
Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
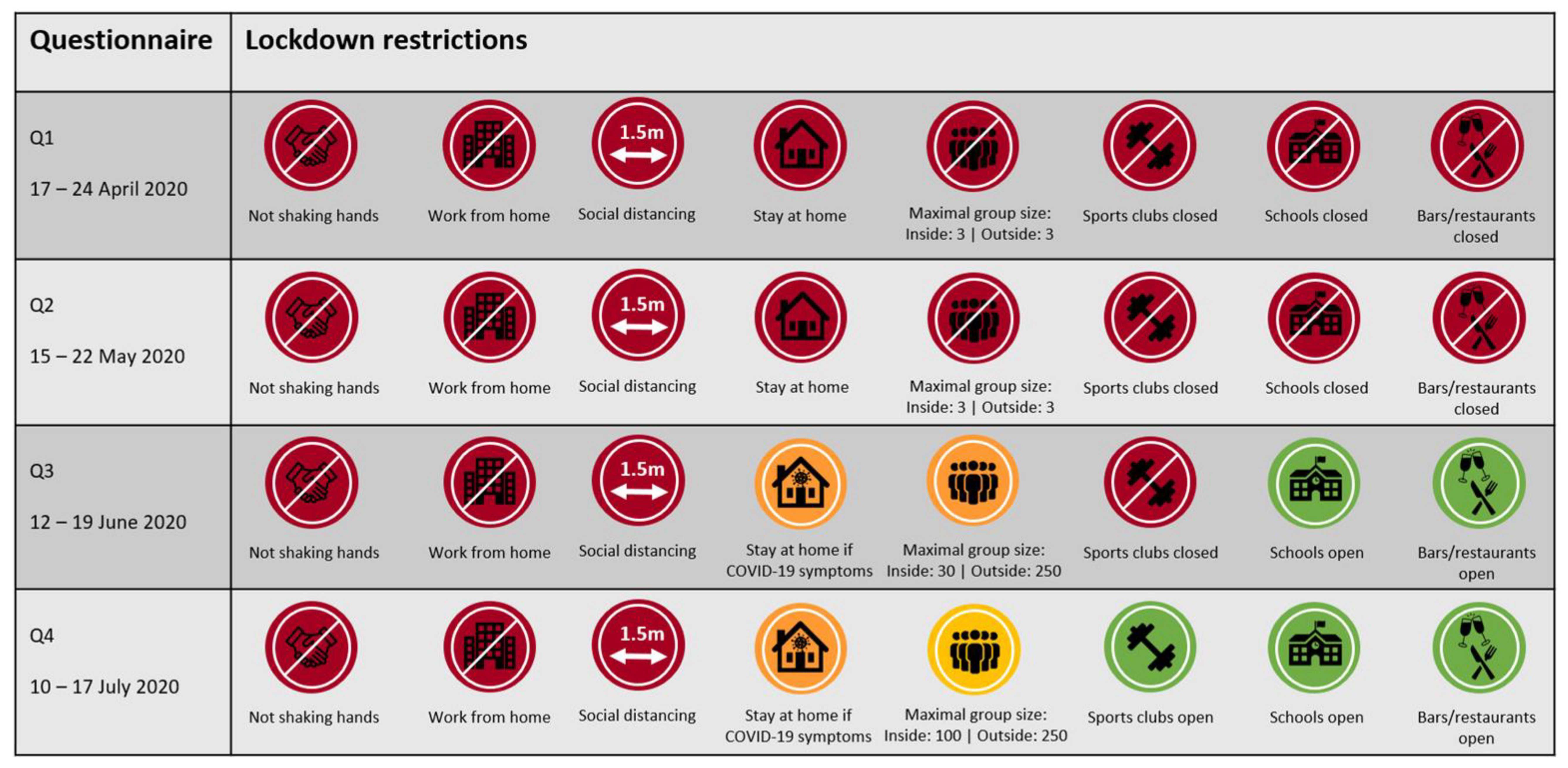
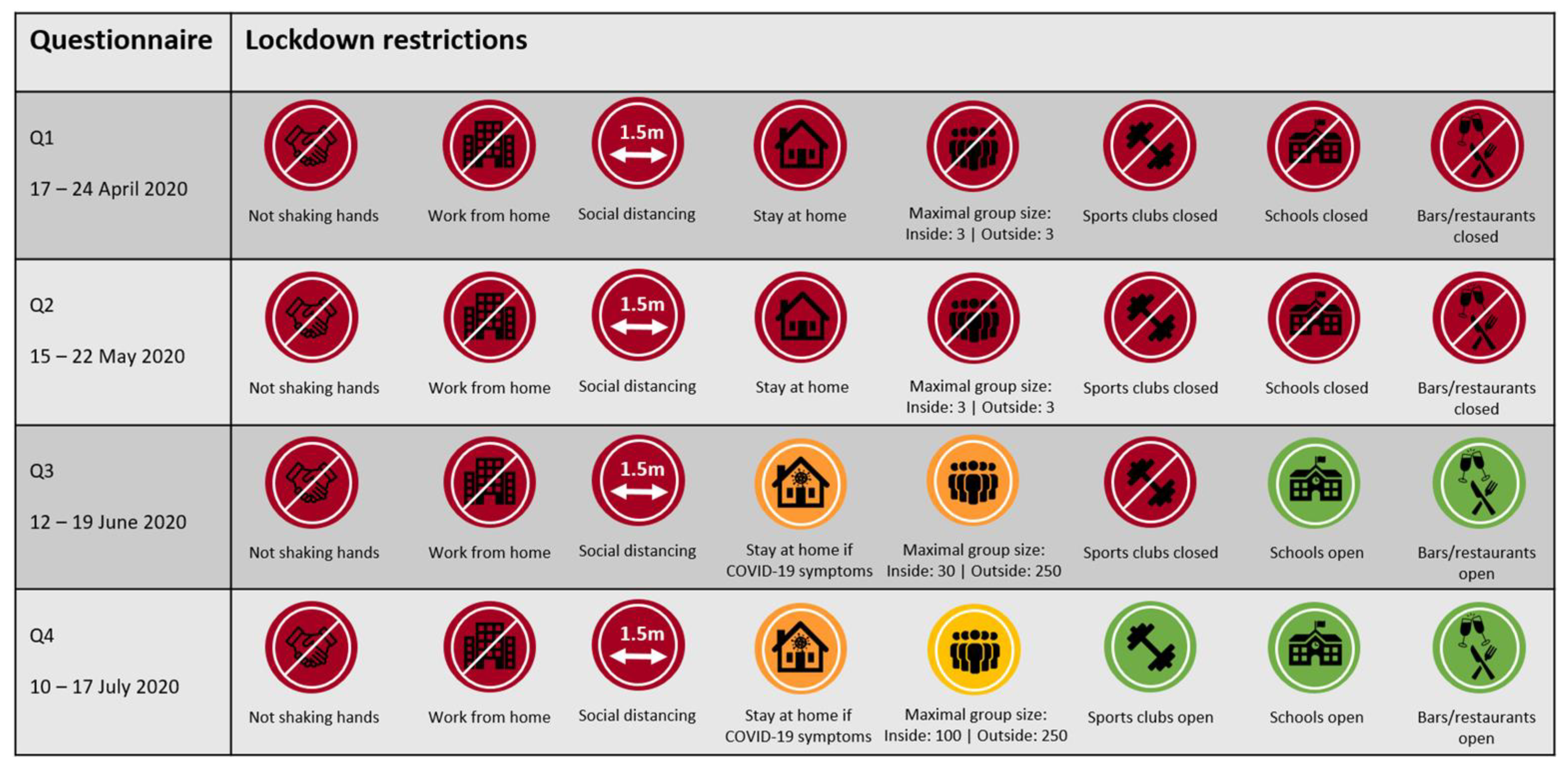
2.2. Study Procedures
2.3. Statistical Analysis
3. Results
3.1. Cohort Characteristics
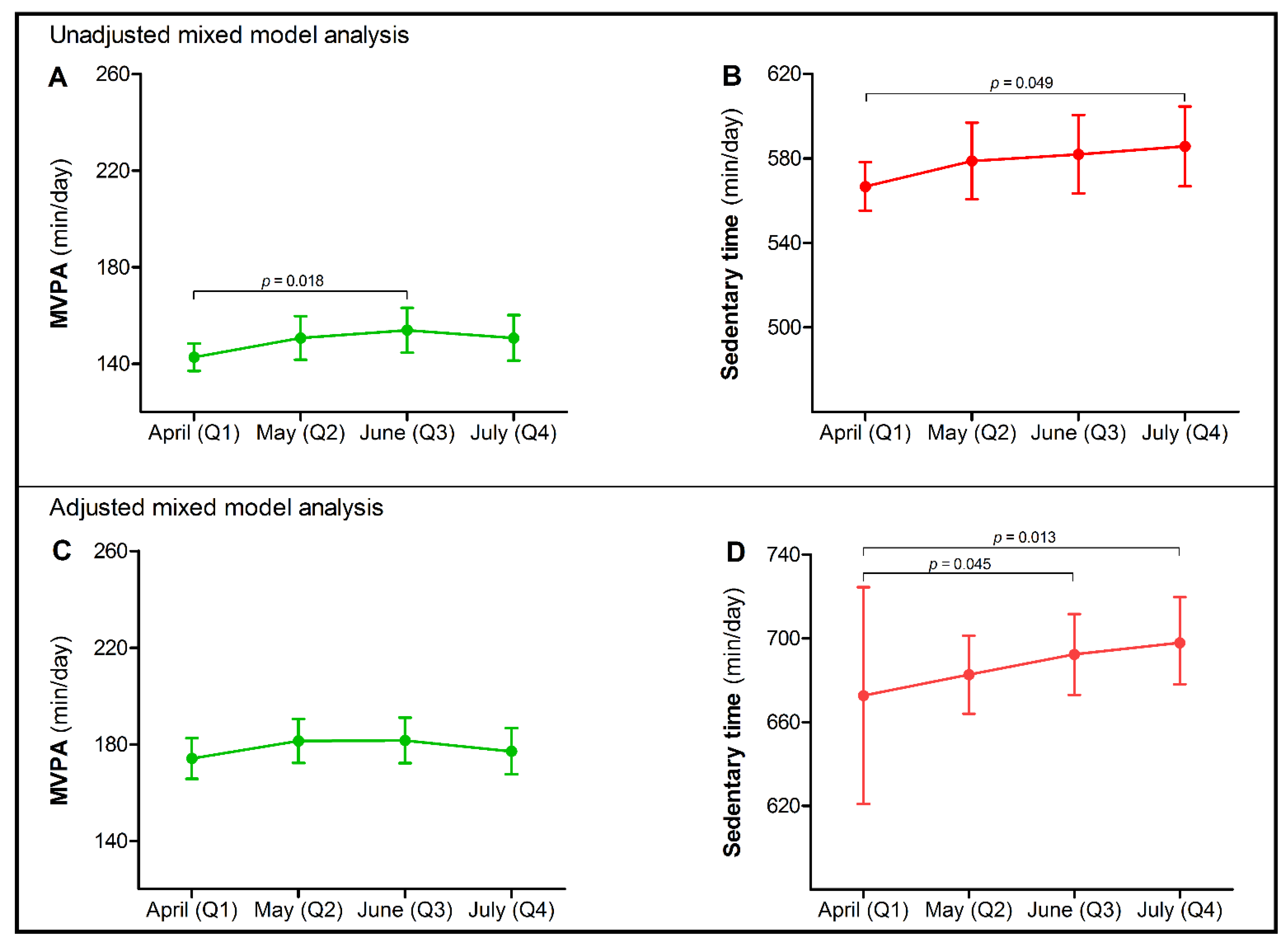
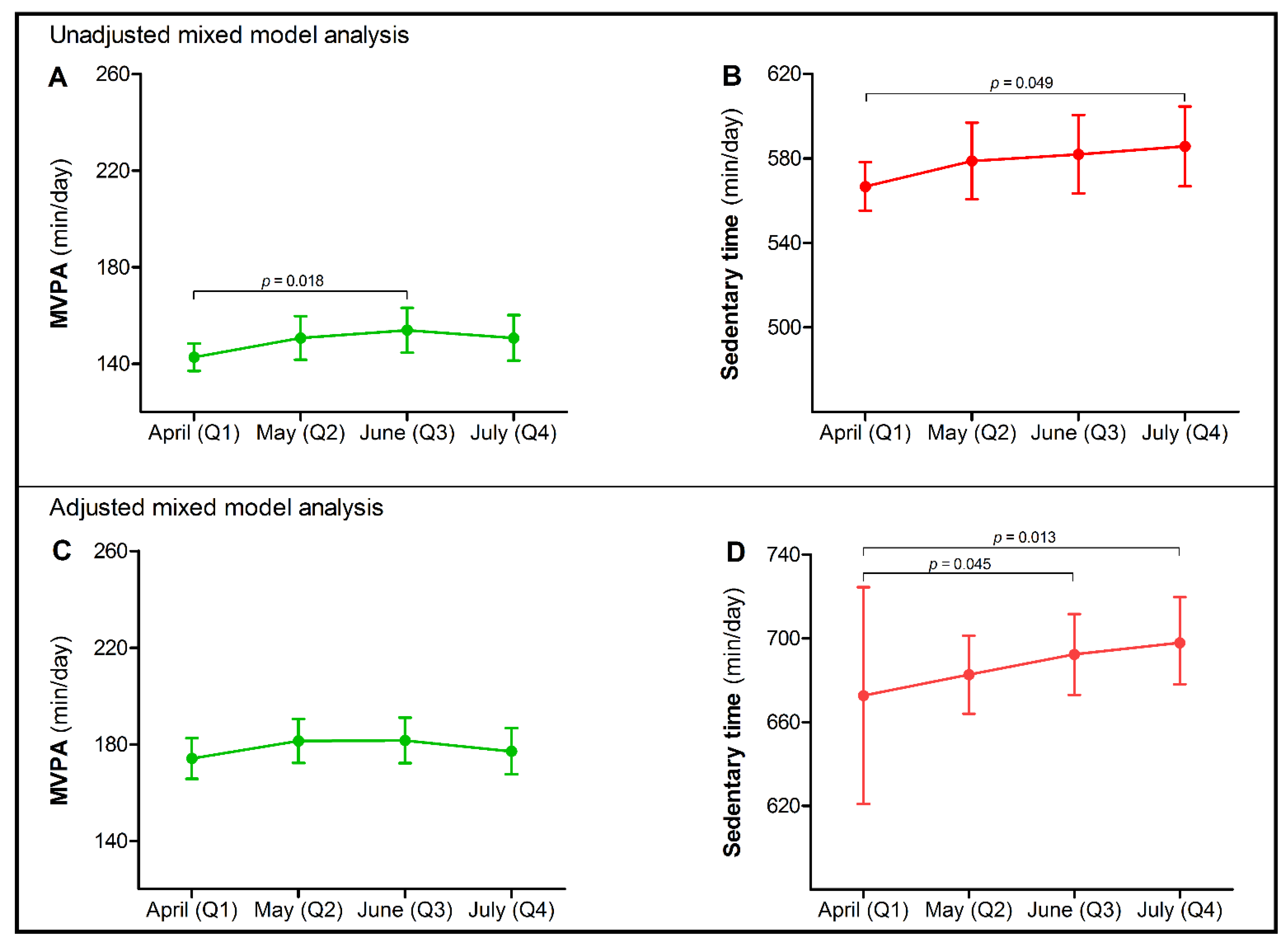
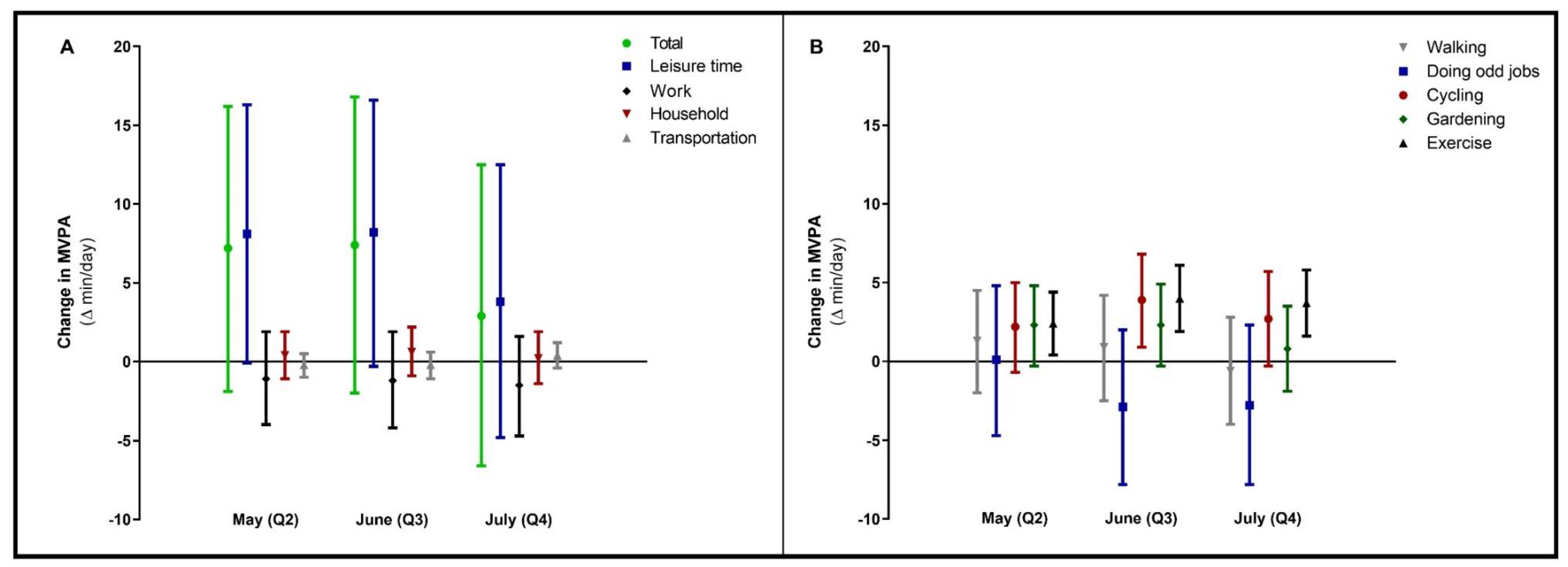
3.2. Changes in Physical Activity
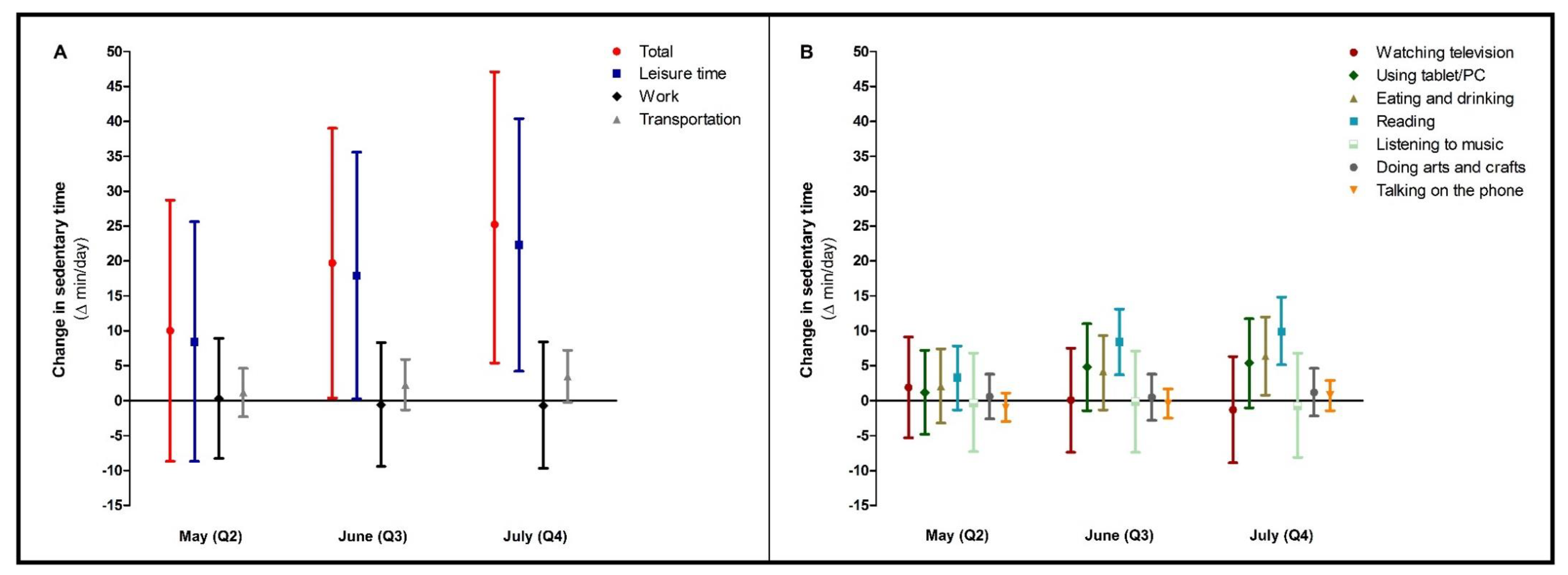
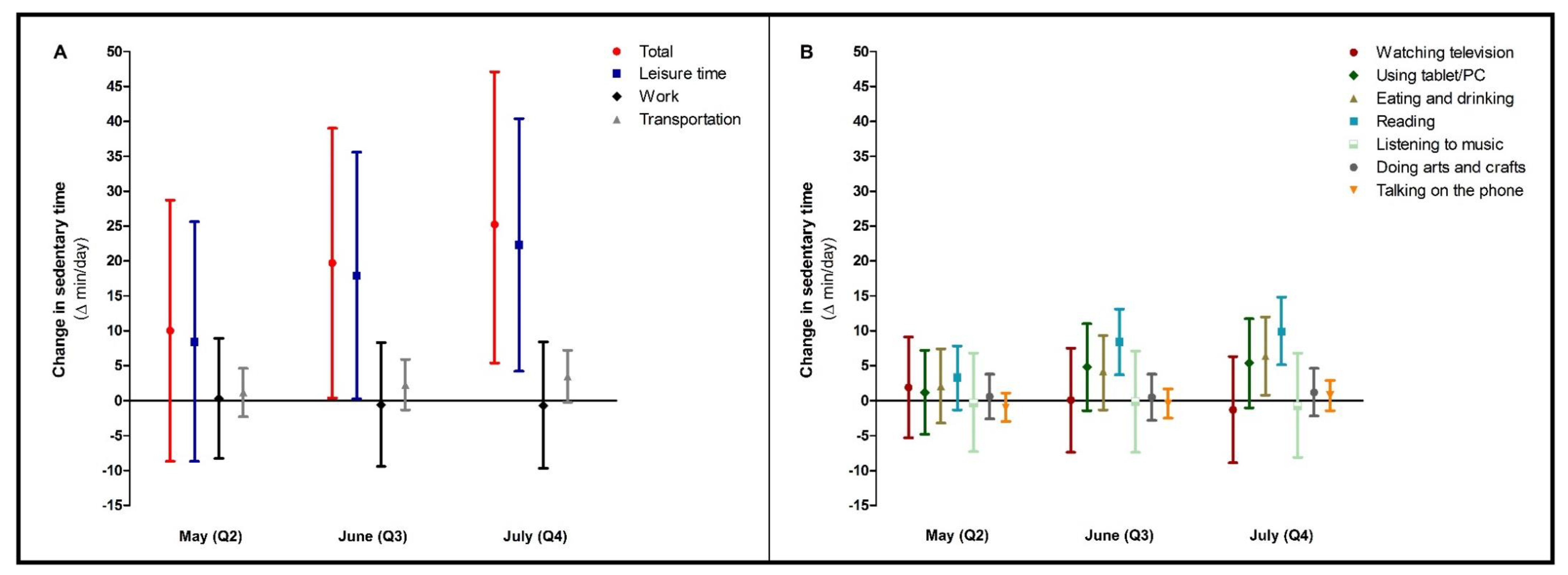
3.3. Changes in Sedentary Behaviour
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2020, 39, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am. J. Physiol. -Heart Circ. Physiol. 2020, 318, H1441–H1446. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [Green Version]
- Stewart, R.A.H.; Held, C.; Hadziosmanovic, N.; Armstrong, P.W.; Cannon, C.P.; Granger, C.B.; Hagström, E.; Hochman, J.S.; Koenig, W.; Lonn, E.; et al. Physical Activity and Mortality in Patients With Stable Coronary Heart Disease. J. Am. Coll. Cardiol. 2017, 70, 1689–1700. [Google Scholar] [CrossRef] [PubMed]
- Moholdt, T.; Lavie, C.J.; Nauman, J. Sustained Physical Activity, Not Weight Loss, Associated With Improved Survival in Coronary Heart Disease. J. Am. Coll. Cardiol. 2018, 71, 1094–1101. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Huang, Z.; Wu, Y.; Huang, S.; Wang, Y.; Zhao, H.; Chen, S.; Wu, S.; Gao, X. Sedentary time, metabolic abnormalities, and all-cause mortality after myocardial infarction: A mediation analysis. Eur. J. Prev. Cardiol. 2019, 26, 96–104. [Google Scholar] [CrossRef]
- Vasankari, V.; Husu, P.; Vähä-Ypyä, H.; Suni, J.H.; Tokola, K.; Borodulin, K.; Wennman, H.; Halonen, J.; Hartikainen, J.; Sievänen, H.; et al. Subjects with cardiovascular disease or high disease risk are more sedentary and less active than their healthy peers. BMJ Open Sport Exerc. Med. 2018, 4, e000363. [Google Scholar] [CrossRef] [PubMed]
- Van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Impact of COVID-19 lockdown on physical activity and sedentary behaviour in Dutch cardiovascular disease patients. Neth. Heart J. 2021, 29, 273–279. [Google Scholar] [CrossRef]
- Vetrovsky, T.; Frybova, T.; Gant, I.; Semerad, M.; Cimler, R.; Bunc, V.; Siranec, M.; Miklikova, M.; Vesely, J.; Griva, M.; et al. The detrimental effect of COVID-19 nationwide quarantine on accelerometer-assessed physical activity of heart failure patients. ESC Heart Fail. 2020, 7, 2093–2097. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.W.; Dogra, S.; Carter, S.E.; Owen, N. Sit less and move more for cardiovascular health: Emerging insights and opportunities. Nat. Rev. Cardiol. 2021, 18, 637–648. [Google Scholar] [CrossRef]
