
Automated Classification of Normal Control and Early-Stage Dementia Based on Activities of Daily Living (ADL) Data Acquired from Smart Home Environment

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Method
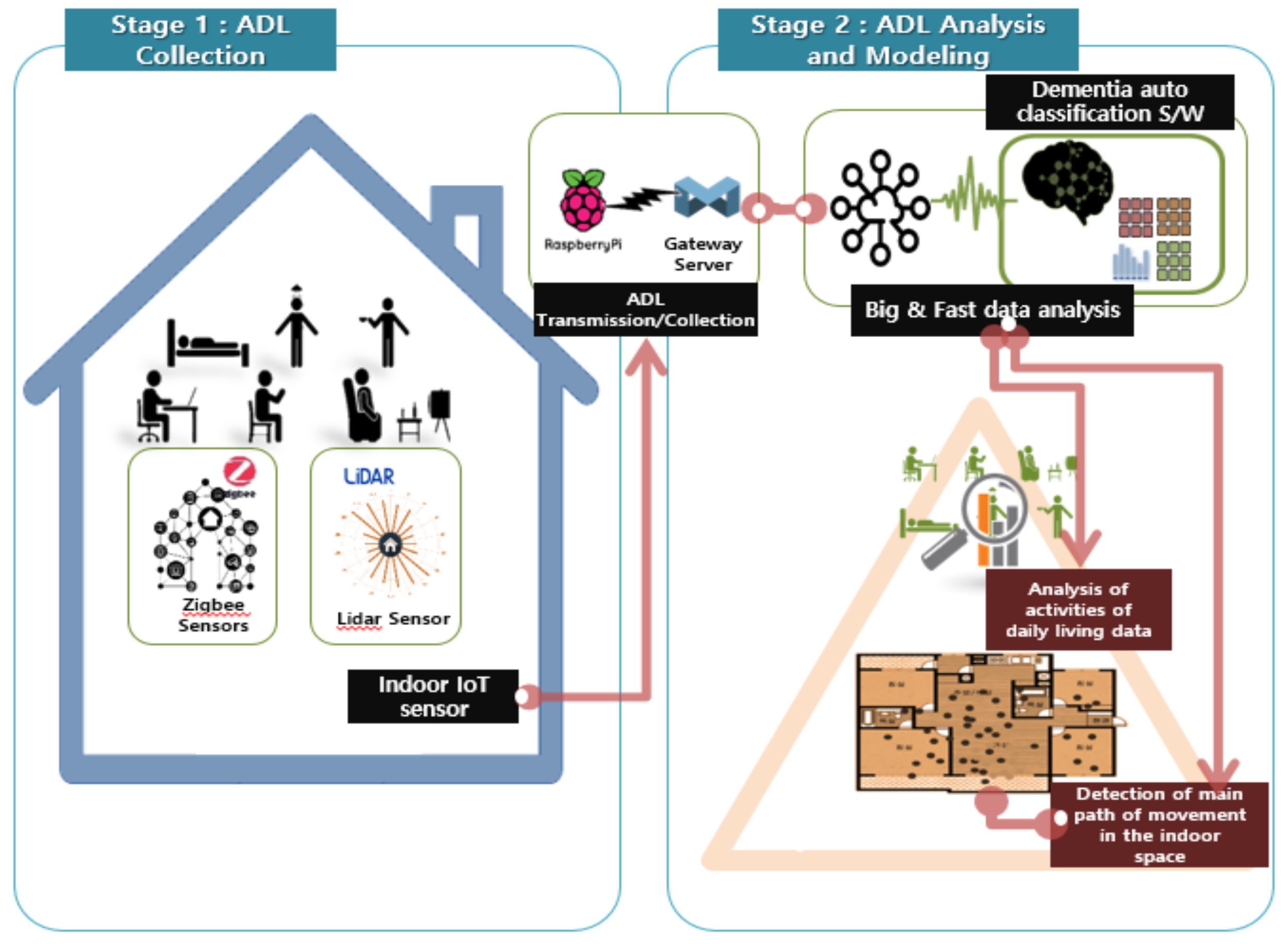
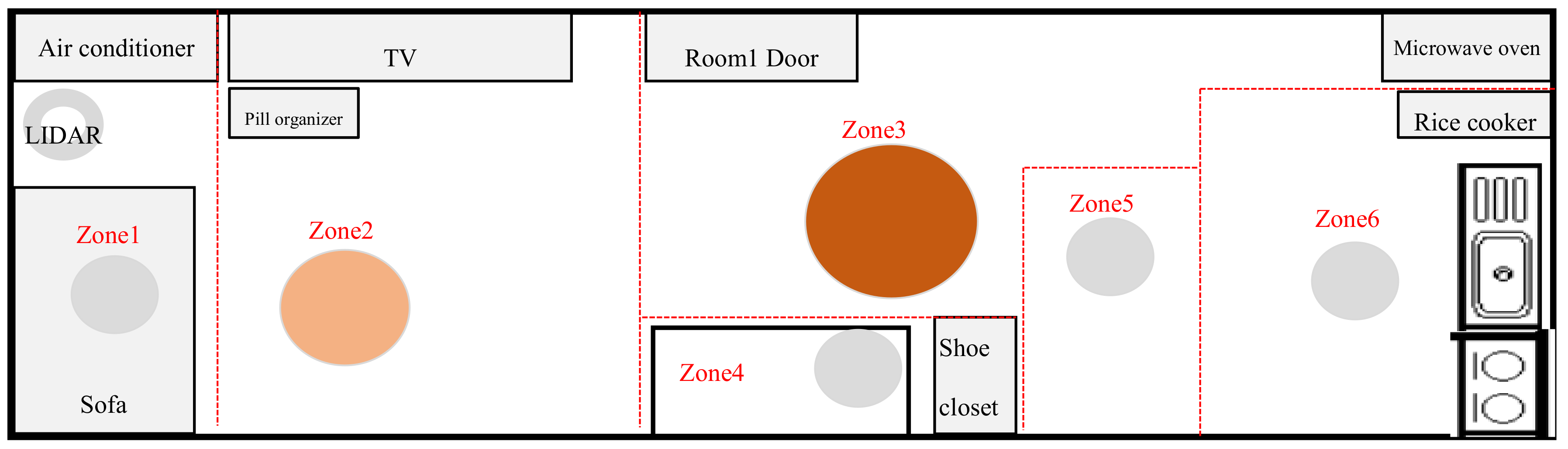
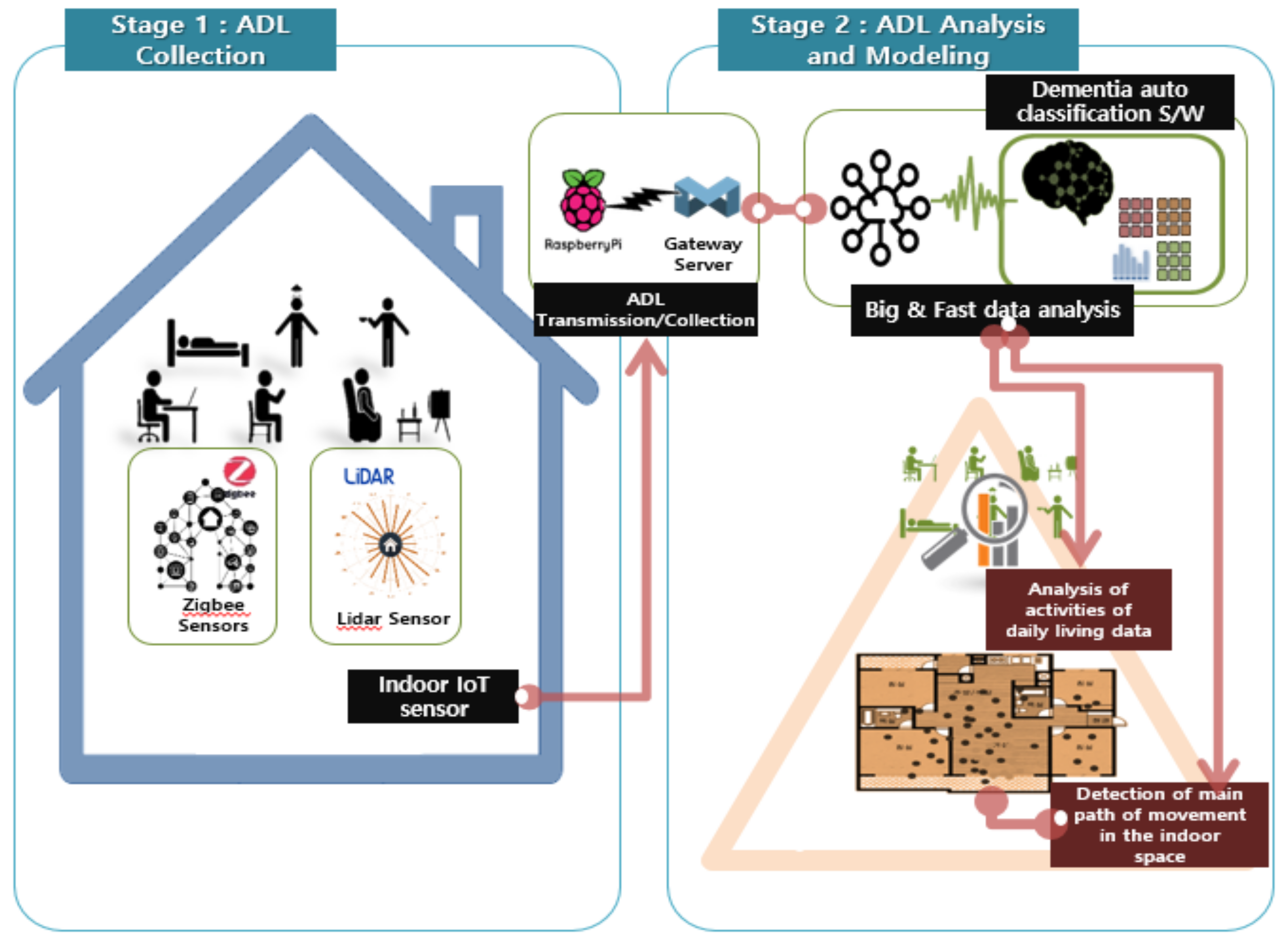
