
Adequacy of Existing Surveillance Systems to Monitor Racism, Social Stigma and COVID Inequities: A Detailed Assessment and Recommendations


 , , ,
, , ,
Abstract
:1. Introduction
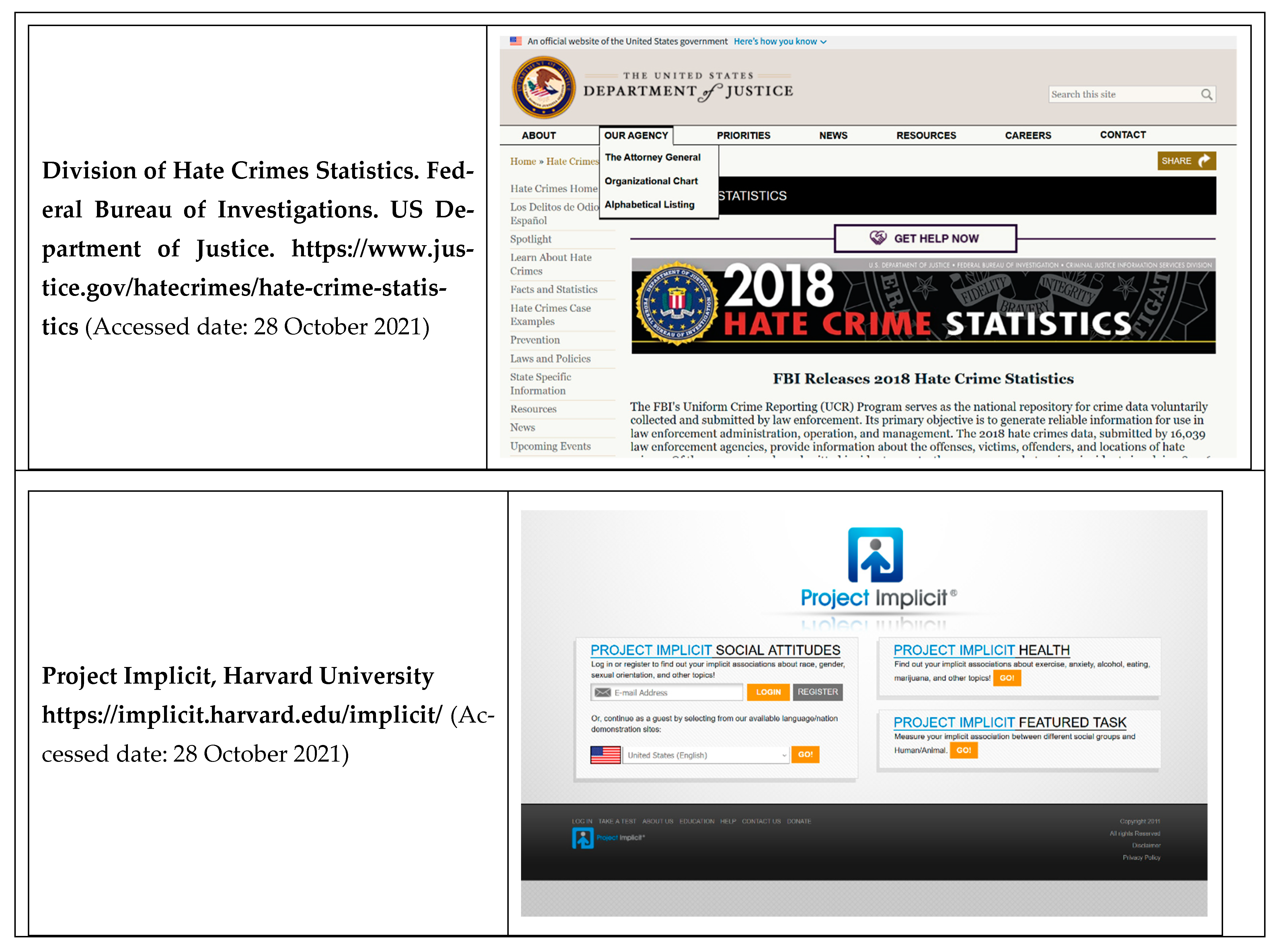
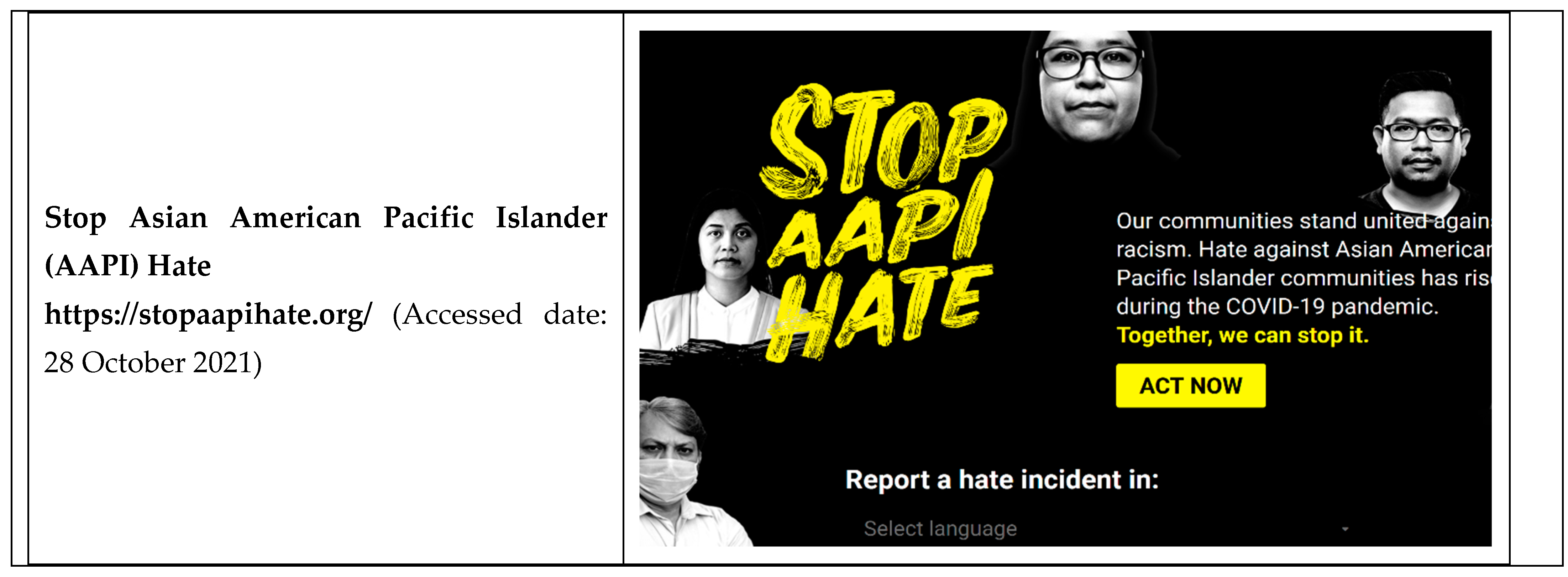
- Hate Crimes, which have increased among Asian populations, in particular, during the COVID pandemic. Annual reports are issued by the US Federal Bureau of Investigations (FBI) Hate Crimes Division. They summarize racist targeting of individuals and serve as an indicator of racialized social stigma.
- Housing Discrimination, which may occur on the basis of race, ethnicity or other characteristics, can increase social vulnerability and exacerbate adherence with COVID guidelines. National data are available from Home Mortgage Disclosure Act reports.
- Residential segregation, which is a key measure of structural racism and estimates the nature and pervasiveness of social exclusion that Black, Indigenous and People of Color groups experience. The indices available via the US Census provide objective data on the amount of racial exclusion in a place, which affects access to care and exposure to hazards.
