
Seated Virtual Reality-Guided Exercise Improved Gait in a Postoperative Hallux Valgus Case

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant
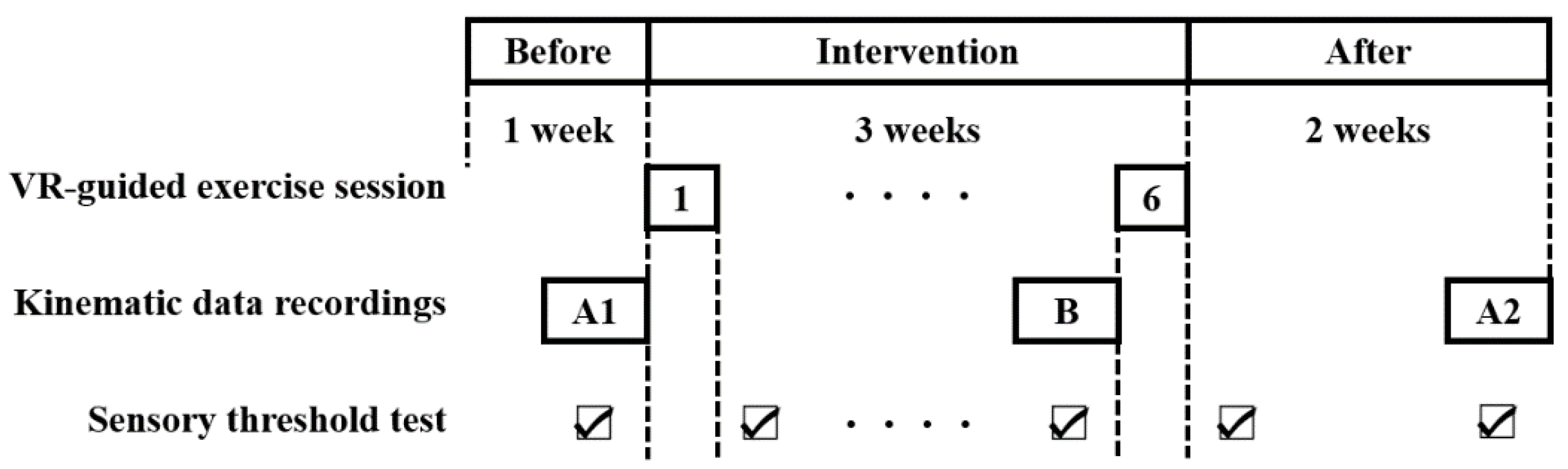
2.2. Experimental Design
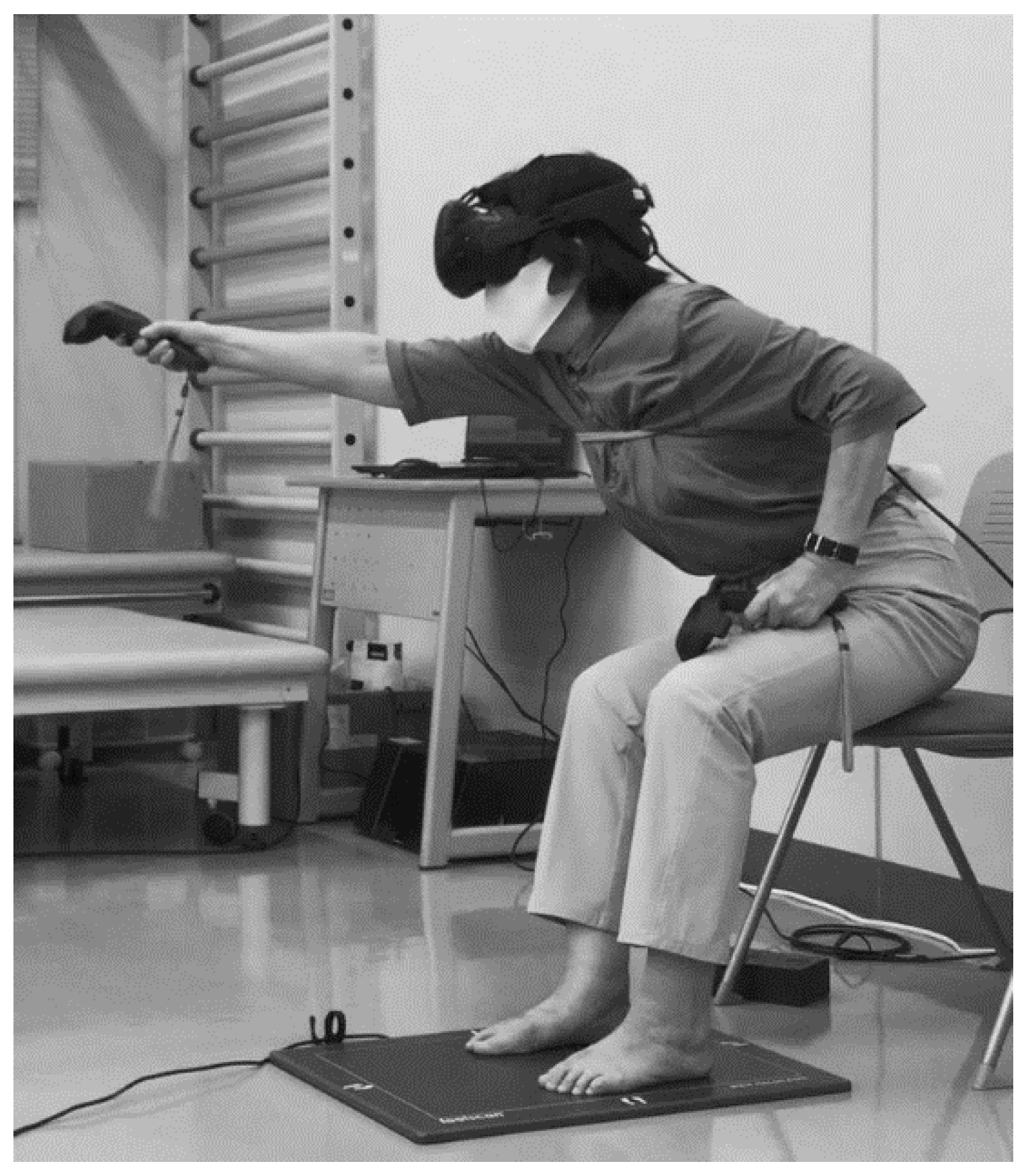
2.3. Intervention
2.4. Measurements
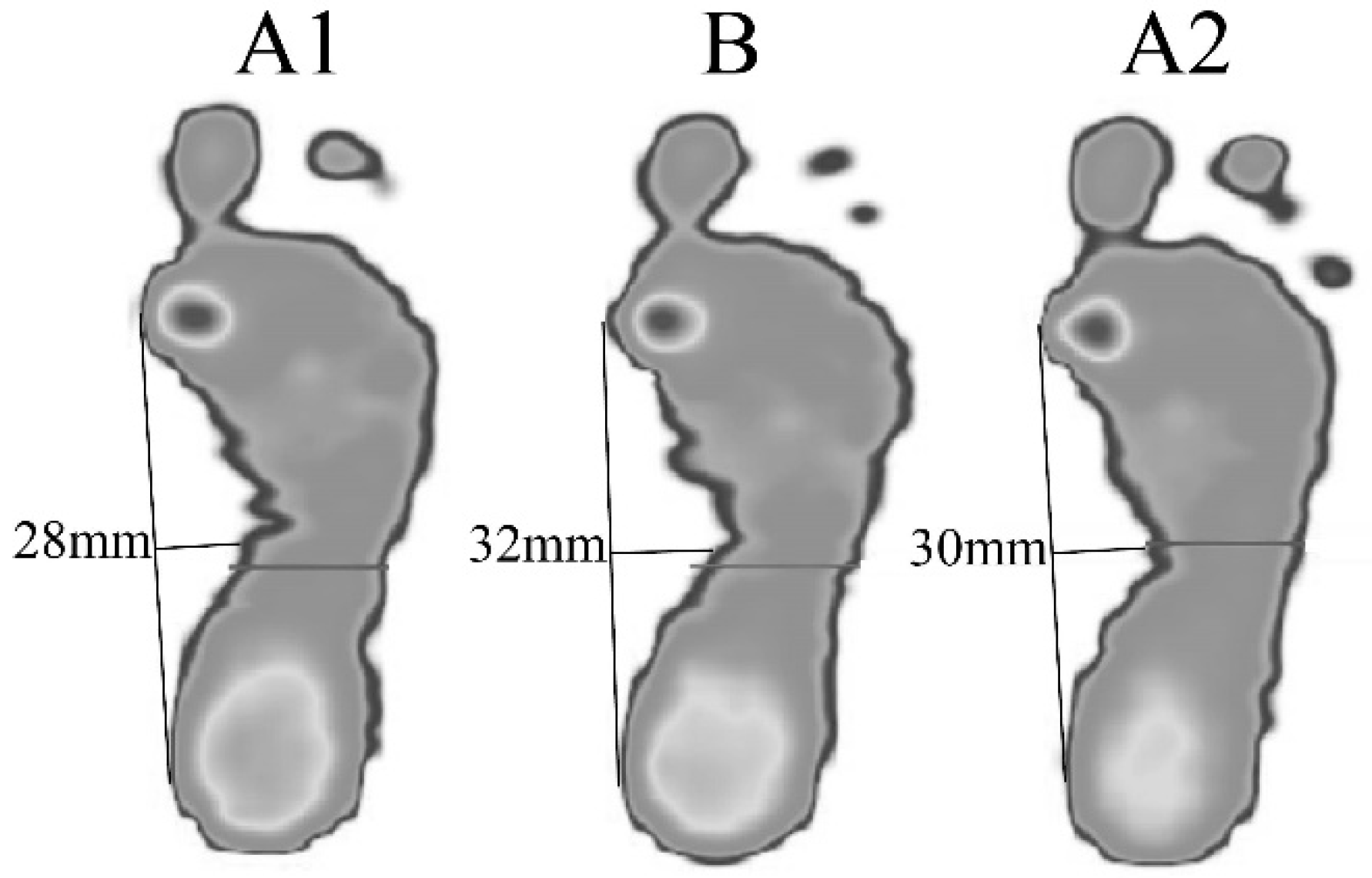
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- O’Leary, C.B.; Cahill, C.R.; Robinson, A.W.; Barnes, M.J.; Hong, J. A Systematic Review: The Effects of Podiatrical Deviations on Nonspecific Chronic Low Back Pain. J. Back Musculoskelet. Rehabil. 2013, 26, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Koken, M.; Guclu, B. The Effect of Hallux Valgus Surgery on Quality of Life. J. Am. Podiatr. Med. Assoc. 2020, 110, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hecht, P.J.; Lin, T.J. Hallux Valgus. Med. Clin. N. Am. 2014, 98, 227–232. [Google Scholar] [CrossRef]
- Ford, L.A.; Hamilton, G.A. Procedure Selection for Hallux Valgus. Clin. Podiatr. Med. Surg. 2009, 26, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Kadakia, A.R. Salvage of Recurrence After Failed Surgical Treatment of Hallux Valgus. Arch. Orthop. Trauma. Surg. 2012, 132, 477–485. [Google Scholar] [CrossRef]
