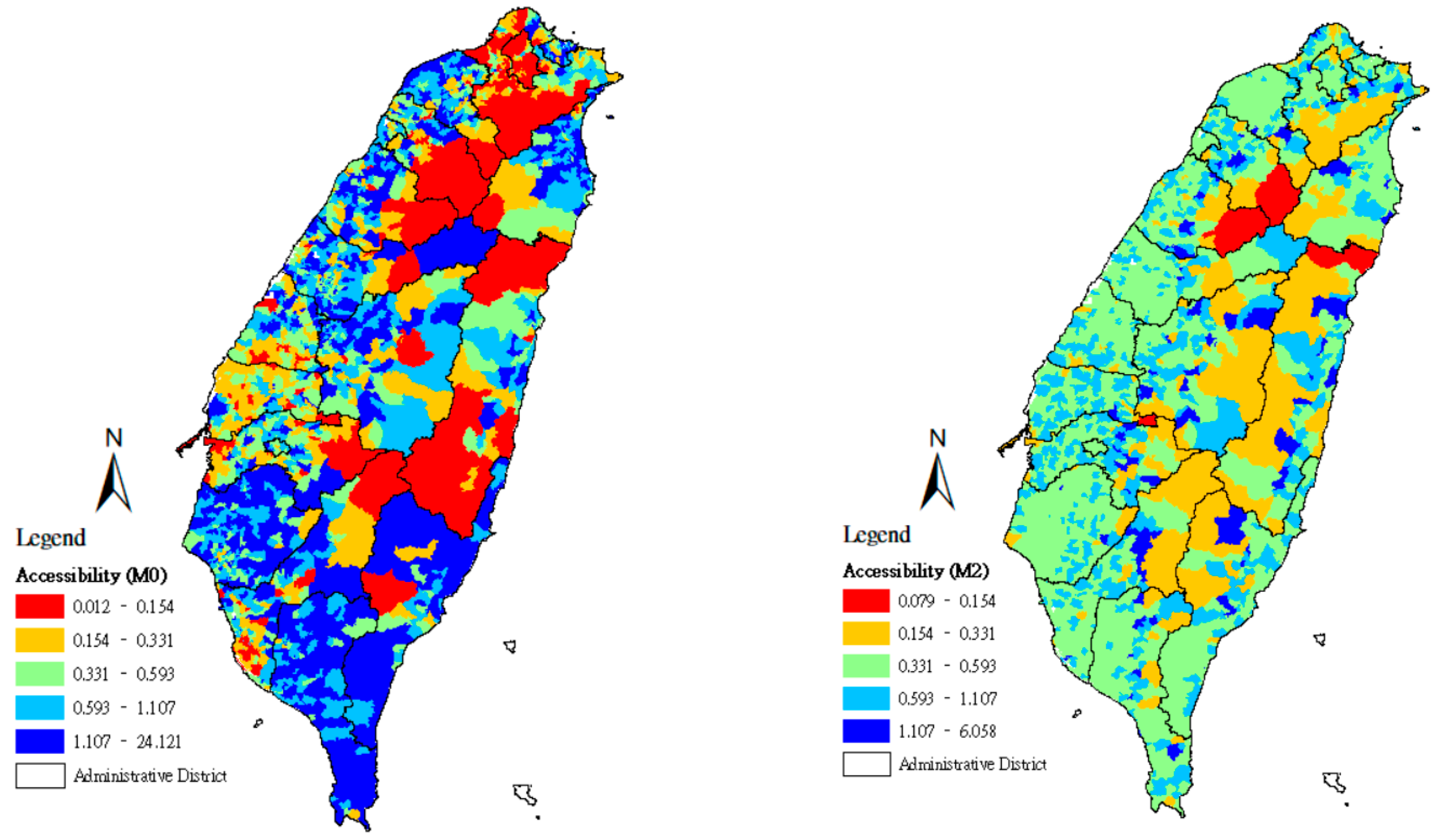
Figure 2 was mapped according to methods M0 and M2. For the results of method M2, the average value for distance is adopted as the approximate representation of the distances between
j and locations at demand
i that rely on its services, from which the average value of resource optimization capacity
can be derived. Accordingly,
Figure 2 exhibits the map results for method M2. Moderate-accessibility areas are widely distributed, and lower-accessibility and higher-accessibility areas are presented only in some areas. A comparison of
Figure 1 and
Figure 2 indicates that when the maximum value for resource optimization capacity is adopted, the accessibility scores tend to reach the maximum value; when the average value of resource optimization capacity is adopted in the estimation,
Figure 2 shows more moderate-accessibility areas than
Figure 1; at the same time, areas of lower accessibility increase, which represents the way that choice of distance produces a considerable effect on the equity of resource accessibility.
