
Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers

 ,
, 
 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
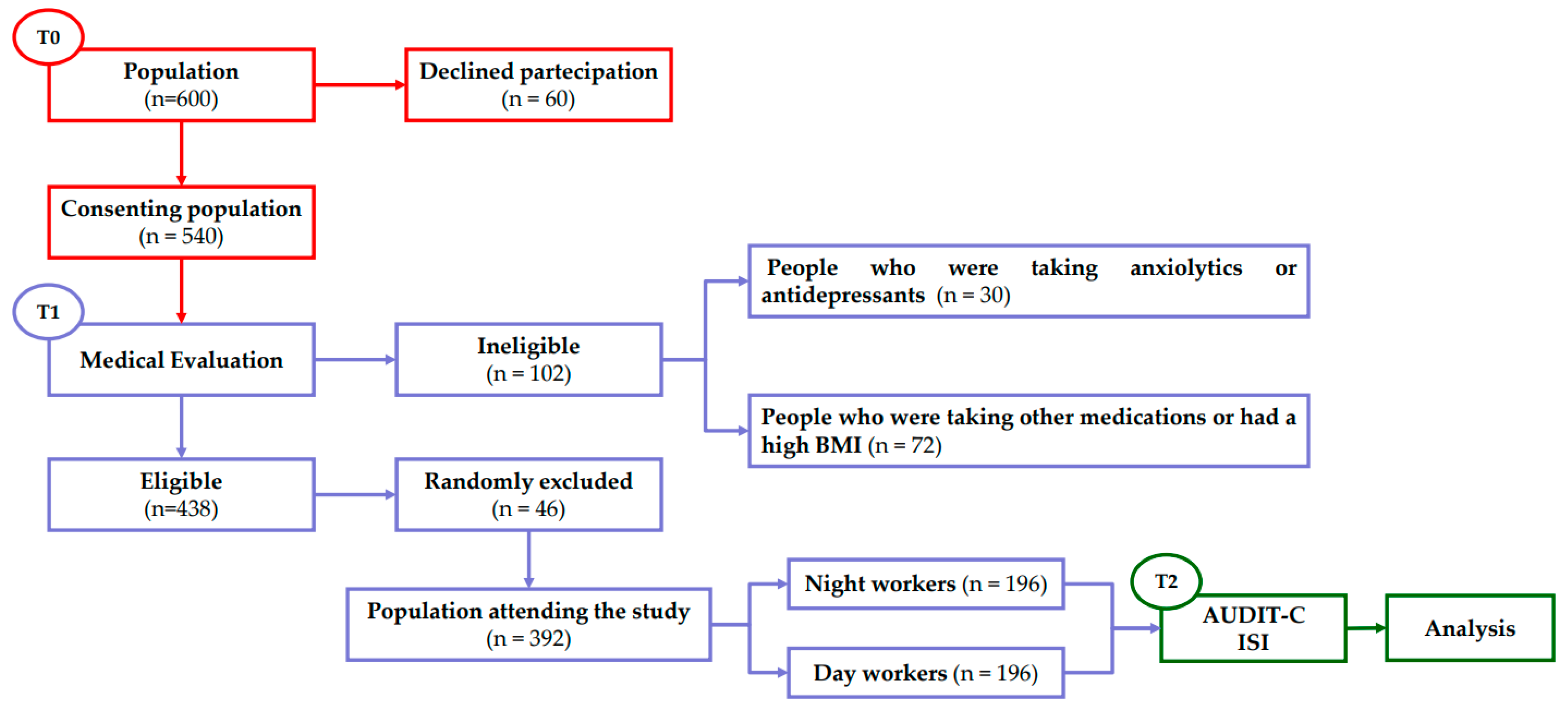
2.1. Design
2.2. Assessment of Alcohol Consumption
2.3. Assessment of Insomnia Disorder
2.4. Statistical Analysis
3. Results
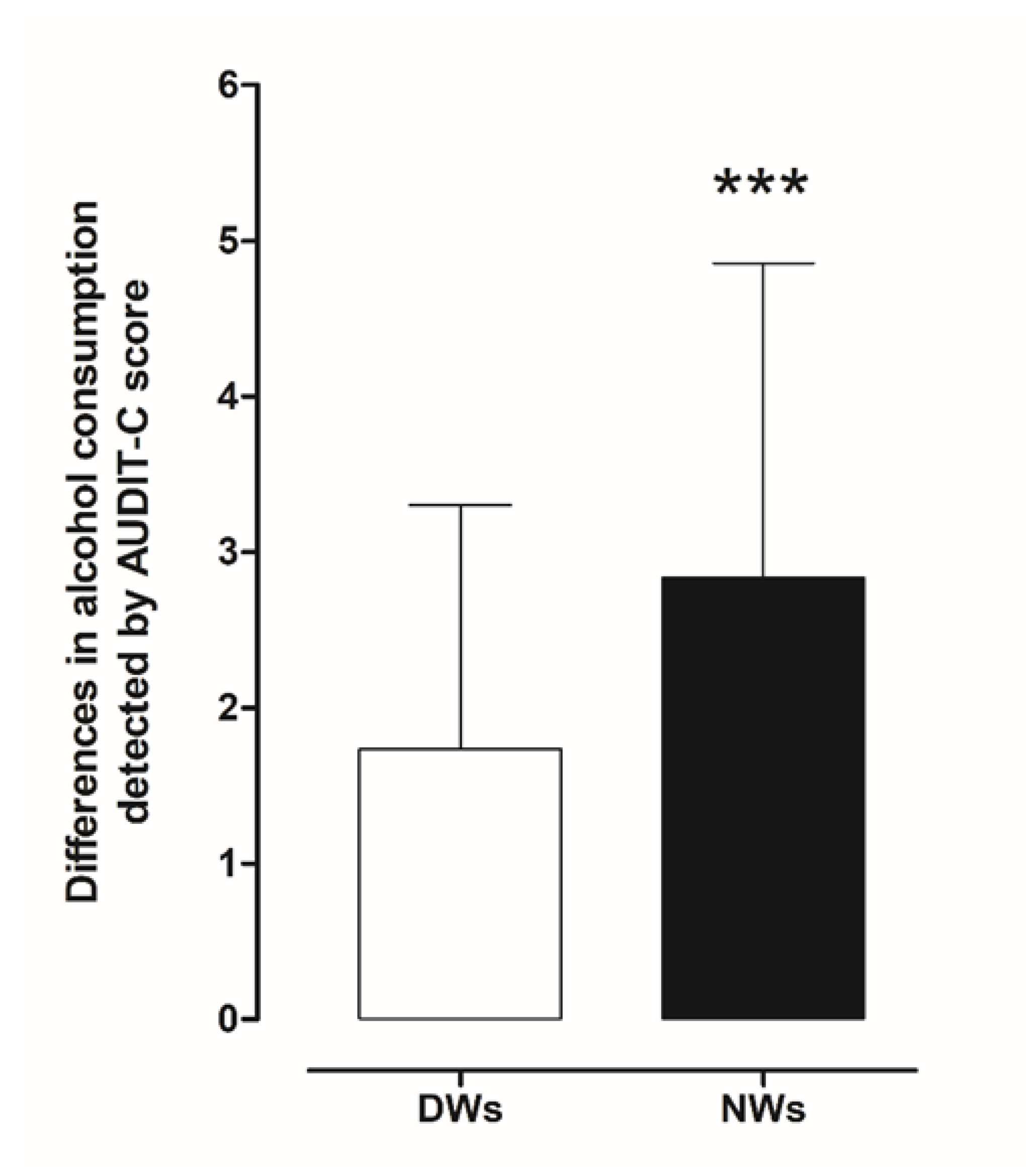
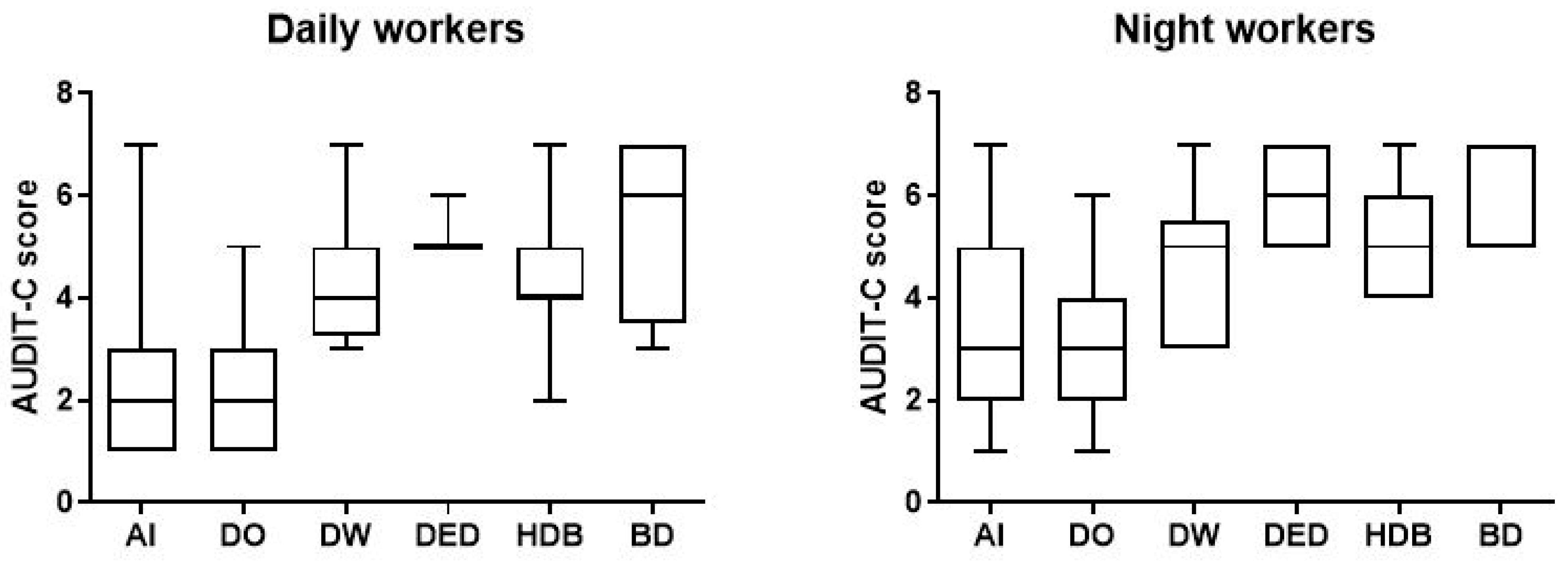
3.1. Alcohol Consumption
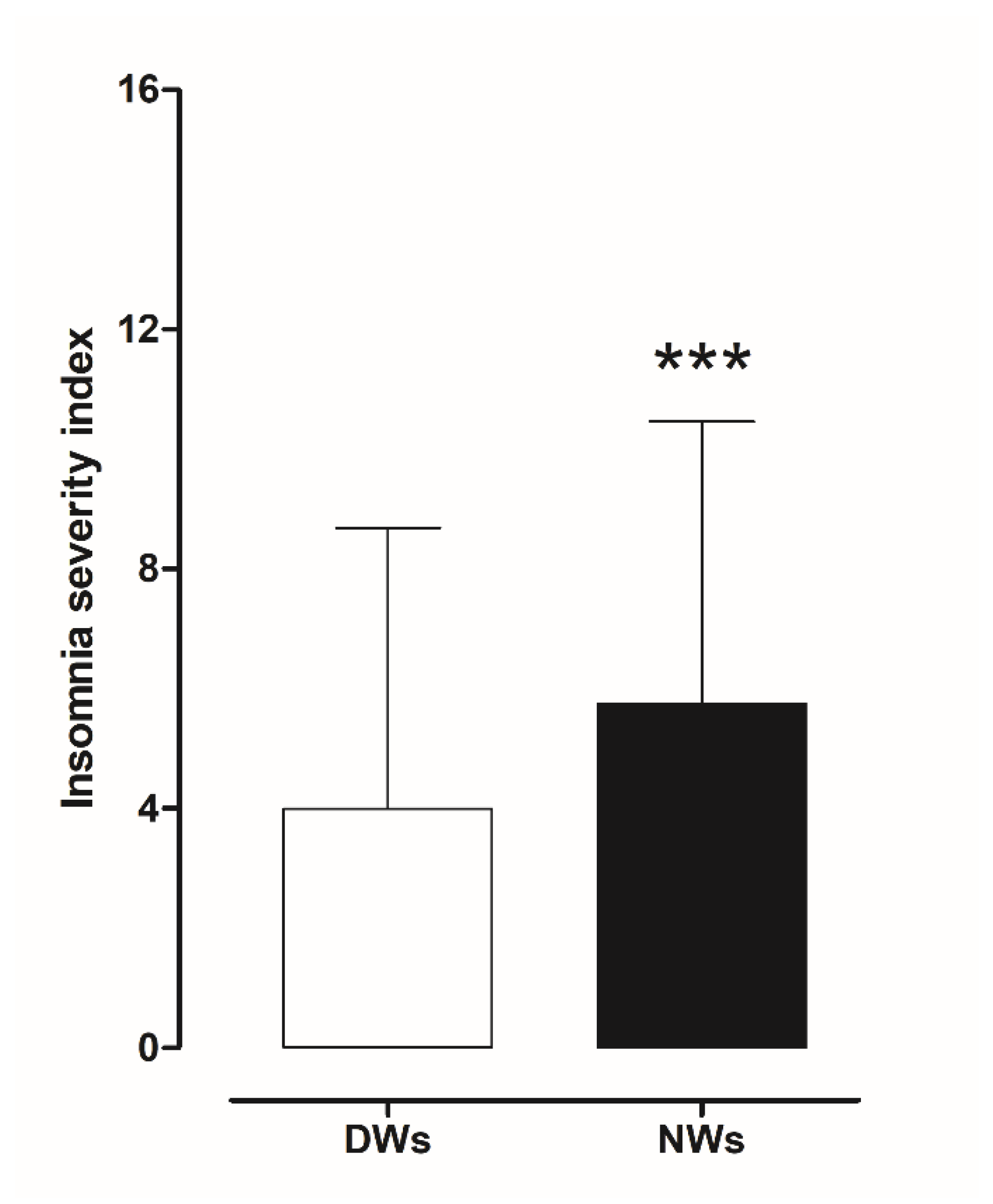
3.2. Insomnia Severity Index (ISI)
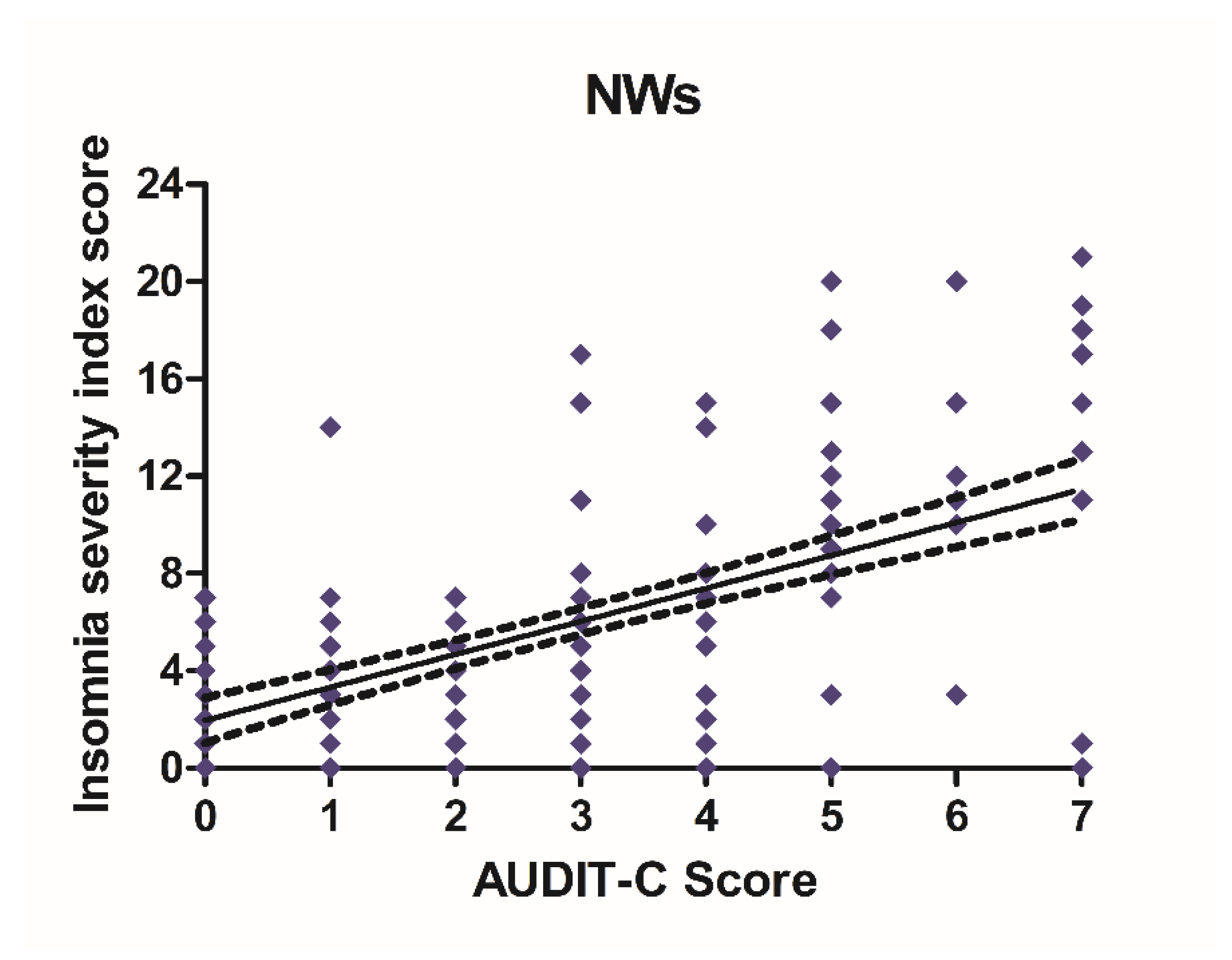
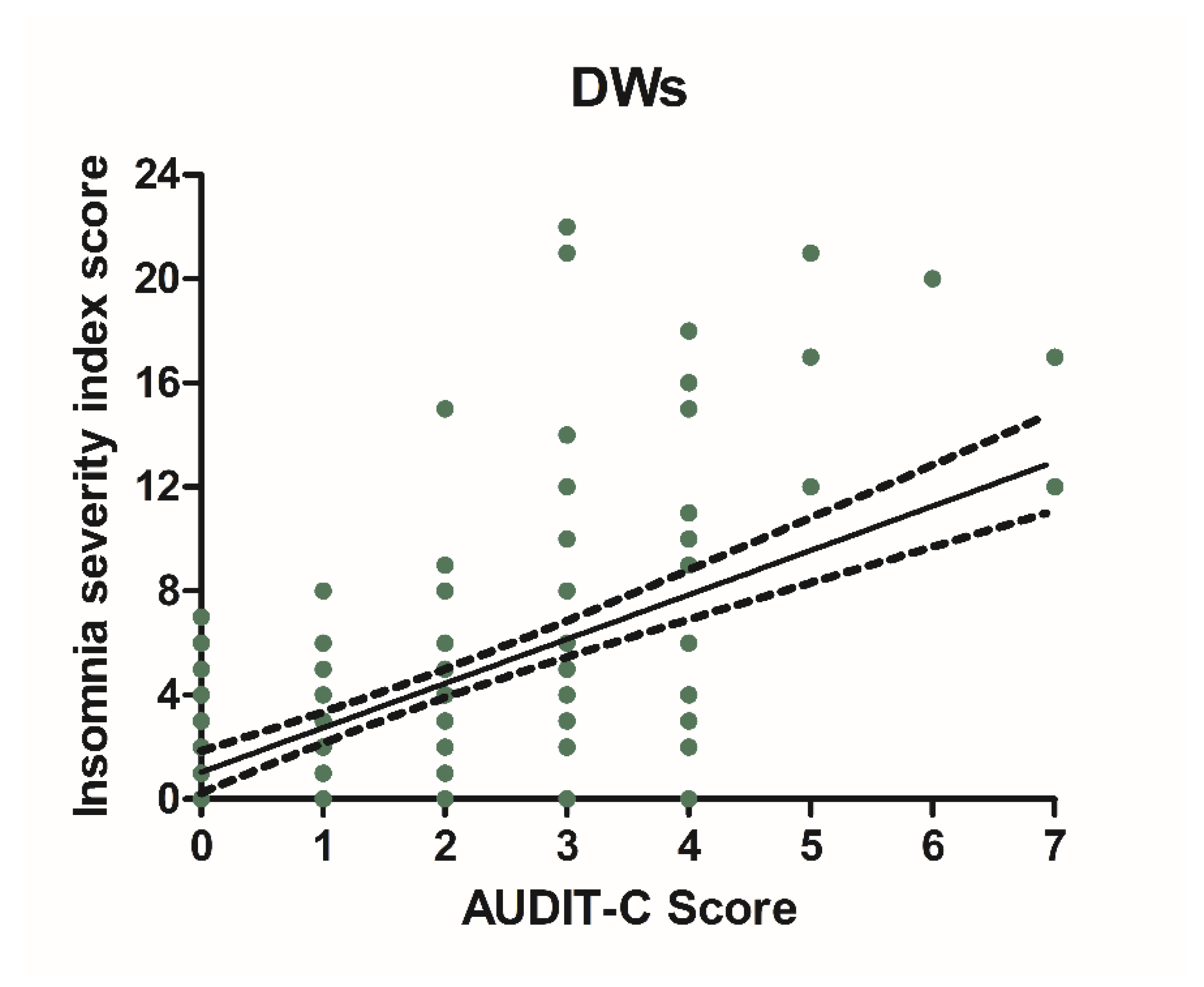
3.3. Alcohol Consumption and Insomnia Disorder
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cipriani, G.; Lucetti, C.; Danti, S.; Nuti, A. Sleep disorders and dementia. Psychogeriatrics 2015, 15, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.J.; Peterson, M.J. Sleep disorders in depression. Sleep Med. Clin. 2015, 10, 17–23. [Google Scholar] [CrossRef]
- Robinson-Shelton, A.; Malow, B.A. Sleep disturbances in neurodevelopmental disorders. Curr. Psychiatry Rep. 2016, 18, 6. [Google Scholar] [CrossRef]
- Angarita, G.A.; Emadi, N.; Hodges, S.; Morgan, P.T. Sleep abnormalities associated with alcohol, cannabis, cocaine, and opioid use: A comprehensive review. Addict. Sci. Clin. Pract. 2016, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Ramaci, T.; Barattucci, M.; Vella, F.; Senia, P.; Cannizzaro, E.; Scorciapino, A.; Ledda, C.; De Giorgio, A.; Rapisarda, V. Straining at Work and Its Relationship with Personality Profiles and Individual Consequences in Healthcare Workers (HCWs). Int. J. Environ. Res. Public Health 2020, 17, 610. [Google Scholar] [CrossRef]
