
The Development of Telemedicine and eHealth in Surgery during the SARS-CoV-2 Pandemic

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
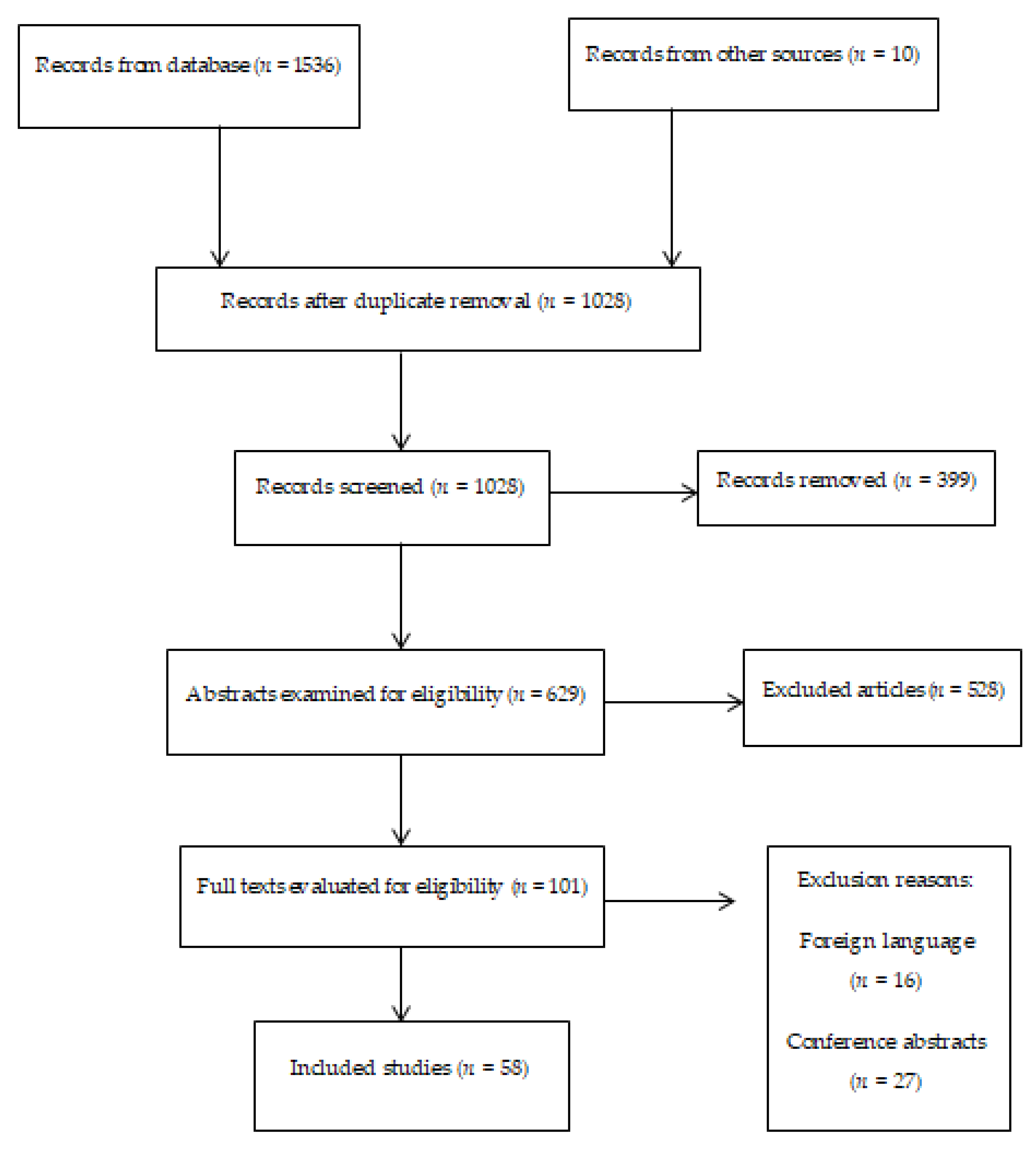
2.1. Search Strategy
2.2. Selection of Criteria and Evidence Quality
2.3. Data Extraction
3. Results
