
Childbirths and the Prevalence of Potential Risk Factors for Adverse Perinatal Outcomes among Asylum Seekers in The Netherlands: A Five-Year Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
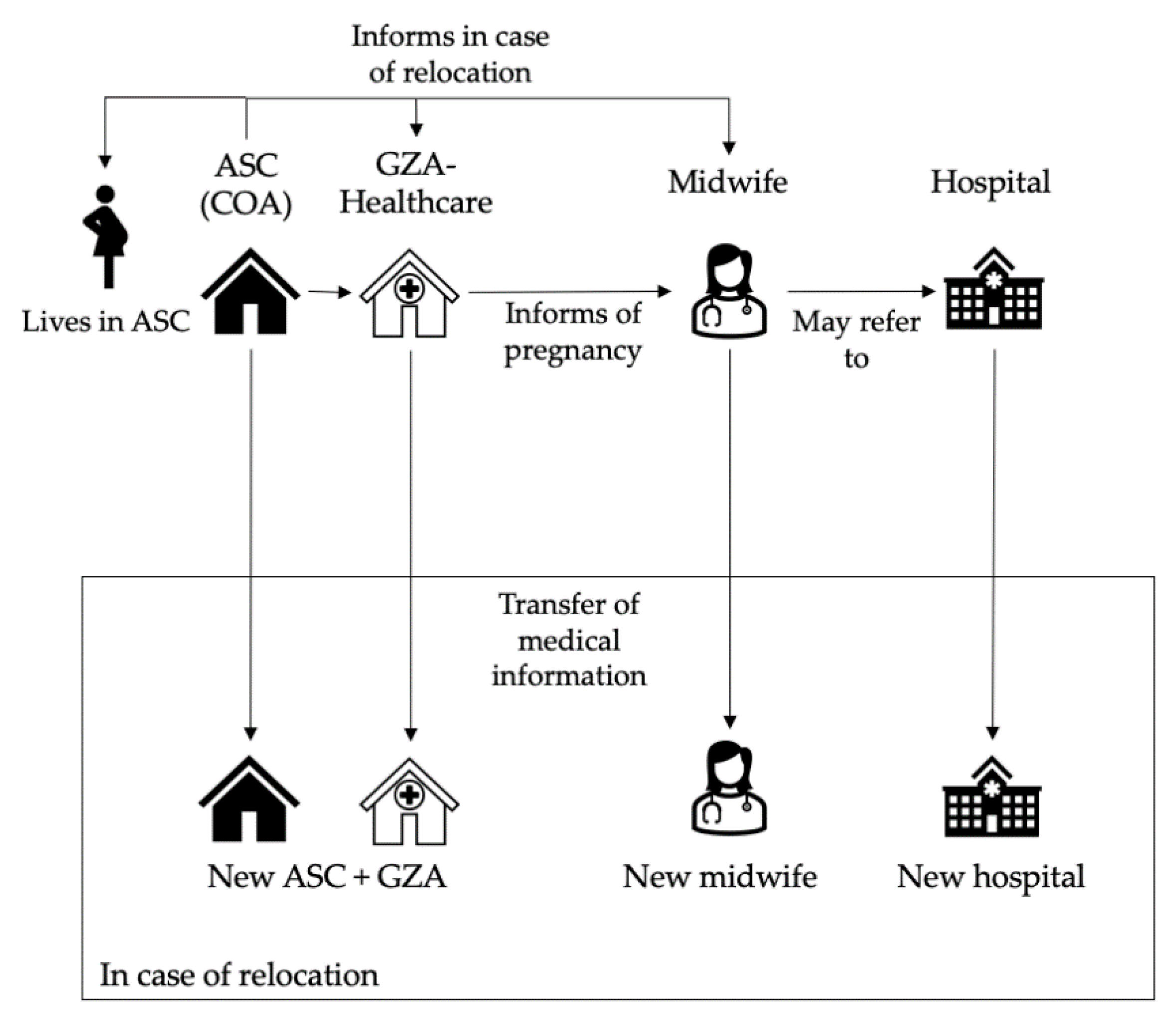
2.2. Healthcare and Perinatal Care for Asylum Seekers
2.3. Study Population
2.4. Data Collection
2.5. Data Processing
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Childbirths and Maternal Characteristics
3.2. Length of Stay and Number of Relocations
3.3. Birthrates and Region of Origin
3.4. Teenage Pregnancies
4. Discussion
4.1. Strengths and Limitations
4.2. Policy and Research Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Year | Number of Births | Person Years of Women Aged 15–49 in ASCs |
|---|---|---|
| 2016 | 778 | 7708 |
| 2017 | 452 | 5412 |
| 2018 | 427 | 5052 |
| 2019 | 652 | 5824 |
| 2020 | 572 | 6198 |
| Total | 2881 | 30,194 |
Appendix B
| Regions of Origin | Countries | Number of Births |
|---|---|---|
| America n = 30 | Brazil Colombia Cuba El Salvador Honduras Nicaragua Suriname Venezuela United States of America | 1 4 5 3 2 1 3 10 1 |
| Asia and Pacific n = 417 | Kazakhstan Kyrgyzstan Uzbekistan China North Korea India Nepal Sri Lanka Bangladesh Indonesia Mongolia Myanmar Thailand Viet Nam Afghanistan Islamic Republic of Iran Pakistan | 2 1 2 32 1 1 1 7 1 1 9 2 1 2 147 165 42 |
| Europe n = 361 | Armenia Azerbaijan Belarus Georgia Russian Federation Turkey Ukraine Austria Germany Italy Latvia Republic of Moldova (the) Romania Albania Bosnia and Herzegovina North Macedonia Serbia Kosovo Yugoslavia Sovjetunie | 23 24 3 19 38 108 19 1 1 1 1 16 1 32 7 17 11 6 25 8 |
| Middle East/North Africa n = 957 | Iraq Israel State of Palestine Jordan Kuwait Lebanon Saudi Arabia Syrian Arab Republic United Arab Emirates Yemen Algeria Egypt Libya Mauritania Morocco Tunisia | 182 4 1 9 4 13 7 620 6 29 4 24 26 1 23 4 |
| East/Horn of Africa n = 528 | Burundi Djibouti Eritrea Ethiopia Kenya Rwanda Somalia Sudan United Republic of Tanzania Uganda | 11 1 236 111 6 3 70 22 5 63 |
| West/Central Africa n = 458 | Burkina Faso Cameroon Côte d’Ivoire Ghana Liberia Guinea Gambia Togo Benin Mali Niger Nigeria Senegal Sierra Leone | 1 6 18 7 4 80 20 1 6 1 2 272 4 36 |
| Southern Africa n = 50 | Angola Democratic Republic of the Congo Madagascar Malawi Zimbabwe | 13 32 2 1 2 |