- Cannizzaro, E.; Plescia, F.; Cirrincione, L.; Lo Pinto, E.; Plescia, F. Sport for job differences in cortisol levels in a water polo team at different times of workout. EuroMediterranean Biomed. J. 2018, 13, 181–184. [Google Scholar]
- Ting, L.; Malhotra, A. Sleep disorders: An overview. Prim. Care Clin. Off. Pr. 2005, 32, 305–318. [Google Scholar] [CrossRef]
- Goldstein, I.B.; Ancoli-Israel, S.; Shapiro, D. Relationship between daytime sleepiness and blood pressure in healthy older adults. Am. J. Hypertens. 2004, 17, 787–792. [Google Scholar] [CrossRef]
- Alvarez, G.G.; Ayas, N.T. The impact of daily sleep duration on health: A review of the literature. Prog. Cardiovasc. Nurs. 2004, 19, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Hanly, P. Sleep apnea and daytime sleepiness in end-stage renal disease. Semin. Dial. 2004, 17, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Hilton, M.F.; Chappell, M.J.; Bartlett, W.A.; Malhotra, A.; Beattie, J.M.; Cayton, R.M. Sleep apnea/hypopnea syndrome depresses vagal tone on awakening independently of sympathetic activation. Eur. Respir J. 2001, 17, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Hepburn, M.; Bollu, P.C.; French, B.; Sahota, P. Sleep Medicine: Stroke and Sleep. Mo. Med. 2018, 115, 527–532. [Google Scholar]
- Duce, B.; Kulkas, A.; Langton, C.; Töyräs, J.; Hukins, C. The prevalence of REM-related obstructive sleep apnoea is reduced by the AASM 2012 hypopnoea criteria. Sleep Breath 2018, 22, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Covassin, N.; Bock, J.M.; Mohamed, E.A.; Pappoppula, L.P.; Shafi, C.; Lopez-Jimenez, F.; Somers, V.K. Excessive