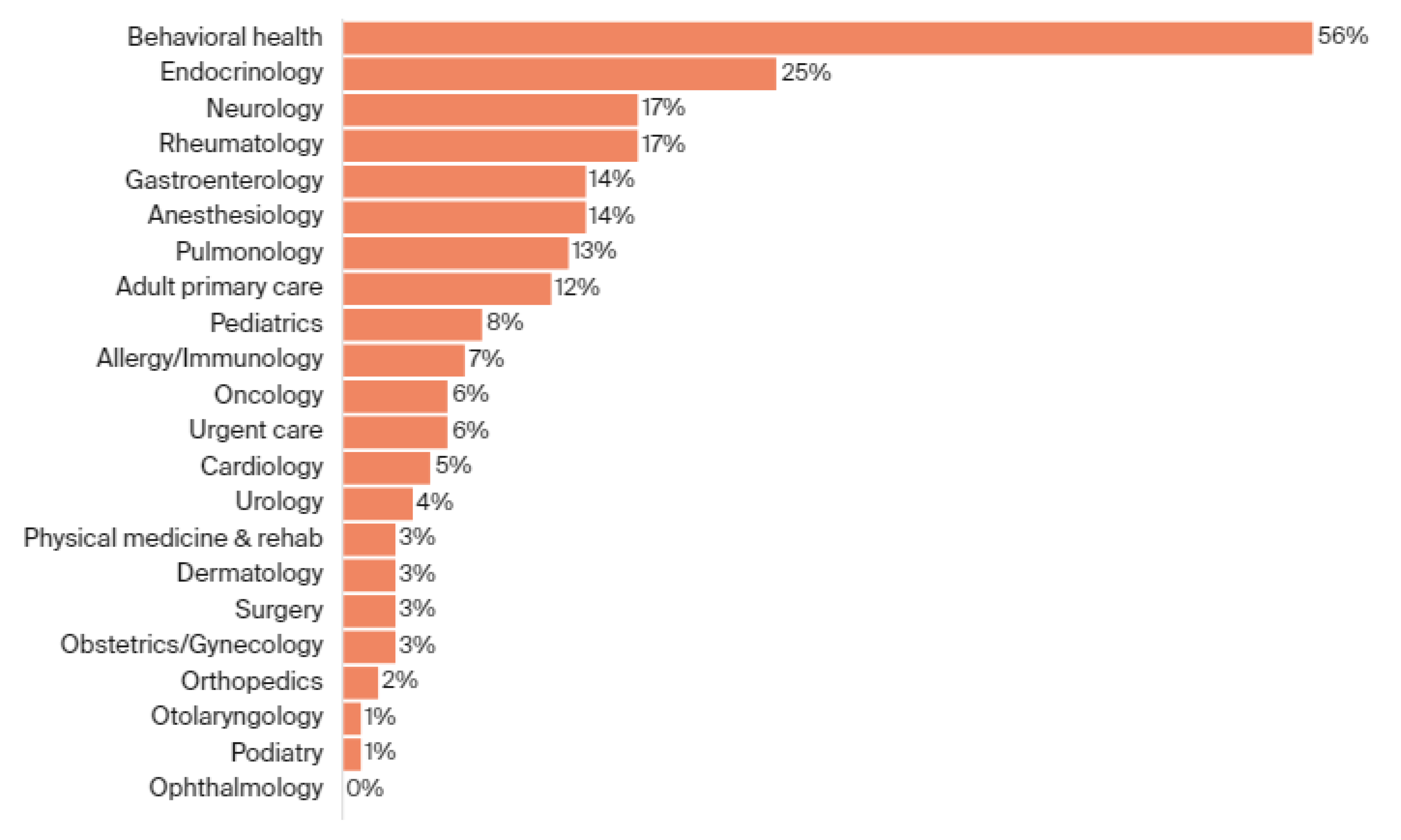
3.1. Multidisciplinary Use of Telemedicine
3.2. Telemedicine in Surgery Globally
3.3. Telemedicine in Surgery in Europe
3.4. Telemedicine in Surgery in the U.S.
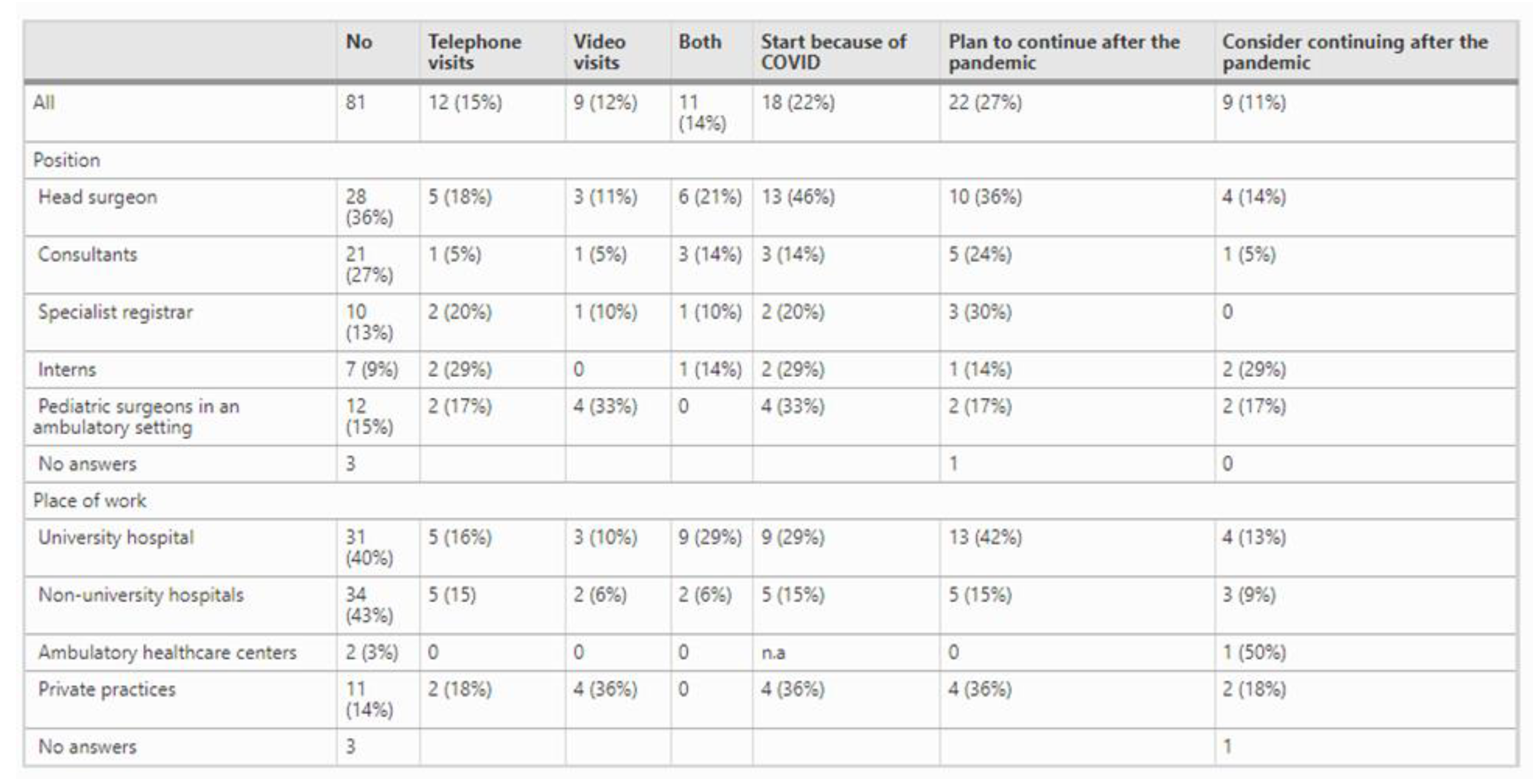
3.5. Telemedicine in Surgery in Switzerland
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Opportunities and Developments TELEMEDICINE in Member States Report on the Second Global Survey on eHealth Global Observatory for eHealth Series-Volume 2. 2010. Available online: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf (accessed on 18 September 2021).
