
Maternal Mental Health following Ultrasonographic Detection of Fetal Structural Anomaly in the Midst of the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Participants/Sampling
2.3.1. Eligibility Criteria
2.3.2. Sample Size
2.3.3. Sampling Technique
2.4. Instruments and Data Collection
2.4.1. Detailed Scan
2.4.2. Clinical Record
2.4.3. Self-Administered Questionnaires
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
3.1. Participants’ Profile
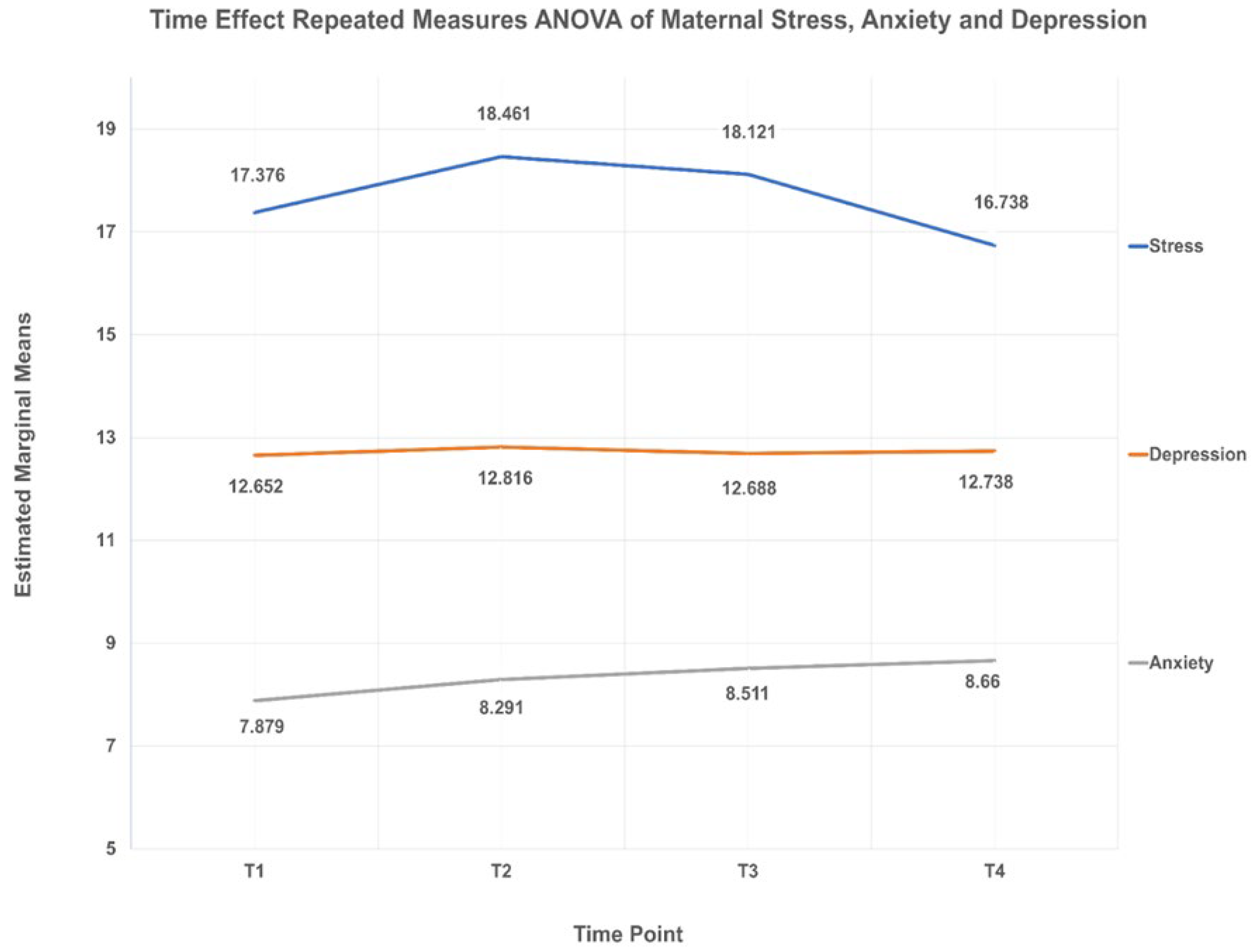
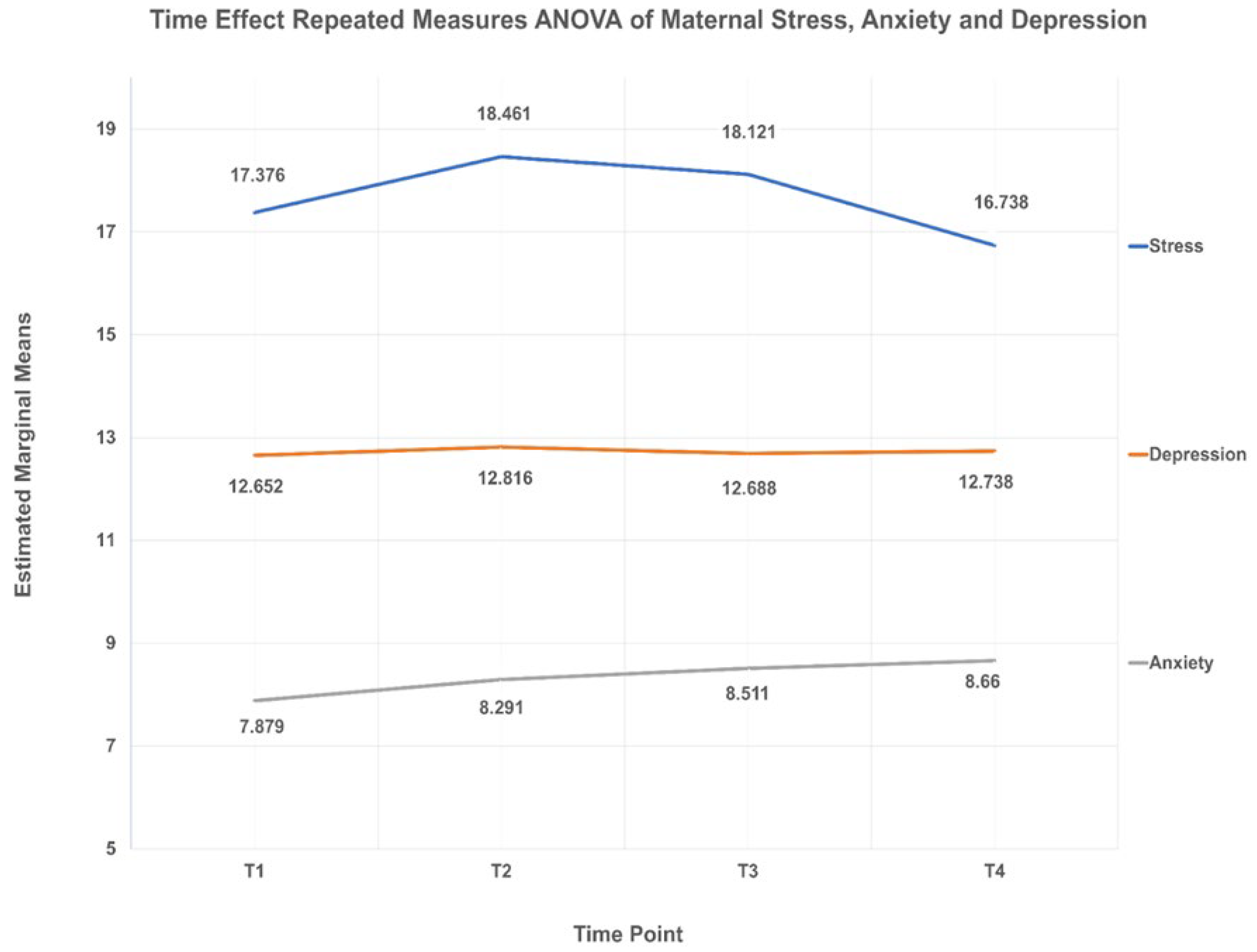
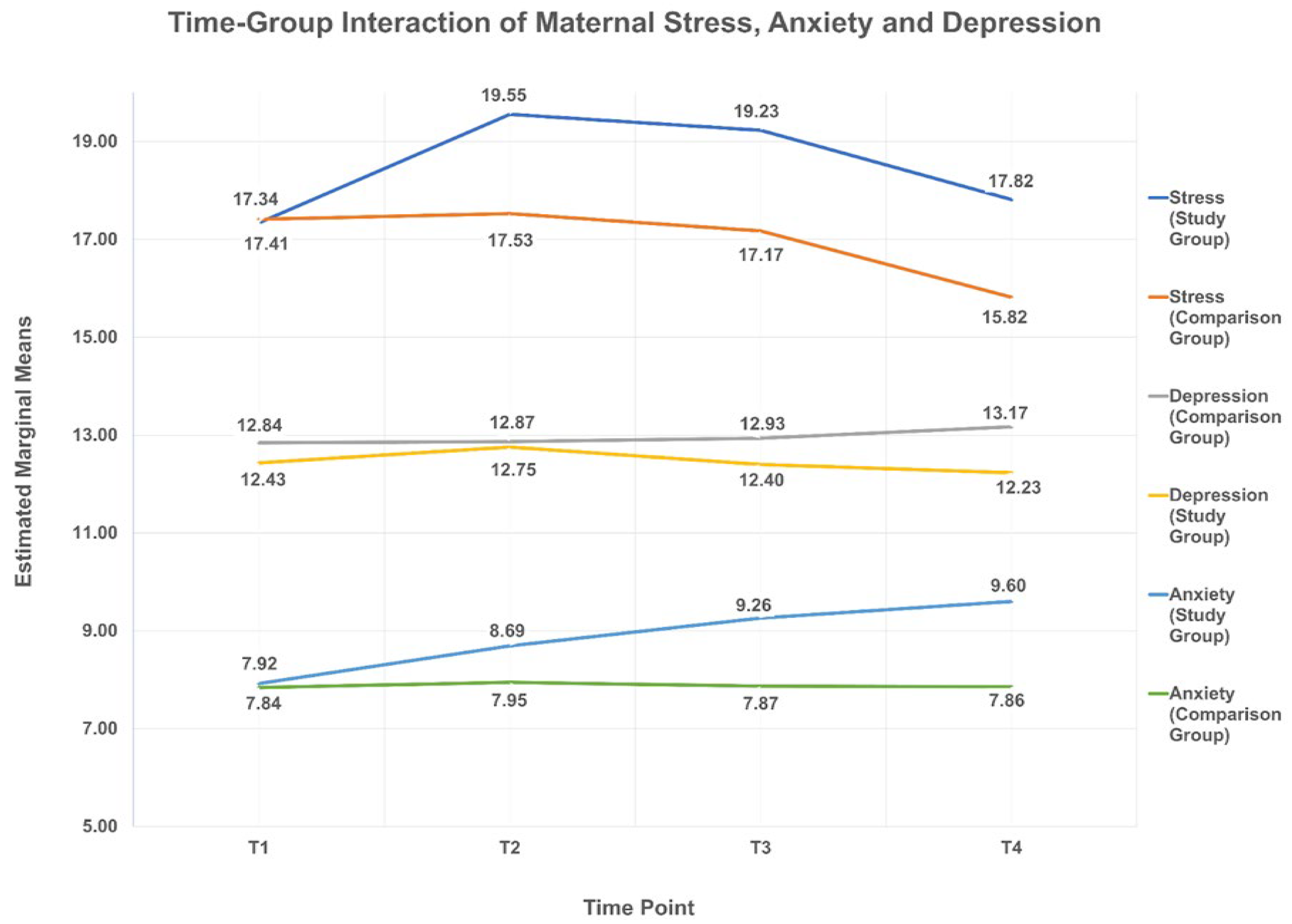
3.2. Participants’ Mental Health Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The prevalence of anxiety disorders during pregnancy and the postpartum period: A multivariate bayesian meta-analysis. J. Clin. Psychiatry 2019, 80, 18r12527. [Google Scholar] [CrossRef] [PubMed]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Wisner, K.L.; Sit, D.K.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.R.; Costantino, M.L.; et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef]
- Patton, G.C.; Romaniuk, H.; Spry, E.; Coffey, C.; Olsson, C.; Doyle, L.W.; Oats, J.; Hearps, S.; Carlin, J.B.; Brown, S. Prediction of perinatal depression from adolescence and before conception (VIHCS): 20-year prospective cohort study. Lancet 2015, 386, 875–883. [Google Scholar] [CrossRef]
- Munk-Olsen, T.; Maegbaek, M.L.; Johannsen, B.M.; Liu, X.; Howard, L.M.; di Florio, A.; Bergink, V.; Meltzer-Brody, S. Perinatal psychiatric episodes: A population-based study on treatment incidence and prevalence. Transl. Psychiatry 2016, 6, e919. [Google Scholar] [CrossRef]
- Glover, V. Prenatal mental health and the effects of stress on the foetus and the child. Should psychiatrists look beyond mental disorders? World Psychiatry 2020, 19, 331–332. [Google Scholar] [CrossRef]
- Dennis, C.L.; Hodnett, E. Psychosocial and psychological interventions for treating postpartum depression. Cochrane Database Syst. Rev. 2007, 4, CD006116. [Google Scholar] [CrossRef] [PubMed]
- Camacho, E.M.; Shields, G.E. Cost-effectiveness of interventions for perinatal anxiety and/or depression: A systematic review. BMJ Open 2018, 8, e022022. [Google Scholar] [CrossRef]