Daytime Sleepiness and Cardiovascular Mortality in US Adults: A NHANES 2005–2008 Follow-Up Study. Nat. Sci. Sleep 2021, 13, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Olszowka, M.; Held, C.; Hadziosmanovic, N.; Denchev, S.; Manolis, A.; Wallentin, L.; White, H.D.; Stewart, R.A.H.; Hagström, E.; STABILITY Investigators. Excessive daytime sleepiness, morning tiredness and major adverse cardiovascular events in patients with chronic coronary syndrome. J. Intern. Med. 2021, 290, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.J.; Mallory, L.J.; Lichstein, K.L.; Durrence, H.H.; Riedel, B.W.; Bush, A.J. Comorbidity of chronic insomnia with medical problems. Sleep 2007, 30, 213–218. [Google Scholar] [CrossRef]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disorders and chronic disease in older adults: Results from the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Ballacchino, A.; Salvago, P.; Cannizzaro, E.; Costanzo, R.; Di Marzo, M.; Ferrara, S.; Mattina, E.L.; Messina, G.; Mucia, M.; Mule, L.; et al. Association between sleep-disordered breathing and hearing disorders: Clinical observation in Sicilian patients. Acta Med. Mediterr. 2015, 31, 607–614. [Google Scholar]
- Pace, A.; Iannella, G.; Rossetti, V.; Visconti, I.C.; Gulotta, G.; Cavaliere, C.; De Vito, A.; Maniaci, A.; Cocuzza, S.; Magliulo, G.; et al. Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis. Medicina 2020, 56, 454. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wu, Y.; Wu, P.; Xu, Z.; Ni, X. Analysis of the impact of allergic rhinitis on the children with sleep disordered breathing. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110380. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Cannizzaro, E.; Alba, D.; Conforto, A.; Cimino, L.; Mazzucco, W. Sars-CoV-2 pandemic in the mediterranean area: Epidemiology and perspectives. EuroMediterranean Biomed. J. 2020, 15, 102–106. [Google Scholar]
- Cirrincione, L.; Rapisarda, V.; Mazzucco, W.; Provenzano, R.; Cannizzaro, E. Sars-CoV-2 and the Risk Assessment Document in Italian Work; Specific or Generic Risk Even If Aggravated? Int. J. Environ. Res. Public Health 2021, 18, 3729. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, E.; Cannizzaro, C.; Martorana, D.; Moscadini, S.; Coco, D.L. Effects of shift work on cardiovascular activity, serum cortisol and white blood cell count in a group of Italian fishermen. EuroMediterranean Biomed. J. 2012, 2012, 109–113. [Google Scholar]
- C171-Convention on Night Work, n. 171; International Labour Organisation (ILO): Geneva, Switzerland, 1990.
- Rajaratnam, S.M.; Arendt, J. Health in a 24-h society. Lancet 2001, 358, 999–1005. [Google Scholar] [CrossRef]
- Cannizzaro, E.; Cirrincione, L.; Mazzucco, W.; Scorciapino, A.; Catalano, C.; Ramaci, T.; Ledda, C.; Plescia, F. Night-Time Shift Work and Related Stress Responses: A study of security guards. Int. J. Environ. Res. Public Health 2020, 17, 562. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, V.; Cannizzaro, E.; Barchitta, M.; Vitale, E.; Cinà, D.; Minciullo, F.; Matera, S.; Bracci, M.; Agodi, A.; Ledda, C. A Combined Multidisciplinary Intervention for Health Promotion in the Workplace: A Pilot Study. J. Clin. Med. 2021, 10, 1512. [Google Scholar] [CrossRef] [PubMed]