2. Materials and Methods
2.1. Research Purpose and Hypotheses
2.2. Methods
3. Results
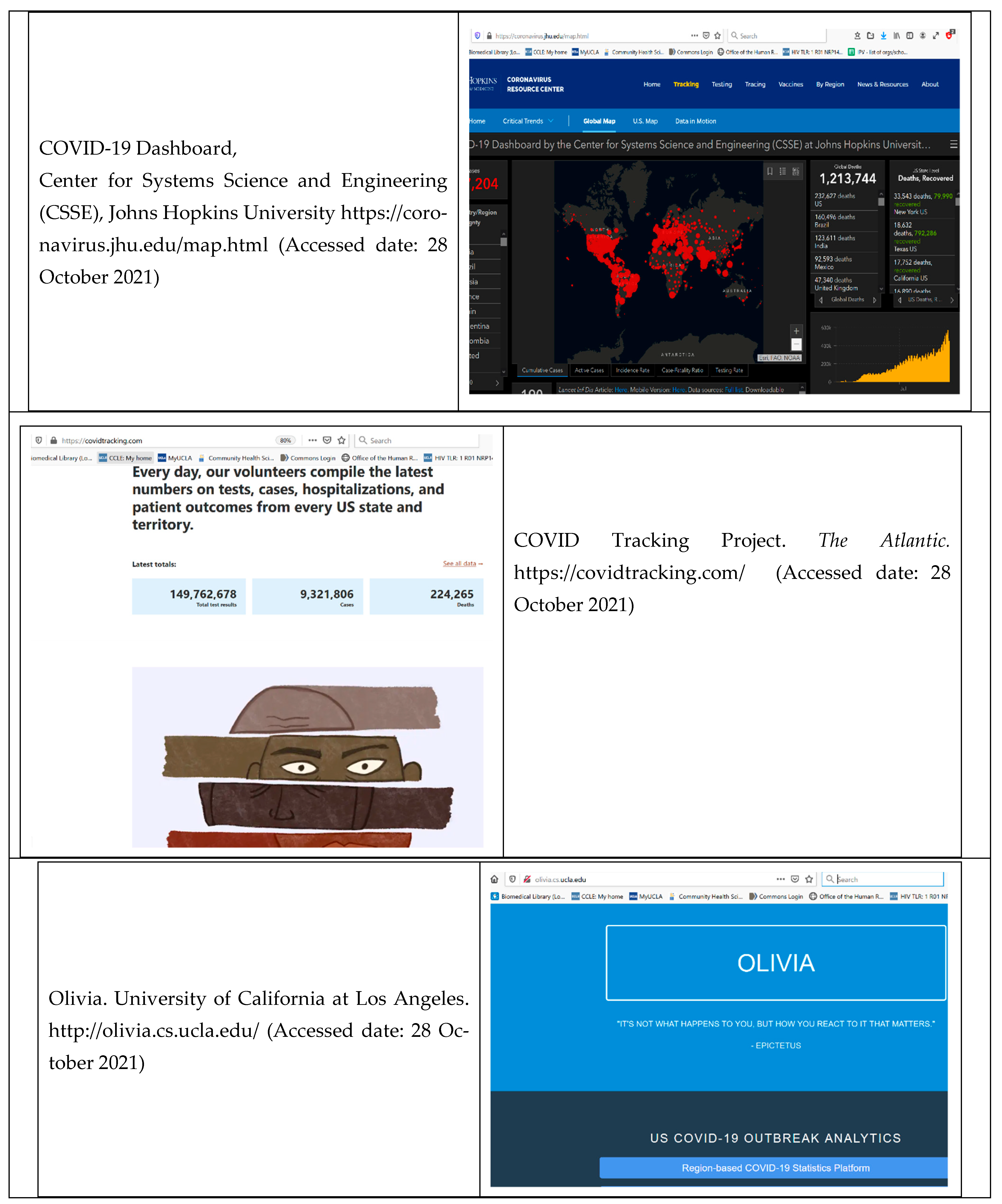
3.1. COVID-19 Surveillance Systems
3.2. Other Public-Health Surveillance Systems
3.3. Systems Tracking Racism and Related Social Stigma
4. Discussion
4.1. Overall Discussion
4.2. Implications and Future Directions
4.3. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jones, C.P. Systems of Power, Axes of Inequity: Parallels, intersections, braiding the strands. Med. Care 2014, 52, S71–S75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonilla-Silva, E. Racism without Racists: Colorblind Racism and the Persistence of Racial Inequality in the United States; Rowman & Littlefield Publishers: Lanham, MD, USA, 2006; p. 277. [Google Scholar]
- Krieger, N. Does racism harm health? Did child abuse exist before 1962? On explicit questions, critical science, and current controversies: An ecosocial perspective. Am. J. Public Health 2008, 98, S20–S25. [Google Scholar] [CrossRef] [PubMed]
- Herek, G.M. Hate crimes and stigma-related experiences among sexual minority adults in the United States: Prevalence estimates from a national probability sample. J. Interpers. Violence 2009, 24, 54–74. [Google Scholar] [CrossRef] [PubMed]
- Herek, G.M.; Capitanio, J.P.; Widaman, K.F. Stigma, social risk, and health policy: Public attitudes toward HIV surveillance policies and the social construction of illness. Health Psychol. 2003, 22, 533–540. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, L.M. Stigmatization, HIV/AIDS, and communities of color: Exploring response to human service facilities. Health Place 1997, 3, 187–199. [Google Scholar] [CrossRef]
- Bailey, Z.; Barber, S.; Robinson, W.; Slaughter, J.; Ford, C.L.; Sealey-Jefferson, S. Racism in the Time of COVID; Interdisciplinary Association of Public Health Sciences (IAPHS), Ed.; 2020; Volume 2020, Available online: https://iaphs.org/racism-in-the-time-of-covid-19/ (accessed on 28 October 2021).
- Nguyen, T.T.; Criss, S.; Dwivedi, P.; Huang, D.; Keralis, J.; Hsu, E.; Phan, L.; Nguyen, L.H.; Yardi, I.; Glymour, M.M.; et al. Exploring U.S. Shifts in Anti-Asian Sentiment with the Emergence of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 7032. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Gee, G.C.; Bahiru, E.; Yang, E.H.; Hsu, J.J. Asian-Americans and Pacific Islanders in COVID-19: Emerging Disparities Amid Discrimination. J. Gen. Intern. Med. 2020, 35, 3685–3688. [Google Scholar] [CrossRef]