2.1. Smart-Home-Based Activities of Daily Living
2.2. Feature Selection
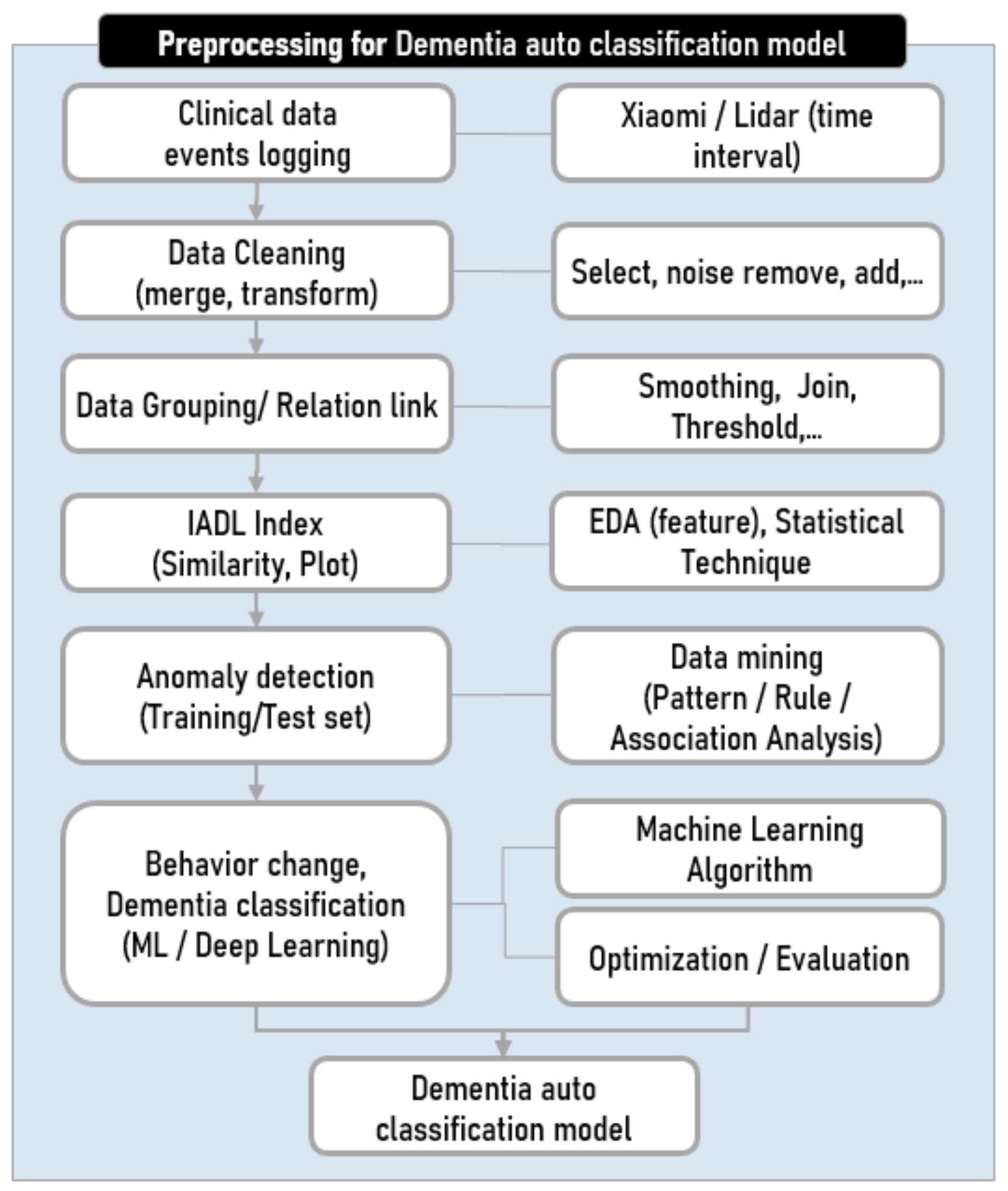
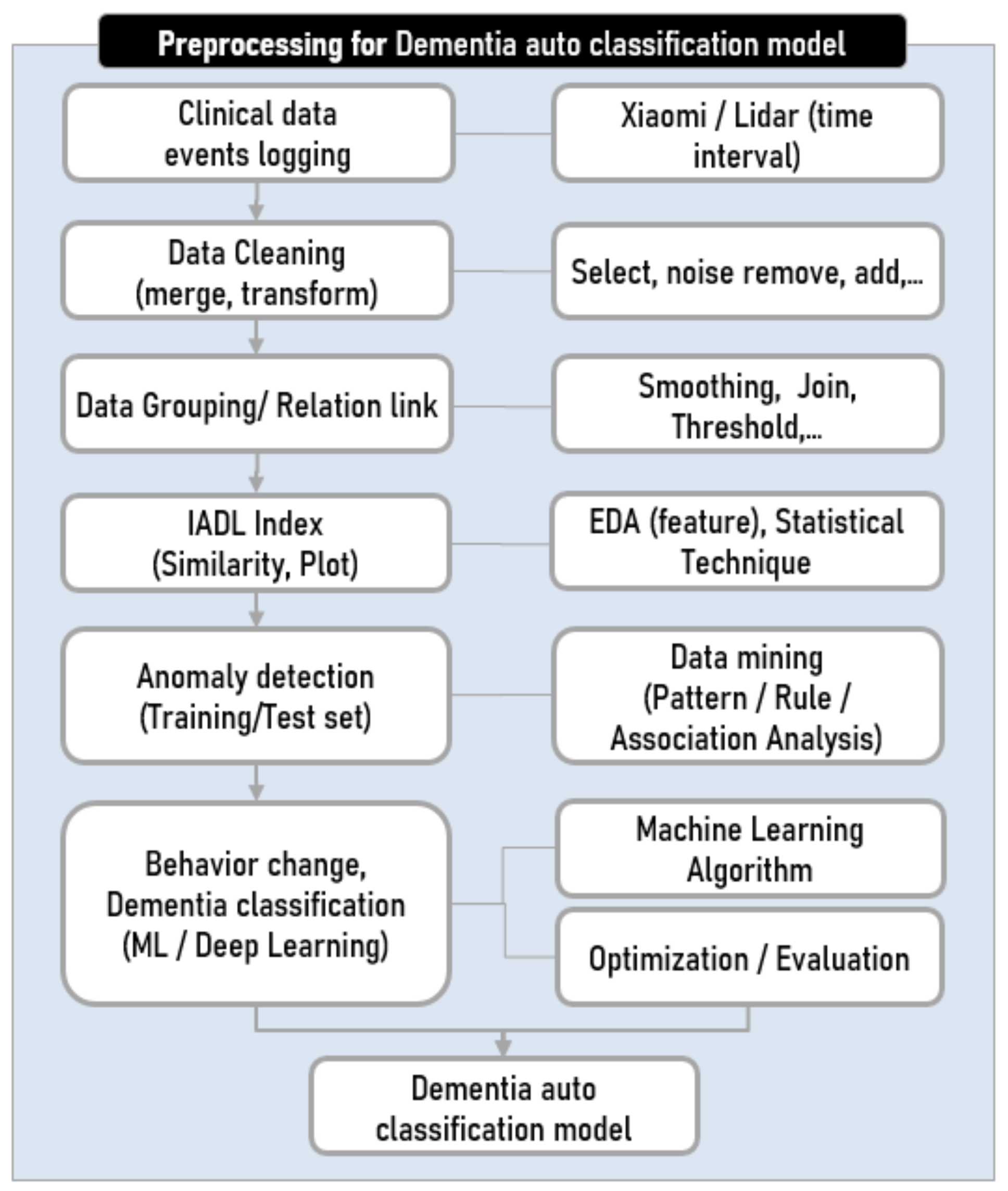
2.2.1. Basic Data Preprocessing
2.2.2. Personalization
2.2.3. Feature Generation
2.3. Classification between the Normal Controls and Those with Early-Stage Dementia