- Wisner, K.L.; Stika, C.S.; Watson, K. Pregnant women are still therapeutic orphans. World Psychiatry 2020, 19, 329–330. [Google Scholar] [CrossRef] [PubMed]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Pandemic-related pregnancy stress and anxiety among women pregnant during the coronavirus disease 2019 pandemic. Am. J. Obstet. Gynecol. MFM 2020, 2, 100155. [Google Scholar] [CrossRef]
- Marazziti, D.; Stahl, S.M. The relevance of COVID-19 pandemic to psychiatry. World Psychiatry 2020, 19, 261. [Google Scholar] [CrossRef]
- Tomfohr-Madsen, L.M.; Racine, N.; Giesbrecht, G.F.; Lebel, C.; Madigan, S. Depression and anxiety in pregnancy during COVID-19: A rapid review and meta-analysis. Psychiatry Res. 2021, 300, 113912. [Google Scholar] [CrossRef]
- López-Morales, H.; Del Valle, M.V.; Canet-Juric, L.; Andrés, M.L.; Galli, J.I.; Poó, F.; Urquijo, S. Mental health of pregnant women during the COVID-19 pandemic: A longitudinal study. Psychiatry Res. 2021, 295, 113567. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Parra-Saavedra, M.; Villa-Villa, I.; Pérez-Olivo, J.; Guzman-Polania, L.; Galvis-Centurion, P.; Cumplido-Romero, Á.; Santacruz-Vargas, D.; Rivera-Moreno, E.; Molina-Giraldo, S.; Guillen-Burgos, H.; et al. Attitudes and collateral psychological effects of COVID-19 in pregnant women in Colombia. Int. J. Gynaecol. Obstet. 2020, 151, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynecol. Obs. 2020, 151, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Fetal. Neonatal. Med. 2020, 18, 1–7. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S. Perinatal mental health and the COVID-19 pandemic. World Psychiatry 2020, 19, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Esegbona-Adeigbe, S. Impact of COVID-19 on antenatal care provision. Eur. J. Midwifery 2020, 4, 16. [Google Scholar] [CrossRef]
- Yassa, M.; Yassa, A.; Yirmibeş, C.; Birol, P.; Ünlü, U.G.; Tekin, A.B.; Sandal, K.; Mutlu, M.A.; Çavuşoğlu, G.; Tug, N. Anxiety levels and obsessive compulsion symptoms of pregnant women during the COVID-19 pandemic. Turk. J. Obs. Gynecol. 2020, 17, 155–160. [Google Scholar] [CrossRef]