- Ford, C.L.; Airhihenbuwa, C.O. Commentary: Just What is Critical Race Theory and What’s it Doing in a Progressive Field like Public Health? Ethn. Dis. 2018, 28, 223–230. [Google Scholar] [CrossRef]
- Ford, C.L.; Airhihenbuwa, C.O. The public health critical race methodology: Praxis for antiracism research. Soc. Sci. Med. 2010, 71, 1390–1398. [Google Scholar] [CrossRef]
- Ford, C.L.; Airhihenbuwa, C.O. Critical Race Theory, race equity, and public health: Toward antiracism praxis. Am. J. Public Health 2010, 100, S30–S35. [Google Scholar] [CrossRef]
- Planey, A.M. Chandra L. Ford, Derek M. Griffith, Marino A. Bruce, Keon L. Gilbert 2019. Racism: Science & Tools for the Public Health Professional. Washington, DC: American Public Health Association Press, 2019. World Med. Health Policy 2020, 12, 545–547. [Google Scholar] [CrossRef]
- National Academies of Sciences Engineering and Medicine. Committee on Community-Based Solutions to Promote Health Equity in the United States. In Communities in Action: Pathways to Health Equity; National Academies Press (US): Washington, DC, USA, 2017. [Google Scholar]
- Bowleg, L.; Fitz, C.C.; Burkholder, G.J.; Massie, J.S.; Wahome, R.; Teti, M.; Malebranche, D.J.; Tschann, J.M. Racial discrimination and posttraumatic stress symptoms as pathways to sexual HIV risk behaviors among urban Black heterosexual men. AIDS Care 2014, 26, 1050–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, R. Assessing risk, automating racism. Science 2019, 366, 421–422. [Google Scholar] [CrossRef] [PubMed]
- Morey, B.; Chang, R.C.; Thomas, K.B.; Tulua; Penaia, C.; Tran, V.D.; Pierson, N.; Greer, J.C.; Bydalek, M.; Ponce, N. No Equity without Data Equity: Data Reporting Gaps for Native Hawaiians and Pacific Islanders as Structural Racism. J. Health Politics Policy Law 2021. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Public Health Surveillance and Informatics Program Office. BRFSS 2010 Survey Data and Documentation. Behavioral Risk Factor Surveillance System 2010. Available online: http://www.cdc.gov/brfss/annual_data/annual_2010.htm (accessed on 27 January 2015).
