
The Sagittal Integral Morphotype in Male and Female Rowers

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Approvals
2.2. Participants
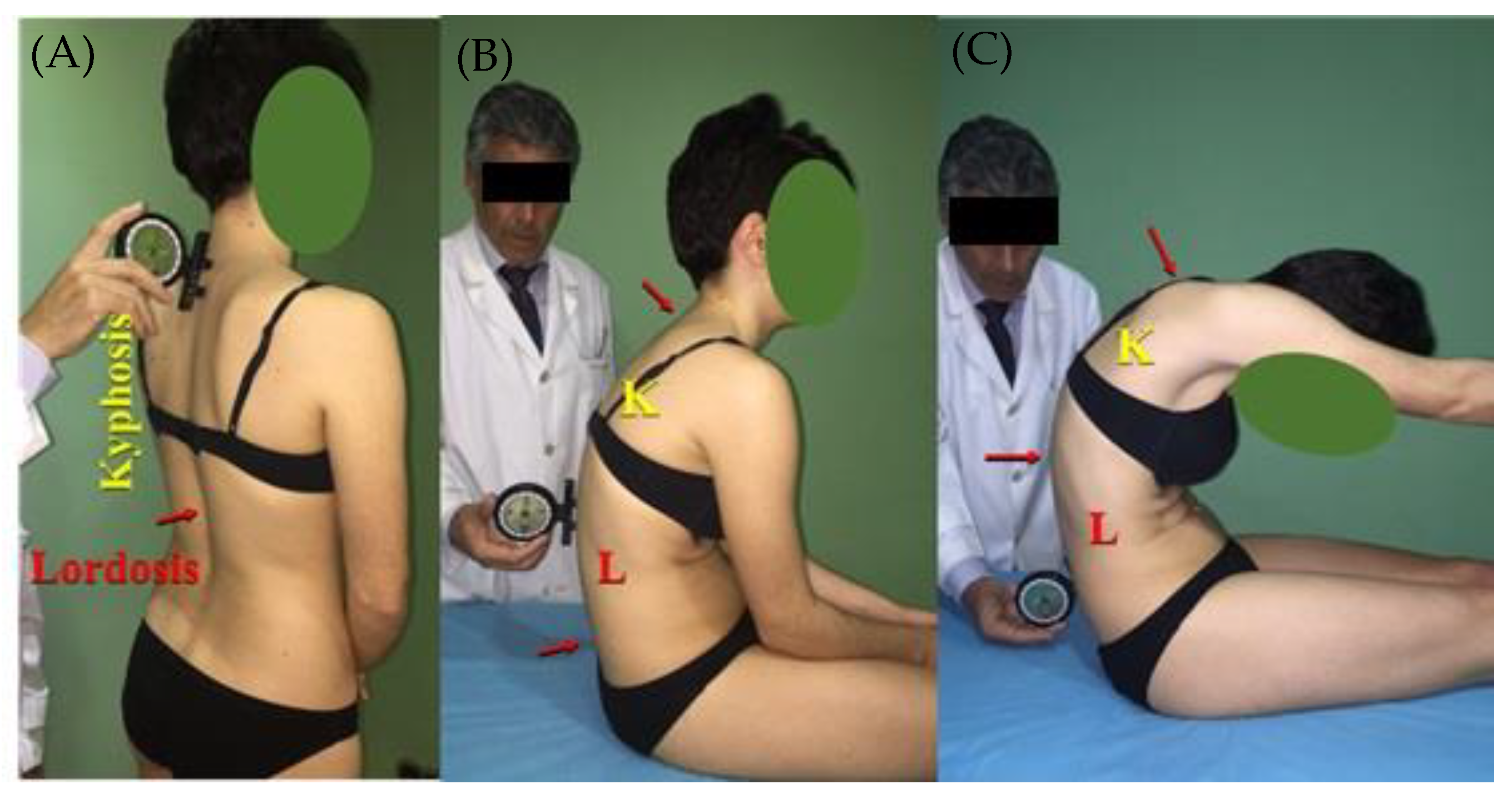
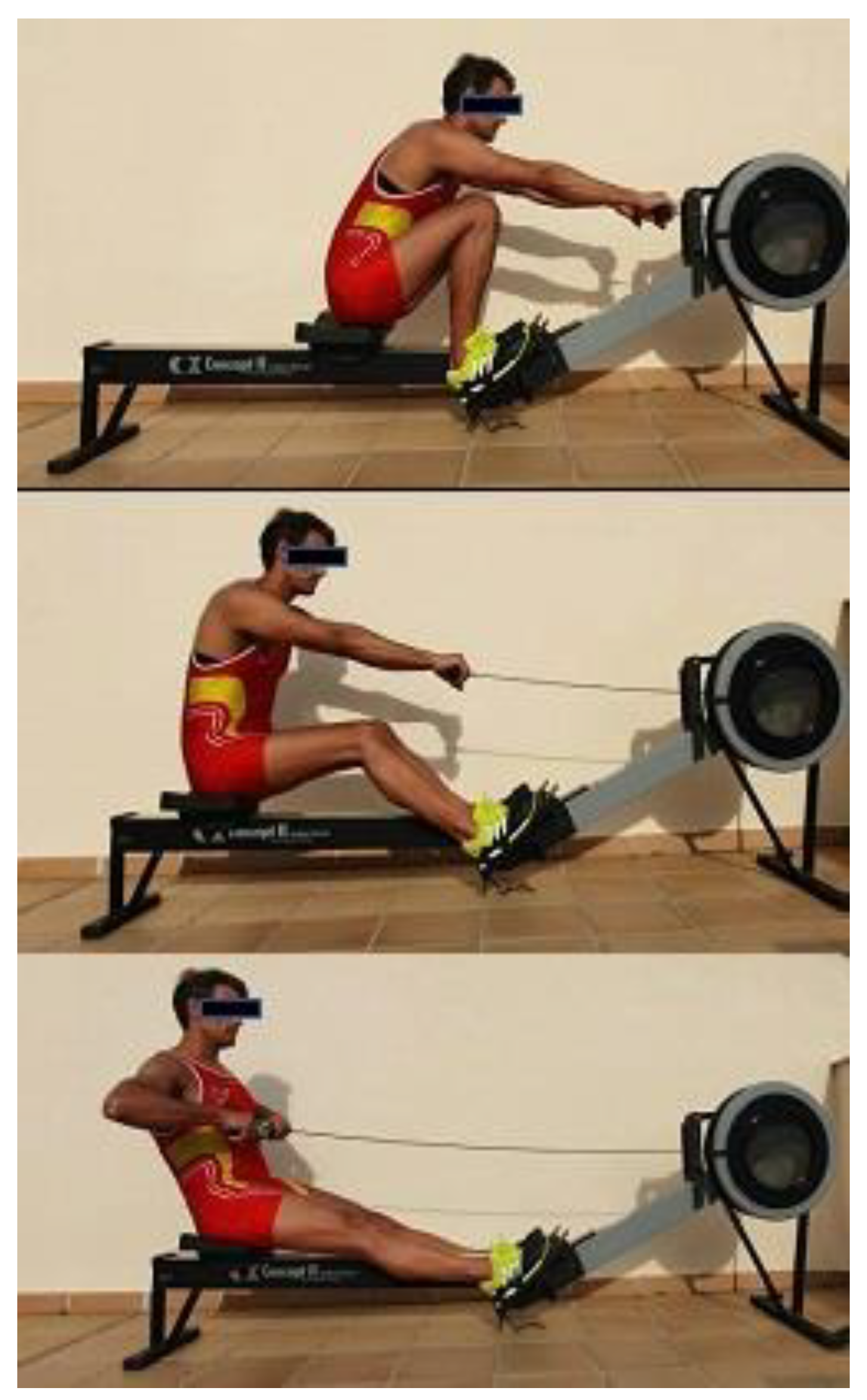
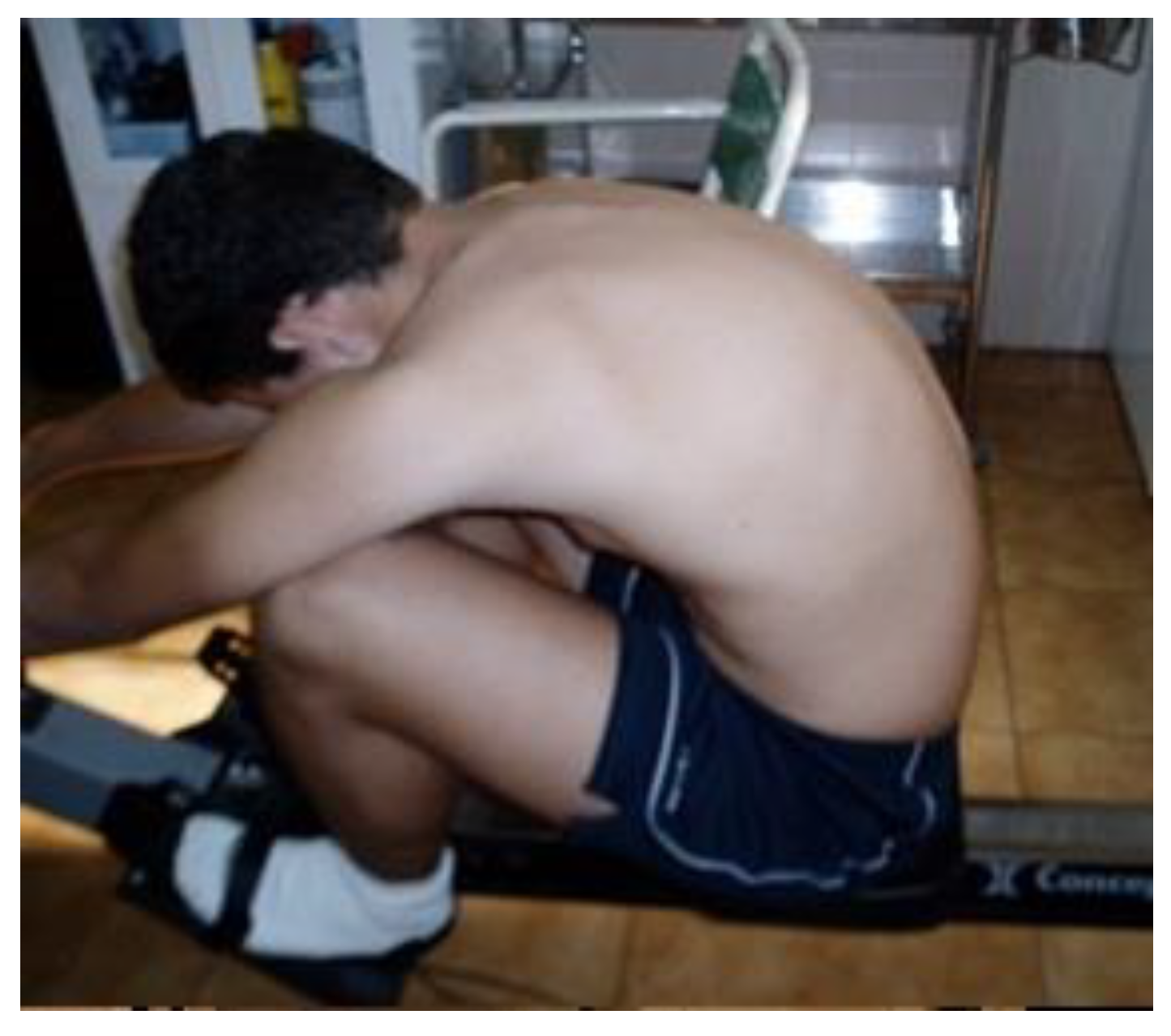
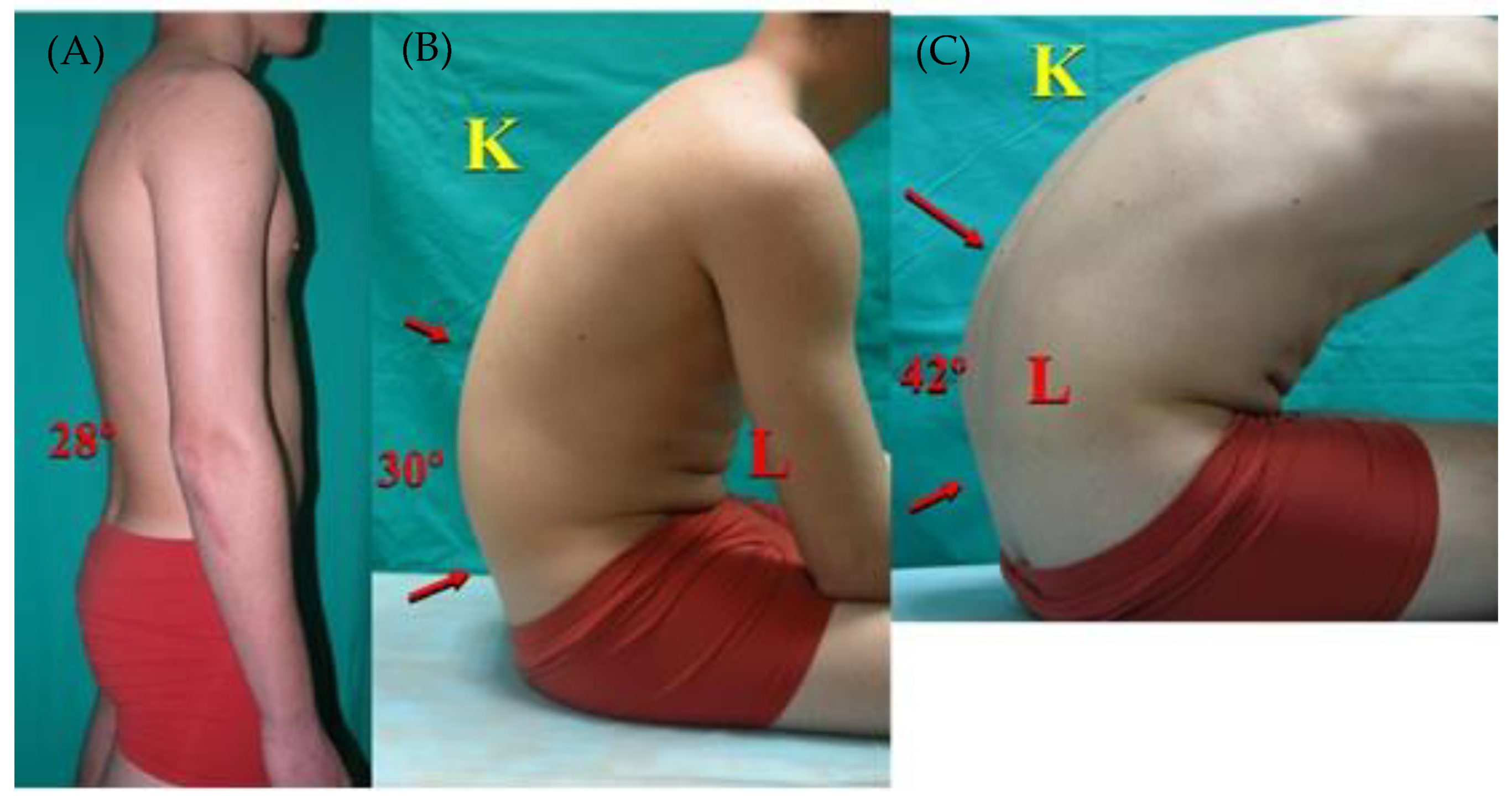
2.3. Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Thoracic Kyphosis
4.2. Lumbar Spine
4.3. Sagittal Integral Morphotype
4.4. Thoracic Morphotype

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thoracic Spine | Thoracic Morphotype | Lumbar Spine | Lumbar Morphotype | Demographics | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | SP | SSP | MTF | ↓ | Normal | ↑ | FTH | SP | SSP | MTF | ↓ | Normal | ↑ | FLK | Age, Mean or Range (Years) | n | |
| Rowers | Male | 30.2° | 47.8° | 63.7° | 7.5% | 91.3% | 1.2% | 57.5% | 27° | 20.1° | 29.3° | 12.5% | 83.8% | 3.7% | 46.3% | 17.2 (14–35) | 82 |
| Female | 30.6° | 39.5° | 59.3° | 10.3% | 86.2% | 3.4% | 27.6% | 33.1° | 14° | 24.3° | 3.4% | 75.9% | 20.7% | 20.7% | 17.8 (14–26) | 29 | |
| Scholars [36] | Both genders | 2.2% | 70.4% | 27.4% | 36.8% | 1.9% | 89.1% | 9% | 82.3% | 8–12 | 731 | ||||||
| In-line hockey [1] | Both genders | 38.5° | 45° | 53.7 | 1.4% | 60.8% | 37.8% | 18.9% | 28.7° | 28.7° | 31.5° | 9.5% | 89.2% | 1.4% | 66.1% | 8–15 | 74 |
| Dressage riders [13] | Both genders | 39.2° | 34.9° | 50.7° | 0 | 61.5% | 38.5% | 23.10% | 40.4° | 10° | 27.4° | 0 | 46.10% | 53.9% | 38.50% | 9–17 | 13 |
| Show jumping riders [13] | Both genders | 43.8° | 44.4° | 54.2° | 0 | 50% | 50% | 40% | 43.2° | 15.4° | 27° | 0 | 50% | 50% | 40% | 9–17 | 10 |
| Artistic gymnasts [3] | Male | 39.6° | 26° | 62.9° | 0% | 73.9% | 26% | 65.2% | 27.7° | 15.5° | 26° | 4.3% | 78.2% | 17.3% | 13% | 8–30 | 24 |
| Female | 31.8° | 49.3° | 61.4° | 8.3% | 87.5% | 4.16% | 75% | 30.5° | 15.7° | 27.7° | 0% | 83.3% | 16.6% | 29% | 24 | ||
| Scholars [40] | Both genders | 35.7° | 41.9° | 53.9° | 71.3% | 28.7% | - | 32.9° | 24.4° | 33.4° | 73.6% | 26.4% | - | 8–13 | 688 | ||
| Skiers [11] | Both genders | 41.2° | 33.4° | 16–19 | 51 | ||||||||||||
| Aesthetic group gymnastics [47] | Female | 29.3° | 47.9° | 69.1° | 22.3% | 67% | 9.6% | 25.4% | 32.9° | 15.9° | 26.4° | 6.4% | 77.7% | 16% | - | 10–18 | 94 |
| Scholars [41] | Male | 36.8° | 43.7° | 55.4° | 2.3% | 70.2% | 27.4% | - | 30.9° | 26.4° | 33.1° | 1.9% | 89.1% | 9% | - | 10–18 | 741 |
| Female | 35.4° | 41.8° | 54.9° | 33.2° | 23° | 33.5° | 10–18 | ||||||||||
| Ballet dancers [48] | 18.5° | 6.3° | 42.6° | 48.6% | 51.3% | 0% | - | 24.7° | 1.7° | 34.5° | 23.7% | 75% | 1.3% | - | 13.2 | 76 | |
| Tennis [31] | Male | 43.8° | 0% | 37.5% | 62.5% | 27.5° | 4.2% | 83.35 | 12.5% | - | 13–18 | 40 | |||||
| Female | 36.1° | 32.6° | |||||||||||||||
| Scholars [51] | Male | 35.5° | 43.1° | 64.8° | 0% | 76.5% | 23.5% | 38.5% | 33.9° | 9.2° | 19.5° | 0% | 88.2% | 11.8% | 20.5–23.9% | 11–12 | 39 |
| Female | 37.5° | 49° | 68.8° | 32.4° | 8.7° | 16.8° | 11–12 | 46 | |||||||||
| Teenagers [42] | Male | 37.6/47° | 43/55.1° | 66/80.7° | 0% | 44.5% | 54.5% | 29.7% | 29/35.7° | 7.3/12° | 16.6/23° | 1.2% | 90.5% | 8.3% | 26.2% | 13–18 | 119 |
| Female | 35/42.5° | 37.2/43° | 64/73.3° | 2.6% | 68.6% | 29% | 34/40.3° | 5.8/10° | 16.6–18° | 3.5% | 65.7% | 30.8% | 13–18 | 103 | |||
| Trampoline gymnasts [4] | Male | 46.9° | 51.3° | 62.8° | 32° | 21° | 30.3° | 14.9 | 34 | ||||||||