- Bakker, E.A.; van Bakel, B.M.A.; Aengevaeren, W.R.M.; Meindersma, E.P.; Snoek, J.A.; Waskowsky, W.M.; van Kuijk, A.A.; Jacobs, M.M.L.M.; Hopman, M.T.E.; Thijssen, D.H.J.; et al. Sedentary behaviour in cardiovascular disease patients: Risk group identification and the impact of cardiac rehabilitation. Int. J. Cardiol. 2021, 326, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, D.E.; Norman, G.J.; Wagner, N.; Patrick, K.; Calfas, K.J.; Sallis, J.F. Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. J. Phys. Act. Health 2010, 7, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in Times of Lockdown: An Analysis of the Impact of COVID-19 on Levels and Patterns of Exercise among Adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Jeong, S.W.; Kim, S.H.; Kang, S.H.; Kim, H.J.; Yoon, C.H.; Youn, T.J.; Chae, I.H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef]
- Turrisi, T.B.; Bittel, K.M.; West, A.B.; Hojjatinia, S.; Hojjatinia, S.; Mama, S.K.; Lagoa, C.M.; Conroy, D.E. Seasons, weather, and device-measured movement behaviors: A scoping review from 2006 to 2020. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; De Bacquer, D.; De Backer, G.; Ryden, L.; Jennings, C.; Gyberg, V.; Abreu, A.; Aguiar, C.; Conde, A.C.; Davletov, K.; et al. On Behalf Of The Euroaspire, I., Lifestyle and risk factor management in