| Unknown/stateless n = 30 | Unknown Stateless | 28 2 |
References
- Gagnon, A.; Zimbeck, M.; Zeitlin, J. Migration to western industrialised countries and perinatal health: A systematic review. Soc. Sci. Med. 2009, 69, 934–946. [Google Scholar] [CrossRef]
- Akker, T.V.D.; Roosmalen, J.v. Maternal mortality and severe morbidity in a migration perspective. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 32, 26–38. [Google Scholar] [CrossRef]
- Gieles, N.C.; Tankink, J.B.; Van Midde, M.; Düker, J.; Van Der Lans, P.; Wessels, C.M.; Bloemenkamp, K.W.M.; Bonsel, G.; Akker, T.V.D.; Goosen, S.; et al. Maternal and perinatal outcomes of asylum seekers and undocumented migrants in Europe: A systematic review. Eur. J. Public Health 2019, 29, 714–723. [Google Scholar] [CrossRef]
- Heslehurst, N.; Brown, H.; Pemu, A.; Coleman, H.; Rankin, J. Perinatal health outcomes and care among asylum seekers and refugees: A systematic review of systematic reviews. BMC Med. 2018, 16, 89. [Google Scholar] [CrossRef]
- Bozorgmehr, K.; Biddle, L.; Preussler, S.; Mueller, A.; Szecsenyi, J. Differences in pregnancy outcomes and obstetric care between asylum seeking and resident women: A cross-sectional study in a German federal state, 2010–2016. BMC Pregnancy Childbirth 2018, 18, 417. [Google Scholar] [CrossRef]
- Verschuuren, A.E.H.; Postma, I.R.; Riksen, Z.M.; Nott, R.L.; Jong, E.I.F.-D.; Stekelenburg, J. Pregnancy outcomes in asylum seekers in the North of the Netherlands: A retrospective documentary analysis. BMC Pregnancy Childbirth 2020, 20, 320. [Google Scholar] [CrossRef] [PubMed]
- Van Oostrum, I.E.A.; Goosen, S.; Uitenbroek, D.G.; Koppenaal, H.; Stronks, K. Mortality and causes of death among asylum seekers in the Netherlands, 2002-2005. J. Epidemiol. Community Health 2010, 65, 376–383. [Google Scholar] [CrossRef]
- Hanegem, N.v.; Miltenburg, A.S.; Zwart, J.J.; Bloemenkamp, K.W.; Roosmalen, J.v. Severe acute maternal morbidity in asylum seekers: A two-year nationwide cohort study in the Netherlands. Acta Obstet. Gynecol. Scand. 2011, 90, 1010–1016. [Google Scholar] [CrossRef]
- Sturrock, S.; Williams, E.; Dassios, T.; Greenough, A. Antenatal care and perinatal outcomes of asylum seeking women and their infants. J. Perinat. Med. 2021, 49, 619–623. [Google Scholar] [CrossRef]