- Ohannessian, R.; Mattos, S.; Paranhos-Baccalà, G.; Vanhems, P. The Role of Telemedicine in Response to the Zika Virus Outbreak in Brazil; Zika Summit: Paris, France, 2016. [Google Scholar]
- Ohannessian, R. Telemedicine: Potential applications in epidemic situations. Eur. Res. Telemed. 2015, 4, 95–98. [Google Scholar] [CrossRef]
- Zhai, Y.; Wang, Y.; Zhang, M.; Gittell, J.H.; Jiang, S.; Chen, B.; Cui, F.; He, X.; Zhao, J.; Wang, X. From Isolation to Coordination: How Can Telemedicine Help Combat the COVID-19 Outbreak? 2021. Available online: https://link.springer.com/chapter/10.1007%2F978-981-16-3631-8_12 (accessed on 29 August 2021).
- Truex, G. As Telehealth Technology and Methodologies Mature, Consumer Adoption Emerges as Key Challenge for Providers. 2019. Available online: https://discover.jdpa.com/hubfs/Files/Industry%20Campaigns/Healthcare/Telehealth_WP_v6_071919.pdf (accessed on 17 September 2021).
- Hawkins, M. Survey: Physician Practice Patterns Changing as a Result of COVID-19|Merritt Hawkins. 2020. Available online: https://www.merritthawkins.com/news-and-insights/media-room/press/-physician-practice-patterns-changing-as-a-result-of-covid-19/ (accessed on 30 August 2021).
- Zingg, T.; Sojer, R.; Röthlisberger, F. Digitalisierung in der ambulanten Gesundheitsversorgung. Schweiz. Ärzteztg. 2019, 100, 113–116. [Google Scholar] [CrossRef]
- Nittas, V.; Von Wyl, V. COVID-19 and telehealth: A window of opportunity and its challenges. Swiss Med. Wkly. 2020, 150, w20284. [Google Scholar] [CrossRef] [PubMed]
- covidguide.health. (n.d.). COVID-GUIDE. Available online: https://covidguide.health/en/ (accessed on 29 August 2021).
- Serper, M.; Nunes, F.; Ahmad, N.; Roberts, D.; Metz, D.C.; Mehta, S.J. Positive early patient and clinician experience with telemedicine in an academic gastroenterology practice during the COVID-19 pandemic. Gastroenterology 2020, 159, 1589–1591. [Google Scholar] [CrossRef] [PubMed]
- The Commonwealth Fund. The Impact of COVID-19 on Outpatient Visits in 2020: Visits Remained Stable, Despite a Late Surge in Cases. 2021. Available online: https://www.commonwealthfund.org/publications/2021/feb/impact-covid-19-outpatient-visits-2020-visits-stable-despite-late-surge (accessed on 16 September 2021).
- Uscher-Pines, L.; Sousa, J.; Raja, P.; Mehrotra, A.; Barnett, M.L.; Huskamp, H.A. Suddenly Becoming a “Virtual Doctor”: Experiences of Psychiatrists Transitioning to Telemedicine During the COVID-19 Pandemic. Psychiatr. Serv. 2020, 71, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A. Telepsychiatry coming into its own with COVID-19. Brown Univ. Child Adolesc. Psychopharmacol. Update 2020, 22, 1–3. [Google Scholar] [CrossRef][Green Version]
- Tornese, G.; Schiaffini, R.; Mozzillo, E.; Franceschi, R.; Frongia, A.; Scaramuzza, A. Telemedicine in the time of the COVID-19 pandemic: Results from the first survey among italian pediatric diabetes centers. Healthcare 2021, 9, 815. [Google Scholar] [CrossRef]
- Negrini, S.; Kiekens, C.; Bernetti, A.; Capecci, M.; Ceravolo, M.G.; Lavezzi, S.; Zampolini, M.; Boldrini, P. Telemedicine from research to practice during the pandemic. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 327–330. [Google Scholar] [CrossRef]
- Aziz, A.; Zork, N.; Aubey, J.J.; Baptiste, C.D.; D’Alton, M.E.; Emeruwa, U.N.; Fuchs, K.M.; Goffman, D.; Gyamfi-Bannerman, C.; Haythe, J.H.; et al. Telehealth for high-risk pregnancies in the setting of the COVID-19 pandemic. Am. J. Perinatol. 2020, 37, 800–808. [Google Scholar] [CrossRef]
- Parikh, A.; Kumar, A.A.; Jahangir, E. Cardio-oncology care in the time of COVID-19 and the role of telehealth. JACC CardioOncol. 2020, 2, 356–358. [Google Scholar] [CrossRef]
- Badeli, H.; Nejad, A.T.; Rad, A.H. Utilizing Telemedicine for Managing COVID-19. J. Pediatr. Nephrol. 2020, 8, 1–3. Available online: https://journals.sbmu.ac.ir/jpn/article/view/30046 (accessed on 30 August 2021).