people at high risk of cardiovascular disease. A report from the European Society of Cardiology European Action on Secondary and Primary Prevention by Intervention to Reduce Events (EUROASPIRE) IV cross-sectional survey in 14 European regions. Eur. J. Prev. Cardiol. 2016, 23, 2007–2018. [Google Scholar]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Pandey, A.; Salahuddin, U.; Garg, S.; Ayers, C.; Kulinski, J.; Anand, V.; Mayo, H.; Kumbhani, D.J.; de Lemos, J.; Berry, J.D. Continuous Dose-Response Association Between Sedentary Time and Risk for Cardiovascular Disease: A Meta-analysis. JAMA Cardiol. 2016, 1, 575–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, S.A.; Blanchard, C.M.; Grace, S.L.; Reid, R.D. Objectively-measured sedentary time and its association with markers of cardiometabolic health and fitness among cardiac rehabilitation graduates. Eur. J. Prev. Cardiol. 2016, 23, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Rana, J.S.; Liu, J.Y.; Moffet, H.H.; Karter, A.J.; Nasir, K.; Solomon, M.D.; Jaffe, M.G.; Ambrosy, A.P.; Go, A.S.; Sidney, S. Risk of atherosclerotic cardiovascular disease by cardiovascular health metric categories in approximately 1 million patients. Eur J. Prev. Cardiol. 2020, 28, 29–32. [Google Scholar] [CrossRef]
