
Psychological and Physical Distress in Italian People during COVID-19 Pandemic: One Year Later

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Analysis
4. Results
General Information
5. Perception of the COVID Pandemic
6. Psychological Impact
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Contini, C.; Di Nuzzo, M.; Barp, N.; Bonazza, A.; De Giorgio, R.; Tognon, M.; Rubino, S. The novel zoonotic COVID-19 pandemic: An expected global health concern. J. Infect. Dev. Ctries. 2020, 14, 254–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porcheddu, R.; Serra, C.; Kelvin, D.; Kelvin, N.; Rubino, S. Similarity in Case Fatality Rates (CFR) of COVID-19/SARS-CoV-2 in Italy and China. J. Infect. Dev. Ctries. 2020, 14, 125–128. [Google Scholar] [CrossRef]
- Sun, P.; Lu, X.; Xu, C.; Sun, W.; Pan, B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551. [Google Scholar] [CrossRef]
- Hageman, J.R. The Coronavirus Disease 2019 (COVID-19). Paediatr. Ann. 2020, 49, e99–e100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Kock, R.A.; Karesh, W.B.; Veas, F.; Velavan, T.P.; Simons, D.; Mboera, L.E.G.; Dar, O.; Arruda, L.B.; Zumla, A. 2019 n-Cov in context: Lessons learned? Lancet Planet Health 2020, 4, e87–e88. [Google Scholar] [CrossRef] [Green Version]
