
Experience of General Practice Residents Caring for Dependent Elderly during the First COVID-19 Lockdown—A Qualitative Study

 ,
,  , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Method
2.1. Sampling
2.2. Ethical Agreement
2.3. Interview Guide
2.4. Data Collection
2.5. Analysis
2.6. Check
3. Results
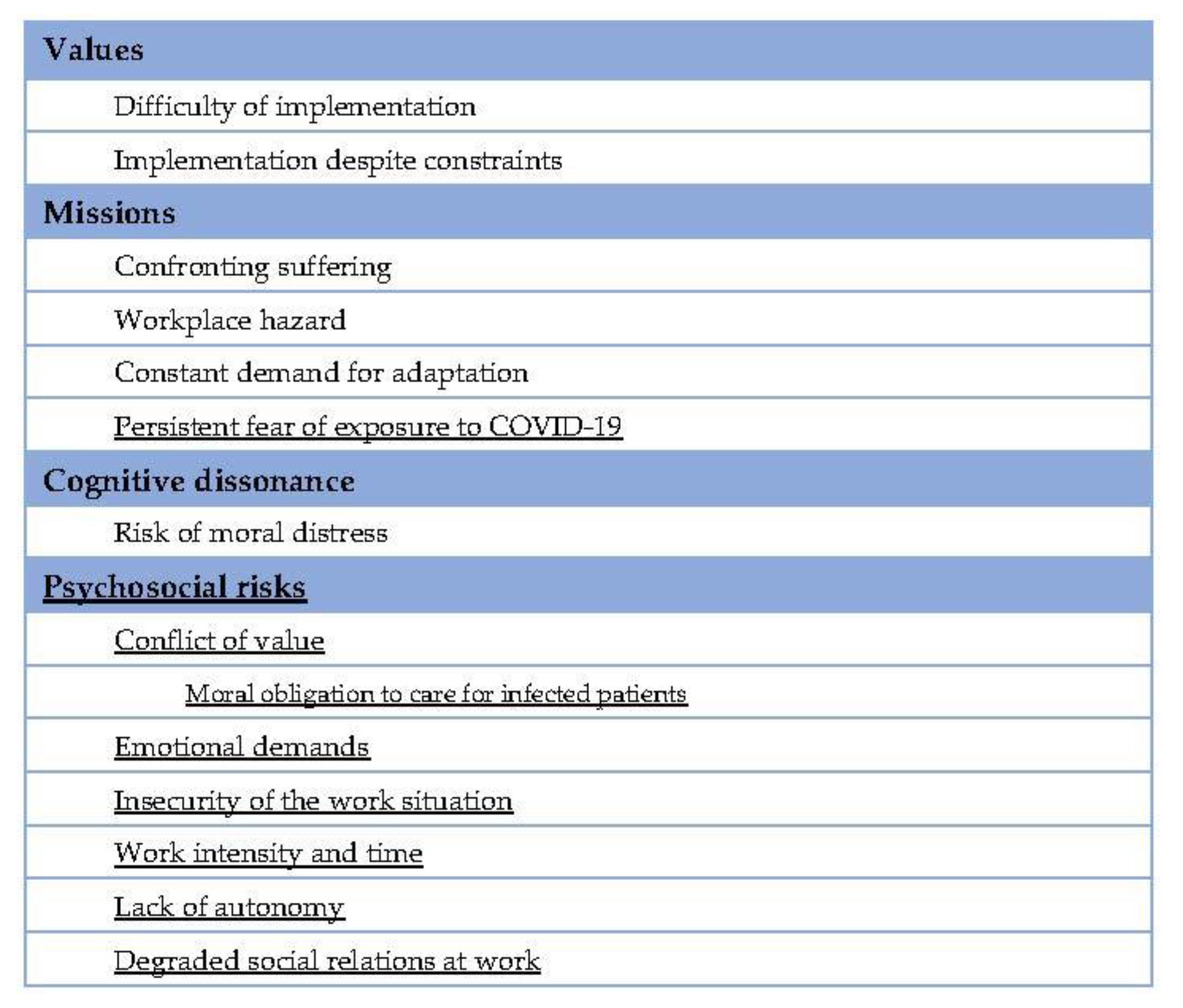
3.1. Coding Grid
3.2. Values and Missions
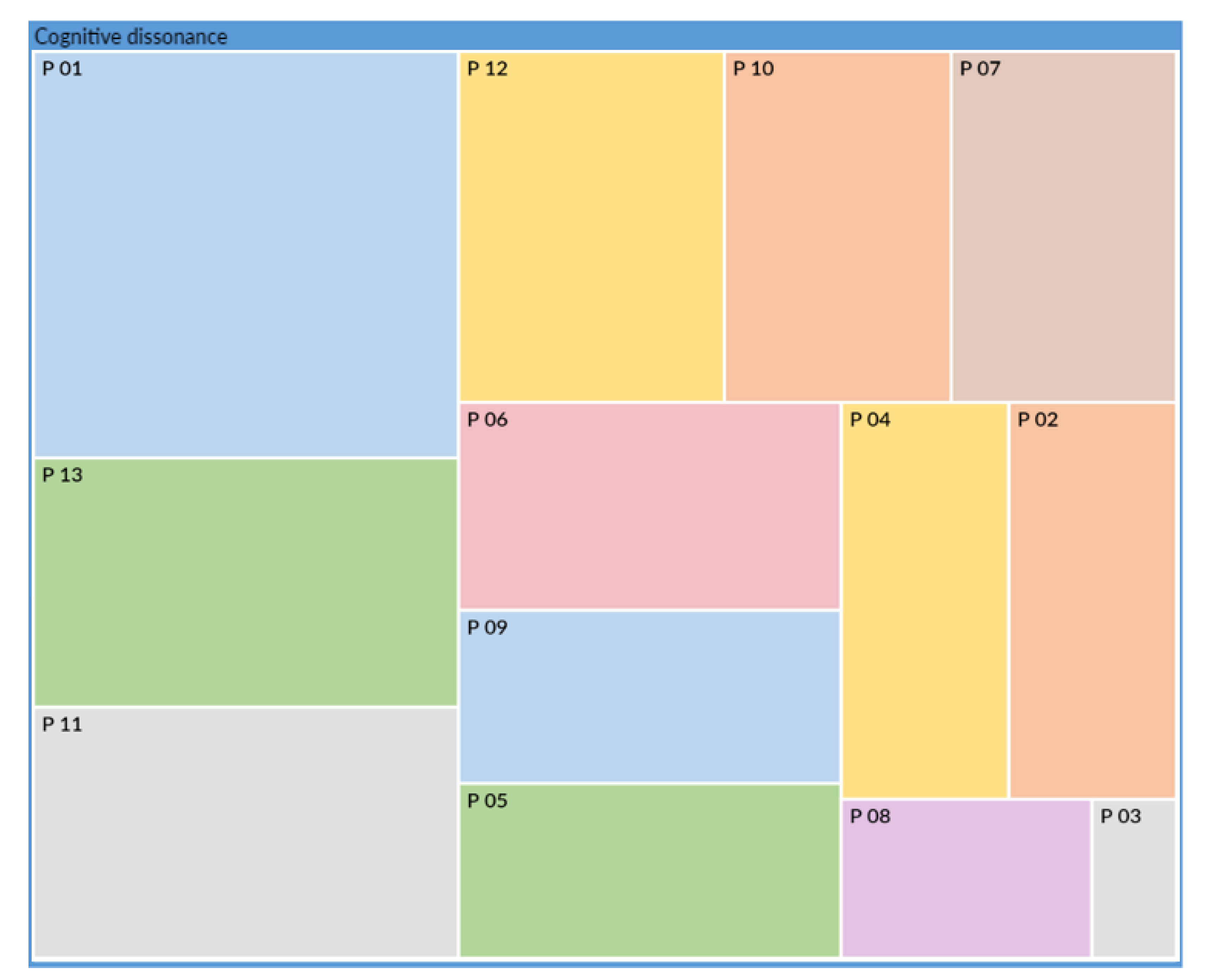
3.3. Cognitive Dissonance
“in my opinion, it was an important measure because the nursing homes were indeed a bit overwhelmed by the epidemic. Well, it affected the elderly a lot, but I think it was still very hard for the residents to live with. Not seeing their families. Some people in the nursing home are at the end of their lives, um… I think they had a very hard time living with the fact that they couldn’t have any contact with their family, or visual contact, or direct contact. That’s it…”
“You see, I didn’t take it well, for example, I thought that, in fact, they were robots who… well, I thought it was so bad of the administration not to authorize the families to come, or else only at the end, at the end of the line”
“It hurt my heart… Personally, it hurt my heart to think that, at that age… perhaps also for those who don’t have cognitive problems or not very many, they are already aware that they are coming to the end of their life. And that they may still have things to live for, but not much. And now we are depriving them of that.”
