
A Narrative Literature Review of Bias in Collecting Patient Reported Outcomes Measures (PROMs)


Abstract
:1. Introduction
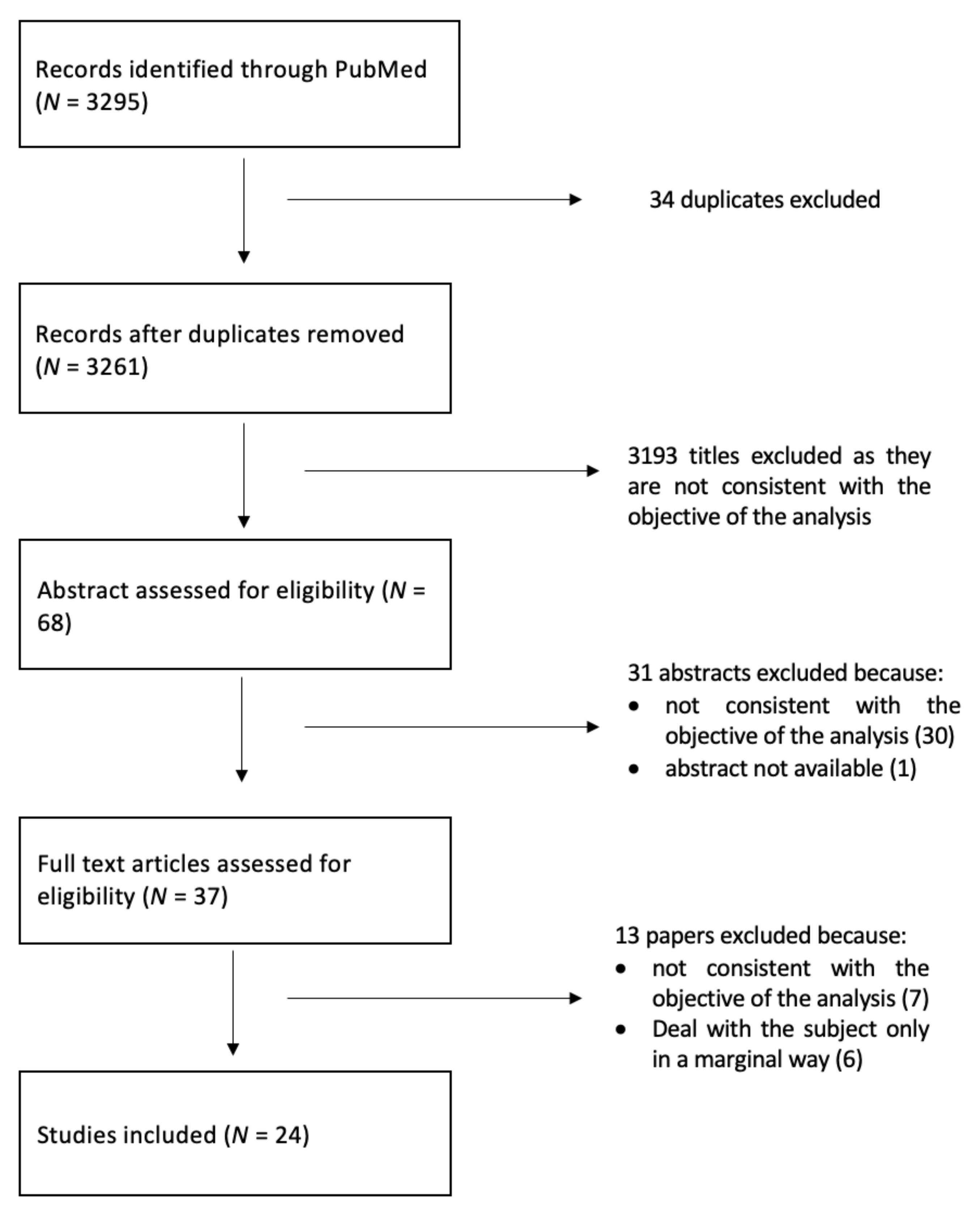
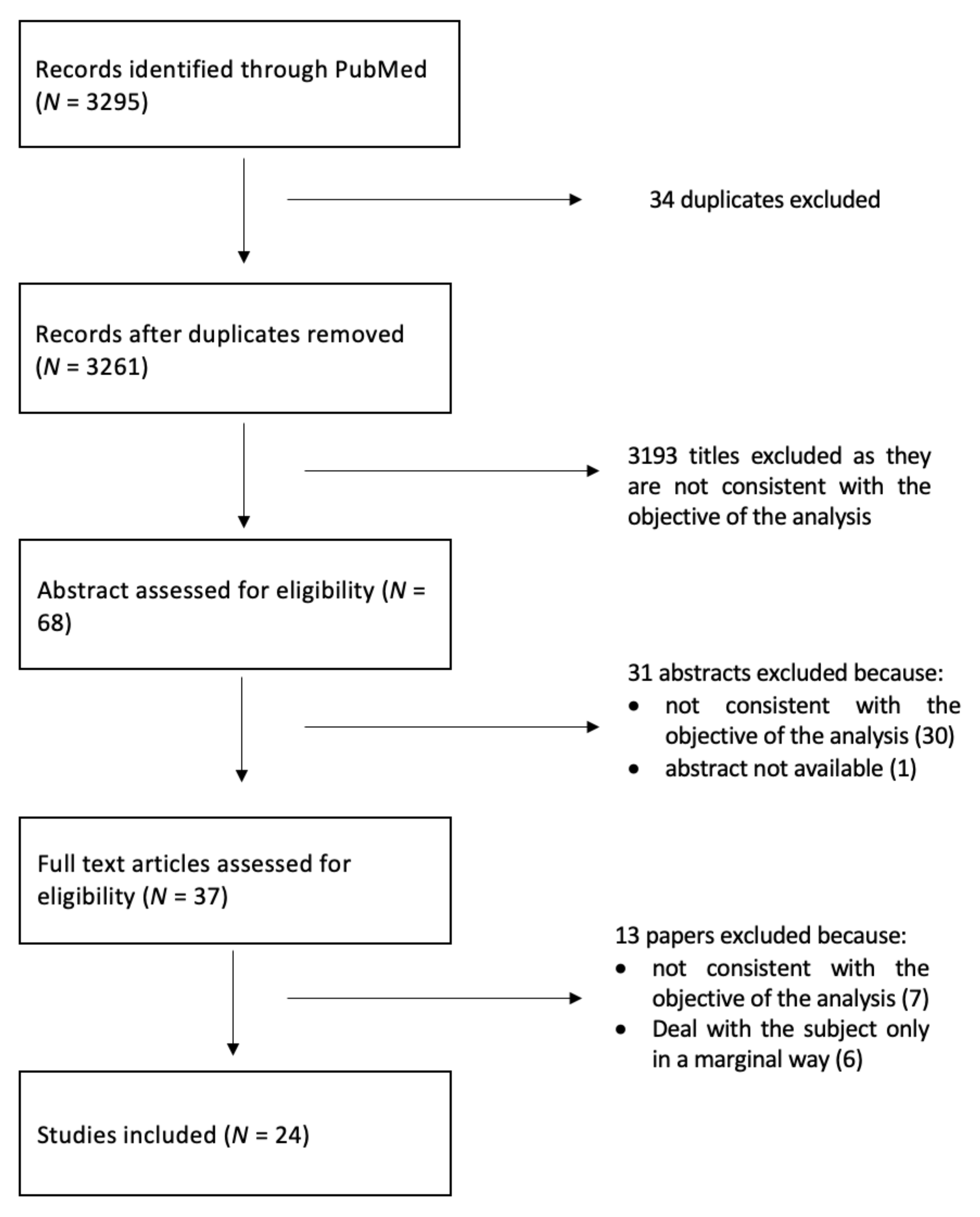
2. Materials and Methods
3. Results
3.1. Collection Mode Related Bias
3.2. Non-Response Bias
3.3. Proxy/Caregiver Response Bias
3.4. Recall Bias
3.5. Language Bias
3.6. Timing Bias
3.7. Fatigue Bias
4. Discussion
- They are formulated in the most accurate way, in order to avoid language bias;
- They are not too long, to minimize fatigue bias;
- The questions are objective and referred to as observable facts, so that caregivers can also answer them in a reliable way.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- FDA. Guidance for Industry Patient-Reported Outcome Measures: Use in Medical Product Development to Support. Labeling Claims; FDA: Silver Spring, MD, USA, 2009; p. 2.