| Female | 43° | 49.2° | 53° | 40.3° | 14° | 25.2° | 35 | ||||||||||
| Scholars [52] | Both genders | 49.4° | 3.5% | 24.1% | 72.4% | - | 49.3° | 17.2% | 65.5% | 17.2% | 6–14 | 58 | |||||
| Weightlifting [10] | 40.5° | 42.7° | 61.6° | 0% | 72.8% | 27.2% | - | 31.9° | 15.4° | 25.4° | 0% | 18.1% | 47.5% | 22.8 | 22 | ||
| Kayakers [49] | Both genders | 42.5° | 72.2° | 28.6° | 35.8° | 14–17 | 30 | ||||||||||
| Dancers [12] | Ballet | 28.3° | 33.1° | 49.7° | 18.2% | 85.8% | 0% | - | 35.1° | 8.3° | 19.8° | 0% | 84.8% | 15.2% | 24.3% | 17–28 (22.7) | 33 |
| Spanish | 22.8° | 30.9° | 49.4° | 48% | 52% | 0% | - | 33.8° | 8.3° | 19.4° | 0% | 93.9% | 6.1% | 12.2% | 16–29 (22.1) | 33 | |
| Control | 37.5 | 39.7° | 71.9° | 0% | 69.7% | 30.3% | - | 40.3° | 5.5° | 15.7° | 0% | 58.8% | 41.2% | 9.3% | 17–29 (22.7) | 33 | |
| Rhythmic gymnasts [46] | Beginner | 33.4° | 37.6° | 56.7° | 3.7% | 82.5% | 13.8% | - | 40.3° | 16.2° | 25.1° | 1.2% | 57.5% | 41.3% | - | 6–18 | 81 |
| Squad | 28.3° | 38.5° | 50.4° | 14.6% | 80.5% | 4.9% | - | 35.8° | 16.8° | 26.3° | 3.7% | 62.2% | 34.1% | - | 82 | ||
| Control | 33.5° | 39.5° | 59.5° | 55 | 70.9% | 24.1% | - | 35.3° | 13.8° | 22.9° | 11.4% | 63.3% | 25.3% | - | 79 | ||
| Swimmers [5] | Male | 40.4° | 78.4° | 1.2% | 47% | 51.8% | - | 31.2° | 24.6° | 2.3% | 82.3% | 15.4% | - | 9–15 | 345 | ||
| Female | 39.5° | 73.4° | 36.3° | 21.6° | |||||||||||||
| Swimmers [7] (+radiograph) | Male | 53.3° | 0% | 18% | 82% | - | 43.5° | 0% | 42% | 58% | - | 9–15 | 99 | ||||
| Female | 48.6° | 0% | 38.8% | 61.2% | - | 50.9° | 0% | 18.45 | 81.6% | - | |||||||
| Scholars + intervention programme [39] | Intervention | 34.1° | 46° | 60.4° | 5.5% | 77.8% | 16.7% | 43.2 | 29.1° | 16.5° | 24° | 5.5% | 94.5% | 0% | 59.7% | 10–11 | 18 |
| Control Both genders | 35.3–36° | 42° | 64° | 6.1% | 66.7% | 27.2% | 24.8–40° | 15–16.5° | 28° | 7.4% | 82.7% | 9.95 | 10–11 | 81 | |||
| Scholars [53] | Both genders | 42.3° | 48.1° | 56.6° | 5 | 65.9% | 34.1% | - | 34.8° | 17.2° | 28.1° | 2.4% | 87.8% | 9.8% | - | ||
| Adults [54] | Both genders | 46.7° | 67.4° | 0% | 24.4% | 75.6% | - | 32.9° | 22.6° | 2.4% | 81.9% | 15.7% | - | 19–22 | 126 | ||
| Weightlifting [55] | Both genders | 46.3° | 0% | 42.5% | 57.5% | - | 32.3° | 3.8% | 83.9% | 12.3% | - | 18–24 | 772 | ||||
4.5. Lumbar Morphotype
4.6. Curve Adaptation According to Sport Technique, Age, and Years of Training
4.6.1. Age and Years of Training
4.6.2. Sport Technique
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sainz de Baranda, P.; Cejudo, A.; Moreno-Alcaraz, V.J.; Martinez-Romero, M.T.; Aparicio-Sarmiento, A.; Santonja-Medina, F. Sagittal spinal morphotype assessment in 8 to 15 years old Inline Hockey players. PeerJ 2020, 8, e8229. [Google Scholar] [CrossRef] [PubMed]
- Gracovetsky, S. Musculoskeletal function of the spine. In Multiple Muscle Systems: Biomechanics and Movement Organization; Winters, J.M., Woo, S.L.-Y., Eds.; Springer: New York, NY, USA, 1990; pp. 410–437. [Google Scholar]
- Sanz-Mengibar, J.M.; Sainz-de-Baranda, P.; Santonja-Medina, F. Training intensity and sagittal curvature of the spine in male and female artistic gymnasts. J. Sport Med. Phys. Fit. 2017, 58, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Sainz de Baranda, P.; Santonja Medina, F.; Rodríguez-Iniesta, M. Tiempo de entrenamiento y plano sagital del raquis en gimnastas de trampolín. Rev. Int. Med. Cienc. Act. Fis. Dep. 2010, 10, 521–536. [Google Scholar]
