
Exploring the Association between Alcohol Drinking and Physical Activity in Adolescence; Two-Year Prospective Study in Younger Adolescents from Bosnia and Herzegovina

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
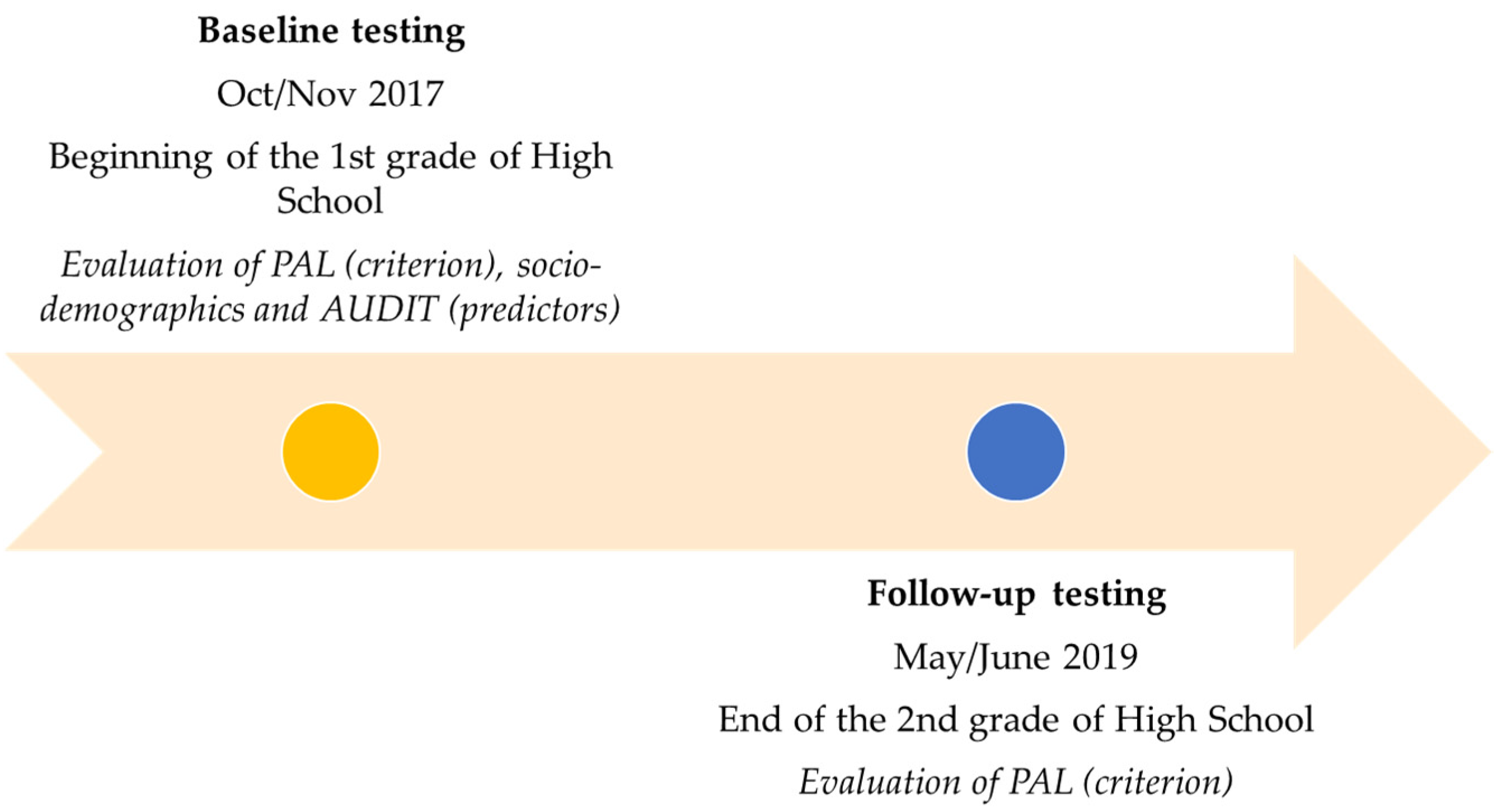
2.1. Participants and Study Design
2.2. Variables
2.3. Statistics
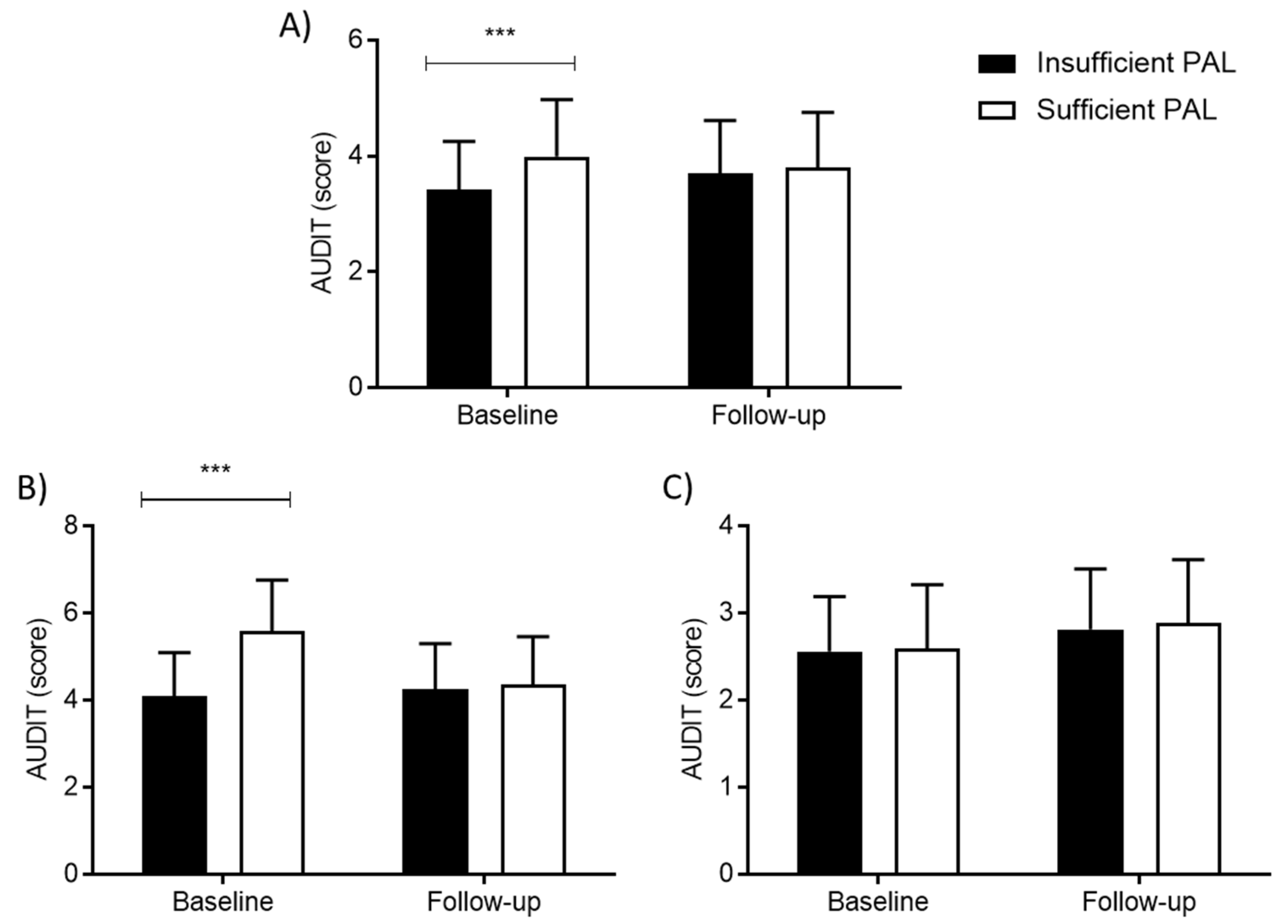
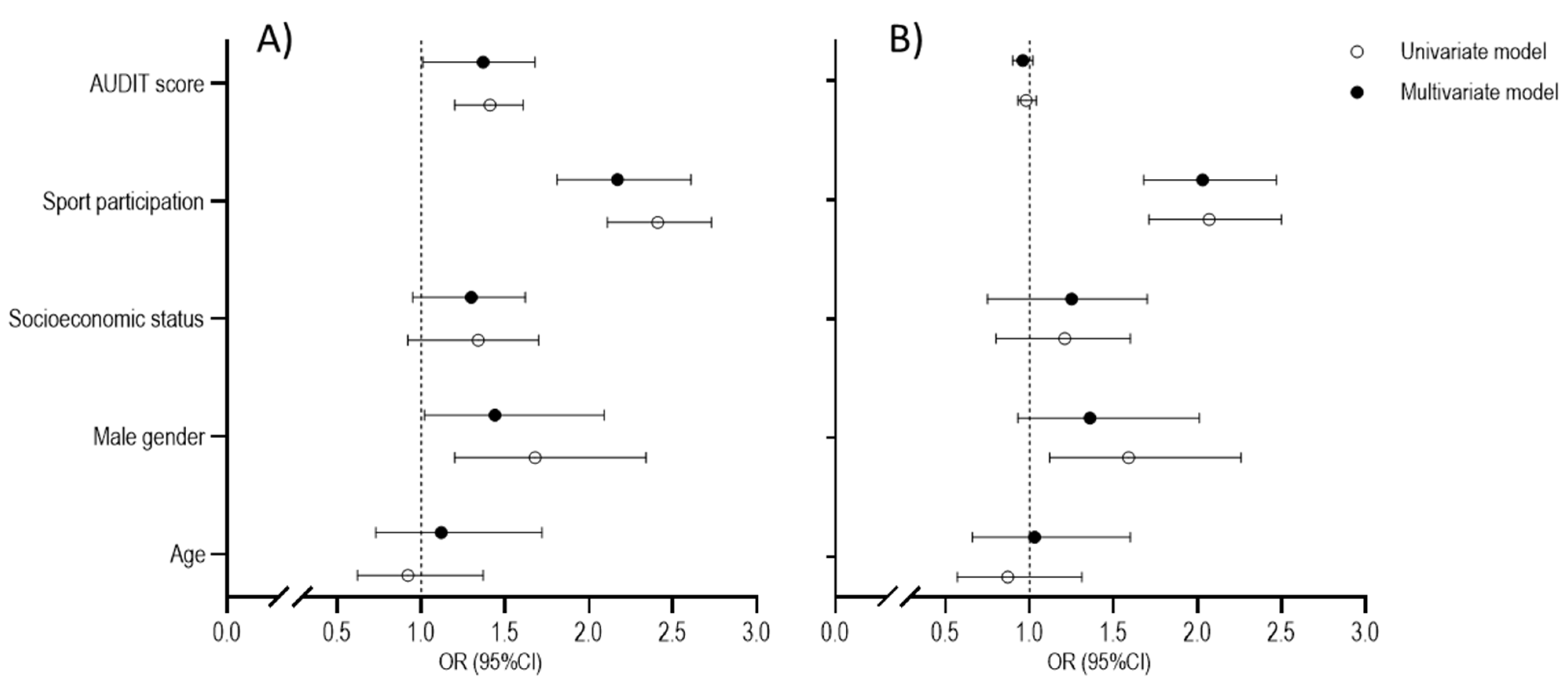
3. Results
4. Discussion
4.1. Alcohol and PAL
4.2. Alcohol and PAL Changes
4.3. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Nunes, H.E.G.; Gonçalves, E.C.D.A.; Vieira, J.A.J.; Silva, D.A.S. Clustering of Risk Factors for Non-Communicable Diseases among Adolescents from Southern Brazil. PLoS ONE 2016, 11, e0159037. [Google Scholar] [CrossRef]
- Dong, X.; Ding, M.; Chen, W.; Liu, Z.; Yi, X. Relationship between Smoking, Physical Activity, Screen Time, and Quality of Life among Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 8043. [Google Scholar] [CrossRef]
- Jochimek, M.; Łada, A.B. Help or hindrance: The relationship of physical activity with aggressiveness and self-esteem in 16-year-old adolescents. Health Psychol. Rep. 2019, 7, 242–253. [Google Scholar] [CrossRef]
- Kumar, B.; Robinson, R.; Till, S. Physical activity and health in adolescence. Clin. Med. 2015, 15, 267–272. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Grao-Cruces, A.; Velázquez-Romero, M.J.; Rodriguez-Rodríguez, F. Levels of Physical Activity during School Hours in Children and Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4773. [Google Scholar] [CrossRef] [PubMed]