- Weldring, T.; Smith, S.M. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, D.C.; Chenok, K.E.; Love, R.M.; Petersen, C.; Holve, E.; Segal, C.D.; Franklin, P.D. Incorporating patient-reported out-comes into health care to engage patients and enhance care. Health Aff. 2006, 35, 575–582. [Google Scholar] [CrossRef]
- Devlin, N.J.; Appleby, J. Getting the Most Out of PROMs: Putting Health Outcomes at the Heart of NHS Decision Making; King’s Fund: London, UK, 2010. [Google Scholar]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Cabitza, F.; Dui, L.G. Collecting Patient Reported Outcomes in the Wild: Opportunities and Challenges. Stud. Health Technol. Inform. 2018, 247, 36–40. [Google Scholar] [PubMed]
- Cabitza, F.; Dui, L.G.; Banfi, G. PROs in the wild: Assessing the validity of patient reported outcomes in an electronic registry. Comput. Methods Programs Biomed. 2019, 181, 104837. [Google Scholar] [CrossRef] [Green Version]
- Hammarstedt, J.E.; Redmond, J.M.; Gupta, A.; Dunne, K.F.; Vemula, S.P.; Domb, B.G. Survey mode influence on patient-reported outcome scores in orthopaedic surgery: Telephone results may be positively biased. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Schilling, C.; Dowsey, M.; Clarke, P.; Choong, P. Using Patient-Reported Outcomes for Economic Evaluation: Getting the Timing Right. Value Health 2016, 19, 945–950. [Google Scholar] [CrossRef]
- Karela, M.; Rickard, L.; Roussou, E. The Semantics of ‘Hip Pain’ and its Impact on Clinical Practice in Patient-Reported Outcome Measures (PROMs) of Disease: Results from a Clinical and Radiological Evaluation Cohort. Mediterr. J. Rheumatol. 2020, 31, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Péchon, P.H.M.; Butler, K.; Murphy, G.; Singer, G.C. The perils of PROMs: Question 5 of the Oxford Hip Score is ambiguous to 10% of English-speaking patients: A survey of 135 patients. HIP Int. 2018, 29, 299–302. [Google Scholar] [CrossRef]
- Polk, A.; Rasmussen, J.V.; Brorson, S.; Olsen, B.S. Reliability of patient-reported functional outcome in a joint replacement registry. A comparison of primary responders and non-responders in the Danish Shoulder Arthroplasty Registry. Acta Orthop. 2013, 84, 12–17. [Google Scholar] [CrossRef]
- Chen, D.A.; Vaishnav, A.S.; Louie, P.K.; Gang, C.H.; McAnany, S.J.; Iyer, S.; Albert, T.J.; Qureshi, S.A. Patient Reported Outcomes in Patients Who Stop Following Up: Are They Doing Better or Worse Than the Patients That Come Back? Spine 2020, 45, 1435–1442. [Google Scholar] [CrossRef]
- Lindman, I.; Olsson, H.; Öhlin, A.; Senorski, E.H.; Stålman, A.; Ayeni, O.R.; Sansone, M. Loss to follow-up: Initial non-responders do not differ from responders in terms of 2-year outcome in a hip arthroscopy registry. J. Hip Preserv. Surg. 2020, 7, 281–287. [Google Scholar] [CrossRef]