- Vu, A.; Adam, A.; Wirtz, A.; Pham, K.; Rubenstein, L.; Glass, N.; Beyrer, C.; Singh, S. The Prevalence of Sexual Violence among Female Refugees in Complex Humanitarian Emergencies: A Systematic Review and Meta-analysis. PLoS Curr. 2014, 6. [Google Scholar] [CrossRef]
- Keygnaert, I.; Vettenburg, N.; Temmerman, M. Hidden violence is silent rape: Sexual and gender-based violence in refugees, asylum seekers and undocumented migrants in Belgium and the Netherlands. Cult. Health Sex. 2012, 14, 505–520. [Google Scholar] [CrossRef]
- Asif, S.; Baugh, A.; Jones, N.W. The obstetric care of asylum seekers and refugee women in the UK. Obstet. Gynaecol. 2015, 17, 223–231. [Google Scholar] [CrossRef]
- Briscoe, L.; Lavender, T. Exploring Maternity care for asylum seekers and refugees. Br. J. Midwifery 2009, 17, 17–23. [Google Scholar] [CrossRef]
- Fair, F.; Raben, L.; Watson, H.; Vivilaki, V.; Muijsenbergh, M.V.D.; Soltani, H. Migrant women’s experiences of pregnancy, childbirth and maternity care in European countries: A systematic review. PLoS ONE 2020, 15, e0228378. [Google Scholar]
- Goosen, S.; Hoebe, C.J.P.A.; Waldhober, Q.; Kunst, A.E. High HIV Prevalence among Asylum Seekers Who Gave Birth in the Netherlands: A Nationwide Study Based on Antenatal HIV Tests. PLoS ONE 2015, 10, e0134724. [Google Scholar] [CrossRef]
- Castaner, M.M.; Villadsen, S.F.; Petersen, J.H.; Norredam, M. First perinatal psychiatric episode among refugee and family-reunified immigrant women compared to Danish-born women: A register-based study. Psychiatry Psychiatr Epidemiol. 2021, 56, 2239–2250. [Google Scholar] [CrossRef]
- Fellmeth, G.; Fazel, M.; Plugge, E. Migration and perinatal mental health in women from low- and middle-income countries: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 742–752. [Google Scholar] [CrossRef]
- Racapé, J.; Schoenborn, C.; Sow, M.; Alexander, S.; De Spiegelaere, M. Are all immigrant mothers really at risk of low birth weight and perinatal mortality? The crucial role of socio-economic status. BMC Pregnancy Childbirth 2016, 16, 75. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, A.J.; Zimbeck, M.; Zeitlin, J. Migration and perinatal health surveillance: An international Delphi survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 149, 37–43. [Google Scholar] [CrossRef]