- Jakubec, L.; Frömel, K.; Chmelík, F.; Groffik, D. Physical Activity in 15–17-Year-Old Adolescents as Compensation for Sedentary Behavior in School. Int. J. Environ. Res. Public Health 2020, 17, 3281. [Google Scholar] [CrossRef]
- Damjanovic, V.M.; Salcin, L.O.; Zenic, N.; Foretic, N.; Liposek, S. Identifying Predictors of Changes in Physical Activity Level in Adolescence: A Prospective Analysis in Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2019, 16, 2573. [Google Scholar] [CrossRef]
- Sekulic, D.; Rodek, J.; Sattler, T. Factors associated with physical activity levels in late adolescence: A prospective study. Med. Pract. 2020, 71, 637–647. [Google Scholar] [CrossRef]
- Wartberg, L.; Kammerl, R. Empirical Relationships between Problematic Alcohol Use and a Problematic Use of Video Games, Social Media and the Internet and Their Associations to Mental Health in Adolescence. Int. J. Environ. Res. Public Health 2020, 17, 6098. [Google Scholar] [CrossRef]
- de Moura, L.R.; Torres, L.M.; Cadete, M.M.M.; Cunha, C.D.F. Fatores associados aos comportamentos de risco à saúde entre adolescentes brasileiros: Uma revisão integrativa. Rev. Esc. Enferm. USP 2018, 52, e03304. [Google Scholar] [CrossRef]
- Engels, R.; Bogt, T.T. Influences of Risk Behaviors on the Quality of Peer Relations in Adolescence. J. Youth Adolesc. 