- Hawson, S.T. Physical Therapy Post-Hallux Abducto Valgus Correction. Clin. Podiatr. Med. Surg. 2014, 31, 309–322. [Google Scholar] [CrossRef]
- Omon, K.; Hara, M.; Ishikawa, H. Virtual Reality-Guided, Dual-Task, Body Trunk Balance Training in the Sitting Position Improved Walking Ability Without Improving Leg Strength. Prog. Rehabil. Med. 2019, 4, 20190011. [Google Scholar] [CrossRef] [PubMed]
- Takimoto, K.; Omon, K.; Murakawa, Y.; Ishikawa, H. Case of Cerebellar Ataxia Successfully Treated by Virtual Reality-Guided Rehabilitation. BMJ Case Rep. 2021, 14, e242287. [Google Scholar] [CrossRef]
- Morikawa, T.; Katoh, H. Spinal Kyphotic Alignment Changes Spinal Movement Strategy During Lateral Reaching Motion While in a Sitting Position. J. Phys. Ther. Sci. 2020, 32, 48–51. [Google Scholar] [CrossRef]
- Kim, C.Y.; Lee, J.S.; Lee, J.H.; Kim, Y.G.; Shin, A.R.; Shim, Y.H.; Ha, H.K. Effect of Spatial Target Reaching Training Based on Visual Biofeedback on the Upper Extremity Function of Hemiplegic Stroke Patients. J. Phys. Ther. Sci. 2015, 27, 1091–1096. [Google Scholar] [CrossRef]
