
Surveillance of Outbreaks of SARS-CoV-2 Infections at School in the Veneto Region: Methods and Results of the Public Health Response during the Second and Third Waves of the Pandemic between January and June 2021

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. COVID-19 Surveillance at School
2.2. Public Health Interventions at Schools in Italy and the Veneto
2.3. Contact Tracing and Quarantine in Veneto Schools
2.4. Statistical Analyses
3. Results
3.1. Trend of School-Related Episodes
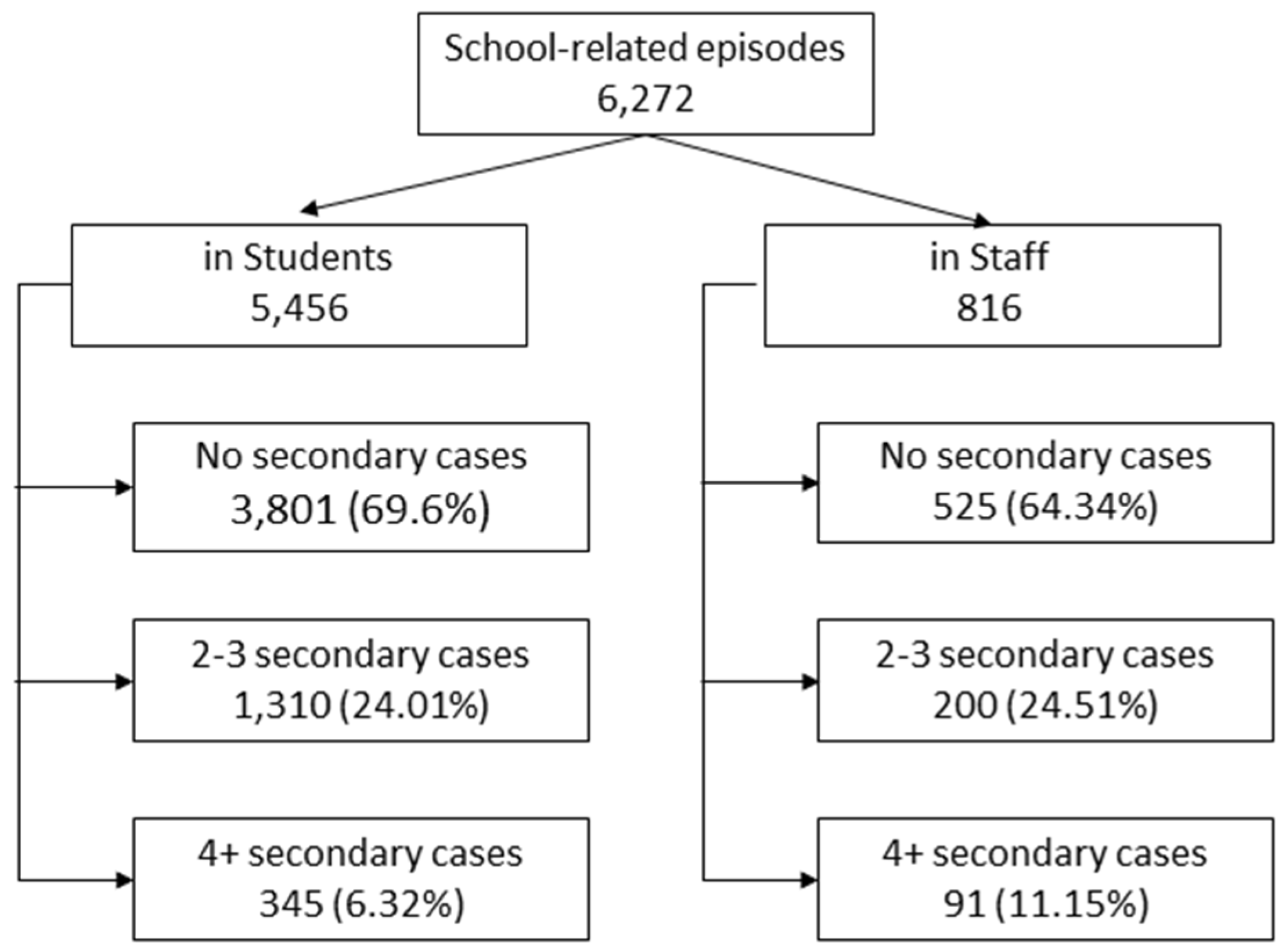
3.2. Secondary Infections
3.3. Index Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jackson, C.; Vynnycky, E.; Hawker, J.; Olowokure, B.; Mangtani, P. School closures and influenza: Systematic review of epidemiological studies. BMJ Open 2013, 3, e002149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaro, M.; Tamburro, P.; La Torre, M.; Dal Mas, F.; Thomas, R.; Cobianchi, L.; Barach, P. Non-pharmaceutical Interventions and the Infodemic on Twitter: Lessons Learned from Italy during the COVID-19. J. Med. Syst. 2021, 45, 50. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Influenza Preparedness Plan. In The Role of WHO and Recommendations for National Measures before and during Pandemics; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- European Centre for Disease Prevention and Control. COVID-19 in Children and the Role of School Settings in COVID-19 Transmission; ECDC: Stockholm, Sweden, 2020.
- European Centre for Disease Prevention and Control. COVID-19 in Children and the Role of School Settings in COVID-19 Transmission—2nd Update; ECDC: Stockholm, Sweden, 2021.
- Crowe, J.; Schnaubelt, A.T.; SchmidtBonne, S.; Angell, K.; Bai, J.; Eske, T.; Nicklin, M.; Pratt, C.; White, B.; Crotts-Hannibal, B.; et al. Assessment of a Program for SARS-CoV-2 Screening and Environmental Monitoring in an Urban Public School District. JAMA Netw Open 2021, 4, e2126447. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Guidelines for Non-Pharmaceutical Interventions to Reduce the Impact of COVID-19 in the EU/EEA and the UK; ECDC: Stockholm, Sweden, 2020.