2001, 30, 675–695. [Google Scholar] [CrossRef]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; De Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.; Barnekow, V. Social Determinants of Health and Well-Being among Young People: Health Behaviour in School-Aged Children (HBSC); International report from the 2009/2010 survey; World Health Organization: Geneve, Switzerland, 2010; p. 271. [Google Scholar]
- Devcic, S.; Sekulic, D.; Ban, D.; Kutlesa, Z.; Rodek, J.; Sajber, D. Evidencing Protective and Risk Factors for Harmful Alcohol Drinking in Adolescence: A Prospective Analysis of Sport-Participation and Scholastic-Achievement in Older Adolescents from Croatia. Int. J. Environ. Res. Public Health 2018, 15, 986. [Google Scholar] [CrossRef]
- Tahiraj, E.; Cubela, M.; Ostojic, L.; Rodek, J.; Zenic, N.; Sekulic, D.; Lesnik, B. Prevalence and Factors Associated with Substance Use and Misuse among Kosovar Adolescents; Cross Sectional Study of Scholastic, Familial-, and Sports-Related Factors of Influence. Int. J. Environ. Res. Public Health 2016, 13, 502. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Terzic, A.; Rodek, J.; Spasic, M.; Sekulic, D. Gender-Specific Analyses of the Prevalence and Factors Associated with Substance Use and Misuse among Bosniak Adolescents. Int. J. Environ. Res. Public Health 2015, 12, 6626–6640. [Google Scholar] [CrossRef]
- Hibell, B.; Guttormsson, U.; Ahlstrom, S. The 2011 ESPAD Report: Substance Use amongst Students in 36 European Countries; EPSAD: Stockholm, Sweden, 2012. [Google Scholar]
- Lees, B.; Meredith, L.; Kirkland, A.E.; Bryant, B.E.; Squeglia, L.M. Effect of alcohol use on the adolescent brain and behavior. Pharmacol. Biochem. Behav. 2020, 192, 172906. [Google Scholar] [CrossRef]