- Ohannessian, R.; Duong, T.A.; Odone, A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: A call to action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- Kruse, C.S.; Krowski, N.; Rodriguez, B.; Tran, L.; Vela, J.; Brooks, M. Telehealth and Patient Satisfaction: A Systematic Review and Narrative Analysis. BMJ Open 2017, 7, e016242. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5629741/ (accessed on 18 September 2021). [CrossRef] [PubMed]
- Giansanti, D. The Italian fight against the COVID-19 pandemic in the second phase: The renewed opportunity of telemedicine. Telemed. e-Health 2020, 26, 1328–1331. [Google Scholar] [CrossRef]
- Nepogodiev, D.; Bhangu, A. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020, 107, 1440–1449. [Google Scholar]
- Dick, L.; Green, J.; Brown, J.; Kennedy, E.; Cassidy, R.; Othman, S.; Berlansky, M. Changes in Emergency General Surgery during Covid-19 in Scotland: A Prospective Cohort Study. World J. Surg. 2020, 44, 3590–3594. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7454130/#CR7 (accessed on 18 September 2021). [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine across the globe-position paper from the COVID-19 pandemic health system resilience PROGRAM (REPROGRAM) international consortium (Part 1). Front. Public Health 2020, 8, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Puliyath, N.; Huda, F.; Rai, A.; Munnamgi, S.; David, L.E.; Kumar, P.; Saxena, V.; Basu, S. The utility of telemedicine in general surgery during Covid-19 pandemic and beyond: Our experience. Nature 2020, 1, 5455–5458. [Google Scholar]
- Bhatia, R. Telehealth and COVID-19: Using technology to accelerate the curve on access and quality healthcare for citizens in India. Technol. Soc. 2021, 64, 101465. [Google Scholar] [CrossRef]
- Thakurani, S.; Gupta, S. Evolution of aesthetic surgery in India, current practice scenario, and anticipated post-COVID-19 changes: A survey-based analysis. Eur. J. Plast. Surg. 2021, 44, 129–138. [Google Scholar] [CrossRef]
- El-Helou, A. Spine surgery in Atlantic Canada in the COVID-19 era: Lessons learned so far. Spine J. 2020, 20, 1379–1380. [Google Scholar] [CrossRef]
- O.T.N. (n.d.). Home. otn.ca. Available online: http://otn.ca (accessed on 3 September 2021).
- Lin, J.C.; Welle, N.; Ding, J.; Chuen, J. A look to the future: Pandemic-induced digital technologies in vascular surgery. In Seminars in Vascular Surgery; WB Saunders: Philadelphia, PA, USA, 2021. [Google Scholar]
- Stoehr, J.R.; Jahromi, A.H.; Chu, Q.D.; Zibari, G.B.; Gosain, A.K. Considerations for resuming global surgery outreach programs during and after the COVID-19 pandemic. Surgery 2021, 1, 2–9. [Google Scholar]
- Metzger, G.A.; Cooper, J.; Lutz, C.; Jatana, K.R.; Nishimura, L.; Deans, K.J.; Minneci, P.C.; Halaweish, I. The value of telemedicine for the pediatric surgery patient in the time of COVID-19 and beyond. J. Pediatr. Surg. 2021, 56, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 pandemic, lessons for the future. Telemed. e-Health 2020, 25, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Lakshin, G.; Banek, S.; Keese, D.; Rolle, U.; Schmedding, A. Telemedicine in the pediatric surgery in Germany during the COVID-19 pandemic. Pediatr. Surg. Int. 2021, 37, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Mouchtouris, N.; Lavergne, P.; Montenegro, T.S.; Gonzalez, G.; Baldassari, M.; Sharan, A.; Jabbour, P.; Harrop, J.; Rosenwasser, R.; Evans, J.J. Telemedicine in neurosurgery: Lessons learned and transformation of care during the COVID-19 pandemic. World Neurosurg. 2020, 140, e387–e394. [Google Scholar] [CrossRef]