- Mackenzi, J.S.; Smith, D.W. COVID-19: A novel zoonotic disease caused by a coronavirus from China: What we know and what we don’t. Microbiol. Aust. 2020, 41, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Harrel, S.K.; Molinari, J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J. Am. Dent. Assoc. 2004, 135, 429–437. [Google Scholar] [CrossRef]
- Checchi, V.; Bellini, P.; Bencivenni, D.; Consolo, U. COVID-19 dentistry-related aspects: A literature overview. Int. Dent. J. 2021, 71, 21–26. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for clinical dental care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Ministero della Salute, Elaborazione e Gestione dati a cura del Dipartimento della Protezione Civile. 2020. Available online: https://emergenze.protezionecivile.gov.it/it/sanitarie/coronavirus (accessed on 18 August 2021).
- WHO. Global Infection Prevention and Control Network Infection Prevention and Control during Health Care when COVID-19 Is Suspected. Available online: https://www.who.int/publications/i/item/10665-331495 (accessed on 5 April 2020).
- WHO (World Health Organization). Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance. 2020. Available online: https://apps.who.int/iris/handle/10665/331446 (accessed on 13 March 2020).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA—J. Am. Med. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) in dentistry. Management of biological risk in dental practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [Google Scholar] [CrossRef] [PubMed]