- Piazza-Gardner, A.K.; Barry, A. Examining Physical Activity Levels and Alcohol Consumption: Are People Who Drink More Active? Am. J. Health Promot. 2012, 26, e95–e104. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Werch, C. Relationship between Vigorous Exercise Frequency and Substance Use among First-Year Drinking College Students. J. Am. Coll. Health 2008, 56, 686–690. [Google Scholar] [CrossRef]
- Sajber, D.; Tahiraj, E.; Zenic, N.; Peric, M.; Sekulic, D. Alcohol drinking among Kosovar adolescents: An examination of gender-specific sociodemographic, sport, and familial factors associated with harmful drinking. Subst. Use Misuse. 2016, 51, 533–539. [Google Scholar] [CrossRef]
- Kwan, M.; Bobko, S.; Faulkner, G.; Donnelly, P.; Cairney, J. Sport participation and alcohol and illicit drug use in adolescents and young adults: A systematic review of longitudinal studies. Addict. Behav. 2013, 39, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, H.; Eslami, B. Relationship between Obesity, Physical Activity, and Cardiorespiratory Fitness Levels in Children and Adolescents in Bosnia and Herzegovina: An Analysis of Gender Differences. Front. Physiol. 2018, 9, 1734. [Google Scholar] [CrossRef]
- Cerkez, I.; Culjak, Z.; Zenic, N.; Sekulic, D.; Kondric, M. Harmful alcohol drinking among adolescents: The influence of sport participation, religiosity, and parental factors. J. Child Adolesc. Subst. Abuse 2015, 24, 94–101. [Google Scholar] [CrossRef]