- Leung, A.K.; Cheng, J.C.; Zhang, M.; Fan, Y.; Dong, X. Contact Force Ratio: A New Parameter to Assess Foot Arch Function. Prosthet. Orthot. Int. 2004, 28, 167–174. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Nelson, M.E.; Kaliton, D.; Layne, J.E.; Bernstein, M.J.; Nuernberger, A.; Singh, M.A. Etiology and Modification of Gait Instability in Older Adults: A Randomized Controlled Trial of Exercise. J. Appl. Physiol. 2001, 90, 2117–2129. [Google Scholar] [CrossRef] [PubMed]
- Bell-Krotoski, J. Advances in Sensibility Evaluation. Hand Clin. 1991, 7, 527–546. [Google Scholar] [CrossRef]
- Galica, A.M.; Hagedorn, T.J.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Casey, V.A.; Hannan, M.T. Hallux Valgus and Plantar Pressure Loading: The Framingham Foot Study. J. Foot Ankle Res. 2013, 6, 42. [Google Scholar] [CrossRef]
- Herron, M.L.; Kar, S.; Beard, D.; Binfield, P. Sensory Dysfunction in the Great Toe in Hallux Valgus. J. Bone Jt. Surg. Br. 2004, 86, 54–57. [Google Scholar] [CrossRef][Green Version]
- Kimoto, Y.; Hasegawa, M.; Kanai, S. Relationship Between the Sense of Touch and Plantar Pressure for the Entire Sole of the Foot. J. Phys. Ther. Pract. Res. 2011, 20, 85–89. (In Japanese) [Google Scholar]
