
Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
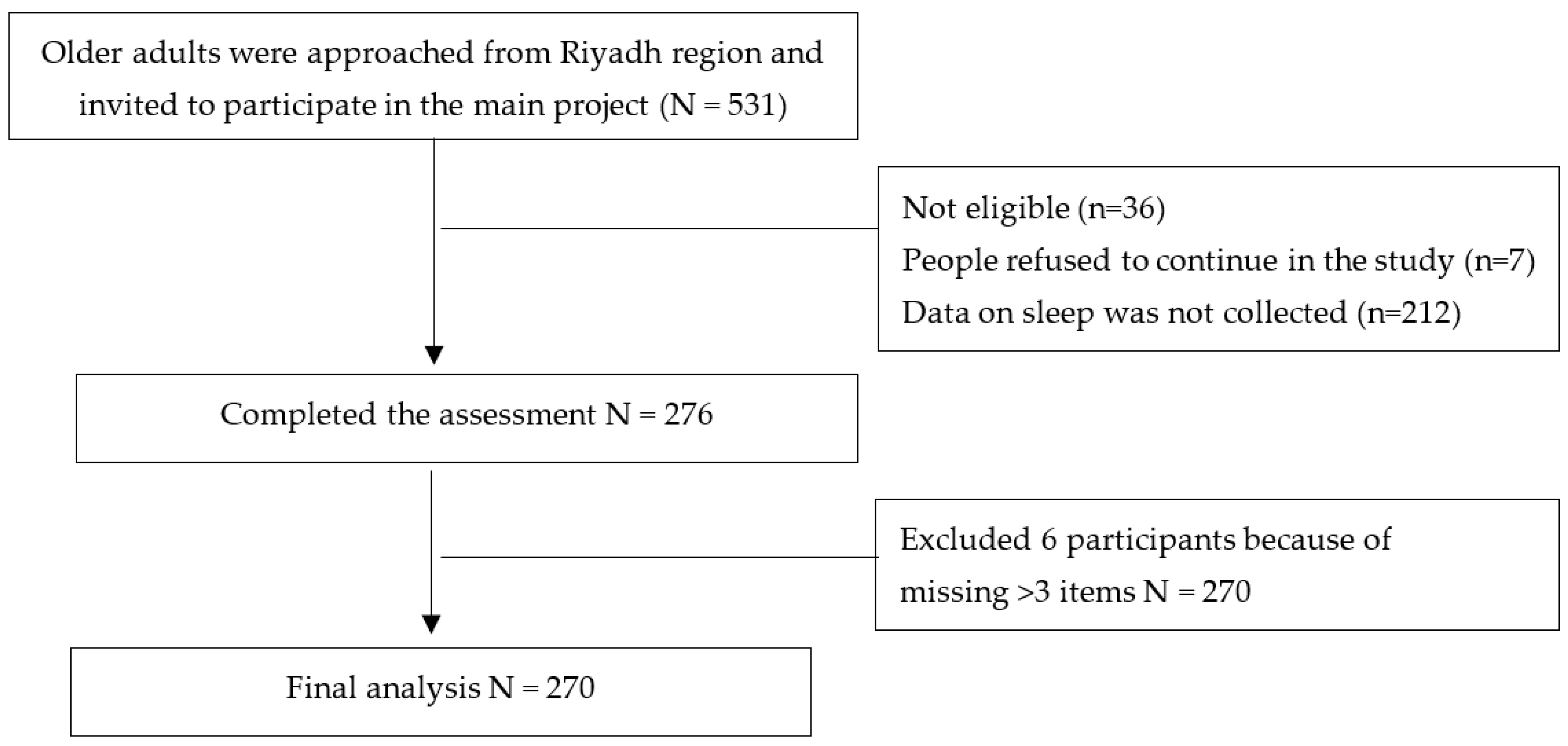
2.1. Study Design and Sample
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measures
2.3.1. Frailty
- Unintentional weight loss. This component was assessed by a self-report of unintentional weight loss of 10 pounds or more in the previous year.
- Exhaustion. This component was measured by answering two questions from the Center for Epidemiological Studies Depression scale, “I felt that everything I did was an effort” and “I could not get going”.
- Slowness. This component was defined by time taken to walk 15 feet (4.57 m), taking into account both gender and height.
- Weakness. Grip strength was measured, stratified by gender and Body Mass Index (BMI).