- Gralinski, L.E.; Menachery, V.D. Return of the coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [Green Version]
- WHO (World Health Organization). Coronavirus Disease (COVID-19) Advice for the Public. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 29 April 2020).
- WHO (World Health Organization). Mental Health and COVID-19. 2020. Available online: https://www.who.int/teams/mental-health-and-substance-use/covid-19 (accessed on 8 April 2020).
- Vinkers, C.H.; Van Amelsvoort, T.; Bisson, J.I.; Branchi, I.; Cryan, J.F.; Domschke, K.; Howes, O.D.; Manchia, M.; Pinto, L.; de Quervain, D.; et al. Stress resilience during the coronavirus pandemic. Eur. Neuropsychopharmacol. 2020, 35, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, A.; Horodynski, M.; Serritella, E.; Romeo, U.; Barbato, E.; Galluccio, G. Three-dimensional evaluation of dental movement in orthodontics|Valutazione tridimensionale del movimento dentale in ortodonzia. J. Dent. Cadmos. 2020, 88, 182–190. [Google Scholar] [CrossRef]
- Putrino, A.; Impellizzeri, A.; Pavese, L.; Barbato, E.; Galluccio, G. Orthodontic treatment and third molars development: Longitudinal study on radiographs|Trattamento ortodontico e sviluppo dei terzi molari: Studio longitudinale su radiografie. J. Dent. Cadmos. 2019, 87, 558–570. [Google Scholar] [CrossRef]