- Kimura, K.; Endo, Y. Age-Related Changes in the Tactile Pressure Sensitivity Threshold in the Sole of the Foot in Diabetic Patients. J. Phys. Ther. Sci. 2018, 30, 917–920. [Google Scholar] [CrossRef][Green Version]
- Perry, J.; Burnfield, J. Gait Analysis: Normal and Pathological Function, 2nd ed.; Slack Inc.: Philadelphia, PA, USA, 2010; pp. 121–127. [Google Scholar]
- Thorstensson, A.; Nilsson, J.; Carlson, H.; Zomlefer, M.R. Trunk Movements in Human Locomotion. Acta. Physiol. Scand. 1984, 121, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Waters, R.L.; Morris, J.; Perry, J. Translational Motion of the Head and Trunk During Normal Walking. J. Biomech. 1973, 6, 167–172. [Google Scholar] [CrossRef]
- Gard, S.A.; Knox, E.H.; Childress, D.S. Two-Dimensional Representation of Three-Dimensional Pelvic Motion During Human Walking: An Example of How Projections Can Be Misleading. J. Biomech. 1996, 29, 1387–1391. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Edelberg, H.K.; Mitchell, S.L.; Goldberger, A.L.; Wei, J.Y. Increased Gait Unsteadiness in Community-dwelling Elderly Fallers. Arch. Phys. Med. Rehabil. 1997, 78, 278–283. [Google Scholar] [CrossRef]