“but on the other hand, you think, an elderly person who won’t be around for much longer, who doesn’t see his family, who is actually dying of loneliness. And… isn’t it perhaps better to leave with the COVID than to die of loneliness alone in their room? I mean, I think it’s… it’s hard”
“having a COVID and at least you’ve seen your children, your grandchildren. I don’t know… because when you’re in a nursing home you’re 90 years old, your days are numbered, I think, it’s perhaps more important to see your family than to say to yourself “well at least I didn’t get the COVID but…” well that’s it. That’s my opinion.”
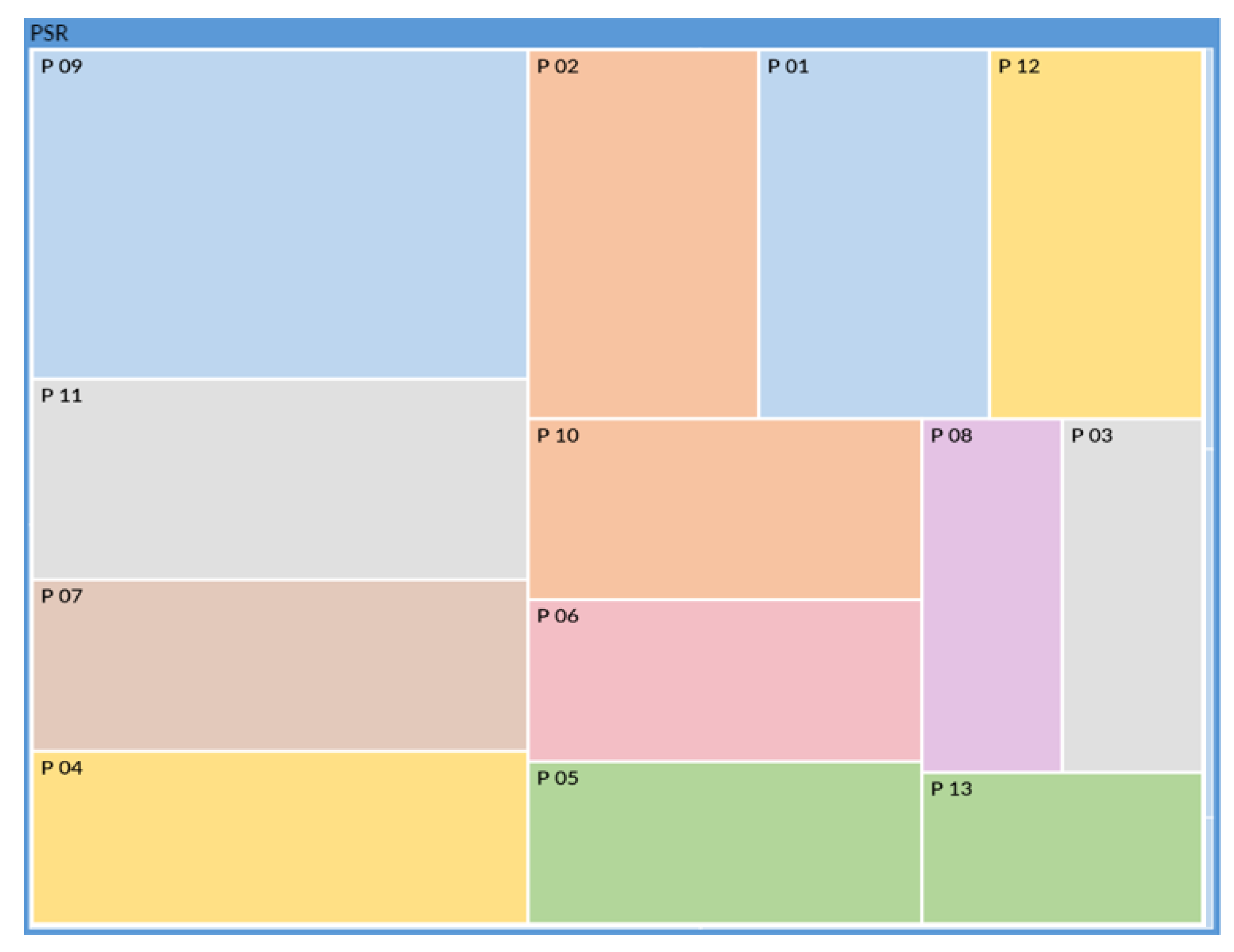
3.4. Psycho-Social Risks
3.5. Fear
“and then it’s true that we were worried because we didn’t know much about it, we didn’t know if there were other modes of transmission that we didn’t know about so um… probably that the care was less; maybe less good than if we weren’t stressed about it what. “
4. Discussion
4.1. Cognitive Dissonance
4.2. Psychosocial Risk
4.3. Fear
4.4. Perspectives
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Interview Guide
References
- Sheather, J.; Fidler, H. COVID-19 has amplified moral distress in medicine. BMJ 2021, 372, n28. [Google Scholar] [CrossRef]
- Norman, S.B.; Feingold, J.H.; Kaye-Kauderer, H.; Kaplan, C.A.; Hurtado, A.; Kachadourian, L.; Feder, A.; Murrough, J.W.; Charney, D.; Southwick, S.M.; et al. Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: Relationship to PTSD symptoms, burnout, and psychosocial functioning. Depress. Anxiety 2021, 38, 1007–1017. [Google Scholar] [CrossRef]
- Lamb, D.; Gnanapragasam, S.; Greenberg, N.; Bhundia, R.; Carr, E.; Hotopf, M.; Razavi, R.; Raine, R.; Cross, S.; Dewar, A.; et al. Psychosocial impact of the COVID-19 pandemic on 4378 UK healthcare workers and ancillary staff: Initial baseline data from a cohort study collected during the first wave of the pandemic. Occup. Environ. Med. 2021, 78, 801–808. [Google Scholar] [CrossRef]
- Ladiesse, M.; Léonard, T.; Birmelé, B. Freedoms in EHPAD, to the test of lockdown. Ethique Sante 2020, 17, 147–154. [Google Scholar]
- Weimann Péru, N.; Pellerin, J. “Slippage syndrome”: Clinical description, psychopathological models, and care management. Encephale 2010, 36 (Suppl. 2), D1–D6. [Google Scholar] [CrossRef]
- Conseil National de L’ORDRE des Médecins. Code de Déontologie; Update 25/02/2021; Conseil National de L’ORDRE des Médecins: Paris, France, 2021. [Google Scholar]
- Thomas, N.K. Resident burnout. JAMA 2004, 292, 2880–2889. [Google Scholar] [CrossRef]