- Acosta, J.; Tang, P.; Regal, S.; Akhavan, S.; Reynolds, A.; Schorr, R.; Hammarstedt, J.E. Investigating the Bias in Orthopaedic Patient-reported Outcome Measures by Mode of Administration: A Meta-analysis. JAAOS Glob. Res. Rev. 2020, 4, e20.00194. [Google Scholar] [CrossRef]
- Lapin, B.R.; Thompson, N.R.; Schuster, A.; Katzan, I.L. Magnitude and Variability of Stroke Patient-Proxy Disagreement Across Multiple Health Domains. Arch. Phys. Med. Rehabil. 2021, 102, 440–447. [Google Scholar] [CrossRef]
- Richter, J.G.; Nannen, C.; Chehab, G.; Acar, H.; Becker, A.; Willers, R.; Huscher, D.; Schneider, M. Mobile App-based documentation of patient-reported outcomes—3-months results from a proof-of-concept study on modern rheumatology patient management. Arthritis Res. 2021, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Imam, M.A.; Barke, S.; Stafford, G.H.; Parkin, D.; Field, R.E. Loss to follow-up after total hip replacement: A source of bias in patient reported outcome measures and registry datasets? HIP Int. 2014, 24, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Schröder, M.L.; de Wispelaere, M.P.; Staartjes, V.E. Are patient-reported outcome measures biased by method of follow-up? Evaluating paper-based and digital follow-up after lumbar fusion surgery. Spine J. 2019, 19, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.N.; Hofmann, M.R.; Schwarzkopf, R.; Pourmand, D.; Bhatia, N.N.; Rafijah, G.; Bederman, S.S. Patient-Reported Outcome Measures: How Do Digital Tablets Stack Up to Paper Forms? A Randomized, Controlled Study. Am. J. Orthop. 2016, 45, E451–E457. [Google Scholar]
- Rutherford, C.; Costa, D.; Mercieca-Bebber, R.; Rice, H.; Gabb, L.; King, M. Mode of administration does not cause bias in patient-reported outcome results: A meta-analysis. Qual. Life Res. 2016, 25, 559–574. [Google Scholar] [CrossRef]
- Kim, J.; Lonner, J.H.; Nelson, C.L.; Lotke, P.A. Response bias: Effect on outcomes evaluation by mail surveys after total knee ar-throplasty. J. Bone Joint Surg. Am. 2004, 86, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, A.; Frie, K.G.; Neuburger, J.; van der Meulen, J.; Black, N. Late response to patient-reported outcome questionnaires after surgery was associated with worse outcome. J. Clin. Epidemiol. 2013, 66, 218–225. [Google Scholar] [CrossRef]