- Doi, T.; Makizako, H.; Tsutsumimoto, K. Gait Variables from Trunk Acceleration and Fall Among Community-Dwelling Older Adults. J. Jpn. Phys. Ther. Assoc. 2016, 43, 75–81. (In Japanese) [Google Scholar]
- Park, C.H.; Chang, M.C. Forefoot disorders and conservative treatment. Yeungnam Univ. J. Med. 2019, 36, 92–98. [Google Scholar] [CrossRef]
- Santamaria, V.; Rachwani, J.; Manselle, W.; Saavedra, S.L.; Woollacott, M. The Impact of Segmental Trunk Support on Posture and Reaching While Sitting in Healthy Adults. J. Mot. Behav. 2018, 50, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Ying, J.; Xu, Y.; István, B.; Ren, F. Adjusted Indirect and Mixed Comparisons of Conservative Treatments for Hallux Valgus: A Systematic Review and Network Meta-Analysis. Int. J. Environ. Res. Public. Health. 2021, 18, 3841. [Google Scholar] [CrossRef] [PubMed]
- Budiman-Mak, E.; Conrad, K.J.; Roach, K.E.; Moore, J.W.; Lertratanakul, Y.; Koch, A.E.; Skosey, J.L.; Froelich, C.; Joyce-Clark, N. Can Foot Orthoses Prevent Hallux Valgus Deformity in Rheumatoid Arthritis? A Randomized Clinical Trial. J. Clin. Rheumatol. 1995, 1, 313–322. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kinematic Parameter | A1 | B | A2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Plantar pressure | ||||||||||||