- Ford, C.L.; Skrine Jeffers, K. Critical Race Theory’s Anti-racism Approaches: Moving from the Ivory Tower to the Frontlines of Public Health. In Racism: Science and Tools for the Public Health Professional; Ford, C.L., Griffith, D.M., Bruce, M., Gilbert, K., Eds.; American Public Health Association: Washington, DC, USA, 2019. [Google Scholar]
- Boyd, R.W.; Lindo, E.G.; Weeks, L.D.; McLemore, M.R. On Racism: A New Standard For Publishing On Racial Health Inequities. In Health Affairs Blog; Affairs, H., Ed.; Health Affairs: Washington, DC, USA, 2020. [Google Scholar]
- Gee, G.C.; Ford, C.L. Structural racism and health inequities: Old issues, new directions. Du Bois Rev. 2011, 8, 115–132. [Google Scholar] [CrossRef] [Green Version]
- Ford, C.L. Hate crimes in the United States. In Racism: Science and Tools for the Public Health Professional; Ford, C.L., Griffith, D.M., Bruce, M., Gilbert, K., Eds.; American Public Health Association: Washington, DC, USA, 2019. [Google Scholar]
- Nosek, B.A.; Greenwald, A.G.; Banaji, M.R. Understanding and using the Implicit Association Test: II. Method variables and construct validity. Personal. Soc. Psychol. Bull. 2005, 31, 166–180. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, A.G.; Banaji, M.R. Understanding and using the implicit association test: I. An improved scoring algorithm. J. Personal. Soc. Psychol. 2003, 85, 197–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stangl, A.L.; Earnshaw, V.A.; Logie, C.H.; van Brakel, W.; Simbayi, L.C.; Barré, I.; Dovidio, J.F. The Health Stigma and Discrimination Framework: A global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. 2019, 17, 31. [Google Scholar] [CrossRef]
- Treichler, P.A. AIDS, Africa, and cultural theory. Transition 1991, 51, 86–103. [Google Scholar] [CrossRef]
- Benjamin, R. (Ed.) Captivating Technology: Race, Carceral Technoscience, and Liberatory Imagination; Duke University Press: Durham, NC, USA, 2019; p. 416. [Google Scholar]
- Noble, S.U. Algorithms of Oppression: How Search Engines Reinforce Racism; NYU Press: New York, NY, USA, 2018; p. 256. [Google Scholar]
- Ford, C.L.; Takahashi, L.M.; Chandanabhumma, P.P.; Ruiz, M.E.; Cunningham, W.E. Anti-Racism Methods for Big Data Research: Lessons Learned from the HIV Testing, Linkage, & Retention in Care (HIV TLR) Study. Ethn. Dis. 2018, 28, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.C. Pandemic Ethics Dashboard. Available online: https://pandemicethics.org/about/ (accessed on 29 October 2020).