- Pastor, A.; Santonja, F.; Ferrer, V.; Domínguez, F.; Canteras, M. Determinación del morfotipo sagital de la columna de jóvenes nadadores de elite españoles. Selección 2002, 11, 268–269. [Google Scholar]
- Uetake, T.; Ohtsuke, F.; Tanaka, H.; Shindo, M. The vertebral curvature of sportsmen. J. Sports Sci. 1998, 16, 621–628. [Google Scholar] [CrossRef]
- Pastor Clemente, A. Estudio del Morfotipo Sagital de la Columna y Extensibilidad de la Musculatura Isquiosural de Jóvenes Nadadores de Elite Españoles. Ph.D. Thesis, Murcia University, Murcia, Spain, 2000. (In Spanish). [Google Scholar]
- Förster, R.; Penka, G.; Bösl, T.; Schöffl, V.R. Climber’s Back-Form and mobility of the thoracolumbar spine leading to postural adaptations in male high ability rock climbers. Int. J. Sports Med. 2009, 30, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Dalichau, S. Der Einfluss Sportmechanischer Belastungsprofile auf die Thorakolumbale Wirbelsäulenfom; Afra: Butzbach-Griedel, Germany, 2001; p. 184. [Google Scholar]
- Segura, D. Programa de Musculación para Desalineaciones Sagitales del Raquis en Adultos Jóvenes. Ph.D. Thesis, Murcia University, Murcia, Spain, 2009. (In Spanish). [Google Scholar]
- Alricsson, M.; Björklund, G.; Cronholm, M.; Olsson, O.; Viklund, P.; Svantesson, U. Spinal alignment, mobility of the hip and thoracic spine and prevalence of low back pain in young elite cross-country skiers. J. Exerc. Rehabil. 2016, 12, 21–28. [Google Scholar] [CrossRef][Green Version]
- Gómez Lozano, S.; Vargas-Macías, A.; Santonja-Medina, F.; Canteras, M. Estudio descriptivo del morfotipo raquídeo sagital en bailarinas de flamenco. Rev. Cent. Investig. Flamenco. Telethusa. 2013, 6, 19–28. [Google Scholar]
- Ginés-Díaz, A.; Martínez-Romero, M.T.; Cejudo, A.; Aparicio-Sarmiento, A.; Sainz de Baranda, P. Sagittal spinal morphotype assessment in dressage and show jumping riders. J. Sport Rehabil. 2019, 29, 533–540. [Google Scholar] [CrossRef]
- Grabara, M. Anteroposterior curvatures of the spine in adolescent athletes. J. Back Musculoskelet. Rehabil. 2014, 27, 513–519. [Google Scholar] [CrossRef]
- Callaghan, J.P.; McGill, S.M. Intervertebral disk herniation: Studies on a porcine model exposed to highly repetitive flexion/extension motion with compressive force. Clin. Biomech. 2001, 16, 28–37. [Google Scholar] [CrossRef]
- Newlands, C.; Reid, D.; Parmar, P. The prevalence, incidence and severity of low back pain among international level rowers. Br. J. Sports Med. 2015, 49, 951–956. [Google Scholar] [CrossRef]
- Wilson, F.; Gissane, C.; McGregor, A. Ergometer training volume and previous injury predict back pain in rowing; strategies for injury prevention and rehabilitation. Br. J. Sports Med. 2014, 48, 1534–1537. [Google Scholar] [CrossRef]
- Howell, D.W. Musculoskeletal profile and incidence of musculoskeletal injuries in lightweight women rowers. Am. J. Sports Med. 1984, 12, 278–282. [Google Scholar] [CrossRef]
- Ng, L.; Perich, D.; Burnett, A.; Campbell, A.; O’Sullivan, P. Self-reported prevalence, pain intensity and risk factors for low back pain in adolescent rowers. J. Sci. Med. Sport 2014, 17, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, J.; McNair, P.; Williams, M. The effects of repetitive motion on lumbar flexion and erector spinae muscle activity in rowers. Clin. Biomech. 2003, 18, 704–711. [Google Scholar] [CrossRef]