- Menendez, M.E.; Jawa, A.; Haas, D.A.; Warner, J.J. Orthopedic surgery post COVID-19: An opportunity for innovation and transformation. J. Shoulder Elb. Surg. 2020, 29, 1083–1086. [Google Scholar] [CrossRef]
- Omboni, S. Telemedicine during the COVID-19 in Italy: A missed opportunity? Telemed. e-Health 2020, 26, 973–975. [Google Scholar] [CrossRef]
- Pignatti, M.; Pinto, V.; Miralles, M.E.L.; Giorgini, F.A.; Cannamela, G.; Cipriani, R. How the COVID-19 pandemic changed the Plastic Surgery activity in a regional referral center in Northern Italy. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 1348–1356. [Google Scholar] [CrossRef]
- Donatelli, F.; Miceli, A.; Glauber, M.; Cirri, S.; Maiello, C.; Coscioni, E.; Napoli, C. Adult cardiovascular surgery and the coronavirus disease 2019 (COVID-19) pandemic: The Italian experience. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 755–762. [Google Scholar] [CrossRef]
- Pinar, U.; Anract, J.; Perrot, O.; Tabourin, T.; Chartier-Kastler, E.; Parra, J.; Vaessen, C.; De La Taille, A.; Roupret, M. Preliminary assessment of patient and physician satisfaction with the use of teleconsultation in urology during the COVID-19 pandemic. World J. Urol. 2021, 39, 1991–1996. [Google Scholar] [CrossRef]
- Heeno, E.; Biesenbach, I.; Englund, C.; Lund, M.; Toft, A.; Lund, L. Patient perspective on telemedicine replacing physical consultations in urology during the COVID-19 lockdown in Denmark. Scand. J. Urol. 2021, 55, 117–183. [Google Scholar] [CrossRef] [PubMed]
- Pappot, N.; Taarnhøj, G.A.; Pappot, H. Telemedicine and e-health solutions for COVID-19: Patients’ perspective. Telemed. e-Health 2020, 26, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Ghomrawi, H.M.; Holl, J.L.; Abdullah, F. Telemedicine in surgery—Beyond a pandemic adaptation. JAMA Surg. 2021, 1, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Kichloo, A.; Albosta, M.; Dettloff, K.; Wani, F.; El-Amir, Z.; Singh, J.; Aljadah, M.; Chakinala, R.C.; Kanugula, A.K.; Solanki, S.; et al. Telemedicine, the current COVID-19 pandemic and the future: A narrative review and perspectives moving forward in the U.S.A. Fam. Med. Community Health 2020, 8, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Fisk, M.; Livingstone, A.; Pit, S.W. Telehealth in the context of COVID-19: Changing perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19–e26. [Google Scholar] [CrossRef]
- Hurley, E.T.; Haskel, J.D.; Bloom, D.A.; Gonzalez-Lomas, G.; Jazrawi, L.M.; Bosco, J.A.; Campbell, K.A. The use and acceptance of telemedicine in orthopedic surgery during the COVID-19 pandemic. Telemed. e-Health 2021, 27, 657–662. [Google Scholar] [CrossRef]
- Dekker, P.K.; Bhardwaj, P.; Singh, T.; Bekeny, J.C.; Kim, K.G.; Steinberg, J.S.; Evans, K.K.; Song, D.H.; Attinger, C.E.; Fan, K.L. Telemedicine in the wake of the COVID-19 pandemic: Increasing access to surgical care. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3228. [Google Scholar] [CrossRef]
- Lanham, N.S.; Bockelman, K.J.; McCriskin, B.J. Telemedicine and orthopaedic surgery: The COVID-19 pandemic and our new normal. JBJS Rev. 2020, 8, e20–e25. [Google Scholar] [CrossRef]