- Ammar, N.; Aly, N.M.; Folayan, M.O.; Khader, Y.; Virtanen, J.I.; Al-Batayneh, O.B.; Mohebbi, S.Z.; Attia, S.; Howaldt, H.P.; Boettger, S.; et al. Behavior changes due to COVID-19 among dental academics—The theory of planned behavior: Stresses, worries, training, and pandemic severity. PLoS ONE 2020, 15, e0239961. [Google Scholar]
- Impellizzeri, A.; Di Benedetto, S.; De Stefano, A.; Guercio-Monaco, E.; Barbato, E.; Galluccio, G. General health & psychological distress in children with temporomandibular disorder. Case Rep. Clin. Ter. 2019, 170, e321–e327. [Google Scholar]
- Marotta, L.; Pesce, A.; Guazzini, A. Before and after the Quarantine: An Approximate Study on the Psychological Impact of COVID-19 on the Italian Population during the Lockdown Period. Future Internet 2020, 12, 229. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatr. 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P.A. Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Sex | Male | 523 | 25 |
| Female | 1552 | 75 | |
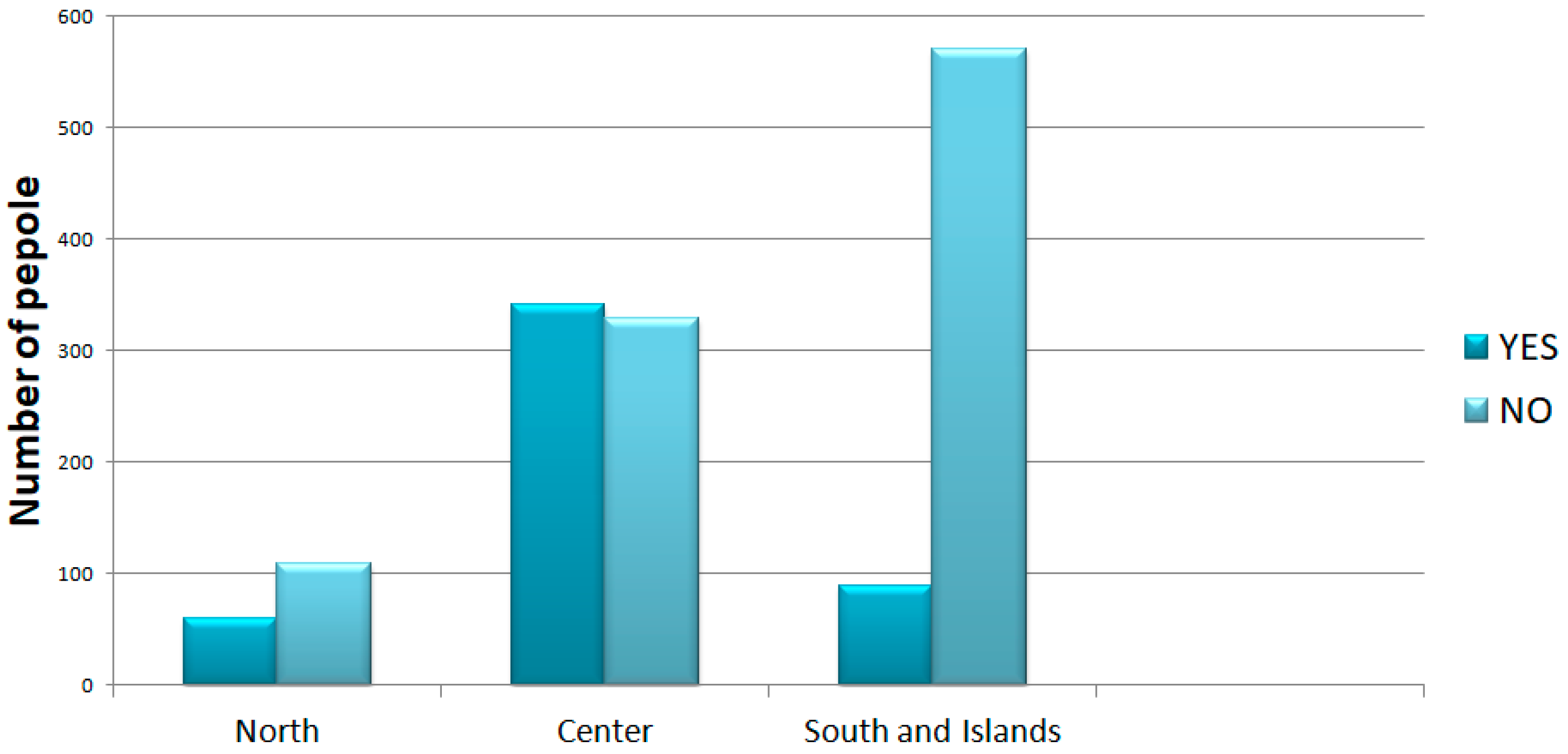
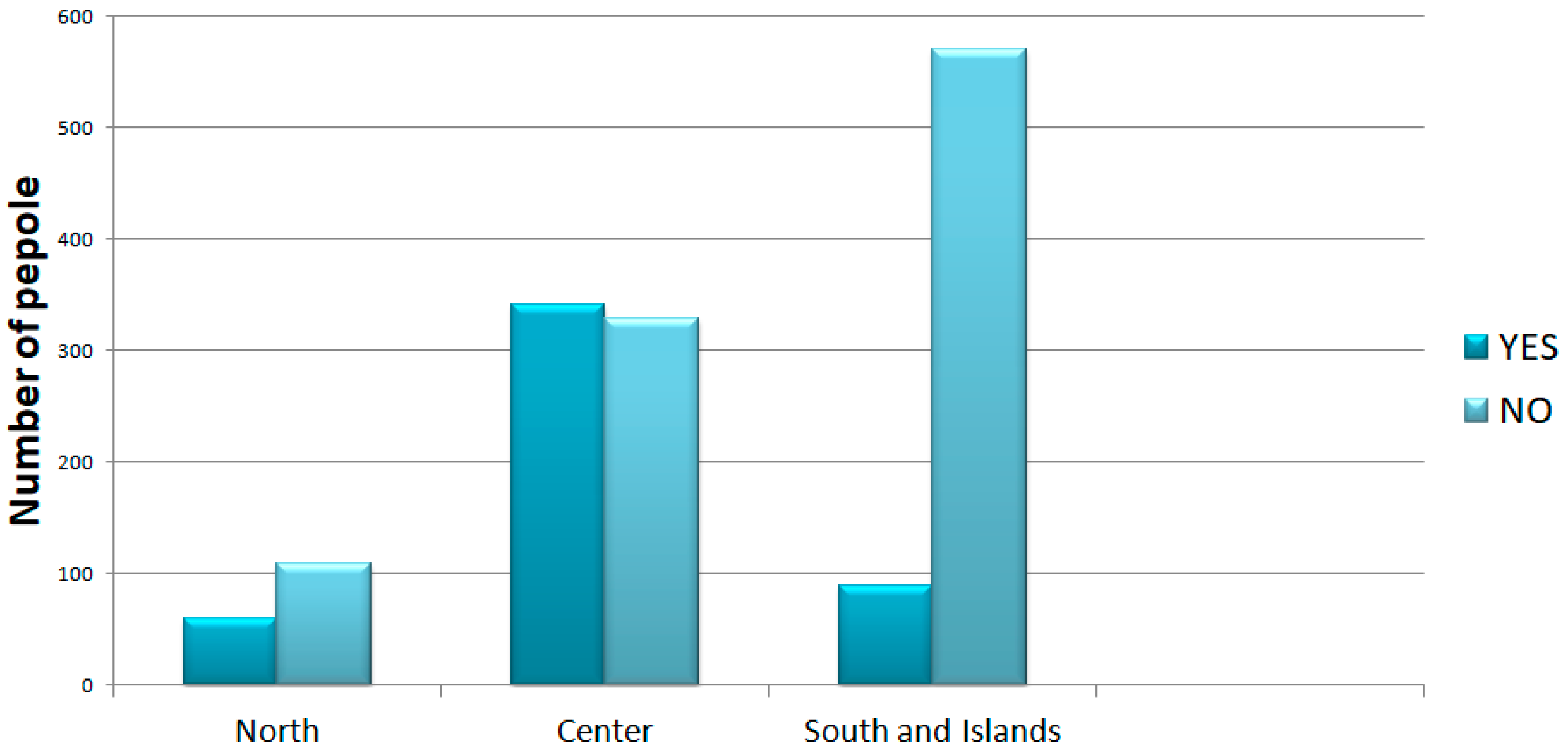
| Regions of Italy | North | 317 | 15.3 |
| Center | 1027 | 49.5 | |
| South and Islands | 731 | 35.2 | |
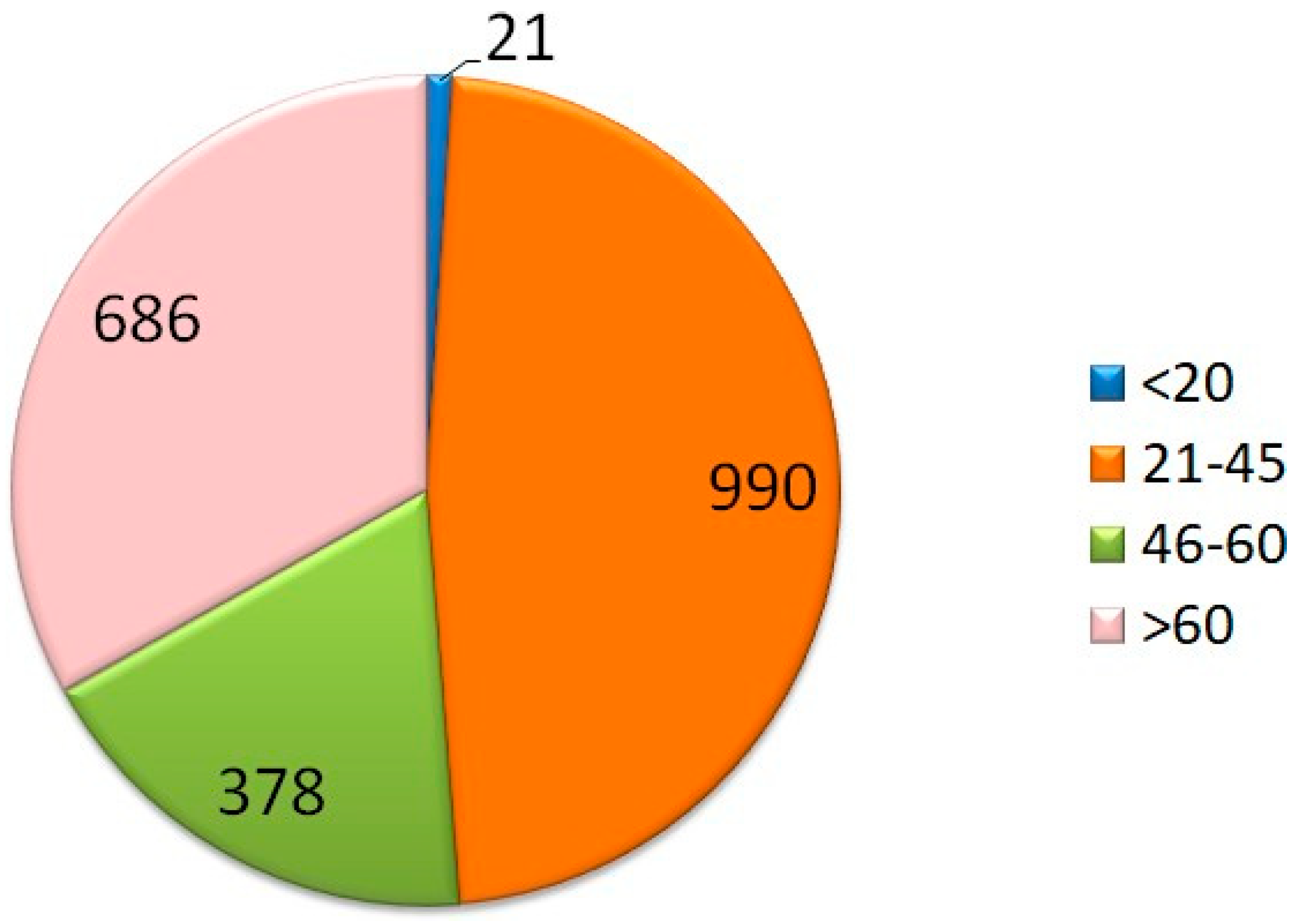
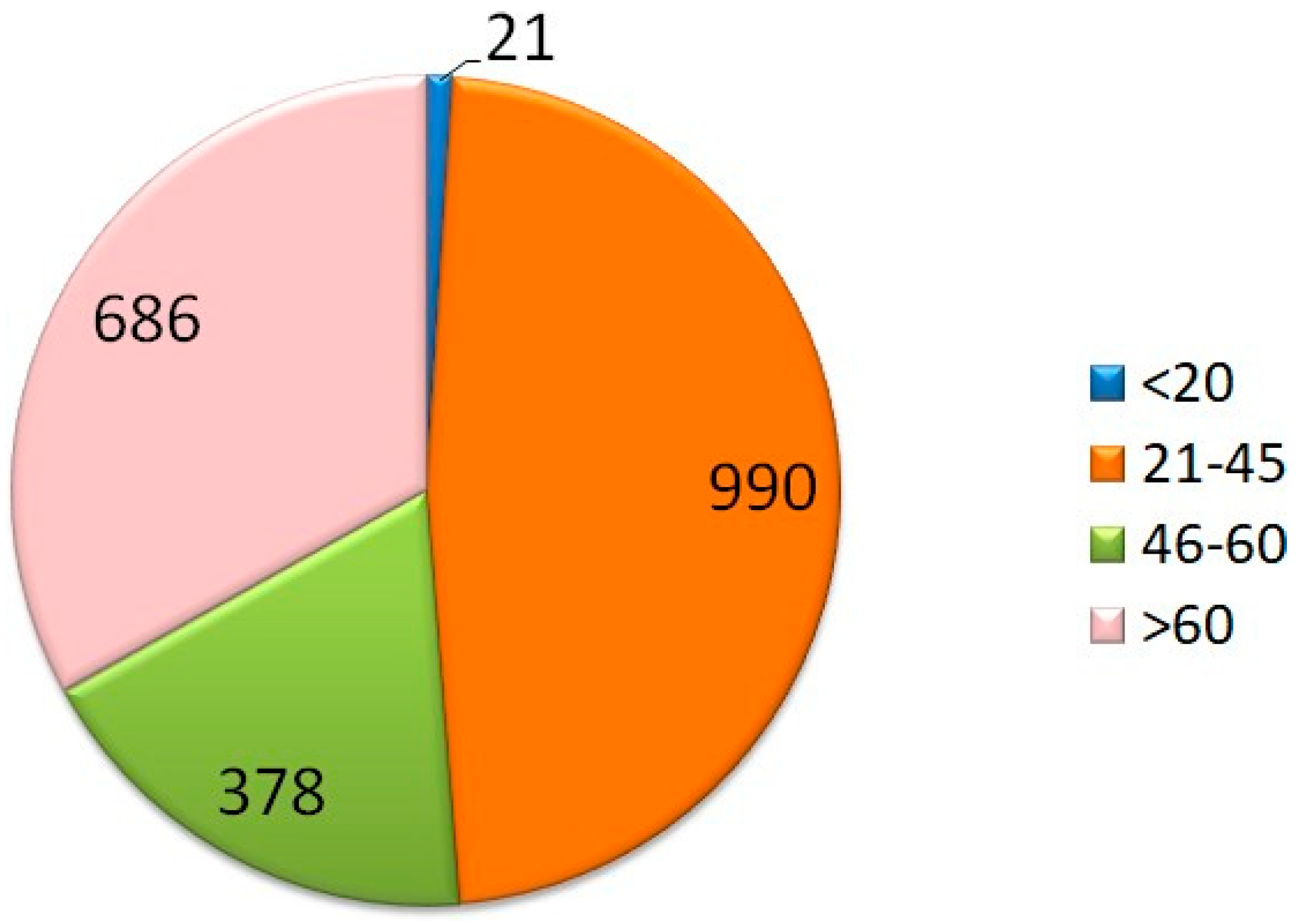
| Age (years) | <20 | 52 | 2.5 |
| 21–45 | 1210 | 60.3 | |
| 46–60 | 527 | 26.3 | |
| >60 | 220 | 10.9 | |
| Work | Freelancer Employee/HousewifeOther | 468 | 22.5 |