- Aleem, I.S.; Duncan, J.; Ahmed, A.M.; Zarrabian, M.; Eck, J.; Rhee, J.; Clarke, M.; Currier, B.L.; Nassr, A. Do Lumbar Decompression and Fusion Patients Recall Their Preoperative Status? Spine 2017, 42, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Hofstedt, O.; Di Giuseppe, D.; Alenius, G.-M.; Stattin, N.; Forsblad-D’Elia, H.; Ljung, L. Comparison of agreement between internet-based registration of patient-reported outcomes and clinic-based paper forms within the Swedish Rheumatology Quality Register. Scand. J. Rheumatol. 2019, 48, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Nebreda, M.L.; Heng, M.; Rosner, B.; McTague, M.; Javedan, H.; Harris, M.B.; Weaver, M.J. Reliability of Proxy-reported Patient-reported Outcomes Measurement Information System Physical Function and Pain Interference Responses for Elderly Patients with Musculoskeletal Injury. J. Am. Acad. Orthop. Surg. 2019, 27, e156–e165. [Google Scholar] [CrossRef]
- Li, M.; Harris, I.; Lu, Z.K. Differences in proxy-reported and patient-reported outcomes: Assessing health and functional status among medicare beneficiaries. BMC Med. Res. Methodol. 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Aleem, I.S.; Currier, B.L.; Yaszemski, M.J.; Poppendeck, H.; Huddleston, P.; Eck, J.; Rhee, J.; Bydon, M.; Freedman, B.; Nassr, A. Do Cervical Spine Surgery Patients Recall Their Preoperative Status? Clin. Spine Surg. 2018, 31, E481–E487. [Google Scholar] [CrossRef]
- Kwong, E.; Black, N. Retrospectively patient-reported pre-event health status showed strong association and agreement with contemporaneous reports. J. Clin. Epidemiol. 2017, 81, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Neumann, P.J.; Sm, S.S.A.; Gutterman, E.M. The Use of Proxy Respondents in Studies of Older Adults: Lessons, Challenges, and Opportunities. J. Am. Geriatr. Soc. 2000, 48, 1646–1654. [Google Scholar] [CrossRef]
- Sneeuw, K.C.; Sprangers, M.A.; Aaronson, N.K. The role of health care providers and significant others in evaluating the quality of life of patients with chronic disease. J. Clin. Epidemiol. 2002, 55, 1130–1143. [Google Scholar] [CrossRef]
- Schmier, J.K.; Halpern, M.T. Patient recall and recall bias of health state and health status. Expert Rev. Pharm. Outcomes Res. 2004, 4, 159–163. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
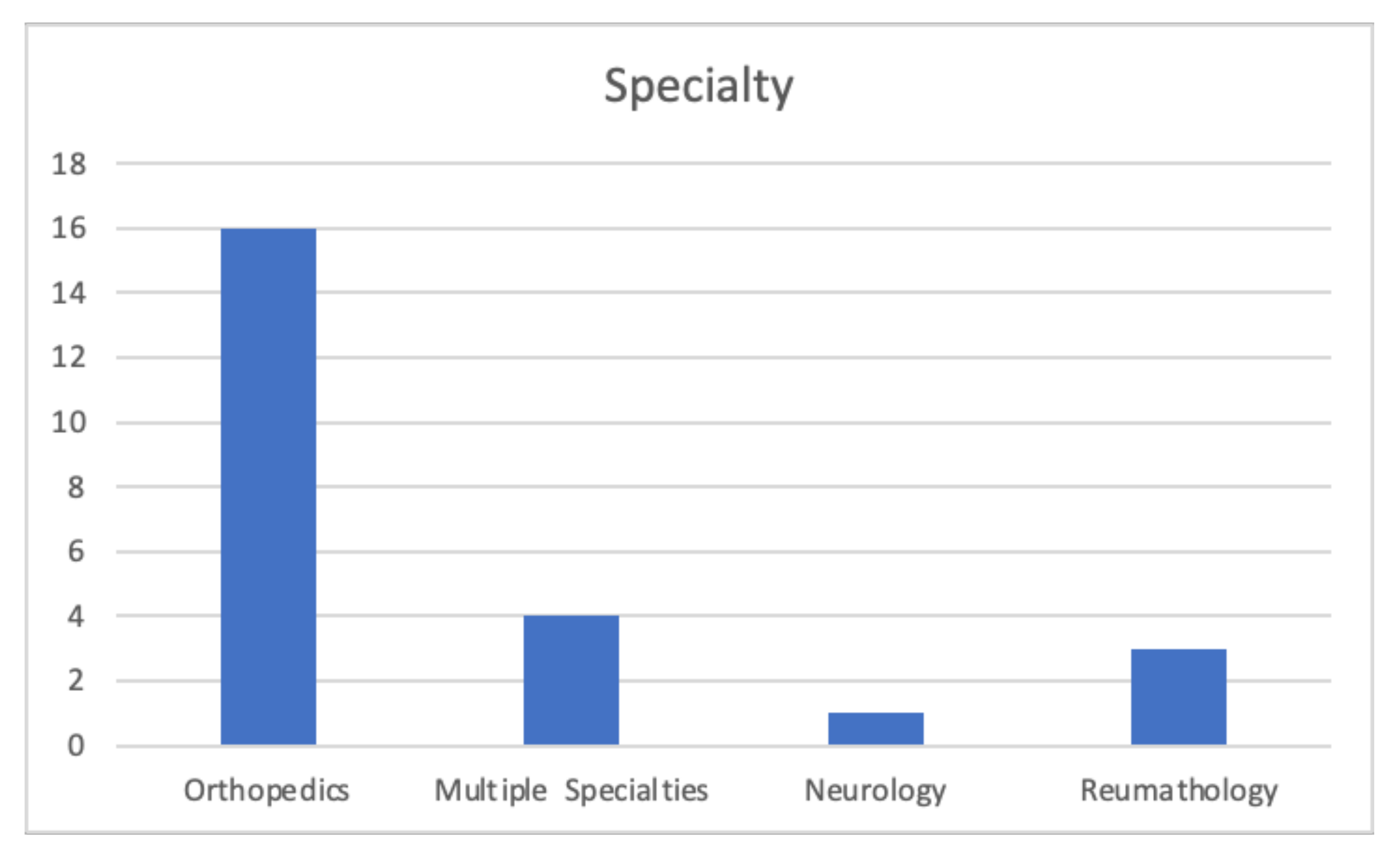
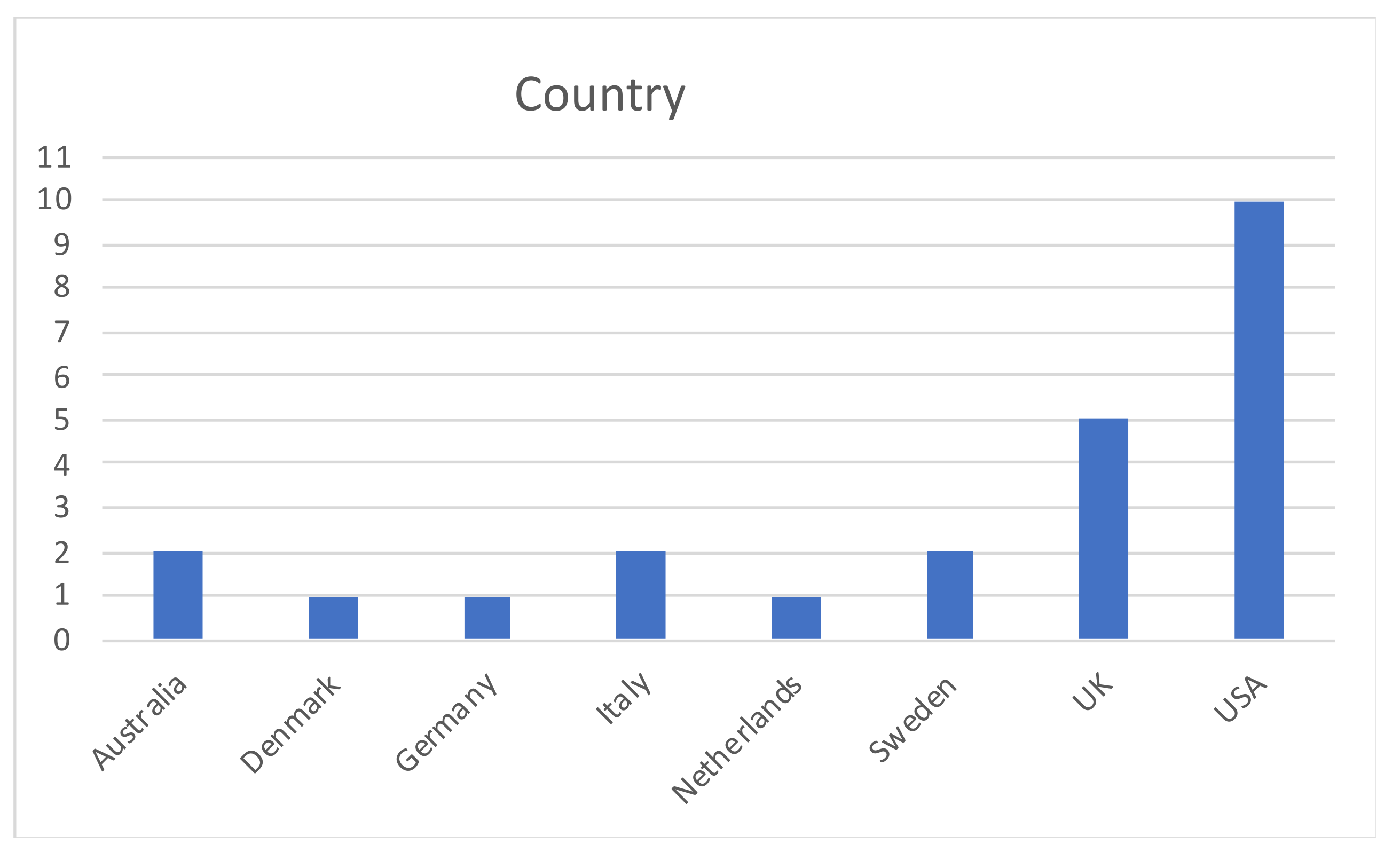
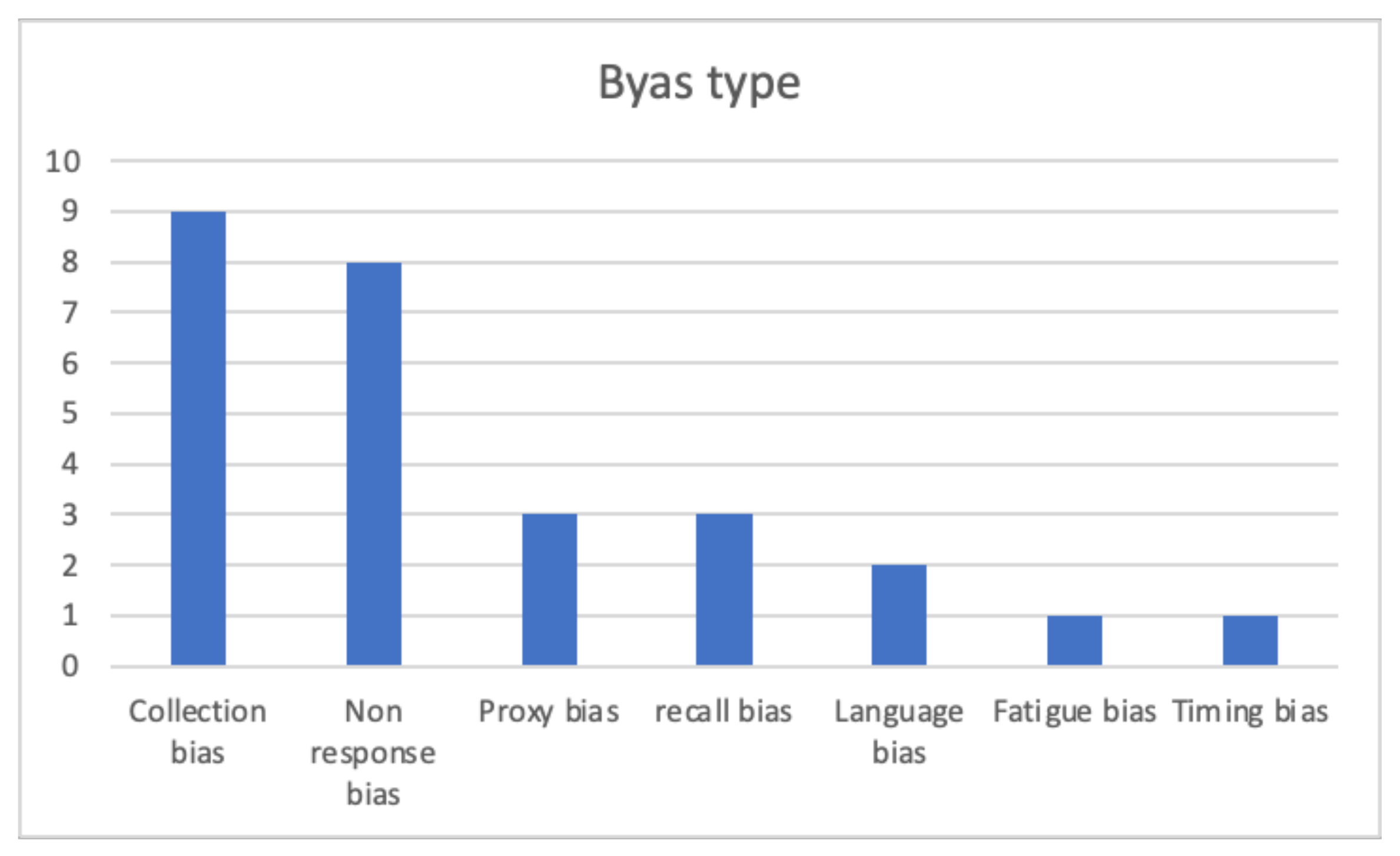
| First Author | Year | Country | Bias | Specialty |
|---|---|---|---|---|
| Cabitza [6] | 2018 | Italy | Non-response bias, collection bias | Orthopedics |
| Cabitza [7] | 2019 | Italy | Non-response bias, collection bias, fatigue bias | Orthopedics |
| Hammarstedt [8] | 2017 | USA | Collection bias | Orthopedics |
| Schilling [9] | 2016 | Australia | Timing bias | Orthopedics |
| Karela [10] | 2020 | UK | Language bias | Rheumatology |
| Péchon [11] | 2019 | UK | Language bias | Orthopedics |