- Samari, G.; Alcala, H.E.; Sharif, M.Z. Islamophobia, Health, and Public Health: A Systematic Literature Review. Am. J. Public Health 2018, 108, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Heipke, C. Crowdsourcing geospatial data. ISPRS J. Photogramm. Remote Sens. 2010, 65, 550–557. [Google Scholar] [CrossRef]
- Grove, N.S. The cartographic ambiguities of HarassMap: Crowdmapping security and sexual violence in Egypt. Secur. Dialogue 2015, 46, 345–364. [Google Scholar] [CrossRef]
- Liu, Y.; Guo, B.; Chen, C.; Du, H.; Yu, Z.; Zhang, D.; Ma, H. FooDNet: Toward an optimized food delivery network based on spatial crowdsourcing. IEEE Trans. Mob. Comput. 2018, 18, 1288–1301. [Google Scholar] [CrossRef]
- Jones, C.P. Confronting institutionalized racism. Phylon. Clark Atlanta Univ. Rev. Race Cult. 2002, 50, 7–22. [Google Scholar] [CrossRef]
- Jones, C.P.; Truman, B.I.; Elam-Evans, L.D.; Jones, C.A.; Jones, C.Y.; Jiles, R.; Rumisha, S.F.; Perry, G.S. Using “socially assigned race” to probe white advantages in health status. Ethn. Dis. 2008, 18, 496–504. [Google Scholar] [PubMed]
- Ford, C.L.; Harawa, N.T. A new conceptualization of ethnicity for social epidemiologic and health equity research. Soc. Sci. Med. 2010, 71, 251–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office of Management and Budget. Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. Fed. Regist. 1997, 62, 58781–58790. [Google Scholar]
- Southall, A. Scrutiny of Social-Distance Policing as 35 of 40 Arrested Are Black; New York Times: New York, NY, USA, 2020. [Google Scholar]
- Eubanks, V. Automating Inequality: How High-Tech Tools Profile, Police, and Punish the Poor; St. Martin’s Press: New York, NY, USA, 2018; p. 288. [Google Scholar]
- Choi, B.C. The past, present, and future of public health surveillance. Scientifica 2012, 2012, 875253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuberi, T.; Bonilla-Silva, E. (Eds.) White Logic., White Methods: Racism and Methodology; Rowman & Littlefield Publishers: Lanham, MD, USA, 2008; p. 424. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Key Considerations |
|---|---|
| For Surveillance in General | |
| Usefulness | To what extent does the system support the achievement of the stated goals? |
| Timeliness | How long does it take for the system to acquire needed data and make them available? |
| Flexibility | To what extent can the system adapt to new circumstances or needs? |
| Simplicity | How easy is it for users to operate the system? |
| Data Quality * | How complete and accurate are the data fields in the reports the system receives? How reliable are the data? |
| Informed by Public Health Critical Race Praxis | |
| Race/ethnicity data | Which race/ethnicity data are included? To what extent do they support the achievement of Project REFOCUS aims? |
| Stigma measures | What valid measures of stigma are included? |
| Racism measures | What relevant measures of racism are included? |
| Surveillance Implications | To what extent might the system contribute to harm of racial/ethnic minority and vulnerable populations or aid community-originated surveillance projects? |
| COVID-19 Outcomes a | Measures | Race/Ethnicity b | Updates | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| System Name | T | C | H | V | D | O | Stigma | Racism | W | B | L | A | NA/AN | H/PI | O | N/A | |
| 1point3acres | x | x | x | x | x | x | x | x | x | x | Daily | ||||||
| Olivia | x | x | -- | x | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | x | Weekly | |
| JHU COVID-19 Dashboard | x | x | x | x | -- | -- | -- | -- | -- | -- | -- | -- | -- | x | Daily | ||
| COVID-19 Case Surveillance | ? | x | x | ? | x | x | -- | -- | x | x | x | x | x | x | x | x | Daily |
| COVID Tracking Project | x | x | x | -- | x | -- | -- | -- | x | x | x | x | x | x | x | x | Daily |
| LA County Dept. of Public Health | x | x | x | x | x | x | -- | -- | x | x | x | x | x | x | x | x | Daily |
| COVID Behind Bars project | x | x | x | x | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | Daily | ||
| CDC COVID Data Tracker | x | -- | x | x | -- | -- | x | x | x | x | x | x | x | x | Daily | ||
| NC DHHS COVID-19 Response | x | x | x | x | x | x | x | x | x | x | x | x | Weekly | ||||