- Ilska, M.; Brandt-Salmeri, A.; Kołodziej-Zaleska, A.; Banaś, E.; Gelner, H.; Cnota, W. Factors associated with fear of childbirth among Polish pregnant women. Sci. Rep. 2021, 11, 4397. [Google Scholar] [CrossRef] [PubMed]
- Syed Anwar Aly, S.A.; Abdul Rahman, R.; Sharip, S.; Shah, S.A.; Abdullah Mahdy, Z.; Kalok, A. Pregnancy and COVID-19 pandemic perception in Malaysia: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 5762. [Google Scholar] [CrossRef] [PubMed]
- Romosan, G.; Henriksson, E.; Rylander, A.; Valentin, L. Diagnostic performance of routine ultrasound screening for fetal abnormalities in an unselected Swedish population in 2000–2005. Ultrasound Obs. Gynecol. 2009, 34, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Bardi, F.; Bakker, M.; Kenkhuis, M.J.A.; Ranchor, A.V.; Bakker, M.K.; Elvan, A.; Birnie, E.; Bilardo, C.M. Psychological outcomes, knowledge and preferences of pregnant women on first-trimester screening for fetal structural abnormalities: A prospective cohort study. PLoS ONE 2021, 16, e0245938. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, T.; Mattsson, E. Emotional and cognitive experiences during the time of diagnosis and decision-making following a prenatal diagnosis: A qualitative study of males presented with congenital heart defect in the fetus carried by their pregnant partner. BMC Pregnancy Childbirth 2018, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Wilpers, A.B.; Kennedy, H.P.; Wall, D.; Funk, M.; Bahtiyar, M.O. Maternal anxiety related to prenatal diagnoses of fetal anomalies that require surgery. J. Obs. Gynecol. Neonatal. Nurs. 2017, 46, 456–464. [Google Scholar] [CrossRef]
- Cardwell, M.S. Stress: Pregnancy considerations. Obs. Gynecol. Surv. 2013, 68, 119–129. [Google Scholar] [CrossRef]
- Khashan, A.S.; Wicks, S.; Dalman, C.; Henriksen, T.B.; Li, J.; Mortensen, P.B.; Kenny, L.C. Prenatal stress and risk of asthma hospitalization in the offspring: A Swedish population-based study. Psychosom. Med. 2012, 74, 635–641. [Google Scholar] [CrossRef]