| Polk [12] | 2013 | Denmark | Non response bias | Orthopedics |
| Chen [13] | 2020 | USA | Non response bias | Orthopedics |
| Lindman [14] | 2020 | Sweden | Non response bias | Orthopedics |
| Acosta [15] | 2020 | USA | Collection bias | Orthopedics |
| Lapin BR [16] | 2021 | USA | Proxy bias | Neurology |
| Richter [17] | 2021 | Germany | Collection bias | Rheumatology |
| Imam [18] | 2014 | UK | Non response bias | Orthopedics |
| Schröder [19] | 2019 | Netherlands | Collection bias | Orthopedics |
| Shah [20] | 2016 | USA | Collection bias | Orthopedics |
| Rutherford [21] | 2016 | Australia | Collection bias | Multiple specialties |
| Kim [22] | 2004 | USA | Non response bias | Orthopedics |
| Hutchings [23] | 2013 | UK | Non response bias | Multiple specialties |
| Aleem [24] | 2017 | USA | Recall bias | Orthopedics |
| Hofstedt [25] | 2019 | Sweden | Collection bias | Rheumatology |
| Alvarez-Nebreda [26] | 2019 | USA | Proxy bias | Orthopedics |
| Li [27] | 2015 | USA | Proxy bias | Multiple specialties |
| Aleem [28] | 2018 | USA | Recall bias | Orthopedics |
| Kwong [29] | 2016 | UK | Recall bias | Multiple specialties |
| 1st Author | Collection Methods | Results |
|---|---|---|
| Cabitza [6] | Electronic/Online (self-administrated) Telephone (with interviewer) | Collection methods can bias PROM scores: Scores reported on the phone are better than the ones reported online. |
| Cabitza [7] | Electronic/Online (self-administrated) Telephone (with interviewer) | Collection methods can bias PROM scores: Scores collected on the telephone with an interviewer are significantly better than those collected online. |
| Hammarstedt [8] | In person (self-administrated) Electronic/Online (self-administrated) Telephone (with interviewer) | Collection methods can bias PROM scores: PROMs collected via telephone are higher than online and in person. |
| Acosta [15] | Telephone Electronic/Online Paper based In person | Collection method can bias PROM scores: PROMs collected via telephone are higher than online and paper. |
| Richter [17] | App Paper based | No significant differences between paper based and online method. |
| Schröder [19] | Paper based Electronic/Online | No significant differences between paper based and online method. |
| Shah [20] | Paper based Electronic/Online | No significant differences between paper based and online method. Differences in scores on the EQ-5D descriptive questions, pain visual analog scale (VAS), and the NDI. |
| Rutherford [21] | Paper based vs. Electronic/Online Self-completed vs. Assisted | No significant differences between self-completed paper and electronic. Self-completion and assisted completion generate equivalent scores overall. |