- Low physical activity. This component was defined as the rate of energy expenditure weekly, using questions from the Minnesota Leisure Time Activities Questionnaire [8].
2.3.2. Sleep Quality Measurements
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs PD. World Population Ageing 2017; United Nations: 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 30 November 2021).
- Alenazi, A.M.; Alhowimel, A.S.; Alotaibi, M.A.; Alqahtani, B.A.; Alshehri, M.M.; Alanazi, A.D.; Alanazi, A.A.; Alanazi, S.F.; Bindawas, S.M. Prevalence and incidence of osteoarthritis among people living in the Gulf Cooperation Council countries: A systematic review and meta-analysis. Clin. Rheumatol. 2021, 40, 3523–3531. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, B.A.; Alenazi, A.M.; Hoover, J.C.; Alshehri, M.M.; Alghamdi, M.S.; Osailan, A.M.; Khunti, K. Incidence of stroke among Saudi population: A systematic review and meta-analysis. Neurol. Sci. 2020, 41, 3099–3104. [Google Scholar] [CrossRef]
- Gangavati, A.; Hajjar, I.; Quach, L.; Jones, R.N.; Kiely, D.K.; Gagnon, P.; Lipsitz, L.A. Hypertension, Orthostatic Hypotension, and the Risk of Falls in a Community-Dwelling Elderly Population: The Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J. Am. Geriatr. Soc. 2011, 59, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Ensrud, K.E. Comparison of 2 Frailty Indexes for Prediction of Falls, Disability, Fractures, and Death in Older Women. Arch. Intern. Med. 2008, 168, 382. [Google Scholar] [CrossRef] [Green Version]
- Cawthon, P.M.; Marshall, L.M.; Michael, Y.; Dam, T.T.; Ensrud, K.E.; Barrett-Connor, E.; Orwoll, E.S. Frailty in older men: Prevalence, progression, and relationship with mortality. J. Am. Geriatr. Soc. 2007, 55, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Ageing [Highlights]. 2017 [cited 20 March 2018]. Available online: http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 30 November 2021).
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Siriwardhana, D.D.; Hardoon, S.; Rait, G.; Weerasinghe, M.C.; Walters, K.R. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle- income countries: A systematic review and meta-analysis. BMJ Open 2018, 8, e018195. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, B.A.; Alenazi, A.M.; Alshehri, M.M.; Osailan, A.M.; Alsubaie, S.F.; Alqahtani, M.A. Prevalence of frailty and associated factors among Saudi community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2021, 21, 185. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, B.A.; Nasser, T.A. Assessment of frailty in Saudi community-dwelling older adults: Validation of measurements. Ann. Saudi Med. 2019, 39, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtani, B.A.; Abdelbasset, W.K.; Alenazi, A.M. Psychometric analysis of the Arabic (Saudi) Tilburg Frailty Indicator among Saudi community-dwelling older adults. Arch. Gerontol. Geriatr. 2020, 90, 104128. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.K.; Fielding, R.A. Exercise as an intervention for frailty. Clin. Geriatr. Med. 2011, 27, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-C.; Su, T.-P.; Chou, P. A Nine-Year Follow-up Study of Sleep Patterns and Mortality in Community-Dwelling Older Adults in Taiwan. Sleep 2013, 36, 1187–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Li, L. Epidemiological study of sleep disorder in the elderly. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 988. [Google Scholar]
- Magnavita, N.; Garbarino, S. Sleep, health and wellness at work: A scoping review. Int. J. Environ. Res. Public Health 2017, 14, 1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbarino, S.; Lanteri, P.; Durando, P.; Magnavita, N.; Sannita, W.G. Co-morbidity, mortality, quality of life and the healthcare/welfare/social costs of disordered sleep: A rapid review. Int. J. Environ. Res. Public Health 2016, 13, 831. [Google Scholar] [CrossRef]