- Talge, N.M.; Neal, C.; Glover, V. Early Stress, Translational Research and Prevention Science Network: Fetal and Neonatal Experience on Child and Adolescent Mental Health. Antenatal maternal stress and long-term effects on child neurodevelopment: How and why? J. Child Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef]
- Van den Bergh, B.R.; Mulder, E.J.; Mennes, M.; Glover, V. Antenatal maternal anxiety and stress and the neurobehavioural development of the fetus and child: Links and possible mechanisms. A review. Neurosci. Biobehav. Rev. 2005, 29, 237–258. [Google Scholar] [CrossRef]
- Kaasen, A.; Helbig, A.; Malt, U.F.; Næs, T.; Skari, H.; Haugen, G. Maternal psychological responses during pregnancy after ultrasonographic detection of structural fetal anomalies: A prospective longitudinal observational study. PLoS ONE 2017, 12, e0174412. [Google Scholar] [CrossRef]
- Titapant, V.; Chuenwattana, P. Psychological effects of fetal diagnoses of non-lethal congenital anomalies on the experience of pregnant women during the remainder of their pregnancy. J. Obs. Gynaecol. Res. 2015, 41, 77–83. [Google Scholar] [CrossRef]
- Kaasen, A.; Helbig, A.; Malt, U.F.; Naes, T.; Skari, H.; Haugen, G.N. Paternal psychological response after ultrasonographic detection of structural fetal anomalies with a comparison to maternal response: A cohort study. BMC Pregnancy Childbirth 2013, 13, 147. [Google Scholar] [CrossRef] [Green Version]
- Al-Dubai, S.A.R.; Alshagga, M.A.; Rampal, K.G.; Sulaiman, N.A. Factor structure and reliability of the malay version of the Perceived Stress Scale among Malaysian medical students. Malays. J. Med. Sci. 2012, 19, 43–49. [Google Scholar]
- Matthey, S.; Valenti, B.; Souter, K.; Ross-Hamid, C. Comparison of four self-report measures and a generic mood question to screen for anxiety during pregnancy in English-speaking women. J. Affect. Disord. 2013, 148, 347–351. [Google Scholar] [CrossRef]
- Karimova, G.; Martin, C. A psychometric evaluation of the Hospital Anxiety and Depression Scale during pregnancy. Psychol. Health Med. 2003, 8, 89–103. [Google Scholar] [CrossRef]
- Jomeen, J.; Martin, C. Is the hospital anxiety and depression scale (HADS) a reliable screening tool in early pregnancy? Psychol. Health 2004, 19, 787–800. [Google Scholar] [CrossRef]