- Biscaglia, S.; Campo, G.; Sorbets, E.; Ford, I.; Fox, K.M.; Greenlaw, N.; Parkhomenko, A.; Tardif, J.-C.; Tavazzi, L.; Tendera, M.; et al. Relationship between physical activity and long-term outcomes in patients with stable coronary artery disease. Eur. J. Prev. Cardiol. 2020, 27, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Lechner, K.; von Schacky, C.; McKenzie, A.L.; Worm, N.; Nixdorff, U.; Lechner, B.; Kränkel, N.; Halle, M.; Krauss, R.M.; Scherr, J. Lifestyle factors and high-risk atherosclerosis: Pathways and mechanisms beyond traditional risk factors. Eur. J. Prev. Cardiol. 2020, 27, 394–406. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Butler, E.N.; Rosamond, W.D. Prevalence of physical activity and sedentary behavior among adults with cardiovascular disease in the United States. J. Cardiopulm. Rehabil. Prev. 2014, 34, 406–419. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Jensen, M.T.; Treskes, R.W.; Caiani, E.G.; Casado-Arroyo, R.; Cowie, M.R.; Dilaveris, P.; Duncker, D.; Di Rienzo, M.; Frederix, I.; De Groot, N.; et al. ESC working group on e-cardiology position paper: Use of commercially available wearable technology for heart rate and activity tracking in primary and secondary cardiovascular prevention—in collaboration with the European Heart Rhythm Association, European Association of Preventive Cardiology, Association of Cardiovascular Nursing and Allied Professionals, Patient Forum, and the Digital Health Committee. Eur. Heart J. - Digit. Health, 2021; 2, 49–59. [Google Scholar]