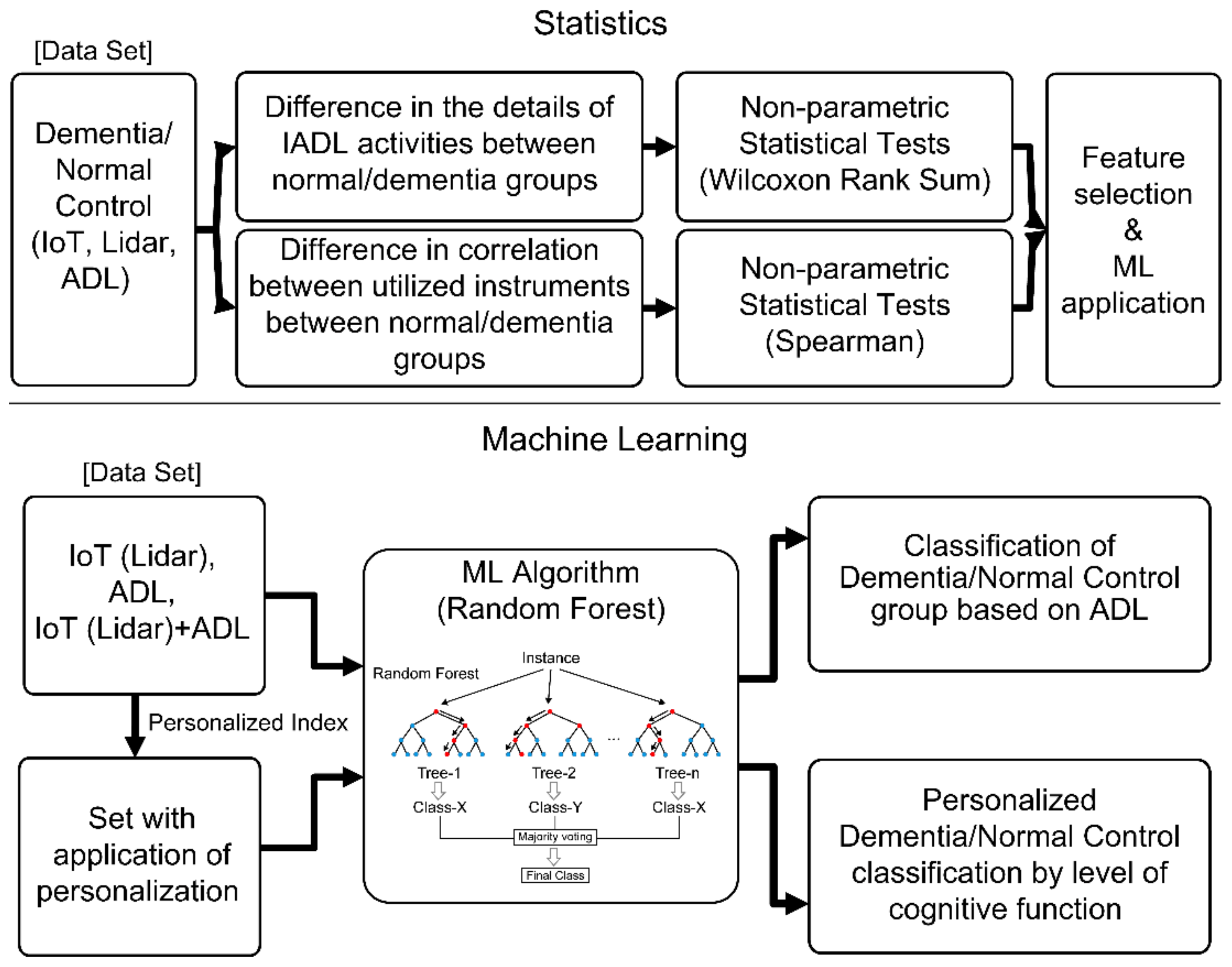
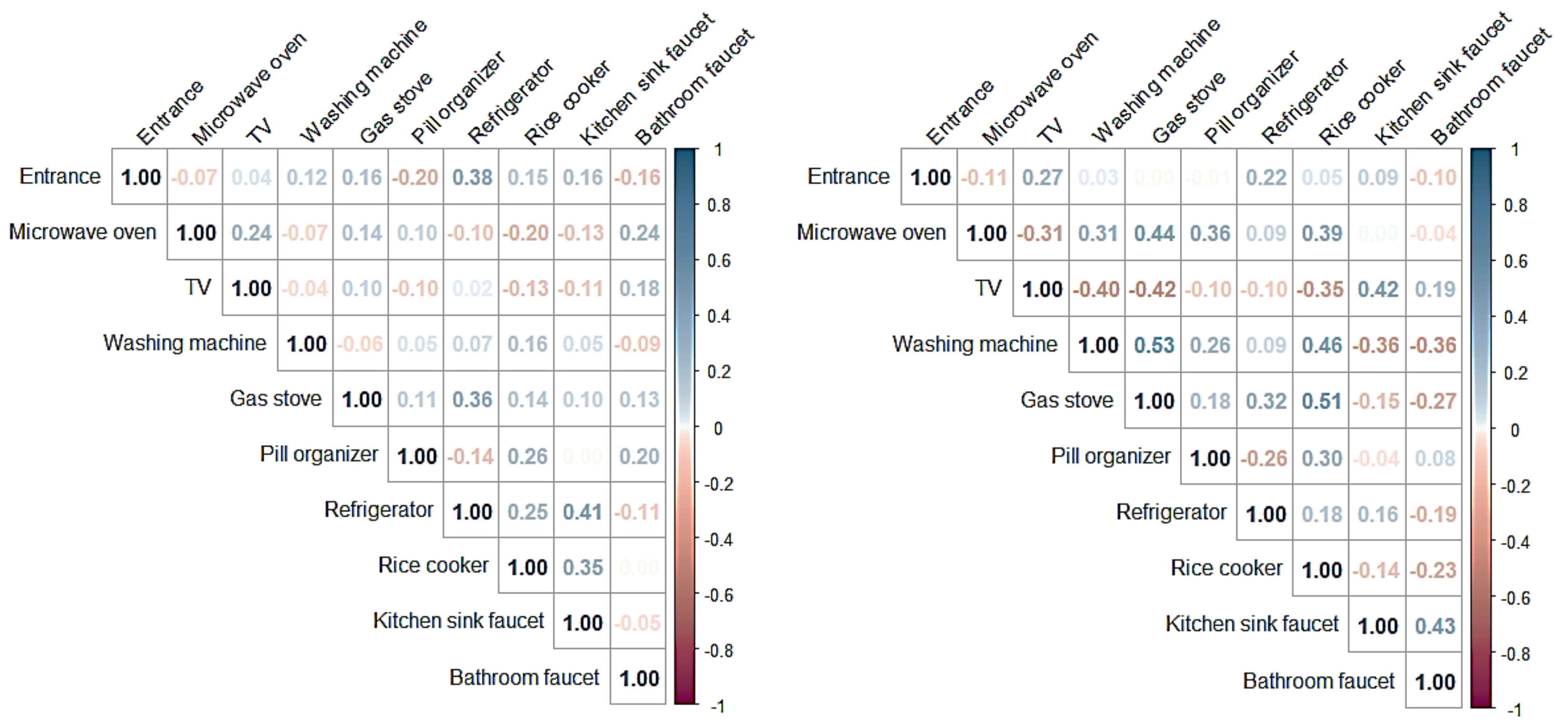
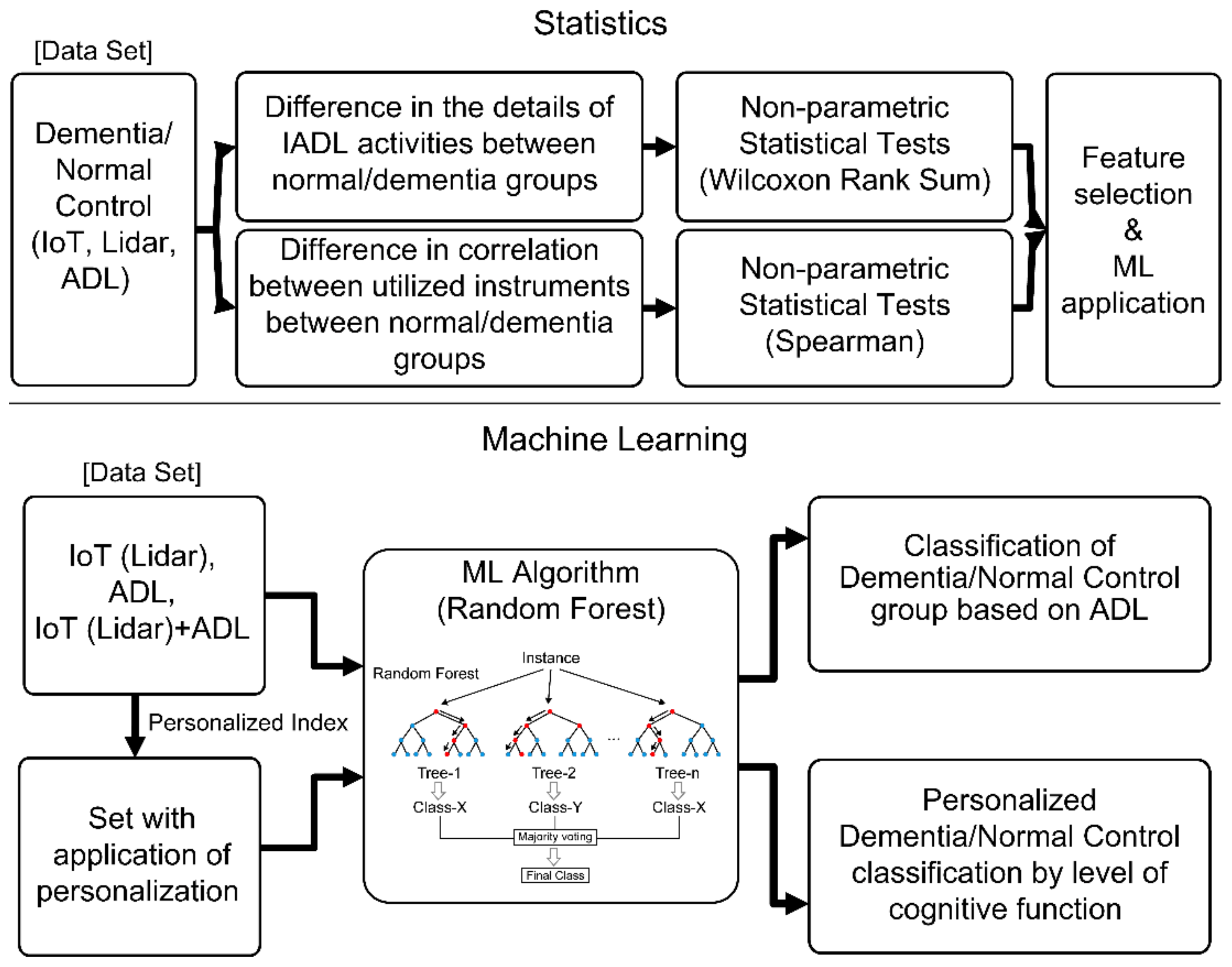
2.3.1. Statistical Method-Based Classification
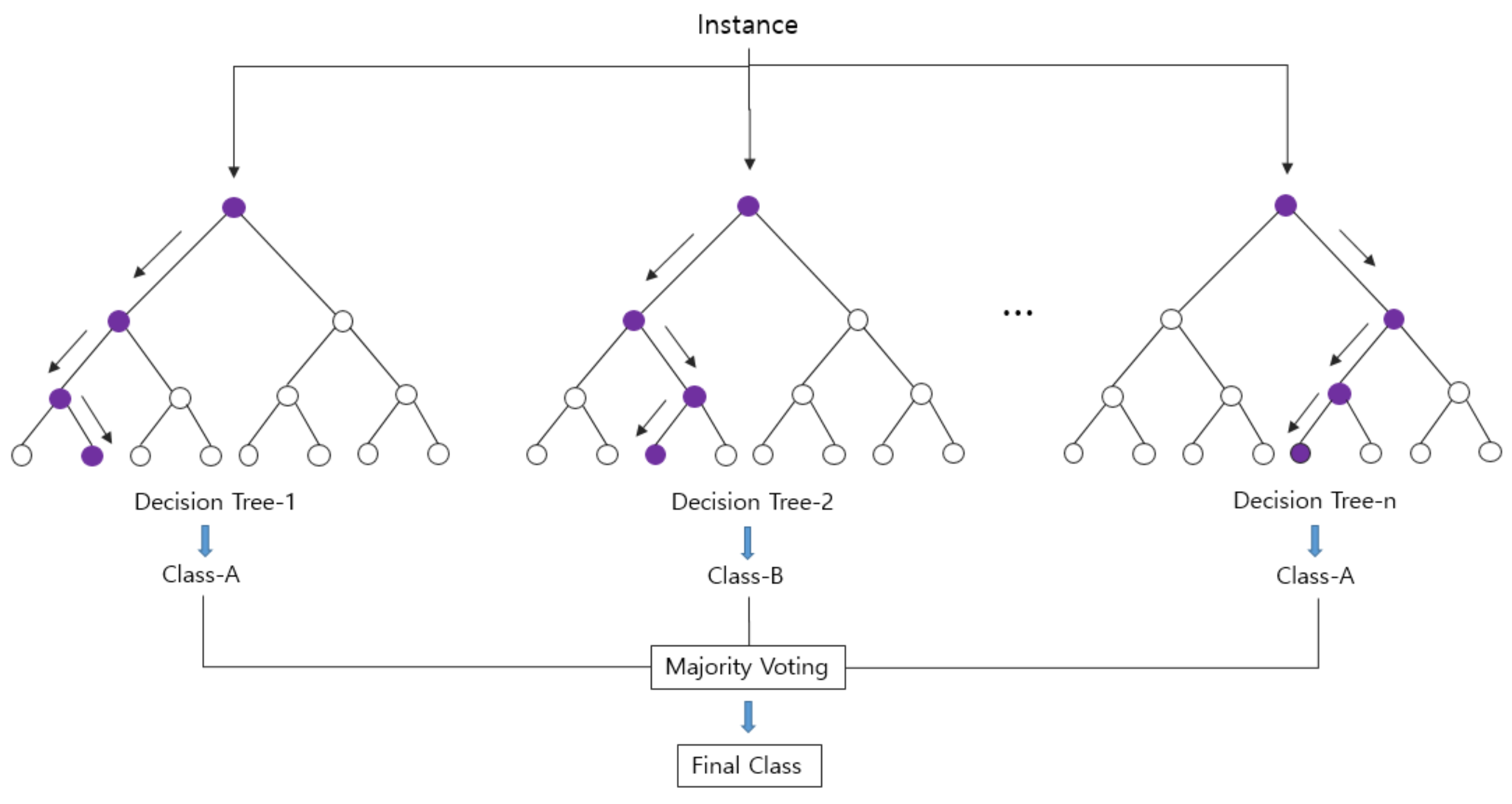
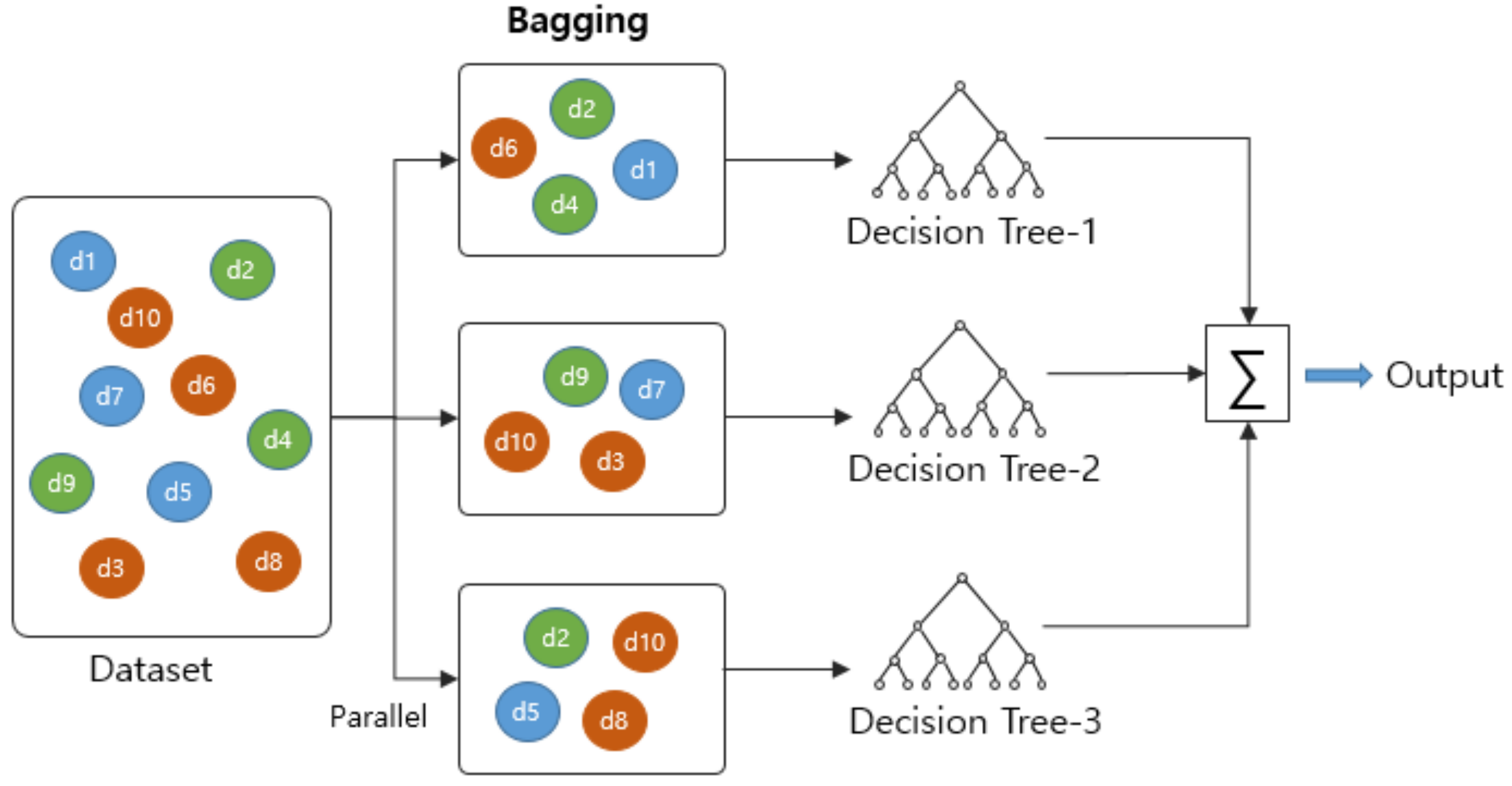
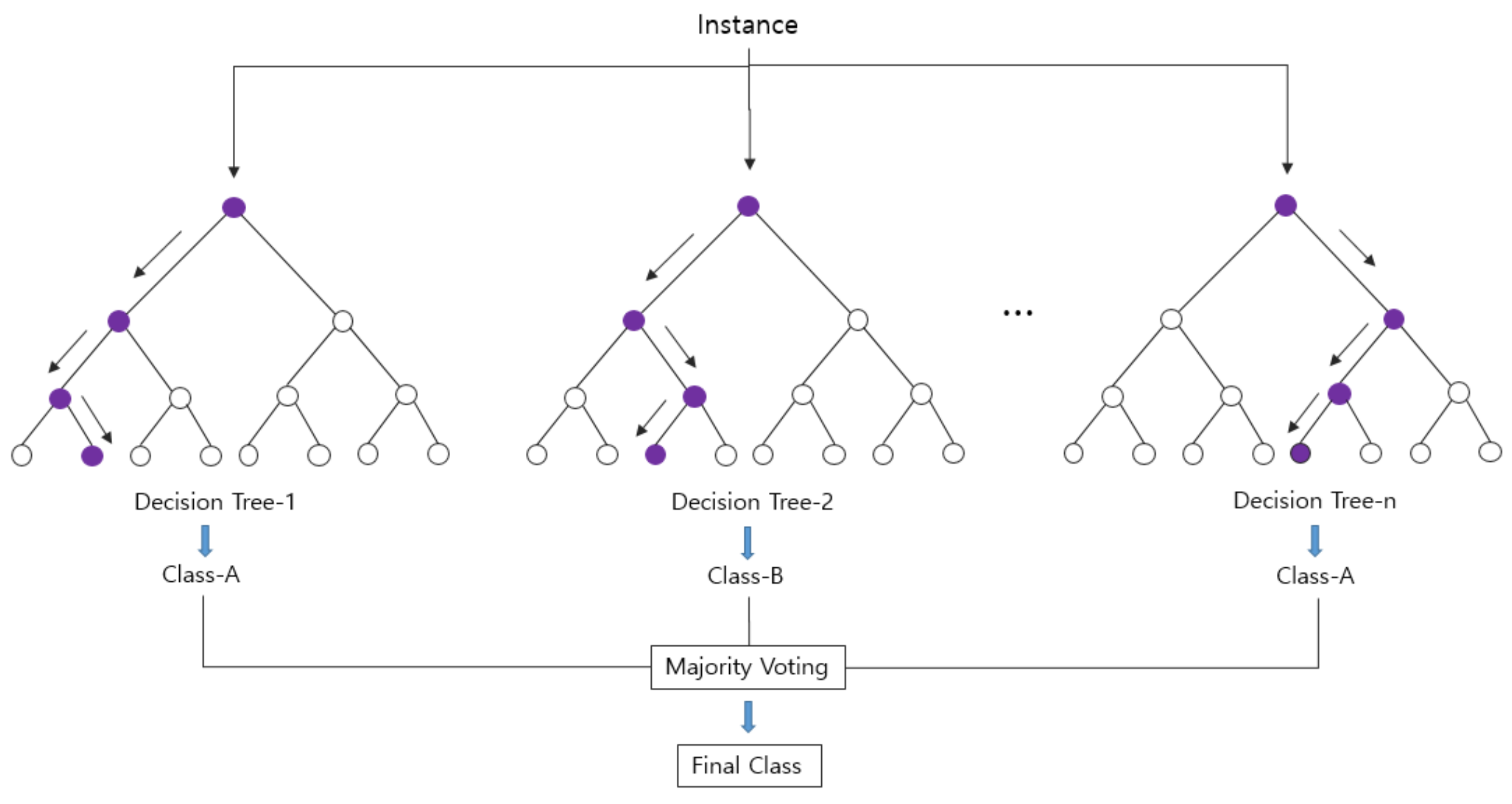