| Census COVID Data | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | ? |
| Google COVID-19 Public Forecaster | ? | x | ? | ? | x | x | -- | -- | ? | ? | ? | ? | ? | ? | ? | ? | Continuous |
| National Vital Statistics Program | x | x | x | x | x | x | x | x | 4 November | ||||||||
| System | Race/Ethnicity a | Measures | COVID-19 Outcomes b | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| W | B | L | A | NA/AN | H/PI | O | DK | Stigma | Racism | T | C | H | V | D | O | Updates | |
| National Longitudinal Study of Adolescent to Adult Health | x | x | x | x | x | x | x | x | x | x | -- | -- | -- | -- | -- | -- | Annual |
| Amerispeak/NORC General Social Survey | x | x | x | x | ? | ? | ? | x | x | x | -- | -- | -- | -- | -- | x | Biennial |
| California Health Interview Survey | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x | Monthly, Annual |
| CDC BRFSS | x | x | x | ? | ? | ? | x | x | x | -- | -- | -- | -- | -- | Annual | ||
| CDC Influenza Surveys | -- | -- | -- | -- | -- | -- | -- | x | -- | -- | x | x | ? | -- | x | x | Varies |
| CDC INFO Query | x | x | x | x | x | x | x | x * | x | -- | -- | -- | -- | -- | x | Continuous | |
| Current Population Survey | x | x | x | x | x | x | x | x | x | x | -- | x | -- | -- | x | -- | Monthly, Annual |
| National Syndromic Surveillance Program | x | x | x | x | x | x | x | x | x | x | x | x | x | x | Continuous | ||
| Youth Risk Behavior Surveillance Survey | x | x | x | x | x | x | x | x | x | x | x | x | x | Varies, Continuous | |||
| System Name | Updates | COVID-19 Outcomes a [1] | Race/Ethnicity Data b | Key Measures | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | C | H | V | D | O/DK | W | B | L | A | NA/AN | H/PI | O | N/DK | Stigma | Racism | ||
| Decennial Census | Decade | x | x | x | x | x | x | x | x | x | x | x | x | x | x | ||
| American Community Survey | Annual | x | x | x | x | x | x | x | x | ||||||||
| Home Mortgage Disclosure Act | Varies, Quarterly, Annual | x | x | x | x | x | x | x | x | ||||||||
| Project Implicit | n/a | x | x | x | x | x | x | x | |||||||||
| Continuous | x | x | ? | ? | x | x | x | x | |||||||||
| Continuous | x | x | x | ||||||||||||||
| FBI Hate Crimes | Annual | x | x | x | x | x | x | x | x | x | |||||||
| Equal Opportunity Employment Commission | Annual | x | x | x | x | x | x | x | |||||||||
| Pew Research Center | Varies | x | x | x | x | x | x | x | x | ||||||||
| NORC General Social Survey | Varies | x | x | x | x | x | x | ||||||||||
| STOP AAPI Hate | Continuous | x | x | x | x | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ford, C.L.; Amani, B.; Harawa, N.T.; Akee, R.; Gee, G.C.; Sarrafzadeh, M.; Abotsi-Kowu, C.; Fazeli, S.; Le, C.; Nwankwo, E.; et al. Adequacy of Existing Surveillance Systems to Monitor Racism, Social Stigma and COVID Inequities: A Detailed Assessment and Recommendations. Int. J. Environ. Res. Public Health 2021, 18, 13099. https://doi.org/10.3390/ijerph182413099
Ford CL, Amani B, Harawa NT, Akee R, Gee GC, Sarrafzadeh M, Abotsi-Kowu C, Fazeli S, Le C, Nwankwo E, et al. Adequacy of Existing Surveillance Systems to Monitor Racism, Social Stigma and COVID Inequities: A Detailed Assessment and Recommendations. International Journal of Environmental Research and Public Health. 2021; 18(24):13099. https://doi.org/10.3390/ijerph182413099
Chicago/Turabian StyleFord, Chandra L., Bita Amani, Nina T. Harawa, Randall Akee, Gilbert C. Gee, Majid Sarrafzadeh, Consuela Abotsi-Kowu, Shayan Fazeli, Cindy Le, Ezinne Nwankwo, and et al. 2021. "Adequacy of Existing Surveillance Systems to Monitor Racism, Social Stigma and COVID Inequities: A Detailed Assessment and Recommendations" International Journal of Environmental Research and Public Health 18, no. 24: 13099. https://doi.org/10.3390/ijerph182413099
APA StyleFord, C. L., Amani, B., Harawa, N. T., Akee, R., Gee, G. C., Sarrafzadeh, M., Abotsi-Kowu, C., Fazeli, S., Le, C., Nwankwo, E., Zamanzadeh, D., Ovalle, A., & Ponder, M. L. (2021). Adequacy of Existing Surveillance Systems to Monitor Racism, Social Stigma and COVID Inequities: A Detailed Assessment and Recommendations. International Journal of Environmental Research and Public Health, 18(24), 13099. https://doi.org/10.3390/ijerph182413099