- Scherrenberg, M.; Wilhelm, M.; Hansen, D.; Völler, H.; Cornelissen, V.; Frederix, I.; Kemps, H.; Dendale, P. The future is now: A call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2020, 28, 524–540. [Google Scholar] [CrossRef] [PubMed]
- Shakhovska, N.; Fedushko, S.; Greguš ml, M.; Melnykova, N.; Shvorob, I.; Syerov, Y. Big Data analysis in development of personalized medical system. Procedia Comput. Sci. 2019, 160, 229–234. [Google Scholar] [CrossRef]
- Scherrenberg, M.; Falter, M.; Dendale, P. Providing comprehensive cardiac rehabilitation during and after the COVID-19 pandemic. Eur. J. Prev. Cardiol. 2020, 28, 520–521. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.J.; Wang, Y.-T.L.; Low, T.T. Have a heart during the COVID-19 crisis: Making the case for cardiac rehabilitation in the face of an ongoing pandemic. Eur. J. Prev. Cardiol. 2020, 27, 903–905. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Koenigstorfer, J. Determinants of physical activity maintenance during the Covid-19 pandemic: A focus on fitness apps. Transl. Behav. Med. 2020, 10, 835–842. [Google Scholar] [CrossRef]
- Bakker, E.A.; Hartman, Y.A.W.; Hopman, M.T.E.; Hopkins, N.D.; Graves, L.E.F.; Dunstan, D.W.; Healy, G.N.; Eijsvogels, T.M.H.; Thijssen, D.H.J. Validity and reliability of subjective methods to assess sedentary behaviour in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 75. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MVPA (min/day) Estimate (95% CI) | p | |||
|---|---|---|---|---|
| Questionnaire timepoint | ||||
| Q1—April (ref) | 0 | |||
| Q2—May | 7.2 (−1.9; 16.2) | 0.12 | ||
| Q3—June | 7.4 (−2.0; 16.8) | 0.12 | ||
| Q4—July | 2.9 (−6.6; 12.5) | 0.55 | ||
| Sex | ||||
| Male (ref) | 0 | |||
| Female | −41.4 (−49.2; −33.7) | <0.001 | ||
| CVD subtype | ||||
| Myocardial infarction (ref) | 0 | |||
| Angina pectoris | 4.8 (−4.4; 14.1) | 0.31 | ||
| Heart valve disease | −1.2 (−14.1; 11.4) | 0.85 | ||
| Heart failure | −23.0 (−36.5; −9.5) | 0.001 | ||
| Other * | −0.9 (−10.5; 8.7) | 0.85 | ||
| Extent of being impeded by: | ||||
| Fear of a COVID-19 infection | ||||
| Low (ref) | 0 | |||
| Moderate | −7.4 (−17.3; 2.4) | 0.14 | ||
| High | −16.9 (−24.7; −9.1) | <0.001 | ||
| Limited possibilities for physical activity | ||||
| Low (ref) | 0 | |||
| Moderate | −23.3 (−34.8; −11.9) | <0.001 | ||
| High | −18.2 (−25.9; −10.6) | <0.001 | ||
| Sedentary Time (min/Day) Estimate (95% CI) | p | |||
|---|---|---|---|---|
| Questionnaire timepoint | ||||
| Q1—April (ref) | 0 | |||
| Q2—May | 10.0 (−8.7; 28.7) | 0.29 | ||