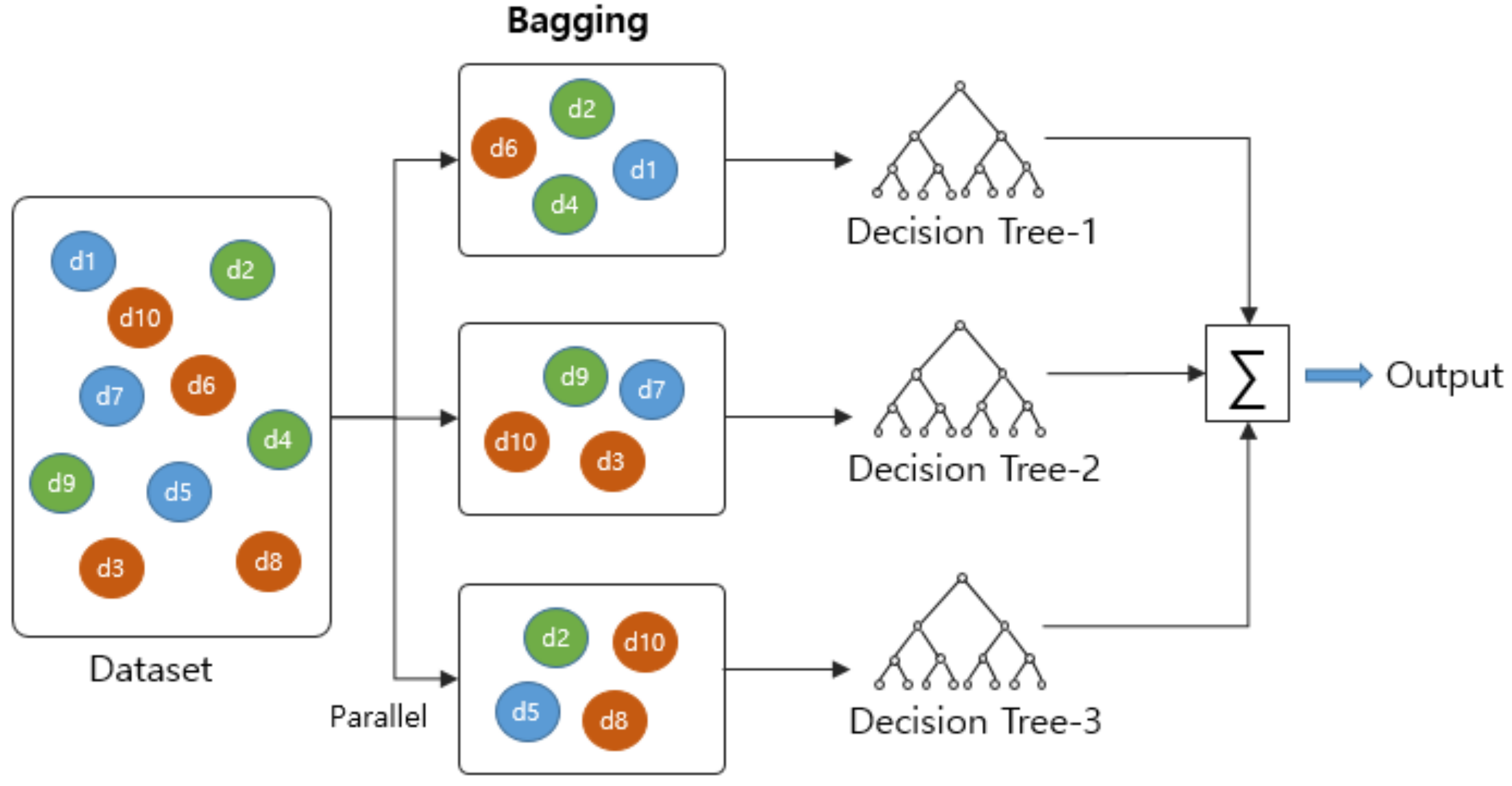
2.3.2. Machine-Learning-Based Classification
3. Experiments
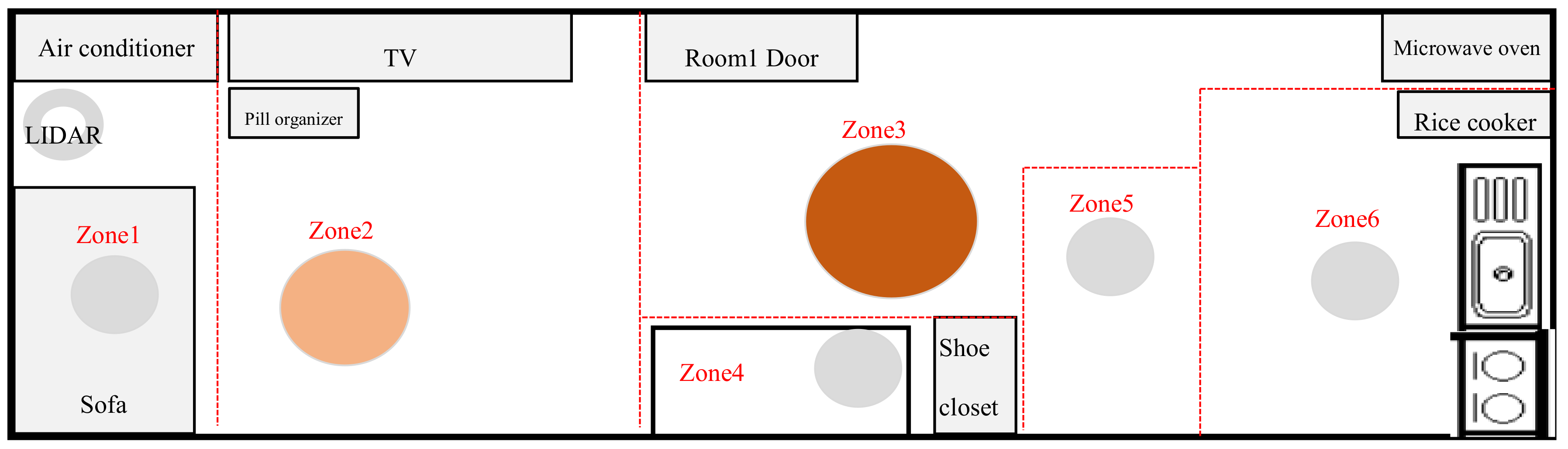
3.1. Experimental Environments
3.2. Experimental Results
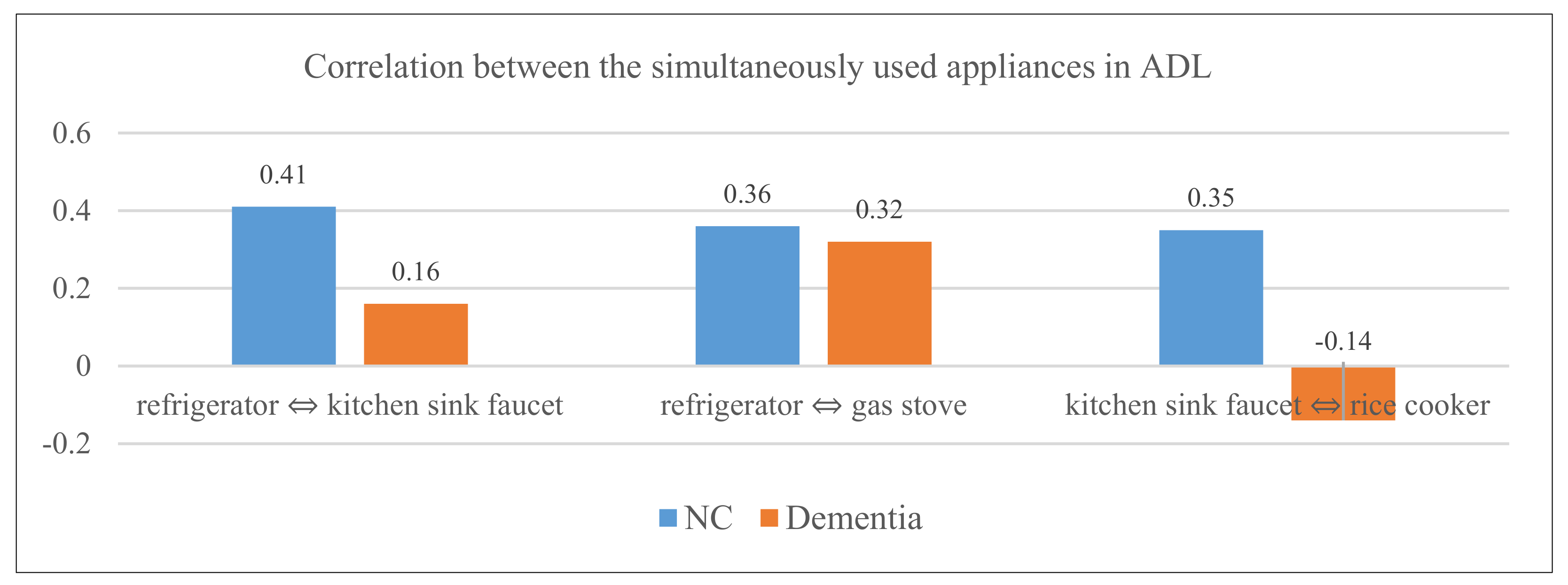
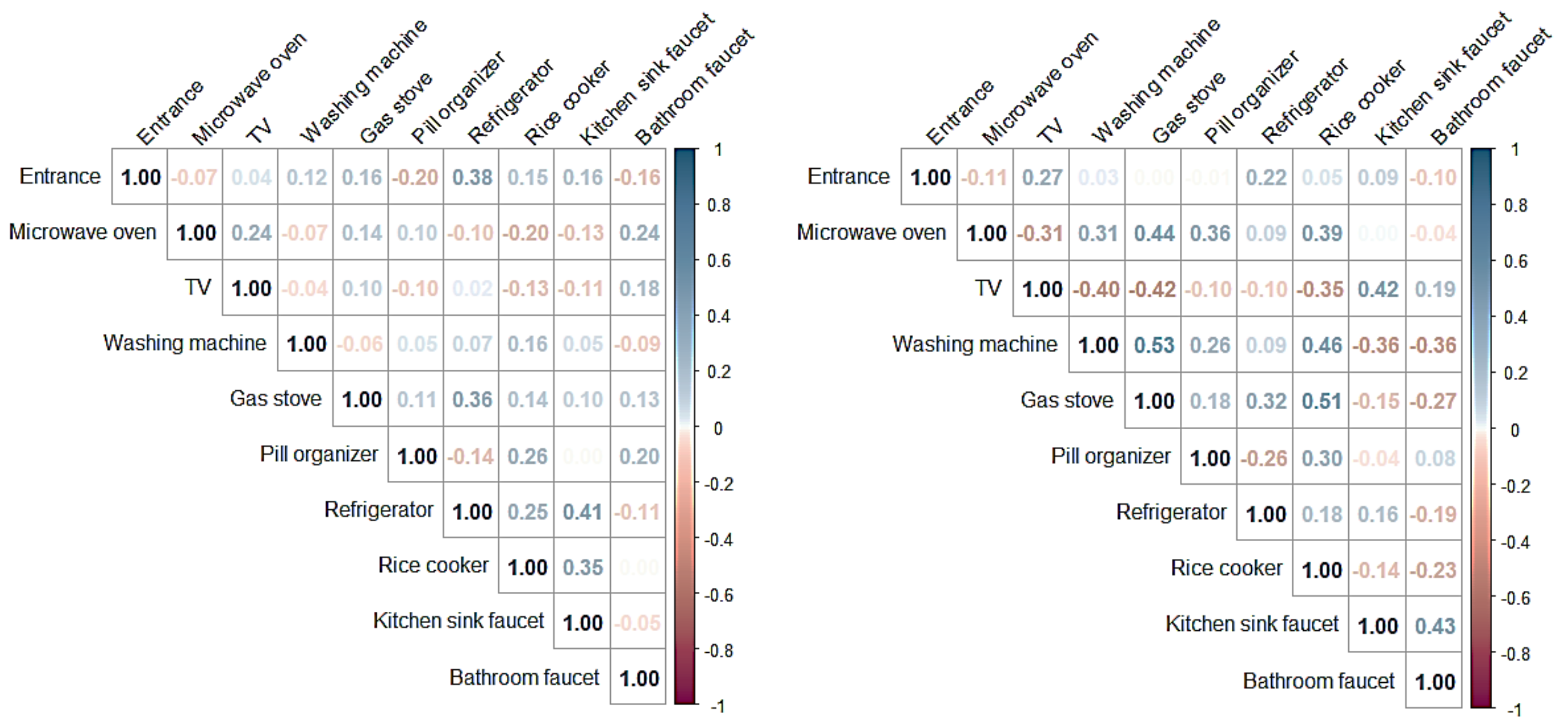
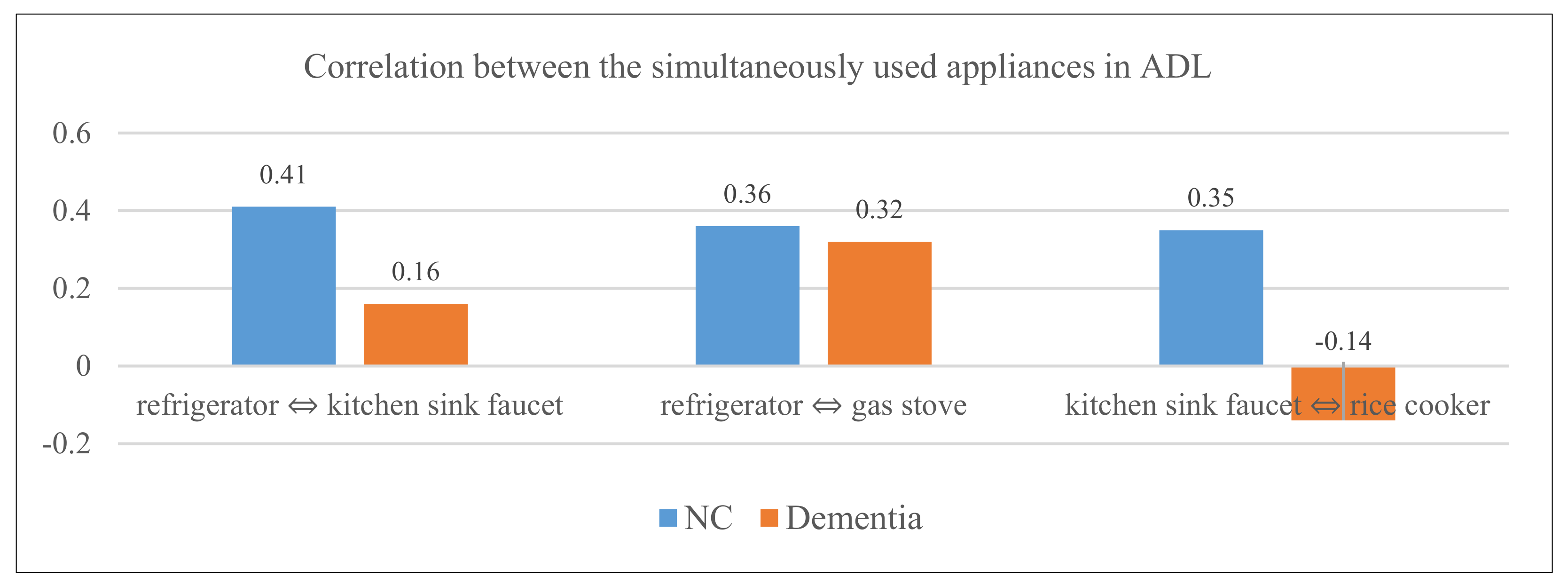
- ‘refrigerator ⇔ kitchen sink faucet’: normal control group (r = 0.41), early-stage dementia group (r = 0.16);
- ‘refrigerator ⇔ gas stove’: normal control group (r = 0.36), early-stage dementia group (r = 0.32);
- ‘kitchen sink faucet ⇔ rice cooker’: normal control group (r = 0.35), early-stage dementia group (r = −0.14).