- Bo Brancheorganisatie Geboortezorg; Asylum Seeker Healthcare (’GZA’); Central Agency for the Reception of Asylum Seekers (’COA’); Royal Dutch Organisation of Midwives (KNOV); RMA Healthcare, Dutch Society of Obstetrics and Gynaecology (’NVOG’); Netherlands Association for Community Health Services (GGD GHOR Nederland). Dutch Guideline Perinatal Care for Asylum Seekers (‘Ketenrichtlijn Geboortezorg Asielzoeksters’). Available online: https://www.kennisnetgeboortezorg.nl/nieuws/actualisatie-ketenrichtlijn-geboortezorg-asielzoekers/ (accessed on 19 July 2021).
- Statistics Netherlands. “StatLine”. Open Data. 2021. Available online: https://opendata.cbs.nl/#/CBS/nl/ (accessed on 4 September 2021).
- Goosen, S.; Uitenbroek, D.; Wijsen, C.; Stronks, K. Induced abortions and teenage births among asylum seekers in The Netherlands: Analysis of national surveillance data. J. Epidemiol. Community Health 2009, 63, 528–533. [Google Scholar] [CrossRef][Green Version]
- United Nations Refugee Agency. UNHCR Operations Worldwide. Available online: https://reporting.unhcr.org/operations#:~:text=UNHCR Works in 134 Countries, Reporting Information for 40 Operations (accessed on 13 July 2021).
- Inci, M.G.; Kutschke, N.; Nasser, S.; Alavi, S.; Abels, I.; Kurmeyer, C.; Sehouli, J. Unmet family planning needs among female refugees and asylum seekers in Germany—Is free access to family planning services enough? Results of a cross-sectional study. Reprod. Health 2020, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, O.; Rai, M.; Kemigisha, E. A Systematic Review of Sexual and Reproductive Health Knowledge, Experiences and Access to Services among Refugee, Migrant and Displaced Girls and Young Women in Africa. Int. J. Environ. Res. Public Health 2018, 15, 1583. [Google Scholar] [CrossRef]
- Raben, L.A.D.; Muijsenbergh, M.E.T.C.V.D. Inequity in contraceptive care between refugees and other migrant women?: A retrospective study in Dutch general practice. Fam. Pract. 2018, 35, 468–474. [Google Scholar] [CrossRef]
- Tanabe, M.; Myers, A.; Bhandari, P.; Cornier, N.; Doraiswamy, S.; Krause, S. Family planning in refugee settings: Findings and actions from a multi-country study. Confl. Health 2017, 11, 1–12. [Google Scholar] [CrossRef]
- Immigration and Naturalisation Service (IND). Asylum Trends. Asylum Trends. 2021. Available online: https://ind.nl/en/about-ind/figures-and-publications/Pages/Asylum-Trends.aspx (accessed on 4 September 2021).