- Maggiulli, R.; Giancani, A.; Fabozzi, G.; Dovere, L.; Tacconi, L.; Amendola, M.G.; Cimadomo, D.; Ubaldi, F.M.; Rienzi, L. Assessment and management of the risk of SARS-CoV-2 infection in an IVF laboratory. Reprod. Biomed. Online 2020, 41, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Soleo, L.; Cannizzaro, E.; Lovreglio, P.; Basso, A.; D’Errico, M.N.; Pira, E. Protocols for the health surveillance [Protocolli per la sorveglianza sanitaria dei lavoratori della pesca]. G. Ital. Med. Lav. Ergon. 2013, 35, 222–226. [Google Scholar]
- Plescia, F.; Brancato, A.; Venniro, M.; Maniaci, G.; Cannizzaro, E.; Sutera, F.M.; Caro, V.D.; Giannola, L.I.; Cannizzaro, C. Acetaldehyde self-administration by a two-bottle choice paradigm: Consequences on emotional reactivity, spatial learning, and memory. Alcohol 2015, 49, 139–148. [Google Scholar] [CrossRef]
- Plescia, F.; Cannizzaro, E.; Brancato, A.; Martines, F.; Di Naro, A.; Mucia, M.; Plescia, F.; Vita, C.; Salvago, P.; Mulè, A.; et al. Acetaldehyde effects in the brain. Acta Med. Mediterr. 2015, 31, 813–817. [Google Scholar]
- Roehrs, T.A.; Roth, T. Sleep Disturbance in Substance Use Disorders. Psychiatr. Clin. N. Am. 2015, 38, 793–803. [Google Scholar] [CrossRef] [PubMed]
- NIDA. Links between Sleep and Substance Use Disorders. National Institute on Drug Abuse Website. Available online: https://www.drugabuse.gov/about-nida/noras-blog/2020/03/connections-between-sleep-substance-use-disorders (accessed on 5 June 2021).