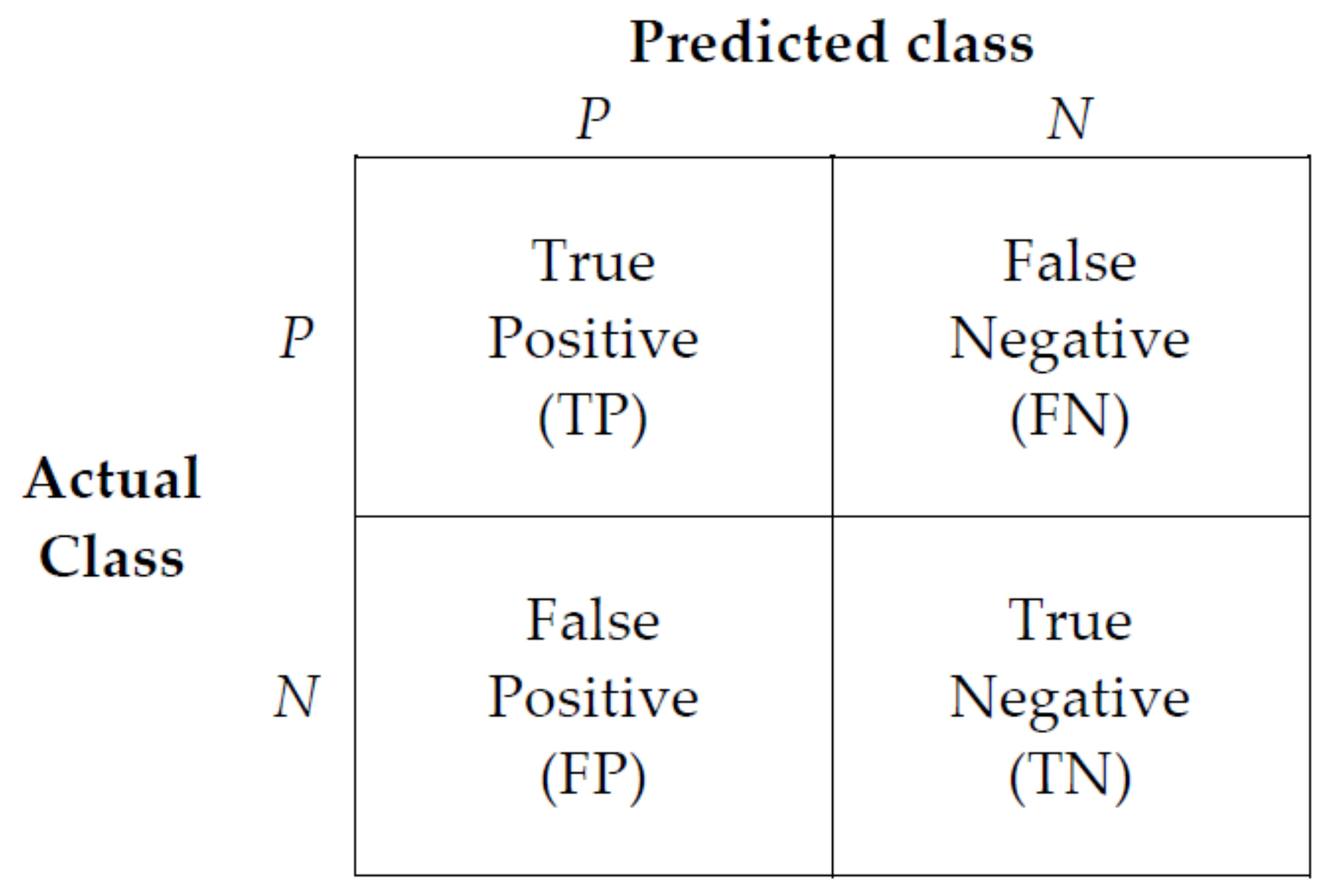
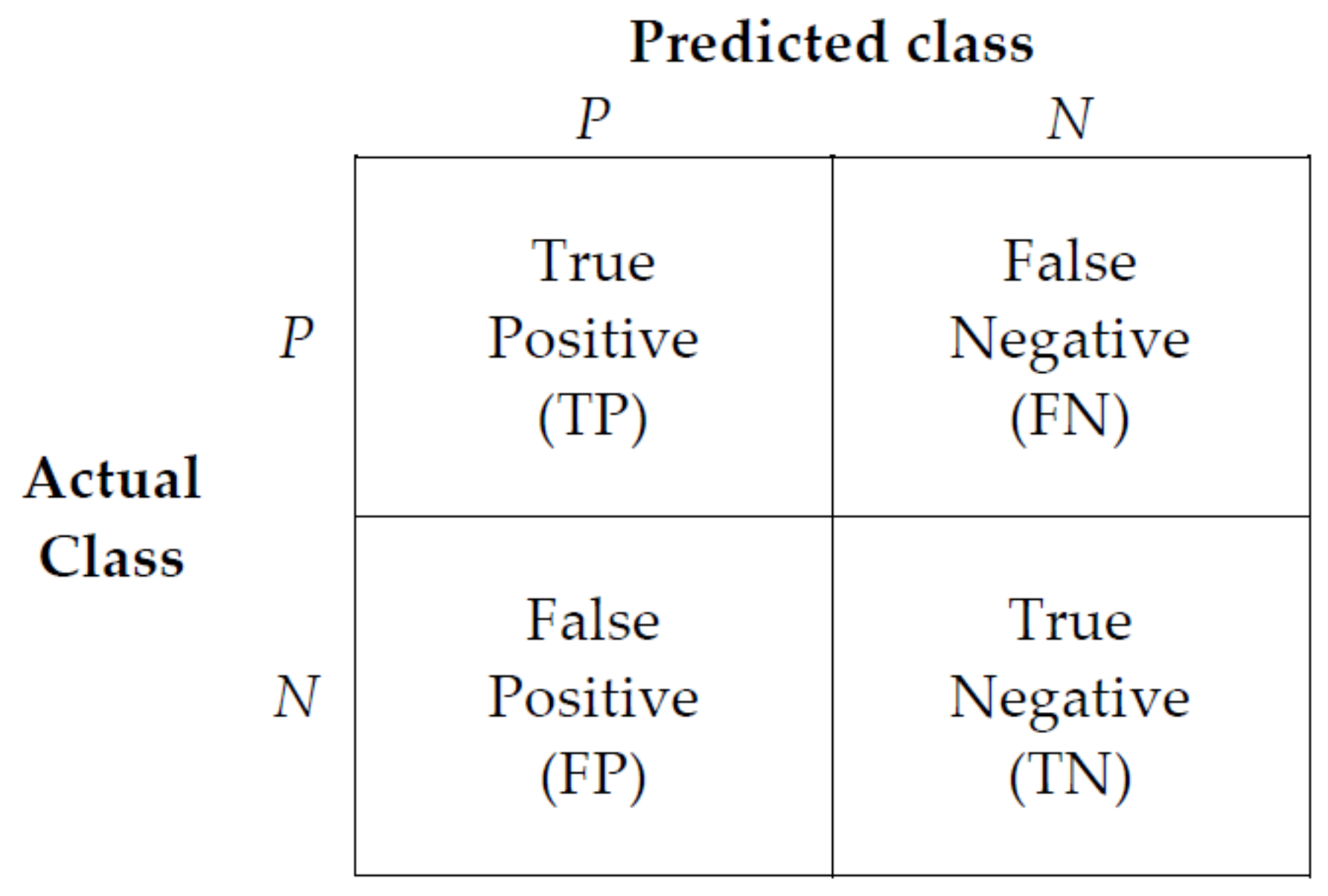
- True Positive (TP): Correct prediction as true when the actual class is true (correct prediction);
- False Positive (FP): Incorrect prediction as true when the actual class is false (incorrect prediction);
- False Negative (FN): Incorrect prediction as false when the actual class is true (incorrect prediction);
- True Negative (TN): Correct prediction as false when the actual class is false (correct prediction).
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Percent of Population Ages 65 and Older, 2020 World Population Data Sheet. Available online: http://prb.org (accessed on 1 June 2021).
- World Health Organisation. Global Action Plan on the Public Health Response to Dementia 2017–2025; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 27 May 2021).
- Ministry of Health and Welfare. 2020 Korean Dementia Observatory; National Institute of Dementia: Seoul, Korea, 2021.