| 953 | 45.9 | ||
| 149 | 7.1 | ||
| 506 | 24.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Impellizzeri, A.; Dilucca, M.; Squillace, F.; Guarnieri, R.; Polimeni, A.; Galluccio, G. Psychological and Physical Distress in Italian People during COVID-19 Pandemic: One Year Later. Int. J. Environ. Res. Public Health 2021, 18, 12525. https://doi.org/10.3390/ijerph182312525
Impellizzeri A, Dilucca M, Squillace F, Guarnieri R, Polimeni A, Galluccio G. Psychological and Physical Distress in Italian People during COVID-19 Pandemic: One Year Later. International Journal of Environmental Research and Public Health. 2021; 18(23):12525. https://doi.org/10.3390/ijerph182312525
Chicago/Turabian StyleImpellizzeri, Alessandra, Maddalena Dilucca, Francesca Squillace, Rosanna Guarnieri, Antonella Polimeni, and Gabriella Galluccio. 2021. "Psychological and Physical Distress in Italian People during COVID-19 Pandemic: One Year Later" International Journal of Environmental Research and Public Health 18, no. 23: 12525. https://doi.org/10.3390/ijerph182312525
APA StyleImpellizzeri, A., Dilucca, M., Squillace, F., Guarnieri, R., Polimeni, A., & Galluccio, G. (2021). Psychological and Physical Distress in Italian People during COVID-19 Pandemic: One Year Later. International Journal of Environmental Research and Public Health, 18(23), 12525. https://doi.org/10.3390/ijerph182312525