| Hofstedt [25] | Paper based Online | No significant difference between paper based and online method. |
| First Author | PROMs and Questionnaire Used | Surgery Type | Results |
|---|---|---|---|
| Cabitza [6] | SF-12 Mental and Physical SF-36 Mental and Physical | Mostly hip and knee prosthetic surgery and spine- related procedures. | There is no evidence that people quitting the follow-up (PRO) program would create either significantly better or worse scores. |
| Cabitza [7] | SF-12 Mental and Physical SF-36 Mental and Physical VAS pain score | Mostly hip and knee prosthetic surgery and spine- related procedures. | Early responders reported a lower pain and better outcomes than late responders. But no difference for SF Mental Score. |
| Polk [12] | Western Ontario Osteoarthritis of the Shoulder (WOOS) index | Shoulder replacement | Non-responders did not bias the overall results, but there is a trend of worst outcome for non-responders. |
| Kim [22] | Modification of the Knee Society clinical rating system and functional score. | Total Knee Arthroplasty | Non-responders introduce a bias: they report poorer outcomes than responders. |
| Hutchings [23] | Oxford Hip Score Oxford Knee Score Aberdeen Varicose Vein Questionnaire EQ-5D (EuroQuol 5 Dimensions) Sociodemographic questionnaires | Varicose vein surgery Hernia repair Knee or hip replacement | Non-responders introduce a bias: late responders reported a slightly poorer outcome (not statistically significant for VV surgery). |
| Chen [13] | ODI (Oswestry Disability Index) VAS (Visual Analog Scale) leg/back Short Form-12 (SF-12) Physical/Mental PROMIS | Spine surgeries (decompression or fusion) | Non-responders introduce a bias: patients who stop follow-up score better. |
| Lindman [14] | HAGOS (Copenhagen Hip and Groin Outcome Score) EQ-5D (EuroQuol 5 Dimensions) iHOT-12 (International Hip Outcome Tool) HSAS (Hip Sports Activity Scale) VAS (Visual Analogue Scale) for hip function | Hip arthroscopies | Non-responders did not bias the overall results: there is no difference except for patient satisfaction. |
| Imam [18] | EQ-5D (EuroQuol 5 Dimensions) Oxford Hip Score complication, service satisfaction and outcome satisfaction questionnaires | Total hip replacement | Non responders introduce a bias: patients reporting good outcomes are overrepresented. |
| 1st Author | PROMs and Questionnaire Used | Results |
|---|---|---|
| Lapin [16] | PROMIS Global Health PROMIS 8-item SF: physical function, satisfaction with social roles and activities, anxiety, fatigue, pain interference, sleep disturbance Patient Health Questionnaire-9 depression screen Neuro-QoL cognitive function | Proxy response bias depends on the domain being tested: it is greater on more subjective domains, with proxies reporting worse outcomes. |