| Maximum force | ||||||||||||
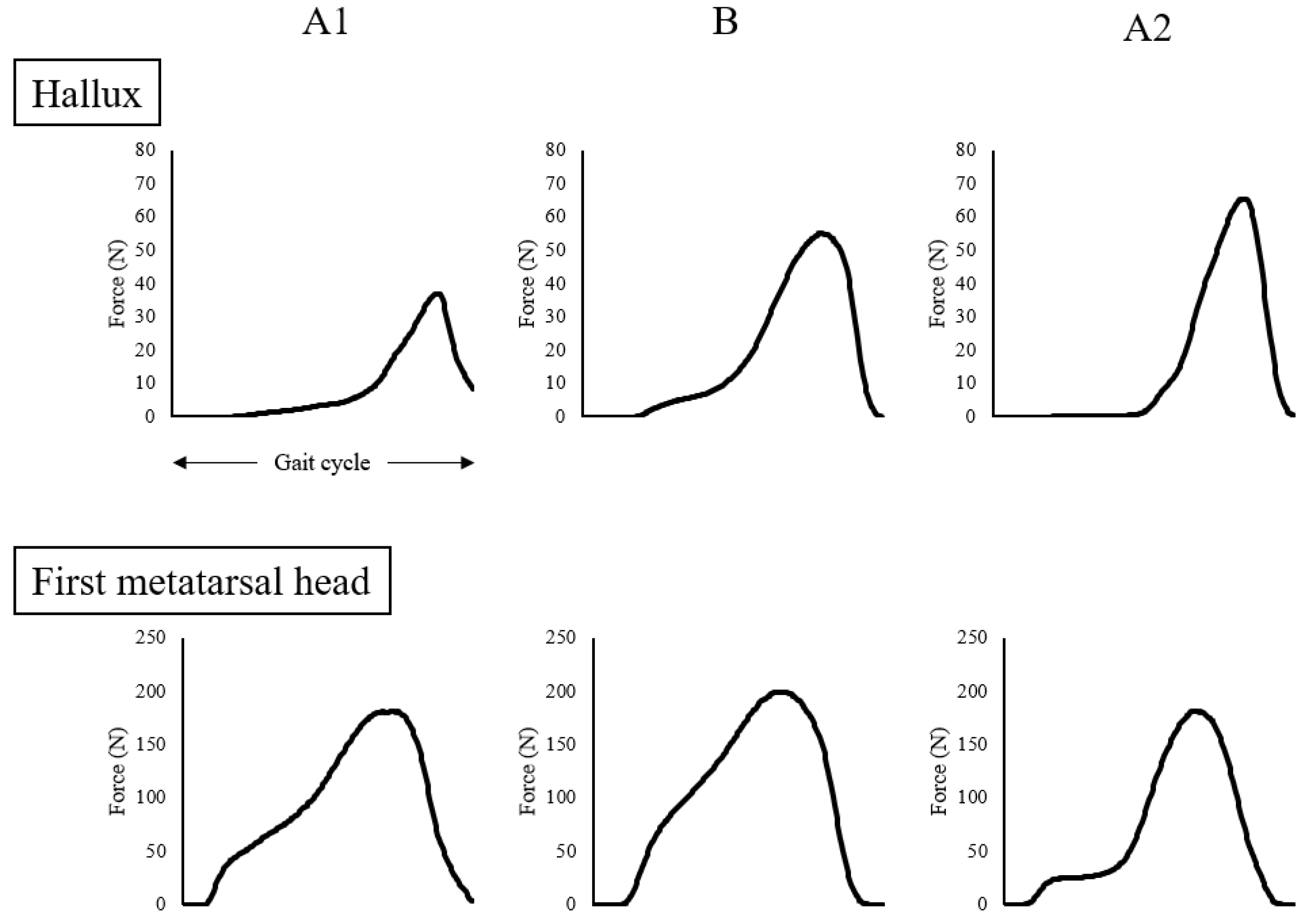
| Hallux | N | 39.6 | ± | 3.3 | 57.7 | ± | 20.1 | 68.3 | ± | 25.7 | ||
| First metatarsal | N | 183.2 | ± | 42.5 | 202.0 | ± | 21.5 | 183.6 | ± | 17.2 | ||
| Impulse | ||||||||||||
| Hallux | N·s | 7.5 | ± | 1.3 | 14.6 | ± | 6.9 | 12.7 | ± | 5.3 | ||
| First metatarsal | N·s | 74.6 | ± | 32.3 | 77.8 | ± | 10.1 | 54.4 | ± | 4.3 | ||
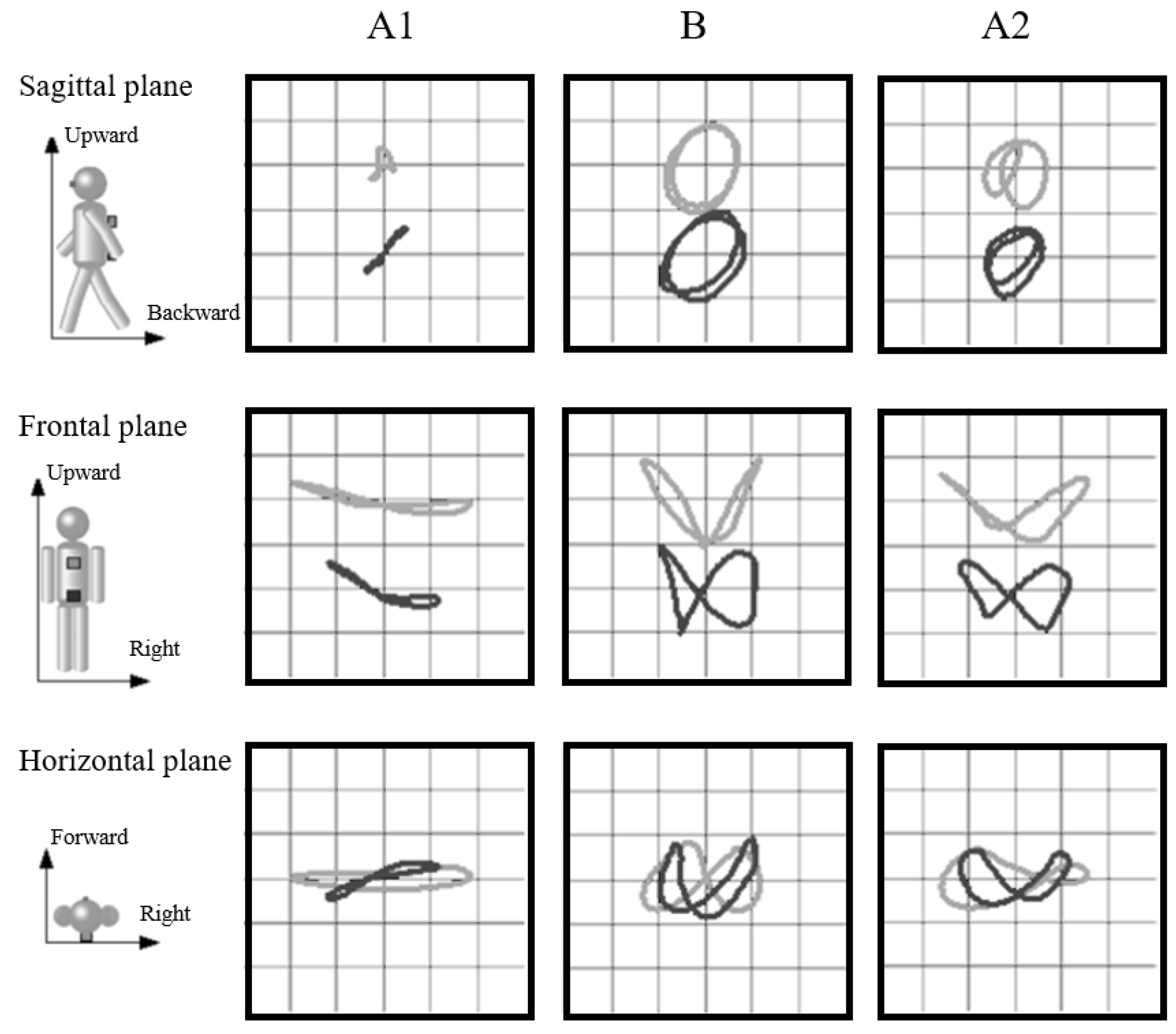
| Amplitudes of the thoracic and pelvic displacement | ||||||||||||
| Seventh thoracic vertebra | ||||||||||||
| Vertical | mm | 14 | 40 | 30 | ||||||||
| Lateral | mm | 76 | 50 | 63 | ||||||||
| Progressional | mm | 10 | 31 | 26 | ||||||||
| First sacral vertebra | ||||||||||||
| Vertical | mm | 20 | 40 | 31 | ||||||||
| Lateral | mm | 47 | 41 | 47 | ||||||||
| Progressional | mm | 17 | 35 | 24 | ||||||||
| Stride-to-stride time variability | % | 15.5 | 3.8 | 3.2 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamoto, M.; Kakuda, A.; Miyashita, T.; Kitagawa, T.; Kitano, M.; Hara, M.; Kudo, S. Seated