- Chakravorty, S.; Vandrey, R.G.; He, S.; Stein, M.D. Sleep management among patients with substance use disorders. Med. Clin. N. Am. 2018, 102, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Nakagawa, H.; Miura, K.; Soyama, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nogawa, K. Effect of shift work on body mass index and metabolic parameters. Scand. J. Work Environ. Health 2007, 33, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Pietroiusti, A.; Neri, A.; Somma, G.; Coppeta, L.; Iavicoli, I.; Bergamaschi, A.; Magrini, A. Incidence of metabolic syndrome among night shift health workers. Occup. Environ. Med. 2010, 67, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Biggi, N.; Consonni, D.; Galluzzo, V.; Sogliani, M.; Costa, G. Metabolic syndrome in permanent night workers. Chronobiol. Int. 2008, 25, 443–454. [Google Scholar] [CrossRef]
- Gibson, M. A systematic review of the relationship between night shift work and oxidative stress. Chronobiol. Int. 2021, 14, 1–14. [Google Scholar] [CrossRef]
- Pearson, T.A.; Blair, S.N.; Daniels, S.R.; Eckel, R.H.; Fair, J.M.; Fortmann, S.P.; Franklin, B.A.; Goldstein, L.B.; Greenland, P.; Grundy, S.M.; et al. AHA guidelines for primary prevention of cardiovascular disease and stroke: 2002 update: Consensus group guidance on comprehensive risk reduction for adult patients without coronary artery disease or other atherosclerotic vascular disease. Circulation 2002, 2002, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Heath, G.; Sargent, C.; Banks, S.; Coates, A. Alcohol use in shift workers. Accid. Anal. Prev. 2017, 99, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Coates, A.; Heath, G.; Banks, S. Patterns of alcohol consumption and sleep in shiftworkers. In Sleep Modulation by Obesity, Diabetes, Age, and Diet; Watson, R.R., Ed.; Academic Press: London, UK, 2014; pp. 353–361. [Google Scholar]
- Buchvold, H.V.; Pallesen, S.; Øyane, N.M.; Bjorvatn, B. Associations between night work and BMI, alcohol, smoking, caffeine and exercise—A cross-sectional study. BMC Public Health 2015, 15, 1112. [Google Scholar] [CrossRef] [PubMed]
- Flo, E.; Pallesen, S.; Magerøy, N.; Moen, B.E.; Grønli, J.; Hilde Nordhus, I.; Bjorvatn, B. Shift Work Disorder in Nurses-Assessment, Prevalence and Related Health Problems. PLoS ONE 2012, 7, e33981. [Google Scholar] [CrossRef] [PubMed]
- Hermansson, U.; Knutsson, A.; Brandt, L.; Huss, A.; Rönnberg, S.; Helander, A. Screening for high risk and high alcohol consumption in day and shift workers using AUDIT and CDT. Occup. Med. 2003, 53, 518–526. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DSM-5. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Arlington, V.A., Ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Chakravorty, S.; Chaudhary, N.S.; Brower, K.J. Alcohol dependence and its relationship to insomnia and other sleep disorders. Alcohol Clin. Exp. Res. 2016, 40, 2271–2282. [Google Scholar] [CrossRef]
- Vitiello, M.V. Sleep, alcohol, and alcohol abuse. Addict. Biol. 1997, 2, 151–158. [Google Scholar] [CrossRef]
- Laniepce, A.; Cabé, N.; André, C.; Bertran, F.; Boudehent, C.; Lahbairi, N.; Maillard, A.; Mary, A.; Segobin, S.; Vabret, F.; et al. The effect of alcohol withdrawal syndrome severity on sleep, brain and cognition. Brain Commun. 2020, 2, fcaa123. [Google Scholar] [CrossRef] [PubMed]
- Brower, K.J. Insomnia, alcoholism, and relapse. Sleep Med. Rev. 2003, 7, 523–539. [Google Scholar] [CrossRef]
- Bazzo, S.; Battistella, G.; Riscica, P.; Moino, G.; Dal Pozzo, G.; Bottarel, M.; Geromel, M.; Czerwinsky, L. Reliability of an Italian self-report version of the AUDIT-C questionnaire used to estimate alcohol consumption by pregnant women in an obstetric setting. Riv. Psychiatr. 2015, 50, 89–94. [Google Scholar]
- Hemiö, K.; Lindström, J.; Peltonen, M.; Härmä, M.; Viitasalo, K.; Puttonen, S. The association of work stress and night work with nutrient intake—A prospective cohort study. Scand. J. Work Environ. Health 2020, 46, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Boucsein, W.; Ottmann, W. Psychophysiological stress effects from the combination of night work and noise. Biol. Psychol. 1996, 42, 301–322. [Google Scholar] [CrossRef]
- Lichtenstein, M.B.; Malkenes, M.; Sibbersen, C.; Hinze, C.J. Work dependence is associated with increased stress and reduced quality of life: Validation of the Bergen Work Dependence Scale in Danish. Scand. J. Psychol. 2019, 60, 145–151. [Google Scholar] [CrossRef]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. Oxidative Stress Markers among Obstructive Sleep Apnea Patients. Oxid. Med. Cell Longev. 2021, 2021, 9681595. [Google Scholar] [CrossRef]
- Maniaci, A.; Iannella, G.; Cocuzza, S.; Vicini, C.; Magliulo, G.; Ferlito, S.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Nicolai, A.; et al. Oxidative Stress and Inflammation Biomarker Expression in Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.A.; Flaherty, J.A.; Rospenda, M. Perceived experiences of workplace harassment and alcohol problems among physicians: Expanding the stress/alienation paradigm. Addiction 1996, 91, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Costa, G. Shift work and health: Current problems and preventive actions. Saf. Health Work 2010, 1, 112–123. [Google Scholar] [CrossRef]
- Cannizzaro, E.; Ramaci, T.; Cirrincione, L.; Plescia, F. Occupational stress, pathophysiological mechanisms and influence of environmental genetic factors. Int. J. Environ. Res. Public Health 2019, 16, 4031. [Google Scholar] [CrossRef]
- Powers, R.J.; Kutash, I.L. Stress and alcohol. Int. J. Addict. 1985, 20, 461–482. [Google Scholar] [CrossRef] [PubMed]
- Kersey, K.; Lyons, A.C.; Hutton, F. Alcohol and drinking within the lives of midlife women: A meta-study systematic review. Int. J. Drug Policy 2021, 99, 103453. [Google Scholar] [CrossRef]