- Maurer, M.; Soder, R.B.; Baldisserotto, M. Spine abnormalities depicted by magnetic resonance imaging in adolescent rowers. Am. J. Sports Med. 2011, 39, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Wojtys, E.M.; Ashton-Miller, J.A.; Huston, L.J.; Moga, P.J. The association between athletic training time and the sagittal curvature of the immature spine. Am. J. Sports Med. 2000, 28, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Ashton-Miller, J.A. Thoracic hyperkyphosis in the young athlete: A review of the biomechanical issues. Curr. Sports Med. Rep. 2004, 3, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Harringe, M.L.; Nordgren, J.S.; Arvidsson, I.; Werner, S. Low back pain in young female rowers and the effect of specific segmental muscle control exercises of the lumbar spine: A prospective controlled intervention study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 1264–1271. [Google Scholar] [CrossRef]
- Wilson, F.; Gissane, C.; Gormley, J.; Simms, C. Sagittal plane motion of the lumbar spine during ergometer and single scull rowing. Sports Biomech. 2013, 12, 132–142. [Google Scholar] [CrossRef]
- O’Sullivan, F.; O’Sullivan, J.; Bull, A.M.; McGregor, A.H. Modelling multivariate biomechanical measurements of the spine during a rowing exercise. Clin. Biomech. 2003, 18, 488–493. [Google Scholar] [CrossRef]
- Wilson, F.; Gormley, J.; Gissane, C.; Simms, C. The effect of rowing to exhaustion on frontal plane angular changes in the lumbar spine of elite rowers. J. Sports Sci. 2012, 30, 481–489. [Google Scholar] [CrossRef]
- Holt, P.; Bull, A.; Cashman, P.; McGregor, A.H. Kinematics of spinal motion during prolonged rowing. Int. J. Sports Med. 2003, 24, 597–602. [Google Scholar] [PubMed]
- Morris, F.L.; Smith, R.M.; Payne, W.R.; Galloway, M.A.; Wark, J.D. Compressive and shear force generated in the lumbar spine of female rowers. Int. J. Sports Med. 2000, 21, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Sainz de Baranda, P.S.; Santonja, F. Valoración de la disposición sagital del raquis en gimnastas especialistas en trampolín. Int. J. Sport Sci. 2009, 5, 21–33. [Google Scholar]
- Muyor, J.M.; Sánchez-Sánchez, E.; Sanz-Rivas, D.; López-Miñarro, P.A. Sagittal Spinal Morphology in Highly Trained Adolescent Tennis Players. J. Sports Sci. Med. 2013, 12, 588–593. [Google Scholar]
- Cejudo, A.; Gómez-Lozano, S.; Sainz de Baranda, P.; Vargas-Macías, A.; Santonja-Medina, F. Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain. Int. J. Environ. Res. Public Health 2021, 18, 5039. [Google Scholar] [CrossRef]
- Cejudo, A.; Centenera-Centenera, J.M.; Santonja-Medina, F. Sagittal Integral Morphotype of Competitive Amateur Athletes and Its Potential Relation with Recurrent Low Back Pain. Int. J. Environ. Res. Public Health 2021, 18, 8262. [Google Scholar] [CrossRef] [PubMed]
- Santonja, F. Las desviaciones sagitales del raquis y su relación con la práctica deportiva. In Escolar, Medicina y Deporte; Ferrer, V., Martínez, L., Santonja, F., Eds.; Diputación Provincial: Albacete, Spain, 1996; pp. 251–268. [Google Scholar]