- He, M.; Deng, X.; Zhu, Y.; Huan, L.; Niu, W. The relationship between sleep duration and all-cause mortality in the older people: An updated and dose-response meta-analysis. BMC Public Health 2020, 20, 1179. [Google Scholar] [CrossRef]
- Vaz Fragoso, C.A.; Gahbauer, E.A.; Van Ness, P.H.; Gill, T.M. Sleep–wake disturbances and frailty in community-living older persons. J. Am. Geriatr. Soc. 2009, 57, 2094–2100. [Google Scholar] [CrossRef] [Green Version]
- Wai, J.L.; Yu, D.S. The relationship between sleep-wake disturbances and frailty among older adults: A systematic review. J. Adv. Nurs. 2020, 76, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Thichumpa, W.; Howteerakul, N.; Suwannapong, N.; Tantrakul, V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol. Health 2018, 40, e2018018. [Google Scholar] [CrossRef] [Green Version]
- Sukegawa, T.; Itoga, M.; Seno, H.; Miura, S.; Inagaki, T.; Saito, W.; Uegaki, J.; Miyaoka, T.; Momose, I.; Kasahara, K.; et al. Sleep disturbances and depression in the elderly in Japan. Psychiatry Clin. Neurosci. 2003, 57, 265–270. [Google Scholar] [CrossRef]
- Luo, J.; Zhu, G.; Zhao, Q.; Guo, Q.; Meng, H.; Hong, Z.; Ding, D. Prevalence and risk factors of poor sleep quality among Chinese elderly in an urban community: Results from the Shanghai aging study. PLoS ONE 2013, 8, e81261. [Google Scholar] [CrossRef] [Green Version]
- Endeshaw, Y.W.; Yoo, W. Association between social and physical activities and insomnia symptoms among community-dwelling older adults. J. Aging Health 2016, 28, 1073–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Yoo, M.S.; Bae, S.H. Prevalence and predictors of poor sleep quality in K orean older adults. Int. J. Nurs. Pract. 2013, 19, 116–123. [Google Scholar] [CrossRef]
- Zhang, B.; Wing, Y.K. Sex differences in insomnia: A meta-analysis. Sleep 2006, 29, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Blackwell, T.L.; Ancoli-Israel, S.; Redline, S.; Cawthon, P.M.; Paudel, M.L.; Dam, T.-T.L.; Stone, K.L. Sleep disturbances and risk of frailty and mortality in older men. Sleep Med. 2012, 13, 1217–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.-T.L.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L. Sleep disturbances and frailty status in older community-dwelling men. J. Am. Geriatr. Soc. 2009, 57, 2085–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, A.C.; Chen, L.H.; Tsai, C.C.; Chen, J.Y. Correlation between Sleep Quality and Frailty Status among Middle-Aged and Older Taiwanese People: A Community-Based, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 9457. [Google Scholar] [CrossRef]
- Fu, P.; Zhou, C.; Meng, Q. Associations of Sleep Quality and Frailty among the Older Adults with Chronic Disease in China: The Mediation Effect of Psychological Distress. Int. J. Environ. Res. Public Health 2020, 17, 5240. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Sedler, M.J.; Zambrano, M.; Nieves, J.L.; Cagino, K.; Fanning, K.D.; Milla-Martinez, M.F.; Castillo, P.R. The Effect of Age in the Association between Frailty and Poor Sleep Quality: A Population-Based Study in Community-Dwellers (The Atahualpa Project). J. Am. Med. Dir. Assoc. 2016, 17, 269–271. [Google Scholar] [CrossRef]
- Álvarez-Satta, M.; Berna-Erro, A.; Carrasco-Garcia, E.; Alberro, A.; Saenz-Antoñanzas, A.; Vergara, I.; Otaegui, D.; Matheu, A. Relevance of oxidative stress and inflammation in frailty based on human studies and mouse models. Aging Albany NY 2020, 12, 9982. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Mao, G.; Leng, S.X. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 43s. [Google Scholar]