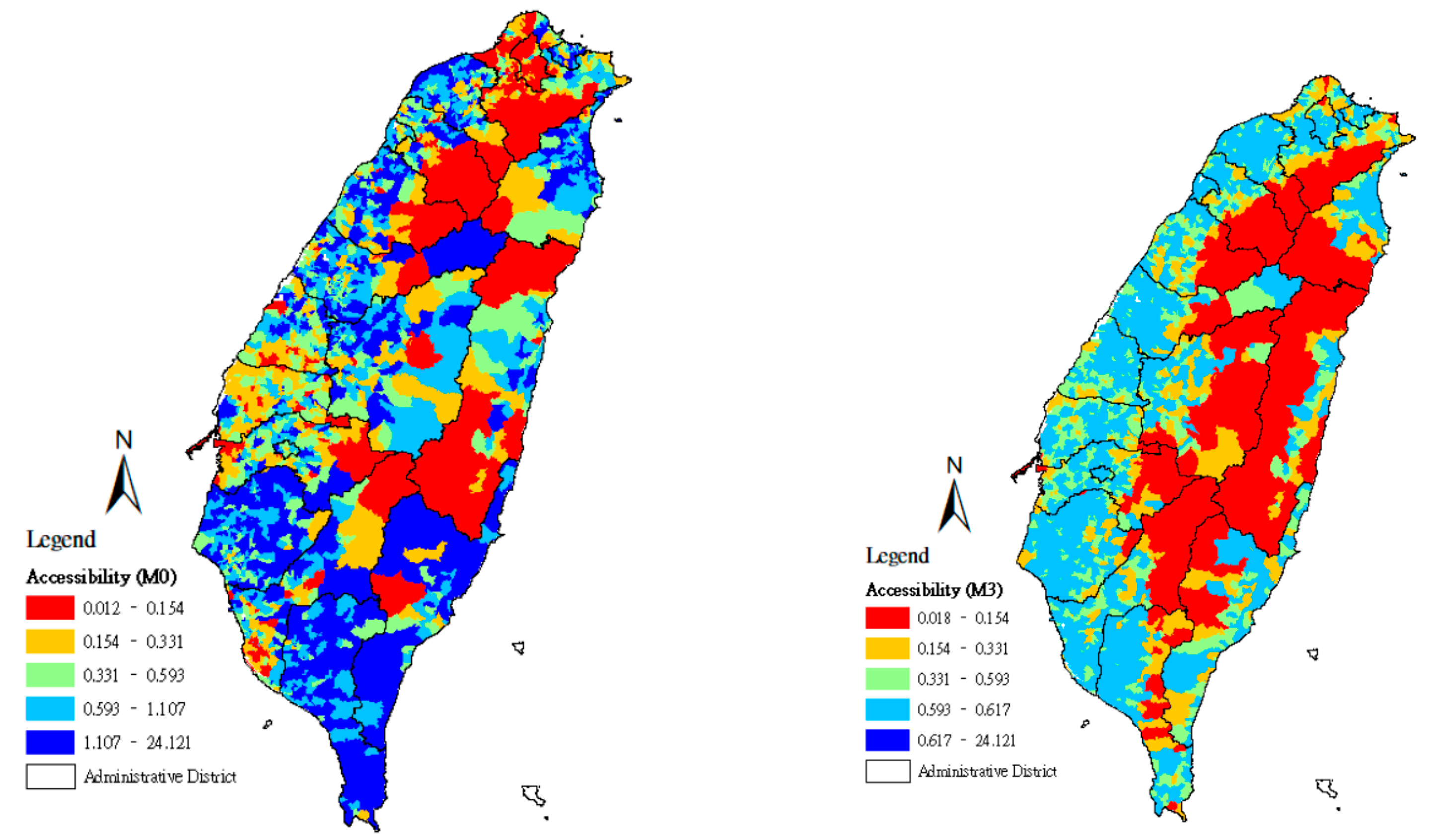
In
Figure 3, minimum-distance values are adopted as the approximate representation of the distances between
j and locations at demand
i that rely on its services, from which the minimum value for resource optimization capacity
can be derived. When the maximum equity for resource allocation is pursued with the minimum value for resource optimization capacity, due to population densities and the convenient transportation system in northern, western, and southern Taiwan, lower, moderate, and higher accessibility become scattered across a larger zone and reveal the possibility of maximum equity. In eastern Taiwan and the mountain zones, fewer community care stations appear, and all service points are located more than 3 km from villages with the population at demand. Thus, when the distance needed to reach a service point is represented by the location of the population at demand in a village through the shortest distance from the point, other locations of the population at demand at a distance value larger than the shortest distance are indicated as having lower accessibility.
Figure 3 also shows that the government should prioritize improving problems in eastern Taiwan and the mountain zones, which have insufficient service points allocated to them, to promote the welfare of the elderly population in counties/cities with lower accessibility.
Using the absolute values for geographical accessibility scores rendered with |Median−Mean|, MSE, and the Gini coefficient, the differences in the resource allocation optimization models evaluated by the four methods are compared in
Table 5 to indicate the degree of improvement in the maximum equity of community care accessibility in counties/cities. When |Median−Mean| is larger than the average value for |Median − Mean| for the whole island, the resource allocation of the county/city is uneven and therefore needs improvement. In method M0, four counties/cities had |Median−Mean| values larger than the average value for median value minus mean value over the entire island. The optimization models for methods M2 and M3 decreased |Median−Mean|. That is to say, the distributions of geographical accessibility in all counties/cities can be redistributed more even using the community-care capacity allocation optimization models M2 and M3.
Table 7 demonstrates that the MSE values for four counties/cities are greater than those for the average of the entire island by method M0, that is, these counties/cities’ accessibility scores are farther away from the fair target value (Ae). Moreover, the MSE values of the five counties/cities have increased in method M1, while methods M2 and M3 bring the accessibility distribution closer to the fair target value in all counties/cities after supply capacity is optimized.
The Gini coefficient was employed to compare the degree of improvement rendered by methods M0–M3 in resource allocation inequity among counties/cities. In all 19 counties/cities,
Table 7 shows that M1–M3 make the Gini coefficient smaller due to the optimization of the supply capacity, indicating that geographical accessibility can become more equal. In the assessment of method M0, two counties/cities are found to have high inequity, and 17 counties/cities have median inequality. In methods M2 and M3, no counties/cities have inequitable distribution. In method M3, the value rendered from the Gini coefficient was the lowest among all optimization models, showing that method M3 is the best way to achieve maximum equity in resource allocation.







{kind=link}
{kind=link}
{kind=link}