- Lao, K.; Ji, N.; Zhang, X.; Qiao, W.; Tang, Z.; Gou, X. Drug development for Alzheimer’s disease: Review. J. Drug Target. 2019, 27, 164–173. [Google Scholar] [CrossRef]
- Kinsella, G.J.; Mullaly, E.; Rand, E.; Ong, B.; Burton, C.; Price, S.; Phillips, M.; Storey, E. Early intervention for mild cognitive impairment: A randomised controlled trial. J. Neurol. Neurosurg. Psychiatry 2009, 80, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.A.; Rentz, D.M.; Frey, M.T.; Locascio, J.J.; Johnson, K.A.; Sperling, R.A. Alzheimer’s Disease Neuroimaging Initiative. Executive function and instrumental activities of daily living in mild cognitive impairment and Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment report of the guideline development, dissemination, and implementation. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Cummings, J. Mild cognitive impairment (MCI) represents early-stage Alzheimer’s disease. J Alzheimer’s Dis. 2005, 7, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia—Meta-analysis of 41 robust inception cohort studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Farias, S.T.; Mungas, D.; Reed, B.R.; Harvey, D.; Cahn-Weiner, D.; Decarli, C. MCI is associated with deficits in everyday functioning. Alzheimer Dis. Assoc. Disord. 2006, 20, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CENSUS 2019. Available online: https://data.census.gov/cedsci/table?q=living%20alone&tid=ACSDP1Y2019.DP02 (accessed on 2 June 2021).
- Statistics Korea KOSIS (2019). Available online: https://kosis.kr (accessed on 10 June 2021).
- Ministry of Health and Welfare 2019. Available online: http://www.mohw.go.kr/react/index.jsp (accessed on 3 June 2021).
- Grande, G.; Vetrano, D.L.; Cova, I.; Pomati, S.; Mattavelli, D.; Maggiore, L.; Cucumo, V.; Ghiretti, R.; Vanacore, N.; Mariani, C.; et al. Living Alone and Dementia Incidence: A Clinical-Based Study in People With Mild Cognitive Impairment. J. Geriatr. Psychiatry Neurol. 2018, 31, 107–113. [Google Scholar] [CrossRef]
- Tierney, M.C.; Charles, J.; Naglie, G.; Jaglal, S.; Kiss, A.; Fisher, R.H. Risk factors for harm in cognitively impaired seniors who live alone: A prospective study. J. Am. Geriatr. Soc. 2004, 52, 1435–1441. [Google Scholar] [CrossRef]
- Clinical practice guideline for dementia by Clinical Research Center for Dementia of South Korea. J. Korean Med. Assoc. 2011, 54, 861–875. [CrossRef] [Green Version]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontology 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA J. Am. Med Assoc. 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Mioshi, E.; Kipps, C.M.; Dawson, K.; Mitchell, J.; Graham, A.; Hodges, J.R. Activities of daily living in frontotemporal dementia and Alzheimer disease. Neurology 2007, 68, 2077–2084. [Google Scholar] [CrossRef] [PubMed]
- Suh, G.H.; Ju, Y.S.; Yeon, B.K.; Shah, A. A longitudinal study of Alzheimer’s disease: Rates of cognitive and functional decline. Int. J. Geriatr. Psychiatry 2004, 19, 817–824. [Google Scholar] [CrossRef]
- Takechi, H.; Kokuryu, A.; Kubota, T.; Yamada, H. Relative preservation of advanced activities in daily living among patients with mild-to-moderate dementia in the community and overview of support provided by family caregivers. Int. J. Alzheimer’s Dis. 2012, in press. [Google Scholar]
- Chen, Y.; Denny, K.G.; Harvey, D.; Farias, S.T.; Mungas, D.; DeCarli, C.; Beckett, L. Progression from normal cognition to mild cognitive impairment in a diverse clinic-based and community-based elderly cohort. Alzheimer’s Dement. 2017, 13, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farias, S.T.; Lau, K.; Harvey, D.; Denny, K.G.; Barba, C.; Mefford, A.N. Early functional limitations in cognitively normal older adults predict diagnostic conversion to mild cognitive impairment. J. Amer. Geriatr. Soc. 2017, 65, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, A.; Baldereschi, M.; Lamassa, M.; Bovis, F.; Inzitari, M.; Solfrizzi, V.; Panza, F.; Galluzzo, L.; Scafato, E.; Inzitari, D. Daily function as predictor of dementia in cognitive impairment no dementia (CIND) and mild cognitive impairment (MCI): An 8-year follow-up in the ILSA study. J. Alzheimer’s Dis. 2016, 53, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Giebel, C.M.; Sutcliffe, C.; Challis, D. Activities of daily living and quality of life across different stages of dementia: A UK study. Aging Ment. Health 2015, 19, 63–71. [Google Scholar] [CrossRef]
- Skurla, E.; Rogers, J.C.; Sunderland, T. Direct assessment of activities of daily living in Alzheimer’s disease; A controlled study. J. Am. Geriatr. Soc. 1988, 36, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kaye, J.A.; Maxwell, S.A.; Mattek, N.; Hayes, T.L.; Dodge, H.; Pavel, M.; Jimison, H.B.; Wild, K.; Boise, L.; Zitzelberger, T.A. Intelligent systems for assessing aging changes: Home-based, unobtrusive, and continuous assessment of aging. J. Gerontol. B-Psychol. 2011, 66, 180–190. [Google Scholar] [CrossRef]
- Seelye, A.M.; Schmitter-Edgecombe, M.; Cook, D.J.; Crandall, A. Naturalistic assessment of everyday activities and prompting technologies in mild cognitive impairment. J. Int. Neuropsychol. Soc. 2013, 19, 442. [Google Scholar] [CrossRef] [Green Version]
- Karakostas, A.; Meditskos, G.; Stavropoulos, T.G.; Kompatsiaris, I.; Tsolaki, M. A Sensor-Based Framework to Support Clinicians in Dementia Assessment: The Results of a Pilot Study. In Ambient Intelligence—Software and Applications. Advances in Intelligent Systems and Computing; Mohamed, A., Novais, P., Pereira, A., Villarrubia González, G., Fernández-Caballero, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 213–221. [Google Scholar]
- Lim, Y.H.; Baek, Y.; Kang, S.J.; Kang, K.; Lee, H.W. Clinical application of the experimental ADL test for patients with cognitive impairment: Pilot study. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Dawadi, P.N.; Cook, D.J.; Schmitter-Edgecombe, M. Automated Clinical Assessment from Smart home-based Behavior Data. IEEE J Biomed Health Inform. 2016, 20, 1188–1194. [Google Scholar] [CrossRef] [Green Version]
- Alberdi, A.; Weakley, A.; Schmitter-Edgecombe, M.; Cook, D.J.; Aztiria, A.; Basarab, A.; Barrenechea, M. Smart home-based prediction of multi-domain symptoms related to Alzheimer’s Disease. IEEE J. Biomed. Health Inform. 2018, 22, 1720–1731. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.K.; Kim, J.-H.; Ku, H.M. Assessment of Instrumental Activities of Daily Living, Seoul-Instrumental Activities of Daily Living; INPSYT: Seoul, Korea, 2006. [Google Scholar]
- Mobius Open Platform. Available online: http://developers.iotocean.org/archives/module/mobius-open-platform (accessed on 6 January 2020).
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Henry, M.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar]
- Myers, J.L.; Well, A.D. Research Design and Statistical Analysis, 2nd ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 2003; p. 508. ISBN 978-0-8058-4037-7. [Google Scholar]
- Brown, T.B.; Mann, B.; Ryder, N.; Subbiah, M.; Kaplan, J.; Dhariwal, P.; Neelakantan, A.; Shyam, P.; Sastry, G.; Askell, A.; et al. Language models are few-shot learners. In Advances in Neural Information Processing Systems; Neural Information Processing Systems Foundation, Inc.: Barcelona, Spain, 2020. [Google Scholar]
- Choi, E.; Bahadori, M.T.; Kulas, J.A.; Schuetz, A.; Stewart, W.F.; Sun, J. RETAIN: An interpretable predictive model for healthcare using reverse time attention mechanism. In Advances in Neural Information Processing Systems; Neural Information Processing Systems Foundation, Inc.: Barcelona, Spain, 2016. [Google Scholar]
- Jumper, J.; Evans, R.; Pritzel, A.; Green, T.; Figurnov, M.; Ronneberger, O.; Tunyasuvunakool, K.; Bates, R.; Žídek, A.; Potapenko, A.; et al. Highly accurate protein structure prediction with AlphaFold. Nature 2021, 596, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Karras, T.; Laine, S.; Aittala, M.; Hellsten, J.; Lehtinen, J.; Aila, T. Analyzing and improving the image quality of stylegan. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 16–18 June 2020. [Google Scholar] [CrossRef]
- Kipf, T.N.; Welling, M. Semi-supervised classification with graph convolutional networks. In Proceedings of the 5th International Conference on Learning Representations, ICLR 2017—Conference Track Proceedings, Toulon, France, 24–26 April 2017. [Google Scholar]
- Kim, S.J.; Ahn, H.C. Application of random forests to corporate credit rating prediction. J. Ind. Innov. 2016, 32, 187–211. [Google Scholar]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, S.; Lee, S.I. A Unified Approach to Interpreting Model Predictions. Adv. Neural Inf. Process. Syst. 2017, 2017, 4766–4775. [Google Scholar]
- Lim, S.J.; Lee, Z.; Kwon, L.N.; Chun, H.W. Medical Health Records-Based Mild Cognitive Impairment (MCI) Prediction for Effective Dementia Care. Int. J. Environ. Res. Public Health 2021, 18, 9223. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | ADL Assessment Items | Place of Installation | Sensors Used |
|---|---|---|---|
| 1 | Cooking | Microwave oven | Door sensor |
| Refrigerator | Vibration sensor | ||
| Rice cooker | Vibration sensor | ||
| Kitchen sink faucet | Vibration sensor | ||
| Gas stove | Temperature–humidity sensor | ||
| Kitchen | Motion sensor | ||
| 2 | Unlocking and closing entrance door | Entrance | Door sensor |
| Household appliances | Smart plug | ||
| 3 | Using household appliances | Electric mat | Smart plug |
| TV | Smart plug | ||
| Fan | Vibration sensor | ||
| 4 | Household chores | Housecleaning—washing machine | Smart plug |
| Housecleaning—bin, vacuum cleaner | Vibration sensor | ||
| Washing dishes—Kitchen sink faucet | Vibration sensor | ||