- Del Carmen, M.G.; Herman, J.; Rao, S.; Hidrue, M.K.; Ting, D.; Lehrhoff, S.R.; Lenz, S.; Heffernan, J.; Ferris, T.G. Trends and Factors Associated With Physician Burnout at a Multispecialty Academic Faculty Practice Organization. JAMA Netw. Open 2019, 2, e190554. [Google Scholar] [CrossRef] [PubMed]
- Bugaj, T.J.; Krug, K.; Rentschler, A.; Nikendei, C.; Szecsenyi, J.; Schwill, S. Mental health of postgraduate trainees in primary care: A cross-sectional study. BMC Fam. Pract. 2020, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Légifrance. Article R4127-32—French Public Health Code; Légifrance: Paris, France, 2004. [Google Scholar]
- Klein, J.; McColl, G. Cognitive dissonance: How self-protective distortions can undermine clinical judgement. Med. Educ. 2019, 53, 1178–1186. [Google Scholar] [CrossRef]
- Schrepel, C.; Jauregui, J.; Brown, A.; Shandro, J.; Strote, J. Navigating Cognitive Dissonance: A Qualitative Content Analysis Exploring Medical Students’ Experiences of Moral Distress in the Emergency Department. AEM Educ. Train. 2019, 3, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Côté, L.; Turgeon, J. Appraising qualitative research articles in medicine and medical education. Med. Teach. 2005, 27, 71–75. [Google Scholar] [CrossRef]
- Clark, J.P. How to Peer Review a Qualitative Manuscript. Peer Review in Health Sciences; BMJ Books: London, UK, 2003; pp. 219–235. [Google Scholar]
- Malterud, K. Qualitative research: Standards, challenges, and guidelines. Lancet 2001, 358, 483–488. [Google Scholar] [CrossRef]
- Lebeau, J.-P. Introduction to Qualitative Health Research: A Guide to Successful Thesis and Dissertation Writing; Co-edition; GMsanté et CNGE Productions: Paris, France, 2021; p. 69. [Google Scholar]
- Mehta, J.; Yates, T.; Smith, P.; Henderson, D.; Winteringham, G.; Burns, A. Rapid implementation of Microsoft Teams in response to COVID-19: One acute healthcare organisation’s experience. BMJ Health Care Inform. 2020, 27, e100209. [Google Scholar] [CrossRef] [PubMed]
- Mukamurera, J.; Lacourse, F.; Couturier, Y. Advances in qualitative analysis: Towards transparency and systematisation of practices. Qual. Res. 2006, 26, 110–138. [Google Scholar]
- Anadón, M.; Guillemette, F. Is qualitative research necessarily inductive? Qual. Res.-Spec. Issue 2007, 5, 26–37. [Google Scholar]
- Berger, J.T. Moral distress in medical education and training. J. Gen. Intern. Med. 2014, 29, 395–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blais, M.; Martineau, S. General Inductive Analysis: A description of an approach to making sense of raw data. Qual. Res. 2006, 26, 26. [Google Scholar]