| Q3—June | 19.7 (0.4; 39.0) | 0.045 | ||
| Q4—July | 25.2 (5.4; 47.1) | 0.013 | ||
| Age (years) * | −2.1 (−2.8; −1.3) | <0.001 | ||
| Extent of being impeded by: | ||||
| Lack of social contact | ||||
| Low (ref) | 0 | |||
| Moderate | 13.0 (−11.3; 37.4) | 0.30 | ||
| High | 23.3 (6.6; 40.1) | 0.006 | ||
| Limited possibilities for physical activity | ||||
| Low (ref) | 0 | |||
| Moderate | 15.1 (−8.9; 37.4) | 0.22 | ||
| High | 41.4 (24.9; 57.8) | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11929. https://doi.org/10.3390/ijerph182211929
van Bakel BMA, Bakker EA, de Vries F, Thijssen DHJ, Eijsvogels TMH. Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(22):11929. https://doi.org/10.3390/ijerph182211929
Chicago/Turabian Stylevan Bakel, Bram M.A., Esmée A. Bakker, Femke de Vries, Dick H.J. Thijssen, and Thijs M.H. Eijsvogels. 2021. "Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown" International Journal of Environmental Research and Public Health 18, no. 22: 11929. https://doi.org/10.3390/ijerph182211929
APA Stylevan Bakel, B. M. A., Bakker, E. A., de Vries, F., Thijssen, D. H. J., & Eijsvogels, T. M. H. (2021). Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. International Journal of Environmental Research and Public Health, 18(22), 11929. https://doi.org/10.3390/ijerph182211929