- Sayette, M.A. Does drinking reduce stress? Alcohol Res. Health 1999, 23, 250–255. [Google Scholar] [PubMed]
- Schepis, T.S.; Rao, U.; Yadav, H.; Adinoff, B. The limbic-hypothalamic-pituitary-adrenal axis and the development of alcohol use disorders in youth. Alcohol. Clin. Exp. Res. 2011, 35, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Majewska, M.D. HPA axis and stimulant dependence: An enigmatic relationship. Psychoneuroendocrinology 2002, 27, 5–12. [Google Scholar] [CrossRef]
- Cannizzaro, C.; La Barbera, M.; Plescia, F.; Cacace, S.; Tringali, G. Ethanol modulates corticotropin-releasing hormone release from the rat hypothalamus: Does acetaldehyde play a role? Alcohol. Clin. Exp. Res. 2010, 34, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, A.F. Stress signaling pathways impairing prefrontal cortex structure and function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar] [CrossRef]
- Herman, J.P.; Ostrander, M.M.; Mueller, N.K.; Figueiredo, H. Limbic system mechanisms of stress regulation: Hypothalamic-pituitary-adrenocortical axis. Adv. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 1201–1213. [Google Scholar] [CrossRef]
- Roozendaal, B.; Quirarte, G.L.; McGaugh, J.L. Glucocorticoids interact with the basolateral amygdala β-adrenoceptor-cAMP/cAMP/PKA receptor system in influencing memory consolidation. Eur. J. Neurosci. 2002, 15, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Belujon, P.; Grace, A.A. Regulation of dopamine system reactivity and its adaptive and pathological response to stress. Proc. R. Soc. Lond. B Biol. Sci. 2015, 282, 20142516. [Google Scholar]
- Schwabe, L.; Dickinson, A.; Wolf, O.T. Stress, habits, and drug addiction: A psychoneuroendocrinological perspective. Exp. Clin. Psychopharmacol. 2011, 19, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Blaine, S.K.; Milivojevic, V.; Fox, H.; Sinha, R. Effects of alcohol on stress pathways: Impact on Craving and risk of relapse. Can. J. Psychiatry 2016, 61, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.D.; Rivier, C.L.; Lee, S.Y. Adolescent alcohol exposure alters central brain circuits known to regulate the stress response. Neuroscience 2011, 182, 162–168. [Google Scholar] [CrossRef]
- McEwen, B.S. Stress, adaptation, and disease: Allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Le Moal, M. Plasticity of the reward neurocircuitry and the ‘dark side’ of drug addiction. Nat. Neurosci. 2005, 8, 1442–1444. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R. How does stress increase the risk of drug abuse and relapse? Psychopharmacology 2001, 158, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R. Chronic stress, drug use, and vulnerability to addiction. Ann. N. Y. Acad. Sci. 2008, 1141, 105–130. [Google Scholar] [CrossRef]
- Sinha, R. Risk factors for substance use, abuse and dependence: Stress. In Encyclopedia of Drugs, Alcohol, and Addictive Behaviors, 3rd ed.; Kranzler, H., Korsmeyer, P., Eds.; MacMillan Reference: New York, NY, USA, 2008. [Google Scholar]
- Lovallo, W.R. Cortisol secretion patterns in addiction and the risk of addiction. Int. J. Psychophysiol. 2006, 59, 195–202. [Google Scholar] [CrossRef]
- Heilig, M.; He, M.; Crabbe, J.C.; Becker, H.C. Acute abstinence, protracted abstinence, and negative affect in alcoholism: Are they related? Biol. Addict. 2010, 15, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Ferri, P.; Guadi, M.; Marcheselli, L.; Balduzzi, S.; Magnani, D.; Di Lorenzo, R. The impact of shift work on the psychological and physical health of nurses in a general hospital: A comparison between rotating night shifts and day shifts. Risk Manag. Healthc. Policy 2016, 9, 203–211. [Google Scholar] [CrossRef] [PubMed]
- McVicar, A. Analysis of common antecedents of nurses’ job stress and job satisfaction (2000–2013) using the demand- and resource-based stress model. J. Nurs. Manag. 2016, 24, E112–E136. [Google Scholar] [CrossRef] [PubMed]
- Haario, P.; Rahkonen, O.; Laaksonen, M.; Lahelma, E.; Lallukka, T. Bidirectional associations between insomnia symptoms and unhealthy behaviors. J. Sleep Res. 2013, 22, 89–95. [Google Scholar] [CrossRef]
- Roehrs, T.; Papineau, K.; Rosenthal, L.; Roth, T. Ethanol as a hypnotic in insomniacs: Self-administration and effects on sleep and mood. Neuropsychopharmacology 1999, 20, 279–286. [Google Scholar] [CrossRef]
- Burke, C.K.; Peirce, J.M.; Kidorf, M.S.; Neubauer, D.; Punjabi, N.M.; Stoller, K.B.; Hursh, S.; Brooner, R.K. Sleep problems reported by patients entering treatment with opioid agonists. J. Subst. Abuse Treat. 2008, 35, 328–333. [Google Scholar] [CrossRef]
- Johanson, C.E.; Roehrs, T.; Schuh, K.; Warbasse, L. The effects of cocaine on mood and sleep in cocaine-dependent males. Exp. Clin. Psychopharmacol. 1999, 7, 338–346. [Google Scholar] [CrossRef]
- He, S.; Hasler, B.P.; Chakravorty, S. Alcohol and sleep problems. Curr. Opin. Psychol. 2019, 30, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Uchimura, N. [Sleep disorders related to alcohol dependence]. Seishin Shinkeigaku Zasshi. 2010, 112, 787–792. [Google Scholar] [PubMed]
- Richardson, G.S.; Miner, J.D.; Czeisler, C.A. Impaired driving performance in shift workers: The role of the circadian system in a multifactorial model. Alcohol Drugs Driv. 1989, 5–6, 265–273. [Google Scholar]
- Gold, D.R.; Rogacz, S.; Bock, N.; Tosteson, T.D.; Baum, T.M.; Speizer, F.E.; Czeisler, C.A. Rotating shift work, sleep, and sleep-related accidents in hospital nurses. Am. J. Public Health 1992, 82, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Knauth, P.; Hornberger, S. Preventive and compensatory measures for shift workers. Occup. Med. 2003, 53, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Dorrian, J.; Paterson, J.; Dawson, D.; Pincombe, J.; Grech, C.; Rogers, A.E. Sleep, stress and compensatory behaviours in Australian nurses and midwives. Rev. Saude Publica 2011, 45, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.; Roth, T. Sleep, drowsiness, and alcohol use. Alcohol Res. Health 2001, 25, 101–109. [Google Scholar] [PubMed]