- United Nations Population Division. World Population Prospects 2019; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Bongaarts, J. Trends in fertility and fertility preferences in sub-Saharan Africa: The roles of education and family planning programs. Genus 2020, 76, 32. [Google Scholar] [CrossRef]
- Sulekova, L.F.; Spaziante, M.; Vita, S.; Zuccalà, P.; Mazzocato, V.; Spagnolello, O.; Lopalco, M.; Pacifici, L.E.; Bello, L.; Borrazzo, C.; et al. The Pregnancy Outcomes Among Newly Arrived Asylum-Seekers in Italy: Implications of Public Health. J. Immigr. Minor. Health 2020, 23, 232–239. [Google Scholar] [CrossRef]
- Trovato, A.; Reid, A.; Takarinda, K.C.; Montaldo, C.; Decroo, T.; Owiti, P.; Bongiorno, F.; Di Carlo, S. Dangerous crossing: Demographic and clinical features of rescued sea migrants seen in 2014 at an outpatient clinic at Augusta Harbor, Italy. Confl. Health 2016, 10, 14. [Google Scholar] [CrossRef]
- UNITED for Intercultural Action. UNITED List of Refugee Deaths; UNITED for Intercultural Action: Amsterdam, The Netherlands, 2021; Available online: http://unitedagainstrefugeedeaths.eu/wp-content/uploads/2014/06/ListofDeathsActual.pdf (accessed on 19 July 2021).
- Médecins Sans Frontières. Vulnerable Refugees Evicted and Left to Sleep on Streets. Available online: https://www.msf.org/greece-evicts-vulnerable-refugees-leaves-them-streets (accessed on 13 July 2021).
- International Organization for Migration. Fatal Journeys: Tracking Lives Lost during Migration; International Organization for Migratio: Geneva, Switzerland, 2014. [Google Scholar]
- Mason-Jones, A.; Nicholson, P. Structural violence and marginalisation. The sexual and reproductive health experiences of separated young people on the move. A rapid review with relevance to the European humanitarian crisis. Public Health 2018, 158, 156–162. [Google Scholar] [CrossRef]
- De Jong, L.; Pavlova, M.; Winters, M.; Rechel, B. A systematic literature review on the use and outcomes of maternal and child healthcare services by undocumented migrants in Europe. Eur. J. Public Health 2018, 27, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Haelterman, E.; Qvist, R.; Barlow, P.; Alexander, S. Social deprivation and poor access to care as risk factors for severe pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, 25–32. [Google Scholar] [CrossRef]
- Tasa, J.; Holmberg, V.; Sainio, S.; Kankkunen, P.; Vehviläinen-Julkunen, K. Maternal health care utilization and the obstetric outcomes of undocumented women in Finland—A retrospective register-based study. BMC Pregnancy Childbirth 2021, 21, 191. [Google Scholar] [CrossRef]
- Liu, C.; Ahlberg, M.; Hjern, A.; Stephansson, O. Perinatal health of refugee and asylum-seeking women in Sweden 2014–17: A register-based cohort study. Eur. J. Public Health 2019, 29, 1048–1055. [Google Scholar] [CrossRef]
- Munro, K.; Jarvis, C.; Munoz, M.; D’Souza, V.; Graves, L. Undocumented pregnant women: What does the literature tell us? J. Immigr. Minor. Health 2013, 15, 281–291. [Google Scholar] [CrossRef]
- Urindwanayo, D.; Richter, S. Teenage Pregnancy in Refugee Camps: A Narrative Synthesis. J. Int. Womens. Stud. 2020, 21, 255–270. [Google Scholar]