- Vlachos, J.; Hertegård, E.; B Svaleryd, H. The effects of school closures on SARS-CoV-2 among parents and teachers. Proc. Natl. Acad. Sci. USA 2021, 118, e2020834118. [Google Scholar] [CrossRef] [PubMed]
- Krishnaratne, S.; Pfadenhauer, L.M.; Coenen, M.; Geffert, K.; Jung-Sievers, C.; Klinger, C.; Kratzer, S.; Littlecott, H.; Movsisyan, A.; Rabe, J.E.; et al. Measures implemented in the school setting to contain the COVID-19 pandemic: A scoping review. Cochrane Database Syst. Rev. 2020, 12, CD013812. [Google Scholar] [PubMed]
- Working Group Istituto Superiore di Sanità (ISS); Ministry of Health; Ministry of Education; INAIL; Foundation Bruno Kessler; Region Emilia-Romagna; Region Veneto. Indicazioni Operative per la Gestione di Casi e Focolai di SARS-CoV-2 Nelle Scuole e Nei Servizi Educativi Dell’infanzia. Operational Indications for the Management of SARS-CoV-2 Cases and Clusters in Schools and Childhood Education Services; ISS: Rome, Italy, 2020; Rapporto ISS COVID-19 n. 58/2020 Rev. Italian.
- Italian Government. DPCM 7 Settembre 2020, Allegato, A. Available online: https://www.gazzettaufficiale.it/eli/id/2020/09/07/20A04814/sg (accessed on 18 November 2021).
- Walsh, S.; Chowdhury, A.; Braithwaite, V.; Russell, S.; Birch, J.M.; Ward, J.L.; Waddington, C.; Brayne, C.; Bonell, C.; Viner, R.M.; et al. Do school closures and school reopenings affect community transmission of COVID-19? A systematic review of observational studies. BMJ Open 2021, 11, e053371. [Google Scholar] [CrossRef] [PubMed]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Contact Tracing: Public Health Management of Persons, Including Healthcare Workers, Who Have Had Contact with COVID-19 Cases in the European Union—Third Update; ECDC: Stockholm, Sweden, 2020.