- Fadzil, A.; Balakrishnan, K.; Razali, R.; Sidi, H.; Malapan, T.; Japaraj, R.P.; Midin, M.; Nik Jaafar, N.R.; Das, S.; Manaf, M.R.A. Depression anxiety among pregnant women. Asia-Pac. Psychiatry 2013, 5, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms are not OK: COVID-19 and maternal mental health. Front. Glob. Women’s Health 2020, 1, 1. [Google Scholar] [CrossRef]
- Racine, N.; Hetherington, E.; McArthur, B.A.; McDonald, S.; Edwards, S.; Tough, S.; Madigan, S. Maternal depressive and anxiety symptoms before and during the COVID-19 pandemic in Canada: A longitudinal analysis. Lancet Psychiatry 2021, 8, 405–415. [Google Scholar] [CrossRef]
- Grumi, S.; Provenzi, L.; Accorsi, P.; Biasucci, G.; Cavallini, A.; Decembrino, L.; Falcone, R.; Fazzi, E.M.; Gardella, B.; Giacchero, R.; et al. Depression and anxiety in mothers who were pregnant during the COVID-19 outbreak in northern Italy: The role of pandemic-related emotional stress and perceived social support. Front. Psychiatry 2021, 12, 716488. [Google Scholar] [CrossRef] [PubMed]
- Shidhaye, R.; Madhivanan, P.; Shidhaye, P.; Krupp, K. An integrated approach to improve maternal mental health and well-being during the COVID-19 crisis. Front. Psychiatry 2020, 11, 598746. [Google Scholar] [CrossRef]
- RCOG (Royal College of Obstetrics and Gynaecology). Coronavirus (COVID-19) Infection in Pregnancy. 2021. Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/2021-02-19-coronavirus-covid-19-infection-in-pregnancy-v13.pdf (accessed on 1 November 2021).
- Cole, J.C.; Moldenhauer, J.S.; Berger, K.; Cary, M.S.; Smith, H.; Martino, V.; Rendon, N.; Howell, L.J. Identifying expectant parents at risk for psychological distress in response to a confirmed fetal abnormality. Arch. Women’s Ment. Health 2016, 19, 443–453. [Google Scholar] [CrossRef]
- Aite, L.; Zaccara, A.; Mirante, N.; Nahom, A.; Trucchi, A.; Capolupo, I.; Bagolan, P. Antenatal diagnosis of congenital anomaly: A really traumatic experience? J. Perinatol. 2011, 31, 760–763. [Google Scholar] [CrossRef] [PubMed]