- Nuebling, M.; Seidler, A.; Garthus-Niegel, S.; Latza, U.; Wagner, M.; Hegewald, J.; Liebers, F.; Jankowiak, S.; Zwiener, I.; Wild, P.S.; et al. The Gutenberg Health Study: Measuring psychosocial factors at work and predicting health and work-related outcomes with the ERI and the COPSOQ questionnaire. BMC Public Health 2013, 13, 538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, C.; Murphy, K.; Meehan, B.; Thomas, J.; Brooker, D.; Casey, D. From screening to synthesis: Using nvivo to enhance transparency in qualitative evidence synthesis. J. Clin. Nurs. 2017, 26, 873–881. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Berhie, A.Y.; Tezera, Z.B.; Azagew, A.W. Moral Distress and Its Associated Factors Among Nurses in Northwest Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol. Res. Behav. Manag. 2020, 13, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweeney, J.C.; Hausknecht, D.; Soutar, G.N. Cognitive dissonance after purchase: A multidimensional scale. Psychol. Mark. 2000, 17, 369–385. [Google Scholar] [CrossRef]
- Brazeau, C.M.; Shanafelt, T.; Durning, S.J.; Massie, F.S.; Eacker, A.; Moutier, C.; Satele, D.V.; Sloan, J.A.; Dyrbye, L.N. Distress among matriculating medical students relative to the general population. Acad. Med. 2014, 89, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Prins, J.T.; Gazendam-Donofrio, S.M.; Tubben, B.J.; van der Heijden, F.M.M.A.; van de Wiel, H.B.M.; Hoekstra-Weebers, J.E.H.M. Burnout in medical residents: A review. Med. Educ. 2007, 41, 788–800. [Google Scholar] [CrossRef] [Green Version]
- Frajerman, A.; Morvan, Y.; Krebs, M.-O.; Gorwood, P.; Chaumette, B. Burnout in medical students before residency: A systematic review and meta-analysis. Eur. Psychiatry 2019, 55, 36–42. [Google Scholar] [CrossRef]
- Laramée, J.; Kuhl, D. Suicidal ideation among family practice residents at the University of British Columbia. Can. Fam. Physician 2019, 65, 730–735. [Google Scholar]
- Dutheil, F.; Aubert, C.; Pereira, B.; Dambrun, M.; Moustafa, F.; Mermillod, M.; Baker, J.S.; Trousselard, M.; Lesage, F.X.; Navel, V. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226361. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.; Xu, H.; Rebaza, A.; Sharma, L.; Dela Cruz, C.S. Protecting health-care workers from subclinical coronavirus infection. Lancet Respir. Med. 2020, 8, e13. [Google Scholar] [CrossRef] [Green Version]
- Shin, L.M.; Liberzon, I. The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology 2010, 35, 169–191. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. Fear of COVID-19 and the mental health consequences in America. Psychol. Trauma 2020, 12 (Suppl. 1), S17–S21. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM 2020, 113, 707–712. [Google Scholar] [CrossRef]