- Santonja-Medina, F.; Collazo, M.; Martínez-Romero, M.T.; Rodríguez-Ferrán, O.; Cejudo, A.; Andújar, P.; Sainz de Baranda, P. Classification System of the Sagittal Integral Morphotype in Children from the ISQUIOS Programme (Spain). Int. J. Environ. Res. Public Health 2020, 17, 2467. [Google Scholar] [CrossRef] [PubMed]
- Sainz de Baranda, P.; Cejudo, A.; Martínez-Romero, M.T.; Aparicio-Sarmiento, A.; Rodríguez-Ferrán, O.; Collazo-Dieguez, M.; Hurtado-Avilés, J.; Andújar, P.; Santonja-Medina, F. Sitting posture, Sagittal Spinal Curvatures and Back Pain in 8 to 12-Year-Old Children from the Region of Murcia (Spain): ISQUIOS Programme. Int. J. Environ. Res. Public Health 2020, 17, 2578. [Google Scholar] [CrossRef]
- Ng, J.K.; Kippers, V.; Richardson, C.A.; Parnianpour, M. Range of motion and lordosis of the lumbar spine: Reliability of measurement and normative values. Spine J. 2001, 26, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Saur, P.M.; Ensink, F.M.; Frese, K.; Seeger, D.; Hildebrandt, J. Lumbar range of motion: Reliability and validity of the inclinometer technique in the clinical measurement of trunk flexibility. Spine J. 1996, 21, 1332–1338. [Google Scholar] [CrossRef]
- Sainz de Baranda, P. Programa para la Mejora del Raquis en el Plano Sagital y Extensibilidad Isquiosural en Enseñanza Primaria. Ph.D. Thesis, Murcia University, Murcia, Spain, 2002. (In Spanish). [Google Scholar]
- Santonja Renedo, F. Efectos de un Programa de Educación Postural Sobre el Morfotipo Sagital del Raquis y la Extensibilidad Isquiosural: Estudio Multicéntrico en Escolares de Educación Primaria. Ph.D. Thesis, Murcia University, Murcia, Spain, 2017. (In Spanish). [Google Scholar]
- Collazo, M. Morfotipos Sagitales del Raquis en Población Escolar en la Región de Murcia. Ph.D. Thesis, Murcia University, Murcia, Spain, 2015. (In Spanish). [Google Scholar]
- Peña, W.A. Educación Física y Salud: Programa para la Mejora del Raquis en el Plano Sagital y la Extensibilidad Isquiosural en Secundaria. Ph.D. Thesis, Murcia University, Murcia, Spain, 2010. (In Spanish). [Google Scholar]
- Harriss, D.J.; Macsween, A.; Atkinson, G. Ethical Standards in Sport and Exercise Science Research: 2020 Update. Int. J. Sports Med. 2019, 40, 813–817. [Google Scholar] [CrossRef]
- Santonja, F.; Pastor, A.; Andújar, P. Cifosis y lordosis. In Cirugía Menor y Procedimientos en Medicina de Familia, 2nd ed.; Arribas, J.M., Castelló, J.R., Rodríguez, N., Santonja, F., Plazas, N., Eds.; Jarpyo Editores: Madrid, Spain, 2006; Volume 4, pp. 1551–1562. [Google Scholar]
- Hinkle, D.; Wiersma, W.; Jurs, S. Applied Statistics for the Behavioural Sciences, 5th ed.; Houghton Mifflin College Division: Boston, MA, USA, 2003. [Google Scholar]
- Martínez-Gallego, F.; Rodríguez, P. Metodología para una Gimnasia Rítmica Saludable; Consejo Superior de Deportes: Madrid, Spain, 2006. [Google Scholar]
- Conesa, E. Valoración de la Columna en el Plano Sagital y Extensibilidad Isquiosural en Gimnasia Estética de Grupo. Ph.D. Thesis, Murcia University, Murcia, Spain, 2015. (In Spanish). [Google Scholar]
- Vaquero-Cristóbal, R.; Esparza-Ros, F.; Gómez-Durán, R.; Martínez-Ruiz, E.; Muyor, J.M.; Alacid, F.; López-Miñarro, P.A. Morfología de las curvaturas torácica y lumbar en bipedestación, sedentación y máxima flexión del tronco con rodillas extendidas en bailarinas. Arch. Med. Deport. 2015, 32, 87–93. [Google Scholar]