- Chung, Y.; Kim, H.; Koh, D.H.; Park, J.H.; Yoon, S. Relationship Between Shift Intensity and Insomnia Among Hospital Nurses in Korea: A Cross-sectional Study. J. Prev. Med. Public Health 2021, 54, 46–54. [Google Scholar] [CrossRef]
- Koob, G.F. Drug addiction: The yin and yang of hedonic homeostasis. Neuron 1996, 16, 893–896. [Google Scholar] [CrossRef][Green Version]
- Jones, K.A.; Tamm, J.A.; Craig, D.A.; Yao, W.; Panic, R. Signal transduction by GABA(B) receptor heterodimers. Neuropsychopharmacology 2000, 23 (Suppl. 4), S41–S49. [Google Scholar] [CrossRef]
- Krystal, J.H.; Staley, J.; Mason, G.; Petrakis, I.L.; Kaufman, J.; Harris, R.A.; Gelernter, J.; Lappalainen, J. Gamma-aminobutyric acid type A receptors and alcoholism: Intoxication, dependence, vulnerability, and treatment. Arch. Gen. Psychiatry 2006, 63, 957–968. [Google Scholar] [CrossRef]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef]
- Brown, C.L.; Gibbons, L.E.; Kennison, R.F.; Robitaille, A.; Lindwall, M.; Mitchell, M.B.; Shirk, S.D.; Atri, A.; Cimino, C.R.; Benitez, R.; et al. Social activity and cognitive functioning over time: A coordinated analysis of four longitudinal studies. J. Aging Res. 2012, 2012, 287438. [Google Scholar] [CrossRef]
- Gent, T.C.; Bandarabadi, M.; Herrera, C.G.; Adamantidis, A.R. Dual thalamic control of sleep and wakefulness. Nat. Neurosci. 2018, 21, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Banks, S.; Catcheside, P.; Lack, L.; Grunstein, R.R.; McEvoy, R.D. Low alcohol levels impair driving simulator performance and reduce perception of crash risk in partially sleep deprived subjects. Sleep 2004, 27, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, M.M.; Sharma, R.; Sahota, P. Alcohol disrupts sleep homeostasis. Alcohol 2015, 49, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Arnedt, J.T.; Rohsenow, D.J.; Almeida, A.B.; Hunt, S.K.; Gokhale, M.; Gottlieb, D.J.; Howland, J. Sleep after alcohol intoxication in healthy, young adults: Effects of sex and family history of alcoholism. Alcohol Clin. Exp. Res. 2011, 35, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Caetano, R.; Clark, C.L.; Greenfield, T.K. Prevalence, trends, and incidence of alcohol withdrawal symptoms: Analysis of general population and clinical samples. Alcohol Health Res. World 1998, 22, 73–79. [Google Scholar] [PubMed]
- Foster, J.H.; Marshall, E.J.; Peters, T.J. Predictors of relapse to heavy drinking in alcohol-dependent individuals after alcohol detoxification—The role of measures of quality of life, ethnicity, social class, cigarette and drug use. Addict. Biol. 1998, 3, 333–343. [Google Scholar] [CrossRef]
- Brower, K.J.; Aldrich, M.S.; Robinson, E.A.; Zucker, R.A.; Greden, J.F. Insomnia, self-medication, and relapse in alcoholism. Am. J. Psychiatry 2001, 158, 399–404. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Percentage | Media | S.D | Min | Med | Max | |
|---|---|---|---|---|---|---|---|
| na | 222 | 56.6% | |||||
| Age | 45.16 | 11.77 | 24 | 45 | 67 | ||
| Height (cm) | 1.74 | 0.079 | 1.6 | 1.75 | 1.91 | ||
| Weight (kg) | 76.9 | 9.68 | 59 | 79 | 100 | ||
| BMI | 25.25 | 3.02 | 18.11 | 25.29 | 31.9 | ||
| Female | |||||||
| na | 170 | 44.4% | |||||
| Age | 44.94 | 11.29 | 27 | 45 | 63 | ||
| Height (cm) | 1.68 | 0.0635 | 1.58 | 1.68 | 1.83 | ||
| Weight (kg) | 67.6 | 7.65 | 50 | 69 | 82 | ||
| BMI | 23.67 | 2.39 | 50 | 69 | 29.73 |
| Daily Workers | Night Workers | |||
|---|---|---|---|---|
| n° | % | n° | % | |
| 196 | 100 | 196 | 100 | |
| Workers reporting alcohol intake | 136 | 69.4 | 162 | 82.7 |
| Workers who drink occasionally | 121 | 62.7 | 129 | 65.8 |
| Workers who drink weekly | 12 | 6.1 | 18 | 9.2 |
| Workers who drink every day | 3 | 1.5 | 16 | 8.2 |
| Workers with harmful drinking behaviour | 25 | 12.8 | 66 | 33.7 |
| Workers who engage in binge drinking | 4 | 2 | 15 | 7.7 |
| Daily Workers | Night Workers | |||
|---|---|---|---|---|
| n° | % | n° | % | |
| 196 | 100 | 196 | 100 | |
| No clinically significant insomnia | 167 | 85.2 | 151 | 77 |
| Subthreshold insomnia | 15 | 7.7 | 29 | 14.8 |
| Moderate clinical insomnia | 12 | 6.1 | 16 | 8.2 |
| Severe clinical insomnia | 1 | 0.51 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plescia, F.; Cirrincione, L.; Martorana, D.; Ledda, C.; Rapisarda, V.; Castelli, V.; Martines, F.; Vinnikov, D.; Cannizzaro, E. Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers. Int. J. Environ. Res. Public Health 2021, 18, 13196. https://doi.org/10.3390/ijerph182413196
Plescia F, Cirrincione L, Martorana D, Ledda C, Rapisarda V, Castelli V, Martines F, Vinnikov D, Cannizzaro E. Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers. International Journal of Environmental Research and Public Health. 2021; 18(24):13196. https://doi.org/10.3390/ijerph182413196
Chicago/Turabian StylePlescia, Fulvio, Luigi Cirrincione, Daniela Martorana, Caterina Ledda, Venerando Rapisarda, Valentina Castelli, Francesco Martines, Denis Vinnikov, and Emanuele Cannizzaro. 2021. "Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers" International Journal of Environmental Research and Public Health 18, no. 24: 13196. https://doi.org/10.3390/ijerph182413196
APA StylePlescia, F., Cirrincione, L., Martorana, D., Ledda, C., Rapisarda, V., Castelli, V., Martines, F., Vinnikov, D., & Cannizzaro, E. (2021). Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers. International Journal of Environmental Research and Public Health, 18(24), 13196. https://doi.org/10.3390/ijerph182413196