- Krupa, S.; Paweł, W.; Mędrzycka-Dąbrowska, W.; Lintowska, A.; Ozga, D. Sleep Disturbances in Individuals Quarantined Due to SARS-CoV-2 Pandemic in Poland: A Mixed Methods Design Study. Glob. Adv. Health Med. 2021, 10, 21649561211020707. [Google Scholar] [CrossRef] [PubMed]
- Crosswell, A.D.; Lockwood, K.G. Best practices for stress measurement: How to measure psychological stress in health research. Health Psychol. Open 2020, 7, 2055102920933072. [Google Scholar] [CrossRef] [PubMed]
- Chew-Graham, C.A.; May, C.R.; Perry, M.S. Qualitative research and the problem of judgement: Lessons from interviewing fellow professionals. Fam. Pract. 2002, 19, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Bergen, N.; Labonté, R. « Everything Is Perfect, and We Have No Problems »: Detecting and Limiting Social Desirability Bias in Qualitative Research. Qual. Health Res. 2020, 30, 783–792. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants’ Characteristics | |
| Gender | Women: 8/Men: 5 |
| GP resident progress in studies Age | 2.5 ± 0.8 semesters 27 ± 0.7 years old |
| Place of work experience | -Geriatric medicine: 7 -Emergency or COVID unit: 3 -Other hospital specialties: 3 |
| Interviews characteristics | |
| Duration | 23 ± 5.5 min |
| Place | Face to face: 6/Online: 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augros, J.; Dutheil, F.; Benson, A.C.; Sauvant-Rochat, M.-P.; Boudet, G.; Laporte, C.; Cambon, B.; Vallet, G.T. Experience of General Practice Residents Caring for Dependent Elderly during the First COVID-19 Lockdown—A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 12281. https://doi.org/10.3390/ijerph182312281
Augros J, Dutheil F, Benson AC, Sauvant-Rochat M-P, Boudet G, Laporte C, Cambon B, Vallet GT. Experience of General Practice Residents Caring for Dependent Elderly during the First COVID-19 Lockdown—A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12281. https://doi.org/10.3390/ijerph182312281
Chicago/Turabian StyleAugros, Johann, Frédéric Dutheil, Amanda C. Benson, Marie-Pierre Sauvant-Rochat, Gil Boudet, Catherine Laporte, Benoit Cambon, and Guillaume T. Vallet. 2021. "Experience of General Practice Residents Caring for Dependent Elderly during the First COVID-19 Lockdown—A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 23: 12281. https://doi.org/10.3390/ijerph182312281
APA StyleAugros, J., Dutheil, F., Benson, A. C., Sauvant-Rochat, M.-P., Boudet, G., Laporte, C., Cambon, B., & Vallet, G. T. (2021). Experience of General Practice Residents Caring for Dependent Elderly during the First COVID-19 Lockdown—A Qualitative Study. International Journal of Environmental Research and Public Health, 18(23), 12281. https://doi.org/10.3390/ijerph182312281