- Grov, E.K.; Fosså, S.D.; Dahl, A.A. Insomnia in elderly cancer survivors—A population-based controlled study of associations with lifestyle, morbidity, and psychosocial factors. Results from the Health Survey of North-Trøndelag County (HUNT-2) Support. Care Cancer 2011, 19, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Wong, P.S.; Hasan, S.S.; Kairuz, T. The relationship between sleep quality, inappropriate medication use and frailty among older adults in aged care homes in Malaysia. PLoS ONE 2019, 14, e0224122. [Google Scholar] [CrossRef] [Green Version]
- Morgan, K.; Hartescu, I. Sleep duration and all-cause mortality: Links to physical activity and prefrailty in a 27-year follow up of older adults in the UK. Sleep Med. 2019, 54, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Pourmotabbed, A.; Ghaedi, E.; Babaei, A.; Mohammadi, H.; Khazaie, H.; Jalili, C.; Symonds, M.E.; Moradi, S. Sleep duration and sarcopenia risk: A systematic review and dose-response meta-analysis. Sleep Breath. 2020, 24, 1267–1278. [Google Scholar] [CrossRef]
- Cooper, C.; Dere, W.; Evans, W.; Kanis, J.A.; Rizzoli, R.; Sayer, A.A.; Sieber, C.; Kaufman, J.-M.; Van Kan, G.A.; Boonen, S. Frailty and sarcopenia: Definitions and outcome parameters. Osteoporos. Int. 2012, 23, 1839s–1848s. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Total Sample N = 270 (%) | Frailty Status, n (%) | p | ||
|---|---|---|---|---|---|
| Robust | Pre-Frail | Frail | |||
| Age groups a | |||||
| 60–69 | 129 (47.6) | 36 (27.9) | 71 (55) | 22 (17) | <0.001 |
| ≥70 | 141 (52) | 53(37.5) | 31 (22.6) | 57 (39.7) | |
| Gender a | |||||
| Male | 176 (65.2) | 56 (31.8) | 65 (36.9) | 55 (31.2) | 0.503 |
| Female | 94 (34.8) | 33 (35.1) | 37 (40.4) | 24 (24.4) | |
| Education a | |||||
| Primary school | 160 (59) | 55 (34.4) | 57 (35.6) | 48 (30) | <0.001 |
| Secondaryschool | 68 (25.1) | 35 (51.4) | 23 (35.2) | 10 (13.2) | |
| College | 42 (15.5) | 21 50) | 13 (30.9) | 8(19) | |
| Marital status a | |||||
| Married | 169 (62.4) | 64 (37.9) | 67 (39.6) | 38 (22.4) | <0.001 |
| Single/widowed/divorced | 101 (37.3) | 25 (24.7) | 35 (35.6) | 41 (39.6) | |
| Living arrangement a | |||||
| Living with others | 237 (87.5) | 82(34.5) | 89 (37.5) | 66 (27.8) | 0.051 |
| Living alone | 33 (12.2) | 7(21.2) | 13 (42.4) | 13 (36.S) | |
| Number of chronic conditions a | |||||
| <3 | 183 (67.7) | 64 (34.9) | 81 (44.2) | 38 (20.7) | <0.001 |
| ≥3 | 87(32.2) | 25 (28.7) | 21 (25.2) | 41 (45.9) | |
| Grip strength, mean (SD) | 270 | 24.66 (12.2) | 21.01 (11.02) | 20.2 (7.5) | <0.001 |
| BMI (kgm−2), mean (SD) b | 236 | 27.8 (4.4) | 26.5 (4.8) | 24.4 (5.5) | <0.001 |
| MMSE score a | |||||
| Normal (>24) | 182 (67.4) | 74 (40.6) | 76 (2.3) | 32 (17.1) | <0.001 |
| Impaired (<24) | 88 (32.5) | 15 (17.1) | 26 (29.5) | 47 (53.4) | |
| Subjective sleep qualitya | |||||
| PSQI score ≤ 5 | 92 (34.1) | 44(47.8) | 36 (39.1) | 12 (13.1) | <0.001 |
| PSQI score > 5 | 178 (65.9) | 45 (25.2) | 66 (37.1) | 67 (37.6) | |
| Mean PSQI score (SD) | 5.8 (2.3) | 7.3 (1.6) | 8.1(2) | ||
| Subjective Sleep Quality | Crude Model | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Pre-frail | Ref. | Ref. | Ref. | |||
| PSQI score ≤ 5 (ref) | ||||||
| PSQI score > 5 | 1.83 * | (1.1–3.2) | 1.73 * | (1.42–2.12) | 1.67 * | (1.26–2.05) |
| Frail | Ref. | Ref. | Ref. | |||
| PSQI score ≤ 5 (ref) | ||||||
| PSQI score > 5 | 2.44 * | (1.28–4.63) | 2.21 * | (1.18–4.11) | 2.13 * | (1.47–3.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, B.A. Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12741. https://doi.org/10.3390/ijerph182312741
Alqahtani BA. Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12741. https://doi.org/10.3390/ijerph182312741
Chicago/Turabian StyleAlqahtani, Bader A. 2021. "Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 23: 12741. https://doi.org/10.3390/ijerph182312741
APA StyleAlqahtani, B. A. (2021). Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(23), 12741. https://doi.org/10.3390/ijerph182312741