- Salehi, P.P.; Torabi, S.J.; Lee, Y.H.; Azizzadeh, B. Telemedicine practices of facial plastic and reconstructive surgeons in the United States: The effect of novel Coronavirus-19. Facial Plast. Surg. Aesthet. Med. 2020, 22, 464–470. [Google Scholar] [CrossRef]
- Smith, W.R.; Atala, A.J.; Terlecki, R.P.; Kelly, E.E.; Matthews, C.A. Implementation guide for rapid integration of an outpatient telemedicine program during the COVID-19 pandemic. J. Am. Coll. Surg. 2020, 231, 216–222. [Google Scholar] [CrossRef]
- De Biase, G.; Freeman, W.D.; Bydon, M.; Smith, N.; Jerreld, D.; Pascual, J.; Casler, J.; Hasse, C.; Quiñones-Hinojosa, A.; Abode-Iyamah, K. Telemedicine utilization in neurosurgery during the COVID-19 pandemic: A glimpse into the future? Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 736–744. [Google Scholar] [CrossRef]
- Allaert, F.A.; Legrand, L.; Carime, N.A.; Quantin, C. Will applications on smartphones allow a generalization of telemedicine? BMC Med. Inform. Decis. Mak. 2020, 20, 30. [Google Scholar] [CrossRef]
- Hübner, M.; Zingg, T.; Martin, D.; Eckert, P.; Demartines, N. Surgery for non-Covid-19 patients during the pandemic. PLoS ONE 2020, 15, e0241331. [Google Scholar]
- Marttos, A.C.; Kuchkarian, F.M.; Abreu-Reis, P.; Pereira, B.M.; Collet-Silva, F.S.; Fraga, G.P. Enhancing trauma education worldwide through telemedicine. In World Journal of Emergency Surgery; BioMed Central: London, UK, 2012; Volume 7, pp. 1–6. [Google Scholar]
- Keshvardoost, S.; Bahaadinbeigy, K.; Fatehi, F. Role of telehealth in the management of COVID-19: Lessons learned from previous SARS, MERS, and Ebola outbreaks. Telemed. e-Health 2020, 26, 850–852. [Google Scholar] [CrossRef] [PubMed]
- Seifert, A.; Batsis, J.A.; Smith, A.C. Telemedicine in long-term care facilities during and beyond COVID-19: Challenges caused by the digital divide. Front. Public Health 2020, 8, 690–695. [Google Scholar] [CrossRef]
- Mamadnabiev, I.; Imfeld, S.; Gürke, L.; Aschwanden, M.; Isaak, A. A telemedicine communication exchange network in Gorno-Badakhshan Autonomic Oblast in collaboration with Swiss Surgical Teams. J. Telemed. Telecare 2020, 1, 1357633X20948989. [Google Scholar] [CrossRef] [PubMed]
- Contreras, C.M.; Metzger, G.A.; Beane, J.D.; Dedhia, P.H.; Ejaz, A.; Pawlik, T.M. Telemedicine: Patient-provider clinical engagement during the COVID-19 pandemic and beyond. J. Gastrointest. Surg. 2020, 24, 1692–1697. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taha, A.; Saad, B.; Enodien, B.; Bachmann, M.; Frey, D.M.; Taha-Mehlitz, S. The Development of Telemedicine and eHealth in Surgery during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11969. https://doi.org/10.3390/ijerph182211969
Taha A, Saad B, Enodien B, Bachmann M, Frey DM, Taha-Mehlitz S. The Development of Telemedicine and eHealth in Surgery during the SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(22):11969. https://doi.org/10.3390/ijerph182211969
Chicago/Turabian StyleTaha, Anas, Bara Saad, Bassey Enodien, Marta Bachmann, Daniel M. Frey, and Stephanie Taha-Mehlitz. 2021. "The Development of Telemedicine and eHealth in Surgery during the SARS-CoV-2 Pandemic" International Journal of Environmental Research and Public Health 18, no. 22: 11969. https://doi.org/10.3390/ijerph182211969
APA StyleTaha, A., Saad, B., Enodien, B., Bachmann, M., Frey, D. M., & Taha-Mehlitz, S. (2021). The Development of Telemedicine and eHealth in Surgery during the SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health, 18(22), 11969. https://doi.org/10.3390/ijerph182211969