- Carvajal, L.; Wilson, E.; Requejo, J.H.; Newby, H.; Eriksson, C.d.C.; Liang, M.; Dennis, M.; Gohar, F.; Simon-Kapeu, A.; Idele, P.; et al. Basic maternal health care coverage among adolescents in 22 sub-Saharan African countries with high adolescent birthrate. J. Glob. Health 2020, 10, 021401. [Google Scholar] [CrossRef]
- Amjad, S.; Macdonald, I.; Chambers, T.; Osornio-Vargas, A.; Chandra, S.; Voaklander, D.; Ospina, M.B. Social determinants of health and adverse maternal and birth outcomes in adolescent pregnancies: A systematic review and meta-analysis. Paediatr. Perinat. Epidemiol. 2019, 33, 88–99. [Google Scholar] [CrossRef]
- Iliadou, M.; Papadakaki, M.; Sioti, E.; Giaxi, P.; Leontitsi, E.; Petelos, E.; Muijsenbergh, M.V.D.; Tziaferi, S.; Mastroyiannakis, A.; Vivilaki, V.G. Addressing mental health issues among migrant and refugee pregnant women: A call for action. Eur. J. Midwifery 2019, 3, 9. [Google Scholar] [CrossRef]
- Collins, C.H.; Zimmerman, C.; Howard, L.M. Refugee, asylum seeker, immigrant women and postnatal depression: Rates and risk factors. Arch. Women’s Ment. Health 2011, 14, 3–11. [Google Scholar] [CrossRef]
- Balaam, M.-C.; Kingdon, C.; Haith-Cooper, M. A Systematic Review of Perinatal Social Support Interventions for Asylum-seeking and Refugee Women Residing in Europe. J. Immigr. Minor. Health 2021, 1–18. [Google Scholar] [CrossRef]
- McKnight, P.; Goodwin, L.; Kenyon, S. A systematic review of asylum-seeking women’s views and experiences of UK maternity care. Midwifery 2019, 77, 16–23. [Google Scholar] [CrossRef]
- Feldman, R. When maternity doesn’t matter: Dispersing pregnant women seeking asylum. Br. J. Midwifery 2014, 22, 23–28. [Google Scholar] [CrossRef]
- Harris, M.; Humphries, K.; Nabb, J. Delivering care for women seeking refuge. RCM Midwives 2006, 9, 190–192. [Google Scholar]
- Reynolds, B.; White, J. Seeking asylum and motherhood: Health and wellbeing needs. Community Pract. 2010, 83, 20–23. [Google Scholar]


| n (%) | |
|---|---|
| Age | |
| 15–19 | 72 (2.5) |
| 20–29 | 1540 (54.4) |
| 30–39 | 1078 (38.1) |
| 40–49 | 139 (4.9) |
| 50+ | 2 (0.1) |
| Regions of Origin | |
| America | 30 (1.1) |
| Asia and Pacific | 417 (14.7) |
| Europe | 361 (12.8) |
| Middle East/North Africa | 957 (33.8) |
| East/Horn of Africa | 528 (18.7) |
| West/Central Africa | 458 (16.2) |
| Southern Africa | 50 (1.8) |
| Unknown/stateless | 30 (1.1) |
| Registered with Partner | |
| Yes | 1560 (55.1) |
| No | 1271 (44.9) |
| Length of Stay | |
| 0–9 months | 1471 (52.0) |
| 9–12 months | 409 (14.4) |
| 12+ months | 951 (33.6) |
| Number of Relocations during Pregnancy | |
| 0 | 864 (30.5) |
| 1 | 1169 (41.3) |
| 2 | 439 (15.5) |
| 3 | 235 (8.3) |
| 4 or more | 124 (4.4) |
| Subgroups | |
| Unaccompanied minors | 49 (1.7) |
| Undocumented women | 319 (11.3) |
| Women of Fertile Age (15–49) | Women Aged 15–19 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Region of Origin of the Mother | Women per 5 Years 1,2 | Births in 5 Years | Birthrate per 1000 3 | 95% CI Birthrate per 1000 | Birth Ratio vs. NL | Women per 5 Years | Teenage Births in 5 Years | Teenage Birthrate per 1000 3 | 95% CI Teenage Birthrate per 1000 | Teenage Pregnancy Ratio vs. NL | ||