- López-Miñarro, P.; Alacid Cárceles, F. Cifosis funcional y actitud cifótica lumbar en piragüistas adolescentes. Retos Nuevas Tend. en Educ. Física Deporte y Recreación 2010, 17, 5–9. [Google Scholar]
- Bado, J.L. Dorso Curvo; Artecolor: Montevideo, Uruguay, 1977. [Google Scholar]
- Fernández Campos, M.J. Efecto de un Programa de Educación Postural en Educación Primaria: Tres años de Seguimiento. Ph.D. Thesis, Murcia University, Murcia, Spain, 2011. (In Spanish). [Google Scholar]
- Andújar, P. Prevalencia de las Desalineaciones Sagitales del Raquis en edad Escolar en el Municipio de Murcia. Ph.D. Thesis, Murcia University, Murcia, Spain, 2010. (In Spanish). [Google Scholar]
- Martínez-García, A.C. Efectos de un Programa de Educación Postural Sobre el Morfotipo Sagital del Raquis, la Extensibilidad de la Musculatura Isquiosural y Psoas Iliaco y la Resistencia Muscular Abdominal y Lumbar en Escolares de Educación Secundaria. Ph.D. Thesis, Murcia University, Murcia, Spain, 2013. (In Spanish). [Google Scholar]
- Ríos de Moya Angeler, R. Evaluación a los Nueve años del Programa de Atención al niño Estudio de Factores Antropométricos, Cardiovasculares y de la Columna Vertebral. Ph.D. Thesis, Murcia University, Murcia, Spain, 2012. (In Spanish). [Google Scholar]
- López Miñarro, P.A. Análisis de Ejercicios de Acondicionamiento Muscular en salas de Musculación, Incidencia Sobre el Raquis en el Plano Sagital. Ph.D. Thesis, Murcia University, Murcia, Spain, 2003. (In Spanish). [Google Scholar]
- Santonja, F. Reconocimiento del aparato locomotor durante la edad escolar. In Valoración Médico-Deportiva del Escolar; Santonja, F., Martínez, I., Eds.; Secretariado de Publicaciones e Intercambio Científico, Universidad de Murcia: Murcia, Spain, 1992; pp. 258–277. [Google Scholar]
- Fon, G.T.; Pitt, M.J.; Thies, A.C., Jr. Thoracic Kyphosis: Range in Normal Subjects Thoracic. Am. J. Roentgenol. 1980, 134, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Mengibar, J.M.; Santonja-Medina, F. Correlation between sagittal spinal curves and gross motor function in children with typical development and with spastic bilateral cerebral palsy. Pilot study. Arch. Paediatr. Dev. Pathol. 2017, 1, 1009. [Google Scholar]
- Cejudo, A.; Centenera-Centenera, J.M.; Santonja-Medina, F. The Potential Role of Hamstring Extensibility on Sagittal Pelvic Tilt, Sagittal Spinal Curves and Recurrent Low Back Pain in Team Sports Players: A Gender Perspective Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8654. [Google Scholar] [CrossRef] [PubMed]
- Nugent, F.J.; Vinther, A.; McGregor, A.; Thornton, J.S.; Wilkie, K.; Wilson, F. The relationship between rowing-related low back pain and rowing biomechanics: A systematic review. Br. J. Sports Med. 2021, 55, 616–628. [Google Scholar] [CrossRef]
- McGregor, A.; Anderton, L.; Gedroyc, W. The assessment of intersegmental motion and pelvic tilt in elite oarsmen. Med. Sci. Sports Exerc. 2002, 34, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Morrison, A.B.; Schoffl, V.R. Physiological responses to rock climbing in young climbers. Br. J. Sports Med. 2007, 41, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Tabard-Fougère, A.; Bonnefoy-Mazure, A.; Dhouib, A.; Valaikaite, R.; Armand, S.; Dayer, R. Radiation-free measurement tools to evaluate sagittal parameters in AIS patients: A reliability and validity study. Eur. Spine J. 2019, 28, 536–543. [Google Scholar] [CrossRef]