| 5 | Grooming | Washbasin, showerhead—bathroom faucet | Vibration sensor |
| Bathroom | Temperature–humidity sensor | ||
| 6 | Taking medications | Pill organizer | Vibration sensor |
| 7 | Indoor wandering | Path of indoor movement and gait speed | Lidar sensor |
| Room | Motion sensor | ||
| Living room | Motion sensor |
| Time | d1 | d2 | d3 | m2 | m3 | m5 | m6 | p2 | p3 | p4 | t1 | v1 | v2 | v3 | v4 | v5 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6 July 2020 | 11 | 4 | 2 | 90 | 3 | 22 | 10 | 5 | 0 | 0 | 1 | 1 | 7 | 0 | 2 | 4 |
| 7 July 2020 | 6 | 0 | 2 | 78 | 1 | 26 | 6 | 2 | 0 | 0 | 3 | 2 | 9 | 1 | 6 | 3 |
| 8 July 2020 | 6 | 2 | 0 | 111 | 3 | 9 | 8 | 4 | 0 | 0 | 1 | 4 | 8 | 0 | 0 | 2 |
| 10 July 2020 | 5 | 3 | 0 | 103 | 0 | 13 | 9 | 3 | 0 | 2 | 3 | 2 | 10 | 0 | 5 | 5 |
| 11 July 2020 | 13 | 4 | 0 | 115 | 0 | 36 | 9 | 4 | 0 | 2 | 0 | 0 | 10 | 0 | 4 | 2 |
| 13 July 2020 | 9 | 4 | 0 | 112 | 0 | 19 | 10 | 2 | 0 | 0 | 2 | 2 | 12 | 3 | 24 | 1 |
| 15 July 2020 | 7 | 5 | 1 | 125 | 0 | 23 | 9 | 3 | 0 | 0 | 3 | 1 | 11 | 0 | 10 | 5 |
| Category | Level of Cognitive Function | MMSE | Range of Personalized Anomaly Detection Criteria |
|---|---|---|---|
| Normal controls | No Cognitive Decline | 30 | When the MMSE score is out of “Lower Q1 − 1.5 × IQR/Upper Q3 + 1.5 × IQR” |
| Very Mild Cognitive Decline | ~ | When the MMSE score is out of “Lower Q1 − 1.2 × IQR/Upper Q3 + 1.2 × IQR” | |
| Mild Cognitive Decline | 24 | When the MMSE score is out of “Lower Q1 − 1 × IQR/Upper Q3 + 1 × IQR” | |
| Early-stage Dementia | Moderate Cognitive Decline | 23 ~ | When the MMSE score is out of “Lower Q1 − 0.5 × IQR/Upper Q3 + 0.5 × IQR” |
| Type of Analysis Data | Description | |
|---|---|---|
| IoT sensor data | IoT Count | All counts detected by the vibration sensor or motion sensor |
| IoT Duration | Duration of movement detected in front of the motion sensor | |
| Lidar | Indoor movement distance and gait speed detected by 2D-Lidar | |
| ADL data | ADL Count | Number of times ADL activities were performed (6 types + indoor wandering) |
| ADL Duration | Time taken for ADL activities (6 types + indoor wandering) | |
| ADL Item | Feature | Description |
|---|---|---|
| Indoor wandering | Movement in a room | Data of the participant’s movements in a room |
| Indoor wandering late at night | All sensor data recorded between 00.00 and 5.00 | |
| Unlocking and closing entrance door | Going out | Data from the time of closing the door and to the opening of the door. In case there was a sensor that started operation, this case was not considered as going out. |
| No locking of the entrance door | Data for cases of the sensor operation during the time of the participant’s going out. | |
| Household chores | Laundering (washing machine) | Data of washing machine use from the start to the end of the washing machine operation |
| Washing dishes | Data of using kitchen sink faucet for longer than 30 s | |
| Cooking | Cooking | When two or more kitchen appliances had been used and the temperature of a gas stove had increased (including all cooking for less than 30 min) |
| Breakfast cooking | Cooking between 5:00 and 10:00 | |
| Lunch cooking | Cooking between 12:00 and 15:00 | |
| Dinner cooking | Cooking between 17:00 and 20:00 | |
| Cooking for over 30 min | Cooking data lasting longer than 30 min | |
| Cooking (gas stove—microwave oven) | When the sensors used during cooking included the gas stove and microwave oven | |
| Cooking (refrigerator—kitchen sink faucet) | When the sensors used during cooking included the refrigerator and kitchen sink faucet | |
| Cooking (refrigerator—gas stove) | When the sensors used during cooking included the refrigerator and gas stove | |
| Cooking (kitchen sink faucet— rice cooker) | When the sensors used during cooking included the kitchen sink faucet and rice cooker | |
| Heating food (microwave oven) | When the sensors used during cooking included the microwave oven but not the gas stove | |
| Taking medications | Morning medications | Taking medications between 5:00 and 10:00 |
| Lunchtime medications | Taking medications between 12:00 and 15:00 | |
| Evening medications | Taking medications between 17:00 and 20:00 | |
| Medications before going to bed | Taking medications between 21:00 and 24:00 | |
| Grooming (personal hygiene) | Use of bathroom faucet (Nighttime) | All the data with the start time of the bathroom faucet use between 00:00 and 04:00 |
| Use of showerhead | Use of the showerhead installed in the bathroom faucet | |
| Use of bathroom faucet for more than 1 min | Use of bathroom faucet over 1 min but not the showerhead | |
| Bathroom faucet (total) | Data for all hours of bathroom faucet use | |
| Using household appliances | TV (total) | Total hours of watching TV over 24 h |
| TV watching in the morning | TV watching between 04:00 and 12:00 | |
| TV watching at night | TV watching between 00:00 and 04:00 | |
| TV after going out | Data of TV turned on for 30 min after the participant’s returning from going out | |
| Electric mat (total) | Total hours of using electric mat over 24 h | |
| Electric mat—Daytime | Use of electric mat between 12:00 and 16:00 | |
| Electric mat—Nighttime | Use of electric mat between 00:00 and 04:00 |
| Category | Age | MMSE | CDR |
|---|---|---|---|
| Normal Controls (n = 7) | 86 | 26 | 0 |
| 79 | 29 | 0 | |
| 84 | 25 | 0 | |
| 72 | 27 | 0 | |
| 67 | 26 | 0 | |
| 74 | 30 | 0 | |
| 90 | 30 | 0 | |
| Average of Normal Controls | 78.8 | 27.5 | 0 |
| Early-stage dementia group (n = 6) | 87 | 20 | 1 |
| 76 | 13 | 1 | |
| 86 | 18 | 1 | |
| 76 | 30 | 0.5 | |
| 85 | 11 | 1 | |
| 72 | 14 | 1 | |
| Average of early-stage dementia group | 80.3 | 17.6 | 0.92 |
| Sensor Location | p-Value |
|---|---|
| Entrance | 0.03643 (<0.05) |
| Microwave oven | 0.4745 |
| Gas stove | 6.431 × 10−12 (<0.05) |
| TV | 4.363 × 10−7 (<0.05) |
| Washing machine | 3.908 × 10−7 (<0.05) |
| Pill organizer | 0.1878 |
| Refrigerator | 0.003404 (<0.05) |
| Rice cooker | 0.03521 (<0.05) |
| Kitchen sink faucet | 5.385 × 10−7 (<0.05) |
| Bathroom faucet | 2.2 × 10−16 (<0.05) |
| ADL | p-Value |
|---|---|
| Grooming | 6.728 × 10−15 (<0.05) |
| Using household appliances | 1.063 × 10−7 (<0.05) |
| Cooking | 0.01343 (<0.05) |
| Household chores | 0.9674 |
| Statistic | Gait Speed of Normal Controls (km/h) | Gait Speed of Early-Stage Dementia Group (km/h) |
|---|---|---|
| Min | 0.600 | 0.6007 |
| Median | 0.930 | 1.0803 |
| Mean | 1.023 | 1.2091 |
| Max | 5.615 | 3.9251 |
| Feature Set | Patients# | Data# | Mean Data Length | Feature# (IoT) | Feature#(ADL) |
|---|---|---|---|---|---|
| IoT | 13 (NC: 7, Dem: 6) | 20,184 (Dem: 7800, NC: 12,384) | 1441 (Dem: 1114, NC: 1769) | 132 | . |
| ADL | 13 (NC: 7, Dem: 6) | 20,184 (Dem: 7800, NC: 12,384) | 1441 (Dem: 1114, NC: 1769) | . | 63 |
| IoT + ADL | 13 (NC: 7, Dem: 6) | 20,184 (Dem: 7800, NC: 12,384) | 1441 (Dem: 1114, NC: 1769) | 132 | 63 |
| Before Personalization | After Personalization | |||||
|---|---|---|---|---|---|---|
| IoT | ADL | IoT + ADL | IoT | ADL | IoT + ADL | |
| Precision | 80.65% | 63.99% | 79.47% | 85.29% | 79.62% | 88.47% |
| Recall | 71.43% | 59.08% | 81.87% | 82.62% | 76.92% | 90.03% |
| F1-score | 75.76% | 61.44% | 80.65% | 83.94% | 78.25% | 89.24% |
| Accuracy | 80.98% | 65.52% | 84.54% | 86.80% | 83.47% | 91.20% |
| No | Major Features with a Significant Impact |
|---|---|
| 1 | Duration of using electric mat (Late-night hours from 0:00 to 5:00 and Evening hours from 17:00 to 24:00) |
| 2 | Duration of using microwave oven (Late-night hours from 0:00 to 5:00) |
| 3 | Duration of TV watching (Late-night hours from 0:00 to 5:00) |
| 4 | Duration of using cooking appliances (Refrigerator-gas stove) |
| 5 | Duration of using gas stove (Daytime hours from 11:00 to 17:00 and Evening hours from 17:00 to 24:00) |
| 6 | Duration of using showerhead |
| 7 | Duration of using entrance |
| 8 | Duration of using bathroom faucet |
| 9 | Duration of using washing machine (Morning hours from 5:00 to 11:00) |
| 10 | Duration of using refrigerator |
| 11 | Duration of washing dishes |
| 12 | Duration of using cooking appliances (refrigerator-kitchen sink faucet) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, L.-N.; Yang, D.-H.; Hwang, M.-G.; Lim, S.-J.; Kim, Y.-K.; Kim, J.-G.; Cho, K.-H.; Chun, H.-W.; Park, K.-W. Automated Classification of Normal Control and Early-Stage Dementia Based on Activities of Daily Living (ADL) Data Acquired from Smart Home Environment. Int. J. Environ. Res. Public Health 2021, 18, 13235. https://doi.org/10.3390/ijerph182413235
Kwon L-N, Yang D-H, Hwang M-G, Lim S-J, Kim Y-K, Kim J-G, Cho K-H, Chun H-W, Park K-W. Automated Classification of Normal Control and Early-Stage Dementia Based on Activities of Daily Living (ADL) Data Acquired from Smart Home Environment. International Journal of Environmental Research and Public Health. 2021; 18(24):13235. https://doi.org/10.3390/ijerph182413235
Chicago/Turabian StyleKwon, Lee-Nam, Dong-Hun Yang, Myung-Gwon Hwang, Soo-Jin Lim, Young-Kuk Kim, Jae-Gyum Kim, Kwang-Hee Cho, Hong-Woo Chun, and Kun-Woo Park. 2021. "Automated Classification of Normal Control and Early-Stage Dementia Based on Activities of Daily Living (ADL) Data Acquired from Smart Home Environment" International Journal of Environmental Research and Public Health 18, no. 24: 13235. https://doi.org/10.3390/ijerph182413235
APA StyleKwon, L.-N., Yang, D.-H., Hwang, M.-G., Lim, S.-J., Kim, Y.-K., Kim, J.-G., Cho, K.-H., Chun, H.-W., & Park, K.-W. (2021). Automated Classification of Normal Control and Early-Stage Dementia Based on Activities of Daily Living (ADL) Data Acquired from Smart Home Environment. International Journal of Environmental Research and Public Health, 18(24), 13235. https://doi.org/10.3390/ijerph182413235