| Lower | Upper | Lower | Upper | |||||||||
| The Netherlands | 18,874,506 | 849,242 | 44.99 | 44.90 | 45.09 | N/A | 2,539,944 | 6678 | 2.63 | 2.57 | 2.69 | N/A |
| Asylum seekers | 30,194 | 2922 | 96.77 | 91.93 | 98.90 | 2.15 | 4045 | 72 | 17.80 | 13.69 | 21.91 | 6.77 |
| America | 577 | 30 | 51.99 | 33.39 | 70.60 | 1.16 | 62 | 0 | 0.00 | 0 | 0 | 0.00 |
| Asia and Pacific | 6489 | 421 | 64.88 | 58.68 | 71.08 | 1.44 | 699 | 7 | 10.01 | 2.60 | 17.43 | 3.81 |
| Europe | 3756 | 368 | 97.98 | 87.97 | 107.99 | 2.18 | 397 | 6 | 15.11 | 3.02 | 27.21 | 5.75 |
| Middle East/North Africa | 10,757 | 971 | 90.27 | 84.59 | 95.94 | 2.01 | 1479 | 28 | 18.93 | 11.92 | 25.94 | 7.20 |
| East/Horn of Africa | 5891 | 536 | 90.99 | 83.28 | 98.69 | 2.02 | 1043 | 21 | 20.13 | 11.52 | 28.75 | 7.66 |
| West/Central Africa | 1976 | 464 | 234.82 | 213.45 | 256.18 | 5.22 | 114 | 8 | 70.18 | 21.55 | 118.80 | 26.69 |
| Southern Africa | 434 | 52 | 119.82 | 87.25 | 152.38 | 2.66 | 42 | 0 | 0.00 | 0 | 0 | 0.00 |
| Unknown/stateless | 314 | 30 | 95.54 | 61.35 | 129.73 | 2.12 | 209 | 2 | 9.57 | −3.69 | 22.83 | 3.64 |
| n (%) | Teenage Mothers | Non-Teenage Mothers n (%) | |
|---|---|---|---|
| n (%) | |||
| Asylum Seekers | 2831 (100) | 72 (100) | 2759 (100) |
| Registered with Partner | |||
| Yes | 1560 (55.1) | 33 (45.8) | 1527 (55.3) |
| Unknown | 1271 (44.9) | 39 (54.2) | 1232 (44.7) |
| Length of Stay in ASC at Childbirth | |||
| 0–9 months | 1471 (52.0) | 48 (66.7) | 1423 (51.6) |
| 9–12 months | 409 (14.4) | 5 (6.9) | 404 (14.6) |
| >12 months | 951 (33.6) | 19 (26.4) | 932 (33.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tankink, J.B.; Verschuuren, A.E.H.; Postma, I.R.; van der Lans, P.J.A.; de Graaf, J.P.; Stekelenburg, J.; Mesman, A.W. Childbirths and the Prevalence of Potential Risk Factors for Adverse Perinatal Outcomes among Asylum Seekers in The Netherlands: A Five-Year Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12933. https://doi.org/10.3390/ijerph182412933
Tankink JB, Verschuuren AEH, Postma IR, van der Lans PJA, de Graaf JP, Stekelenburg J, Mesman AW. Childbirths and the Prevalence of Potential Risk Factors for Adverse Perinatal Outcomes among Asylum Seekers in The Netherlands: A Five-Year Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(24):12933. https://doi.org/10.3390/ijerph182412933
Chicago/Turabian StyleTankink, Julia B., Anouk E. H. Verschuuren, Ineke R. Postma, Peggy J. A. van der Lans, Johanna P. de Graaf, Jelle Stekelenburg, and Annelies W. Mesman. 2021. "Childbirths and the Prevalence of Potential Risk Factors for Adverse Perinatal Outcomes among Asylum Seekers in The Netherlands: A Five-Year Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 24: 12933. https://doi.org/10.3390/ijerph182412933
APA StyleTankink, J. B., Verschuuren, A. E. H., Postma, I. R., van der Lans, P. J. A., de Graaf, J. P., Stekelenburg, J., & Mesman, A. W. (2021). Childbirths and the Prevalence of Potential Risk Factors for Adverse Perinatal Outcomes among Asylum Seekers in The Netherlands: A Five-Year Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(24), 12933. https://doi.org/10.3390/ijerph182412933