| Sagittal Morphotype | Thoracic Curvature | Lumbar Curvature | |
|---|---|---|---|
| Standing | Normal range | 20–45° | (−)20–40° |
| Hyperkyphosis/hyperlordosis | >45° | >(−)40° | |
| Maximal trunk flexion in sit and reach test | Normal range kyphosis | 40–65° | 10–30° |
| Thoracic hyperkyphosis | >65° | ||
| Functional lumbar hyperkyphosis | >0° | ||
| Slump sitting | Normal range kyphosis | 20–45° | ±0–20° |
| Thoracic hyperkyphosis/ | >5° | >0° | |
| Functional lumbar hyperkyphosis |
| Variables | Men (n = 82) | Women (n = 29) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | 95% CI | Mean ± SD | Median | 95% CI | ||
| Demographics | |||||||
| Age (years) | 17.28 ± 3.23 | 16 | 16.0–17.0 | 17.86 ± 3.34 | 16.5 | 16–18.0 | 0.35 |
| Training (years) | 4.72 ± 3.42 | 4 | 3.0–5.0 | 5.73 ± 4.64 | 4 | 3–6.6 | 0.49 |
| Standing position | |||||||
| Thoracic (°) | 30.21 ± 8.27 | 30 | 29.3–33 | 30.62 ± 9.03 | 32 | 26–35.0 | 0.82 |
| Lumbar (°) | 27.01 ± 9.57 | 26 | 25.0–28.0 | 33.14 ± 9.13 | 34 | 30–37.2 | 0.0008 |
| Slump sitting | |||||||
| Thoracic (°) | 47.83 ± 50 | 10.58 | 45.6–50.7 | 39.52 ± 9.48 | 39 | 35–45.2 | 0.003 |
| Lumbar (°) | 20.13 ± 9.04 | 20 | 16.9–23.0 | 14.03 ± 11.5 | 12 | 7.3–15.0 | 0.028 |
| Maximal trunk flexion | |||||||
| Thoracic (°) | 63.7 ± 9.76 | 65 | 61.6–65.0 | 59.38 ± 10.2 | 59 | 55–65.0 | 0.045 |
| Lumbar (°) | 29.35 ± 10.6 | 26 | 25.0–30.0 | 24.31 ± 10.7 | 22 | 18–26.0 | 0.026 |
| Ergometre position | |||||||
| Thoracic catch (°) | 34 ± 12.5 | 31 | 30.0–35.0 | 28.31 ± 13.5 | 25 | 21–30.2 | 0.026 |
| Thoracic finish (°) | 37.05 ± 11.3 | 35.5 | 34.0–40.0 | 30.07 ± 12.2 | 26 | 24.7–35.2 | 0.0086 |
| Thoracic extension (°) | 35.28 ± 11.2 | 35 | 30–38.02 | 36.55 ± 13.3 | 35 | 26–42.0 | 0.86 |
| Lumbar catch (°) | 22.24 ± 8.52 | 22 | 20.0–25.0 | 15.45 ± 5.93 | 16 | 11.7–20 | <0.0001 |
| Lumbar finish (°) | 17.67 ± 6.72 | 18 | 16.0–20.0 | 11.79 ± 6.66 | 12 | 8.0–15.0 | 0.0001 |
| Lumbar extension (°) | 7.64 ± 8.77 | 7 | 5.0–10.0 | −5.55 ± 11.1 | -5 | −8.0–0.0 | <0.0001 |
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| n = 82 | % | n = 29 | % | |||||
| CATEGORY Thoracic Morphotype | SUBCATEGORY | Standing | Slump Sitting | Maximal Trunk Flexion | Thoracic Morphotype | |||
| Hypokyphosis or hypokyphotic attitude | Standing | Hypokyphosis (<20°) | Normal (20–45°) | Normal (40–65°) | 6 (2 > 45° SS) | 7.3 | 3 | 10.3 |
| Hypomobile kyphosis | Normal (20–45°) | Normal (20–45°) | Hypokyphosis (<40°) | 0 | 0 | |||
| Normal kyphosis | Normal (20–45°) | Normal (20–45°) | Normal (40–65°) | 28 | 34.1 | 20 | 68.9 | |
| Hyperkyphosis | Total | Hyperkyphosis (>45°) | Hyperkyphosis (>45°) | Hyperkyphosis (>65°) | 1 | 1.2 | 0 | |
| Standing | Hyperkyphosis (>45°) | Normal (20–40°) | Normal (40–65°) | 0 | 0 | |||
| Static | Hyperkyphosis (>45°) | Hyperkyphosis (>45°) | Normal (40–65°) | 0 | 1 | 3.4 | ||
| Dynamic | Hyperkyphosis (>45°) | Normal (20–40°) | Hyperkyphosis (>65°) | 0 | 0 | |||
| Functional thoracic hyperkyphosis | Static | Normal (20–45°) | Hyperkyphosis (>45°) | Normal (40–65°) | 40 | 48.8 | 4 | 13.7 |
| Dynamic | Normal (20–45°) | Normal (20–40°) | Hyperkyphosis (> 65°) | 3 | 3.7 | 1 | 3.4 | |
| Total | Normal (20–45°) | Hyperkyphosis (>45°) | Hyperkyphosis (>65°) | 4 | 4.9 | 0 | ||