Virtual Reality-Guided Exercise Improved Gait in a Postoperative Hallux Valgus Case. Int. J. Environ. Res. Public Health 2021, 18, 13267. https://doi.org/10.3390/ijerph182413267
Nakamoto M, Kakuda A, Miyashita T, Kitagawa T, Kitano M, Hara M, Kudo S. Seated Virtual Reality-Guided Exercise Improved Gait in a Postoperative Hallux Valgus Case. International Journal of Environmental Research and Public Health. 2021; 18(24):13267. https://doi.org/10.3390/ijerph182413267
Chicago/Turabian StyleNakamoto, Masami, Akihiro Kakuda, Toshinori Miyashita, Takashi Kitagawa, Masashi Kitano, Masahiko Hara, and Shintarou Kudo. 2021. "Seated Virtual Reality-Guided Exercise Improved Gait in a Postoperative Hallux Valgus Case" International Journal of Environmental Research and Public Health 18, no. 24: 13267. https://doi.org/10.3390/ijerph182413267
APA StyleNakamoto, M., Kakuda, A., Miyashita, T., Kitagawa, T., Kitano, M., Hara, M., & Kudo, S. (2021). Seated Virtual Reality-Guided Exercise Improved Gait in a Postoperative Hallux Valgus Case. International Journal of Environmental Research and Public Health, 18(24), 13267. https://doi.org/10.3390/ijerph182413267