- Ministry of Education. Documento per la pianificazione delle attività scolastiche, educative e formative in tutte le Istituzioni del Sistema nazionale di Istruzione per l’anno scolastico 2020/2021. Available online: https://www.miur.gov.it/documents/20182/2467413/Le+linee+guida.pdf/4e4bb411-1f90-9502-f01e-d8841a949429 (accessed on 18 November 2021).
- Head, J.R.; Andrejko, K.L.; Cheng, Q.; Collender, P.A.; Phillips, S.; Boser, A.; Heaney, A.K.; Hoover, C.M.; Wu, S.L.; Northrup, G.R.; et al. School closures reduced social mixing of children during COVID-19 with implications for transmission risk and school reopening policies. J. R. Soc. Interface 2021, 18, 20200970. [Google Scholar] [CrossRef] [PubMed]
- Auger, K.A.; Shah, S.S.; Richardson, T.; Hartley, D.; Hall, M.; Warniment, A.; Timmons, K.; Bosse, D.; Ferris, S.A.; Brady, P.W.; et al. Association Between Statewide School Closure and COVID-19 Incidence and Mortality in the US. JAMA 2020, 324, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening. Israel. Euro. Surveill. 2020, 25, 2001352. [Google Scholar] [CrossRef] [PubMed]
- Iwata, K.; Doi, A.; Miyakoshi, C. Was school closure effective in mitigating coronavirus disease 2019 (COVID-19)? Time series analysis using Bayesian inference. Int. J. Infect. Dis. 2020, 99, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Otte im Kampe, E.; Lehfeld, A.S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks. Germany. March to August 2020. Euro. Surveill. 2020, 25, 2001645. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.; Kim, K.R.; Park, H.; Kim, S.; Kim, Y.J. Stepwise School Opening and an Impact on the Epidemiology of COVID-19 in the Children. J. Korean Med. Sci. 2020, 35, e414. [Google Scholar] [CrossRef] [PubMed]
- Health Ministry. Decreto 12 marzo 2021. Approvazione del Piano strategico nazionale dei vaccini per la prevenzione delle infezioni da SARS-CoV-2 costituito dal documento recante «Elementi di preparazione della strategia vaccinale», di cui al decreto 2 gennaio 2021 nonchè dal documento recante «Raccomandazioni ad interim sui gruppi target della vaccinazione anti SARS-CoV-2/COVID-19» of 10th March 2021. Available online: https://www.gazzettaufficiale.it/eli/id/2021/03/24/21A01802/sg (accessed on 18 November 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of School | Age | 7 Janurary 2021 1 31 Janurary 2021 | 1 February 2021 6 March 2021 | 8 March 2021 13 March 2021 2 | 15 March 2021 6 April 2021 | 7 April 2021 24 May 2021 | 26 May 2021 8 June 2021 |
|---|---|---|---|---|---|---|---|
| Nursery | 0–2 | 100% In-Person attendance | Closed | 100% In-Person attendance | |||
| Kindergarten | 3–5 | 100% In-Person attendance | Closed | 100% In-Person attendance | |||
| Primary school | 6–10 | 100% In-Person attendance | 100% Remote Learning | 100% In-Person attendance | |||
| Middle School | 11–13 | 100% In-Person attendance | 100% Remote Learning | 100% In-Person attendance | |||
| High school | 14–19 | 100% Remote Learning | 50% In-Person attendance | 50–75% In-Person attendance | 100% Remote Learning | 50–75% In-Person attendance | Minimum 70% In-Person attendance; 1st and 5th year students 100% |
| Type of School | No Secondary Cases | Secondary Cases | 1 or 2 Secondary Cases | 3 or More Secondary Cases | Mean of Secondary Cases (SD) | Median of Secondary Cases (5p–95p) |