| CATEGORY Lumbar morphotype | SUBCATEGORY | Standing | Slump sitting | Maximal trunk flexion | Lumbar morphotype | |||
| Hypolordosis | Lumbar hypomobility | Hypolordotic attitude (<20°) | Normal (0 ± 20°) | Normal (10–30°) | 1 | 1.2 | 0 | |
| Normal lordosis | Normal (20–40°) | Normal (0 ± 20°) | Normal (10–30°) | 41 | 50 | 17 | 58.6 | |
| Functional lumbar hyperkyphosis | Static | Normal (20–40°) | Hyperkyphosis (>20°) | Normal (10–30°) | 9 | 11 | 0 | |
| Dynamic | Normal (20–40°) | Normal (0 ± 20°) | Hyperkyphosis (>30°) | 3 | 3.6 | 0 | ||
| Total | Normal (20–40°) | Hyperkyphosis (>20°) | Hyperkyphosis (10–30°) | 16 | 19.5 | 5 | 17.2 | |
| Hyperlordosis | Postural or attitude | >40° | Normal (0 ± 20°) | Normal (10–30°) | 2 | 2.4 | 6 | 20.7 |
| Structural | > 40° | Normal (0 ± 20°) or lordotic (<−20°) | Hypokyphosis (<10°) | 0 | 0 | |||
| Lumbar hypermobility | Hyperlordosis (>40°) | Normal (0±20°) or hyperkyphosis (>20°) | Normal (10–30°) or hyperkyphosis (> 30°) | 1 | 1.2 | 0 | ||
| Lumbar kyphosis | Hypolordosis or kyphosis (< 20°) | Hyperkyphosis (>20°) | Hyperkyphosis (>30°) | 9 | 11 | 1 | 3.4 | |
| Structural lumbar kyphosis | Lumbar kyphosis | Hyperkyphosis (>20°) | Hyperkyphosis (>30°) | 0 | 0 | |||
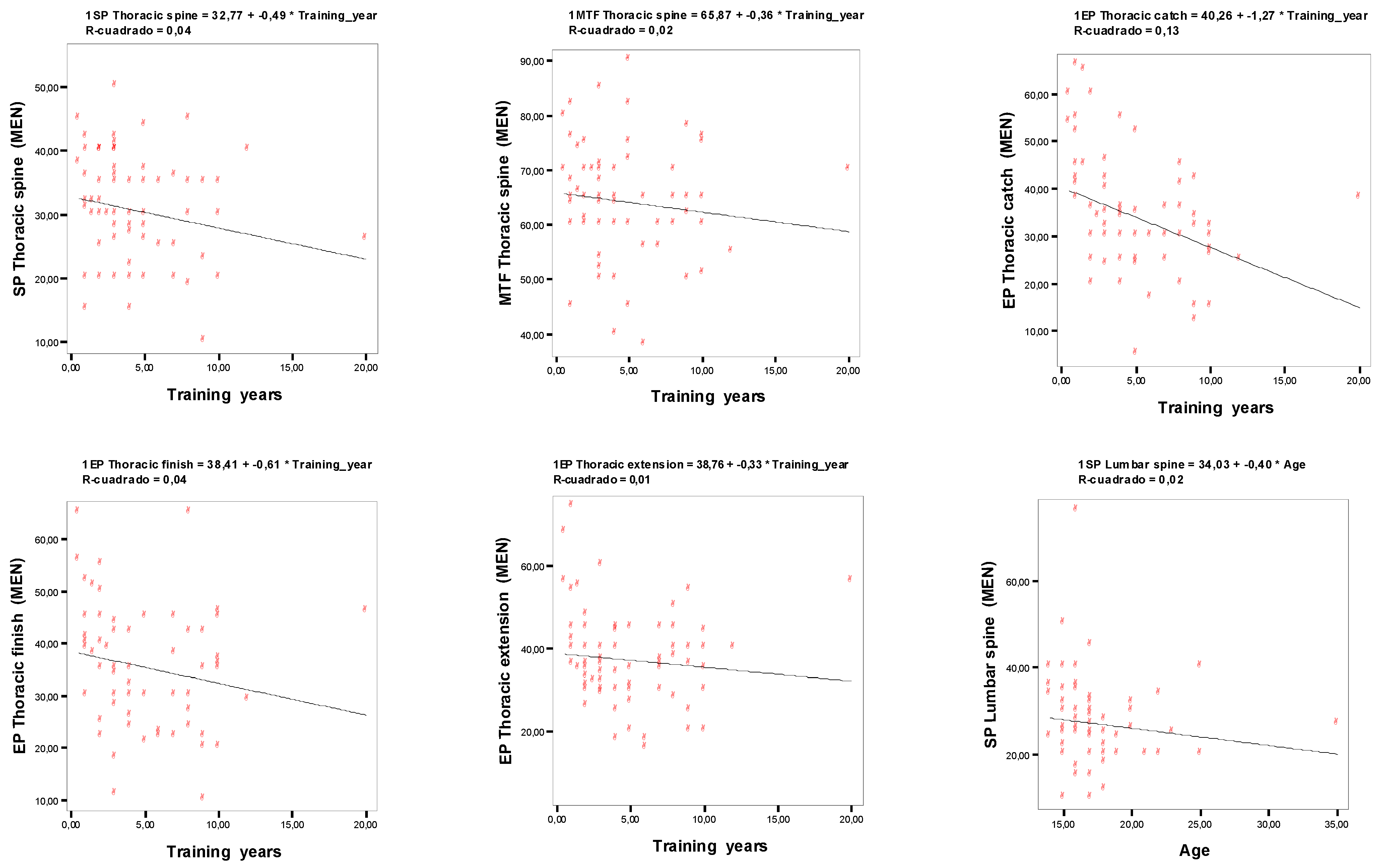
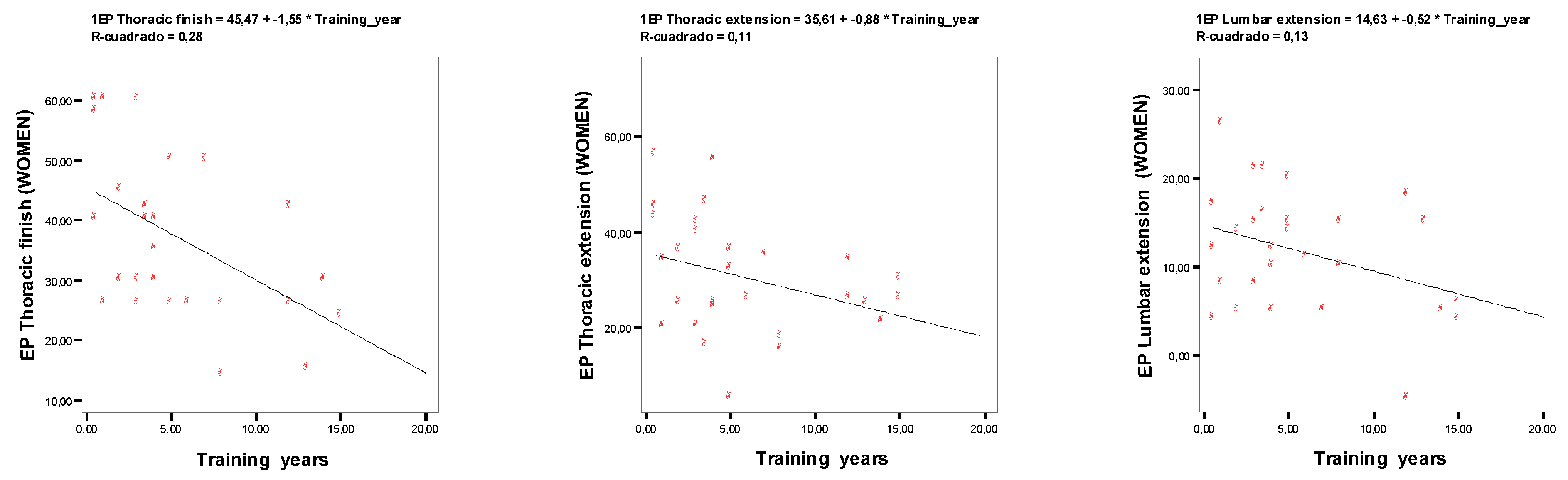
| Men | Women | |||
|---|---|---|---|---|
| Variable | Training Years | Age | Training Years | Age |
| Standing position | ||||
| Thoracic spine | −0.258 * | 0.021 | 0.018 | 0.033 |
| Lumbar spine | −0.204 | −0.302 ** | −0.161 | −0.045 |
| Slump sitting | ||||
| Thoracic spine | −0.069 | −0.038 | −0.031 | 0.086 |
| Lumbar spine | 0.097 | −0.034 | 0.304 | 0.15 |
| Maximal trunk flexion | ||||
| Thoracic spine | −0.249 * | 0.135 | −0.203 | −0.293 |
| Lumbar spine | 0.115 | −0.031 | 0.041 | −0.266 |
| Ergometre position | ||||
| Thoracic catch | −0.419 ** | −0.216 | −0.261 | −0.173 |
| Thoracic finish | −0.229 * | 0.053 | −0.385 * | −0.24 |
| Thoracic extension | −0.337 ** | 0.083 | −0.561 ** | −0.309 |
| Lumbar catch | -0.026 | -0.168 | 0.104 | 0 |
| Lumbar finish | 0.056 | 0.008 | −0.237 | −0.118 |
| Lumbar extension | 0.212 | −0.009 | 0.503 ** | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvero-Cruz, J.R.; Santonja-Medina, F.; Sanz-Mengibar, J.M.; Sainz de Baranda, P. The Sagittal Integral Morphotype in Male and Female Rowers. Int. J. Environ. Res. Public Health 2021, 18, 12930. https://doi.org/10.3390/ijerph182412930
Alvero-Cruz JR, Santonja-Medina F, Sanz-Mengibar JM, Sainz de Baranda P. The Sagittal Integral Morphotype in Male and Female Rowers. International Journal of Environmental Research and Public Health. 2021; 18(24):12930. https://doi.org/10.3390/ijerph182412930
Chicago/Turabian StyleAlvero-Cruz, Jose Ramón, Fernando Santonja-Medina, Jose Manuel Sanz-Mengibar, and Pilar Sainz de Baranda. 2021. "The Sagittal Integral Morphotype in Male and Female Rowers" International Journal of Environmental Research and Public Health 18, no. 24: 12930. https://doi.org/10.3390/ijerph182412930
APA StyleAlvero-Cruz, J. R., Santonja-Medina, F., Sanz-Mengibar, J. M., & Sainz de Baranda, P. (2021). The Sagittal Integral Morphotype in Male and Female Rowers. International Journal of Environmental Research and Public Health, 18(24), 12930. https://doi.org/10.3390/ijerph182412930