| Alvarez-Nebreda [26] | PROMIS physical function (PF) and pain interference (PI) Timed Up and Go (TUG) FRAIL Questionnaire | Good agreement in both PROMIS PF and PROMIS PI even if for PROMIS PI proxies report a slightly higher score. |
| Li [27] | MCBS (Medicare Current Beneficiary Survey) | Proxy response bias depends on the domain being tested: it was present in the physical, affective, cognitive, and social status domains but not in the sensory status domain. |
| 1st Author | PROMs and Questionnaire Used | Results |
|---|---|---|
| Aleem [24] | Numeric Pain Scores (NPS) for back pain and leg pain Oswestry Disability Indices (ODI) | Relying on patient recollection does not provide an accurate measure of preoperative state. |
| Aleem [28] | Numeric Pain Scores (NPS) for neck pain, arm pain Neck Disability Indices (NDI) | Relying on patient recollection does not provide an accurate measure of preoperative state. |
| Kwong [29] | SF-36/SF-12; WOMAC; American Urological Association Symptom Index, Western Ontario Meniscal Evaluation Tool; Knee Injury and Osteoarthritis Outcome Score; Oxford Hip Score; Lower Extremity Functional Scale and the feeling thermometer. | Retrospective collection offers a means of assessing PROMs in emergency admissions. |
| First Author | PROMs and Questionnaire Used | Surgery Type | Results |
|---|---|---|---|
| Shilling [9] | SF-12 | Total knee arthroplasty (TKA) | Timing of PROM collection and the interpolation assumptions can bias economic evaluation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zini, M.L.L.; Banfi, G. A Narrative Literature Review of Bias in Collecting Patient Reported Outcomes Measures (PROMs). Int. J. Environ. Res. Public Health 2021, 18, 12445. https://doi.org/10.3390/ijerph182312445
Zini MLL, Banfi G. A Narrative Literature Review of Bias in Collecting Patient Reported Outcomes Measures (PROMs). International Journal of Environmental Research and Public Health. 2021; 18(23):12445. https://doi.org/10.3390/ijerph182312445
Chicago/Turabian StyleZini, Michela Luciana Luisa, and Giuseppe Banfi. 2021. "A Narrative Literature Review of Bias in Collecting Patient Reported Outcomes Measures (PROMs)" International Journal of Environmental Research and Public Health 18, no. 23: 12445. https://doi.org/10.3390/ijerph182312445
APA StyleZini, M. L. L., & Banfi, G. (2021). A Narrative Literature Review of Bias in Collecting Patient Reported Outcomes Measures (PROMs). International Journal of Environmental Research and Public Health, 18(23), 12445. https://doi.org/10.3390/ijerph182312445