- Teefey, C.P.; Hertzog, J.; Morris, E.D.; Moldenhauer, J.S.; Cole, J.C.M. The impact of our images: Psychological implications in expectant parents after a prenatal diagnosis. Pediatrics Radiol. 2020, 50, 2028–2033. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry 2020, 19, 406–407. [Google Scholar] [CrossRef] [PubMed]
- McDaid, D. Viewpoint: Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry 2021, 64, E32. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Sub Variables | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Ethnicity | Malay | 118 | 83.70 |
| Non-Malay (Chinese/Indian/Others) | 23 | 16.31 | |
| Level of Education | No formal education | 6 | 4.30 |
| School/Pre-University | 40 | 28.37 | |
| University (Diploma/Degree/Master) | 95 | 67.38 | |
| Marital Status | Married | 138 | 97.90 |
| Separated/Divorced | 3 | 2.10 | |
| Household Income | B40 (less than RM 4360.00) | 93 | 66.00 |
| M40 (RM 4360.00 to RM 9619.00) | 40 | 28.40 | |
| T20 (more than RM 9619.00) | 8 | 5.70 | |
| Parity | Nulliparous | 40 | 28.40 |
| Multiparous | 101 | 71.60 | |
| IVF Pregnancy Status | Yes | 4 | 2.80 |
| No | 137 | 97.20 |
| Variables | Sub Variables | n (%) 1 | χ2 | df | p-Value | |
|---|---|---|---|---|---|---|
| Study Group (n = 65) | Comparison Group (n = 76) | |||||
| Age, in years | 18 to 35 | 56 (47.5) | 62 (52.5) | 0.537 | 1 | 0.464 |
| More than 35 | 9 (39.1) | 14 (60.9) | ||||
| Ethnics | Malay | 52 (44.1) | 66 (55.9) | 1.201 | 1 | 0.273 |
| Non-Malay | 13 (56.5) | 10 (43.5) | ||||
| Level of Education | Non-University | 24 (52.2) | 22 (47.8) | 1.014 | 1 | 0.314 |
| University | 41 (43.2) | 54 (56.8) | ||||
| IVF Pregnancy Status | No | 64 (46.7) | 73 (53.3) | 0.738 | 1 | 0.390 |
| Yes | 1 (25.0) | 3 (75.0) | ||||
| Variables | Sub Variables | n (%) | Mean Difference | t (df) | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| All (n = 141) | Study Group (n = 65) | Comparison Group (n = 76) | ||||||
| Stress 1 | T1 | 17.38 (5.530) | 17.34 (4.960) | 17.41 (6.007) | −0.069 | −0.074 (139) | −1.923, 1.784 | 0.941 |
| T2 | 18.46 (5.944) | 19.55 (4.899) | 17.53 (6.600) | 2.028 | 2.042 (139) | 0.064, 3.991 | 0.043 4 | |
| T3 | 18.12 (4.554) | 19.23 (4.130) | 17.17 (4.709) | 2.060 | 2.739 (139) | 0.573, 3.547 | 0.007 4 | |