|---|---|---|---|---|---|---|
| Nursery | 70.5% | 29.5% | 21.5% | 8.0% | 2.15 (2.14) | 1 (1–5) |
| Kindergarten | 62.4% | 37.6% | 26.0% | 11.7% | 2.55 (2.83) | 1 (1–9) |
| Primary school | 70.4% | 29.6% | 23.3% | 6.3% | 2.16 (2.36) | 1 (1–6) |
| Middle school | 69.0% | 31.0% | 24.5% | 6.5% | 2.04 (1.80) | 1 (1–6) |
| High school | 70.9% | 29.1% | 24.0% | 5.1% | 1.83 (1.57) | 1 (1–5) |
| Total | 69.0% | 31.0% | 24.1% | 7.0% | 2.13 (2.19) | 1 (1–6) |
| Index Case: Student | Index Case: Educator or Staff | |||||
|---|---|---|---|---|---|---|
| Type of School | No Secondary Cases | 1 or 2 Secondary Cases | 3 or More Secondary Cases | No Secondary Cases | 1 or 2 Secondary Cases | 3 or More Secondary Cases |
| Nursery | 77.2% | 17.9% | 4.8% | 52.7% | 30.9% | 16.7% |
| Kindergarten | 63.8% | 25.9% | 10.3% | 58.8% | 26.1% | 15.0% |
| Primary school | 71.5% | 22.9% | 5.6% | 62.9% | 25.8% | 11.3% |
| Middle School | 68.1% | 25.2% | 6.7% | 83.0% | 13.6% | 3.4% |
| High school | 70.8% | 24.0% | 5.2% | 74.2% | 22.5% | 3.4% |
| Total | 69.7% | 24.0% | 6.3% | 64.3% | 24.5% | 11.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonon, M.; Da Re, F.; Zampieri, C.; Nicoletti, M.; Caberlotto, R.; De Siena, F.P.; Lattavo, G.; Minnicelli, A.; Zardetto, A.; Sforzi, B.; et al. Surveillance of Outbreaks of SARS-CoV-2 Infections at School in the Veneto Region: Methods and Results of the Public Health Response during the Second and Third Waves of the Pandemic between January and June 2021. Int. J. Environ. Res. Public Health 2021, 18, 12165. https://doi.org/10.3390/ijerph182212165
Tonon M, Da Re F, Zampieri C, Nicoletti M, Caberlotto R, De Siena FP, Lattavo G, Minnicelli A, Zardetto A, Sforzi B, et al. Surveillance of Outbreaks of SARS-CoV-2 Infections at School in the Veneto Region: Methods and Results of the Public Health Response during the Second and Third Waves of the Pandemic between January and June 2021. International Journal of Environmental Research and Public Health. 2021; 18(22):12165. https://doi.org/10.3390/ijerph182212165
Chicago/Turabian StyleTonon, Michele, Filippo Da Re, Chiara Zampieri, Michele Nicoletti, Riccardo Caberlotto, Francesco Paolo De Siena, Gaia Lattavo, Anil Minnicelli, Alberto Zardetto, Benedetta Sforzi, and et al. 2021. "Surveillance of Outbreaks of SARS-CoV-2 Infections at School in the Veneto Region: Methods and Results of the Public Health Response during the Second and Third Waves of the Pandemic between January and June 2021" International Journal of Environmental Research and Public Health 18, no. 22: 12165. https://doi.org/10.3390/ijerph182212165
APA StyleTonon, M., Da Re, F., Zampieri, C., Nicoletti, M., Caberlotto, R., De Siena, F. P., Lattavo, G., Minnicelli, A., Zardetto, A., Sforzi, B., Ros, E., Mongillo, M., Scatto, A., Vecchiato, E., Baldo, V., Cocchio, S., & Russo, F. (2021). Surveillance of Outbreaks of SARS-CoV-2 Infections at School in the Veneto Region: Methods and Results of the Public Health Response during the Second and Third Waves of the Pandemic between January and June 2021. International Journal of Environmental Research and Public Health, 18(22), 12165. https://doi.org/10.3390/ijerph182212165