| T4 | 16.74 (4.788) | 17.82 (4.673) | 15.82 (4.721) | 2.000 | 2.519 (139) | 0.430, 3.569 | 0.013 4 | |
| Anxiety 2 | T1 | 7.88 (1.962) | 7.92 (1.753) | 7.84 (2.136) | 0.081 | 0.243 (139) | −0.577, 0.739 | 0.808 |
| T2 | 8.29 (2.113) | 8.69 (1.968) | 7.95 (2.184) | 0.745 | 2.112 (139) | 0.048, 1.442 | 0.036 4 | |
| T3 | 8.51 (2.260) | 9.26 (2.167) | 7.87 (2.150) | 1.393 | 3.821 (139) | 0.672, 2.114 | <0.001 4 | |
| T4 | 8.66 (2.390) | 9.60 (2.397) | 7.86 (2.083) | 1.745 | 4.625 (139) | 0.999, 2.491 | <0.001 4 | |
| Depression 3 | T1 | 12.65 (1.993) | 12.43 (1.936) | 12.84 (2.033) | −0.411 | −1.224 (139) | −1.076, 0.253 | 0.223 |
| T2 | 12.82 (2.212) | 12.75 (2.312) | 12.87 (2.138) | −0.115 | −0.306 (139) | −0.856, 0.627 | 0.760 | |
| T3 | 12.69 (1.979) | 12.40 (2.022) | 12.93 (1.921) | −0.534 | −1.607 (139) | −1.192, 0.123 | 0.110 | |
| T4 | 12.74 (2.086) | 12.23 (2.037) | 13.17 (2.042) | −0.940 | −2.729 (139) | −1.622, −0.259 | 0.007 4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roslan, N.R.; Mohd Fauzi, M.F.; Wan Teng, L.; Nur Azurah, A.G. Maternal Mental Health following Ultrasonographic Detection of Fetal Structural Anomaly in the Midst of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 12900. https://doi.org/10.3390/ijerph182412900
Roslan NR, Mohd Fauzi MF, Wan Teng L, Nur Azurah AG. Maternal Mental Health following Ultrasonographic Detection of Fetal Structural Anomaly in the Midst of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(24):12900. https://doi.org/10.3390/ijerph182412900
Chicago/Turabian StyleRoslan, Nur Rowaidah, Mohd Fadhli Mohd Fauzi, Lim Wan Teng, and Abdul Ghani Nur Azurah. 2021. "Maternal Mental Health following Ultrasonographic Detection of Fetal Structural Anomaly in the Midst of the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 24: 12900. https://doi.org/10.3390/ijerph182412900
APA StyleRoslan, N. R., Mohd Fauzi, M. F., Wan Teng, L., & Nur Azurah, A. G. (2021). Maternal Mental Health following Ultrasonographic Detection of Fetal Structural Anomaly in the Midst of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(24), 12900. https://doi.org/10.3390/ijerph182412900