- Sekulic, D.; Ostojic, M.; Ostojic, Z.; Hajdarevic, B.; Ostojic, L. Substance abuse prevalence and its relation to scholastic achievement and sport factors: An analysis among adolescents of the Herzegovina–Neretva Canton in Bosnia and Herzegovina. BMC Public Health 2012, 12, 274. [Google Scholar] [CrossRef] [PubMed]
- Quintero, L.A.M.; Jiménez, M.D.L.V.M.; Rojas-Solís, J.L.; Molleda, C.B.; Chilaca, A.S.; Díaz, F.J.R. Psychometric properties of the Alcohol Use Disorder Identification Test (AUDIT) in adolescents and young adults from Southern Mexico. Alcohol 2019, 81, 39–46. [Google Scholar] [CrossRef]
- Santis, R.; Garmendia, M.L.; Acuña, G.; Alvarado, M.E.; Arteaga, O. The Alcohol Use Disorders Identification Test (AUDIT) as a screening instrument for adolescents. Drug Alcohol Depend. 2009, 103, 155–158. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.; Donen, R.M. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual; College of Kinesiology, University of Saskatchewan: Saskatoon, SK, Canada, 2004; Volume 87, pp. 1–38. [Google Scholar]
- Benítez-Porres, J.; Alvero-Cruz, J.R.; Sardinha, L.; López-Fernández, I.; Carnero, E.A. Cut-off values for classifying active children and adolescentes using the Physical Activity Questionnaire: PAQ-C and PAQ-A. Nutr. Hosp. 2016, 33, 564. [Google Scholar] [CrossRef]
- Gilic, B.; Zenic, N.; Separovic, V.; Savicevic, A.J.; Sekulic, D. Evidencing the influence of pre-pandemic sports participation and substance misuse on physical activity during the COVID-19 lockdown: A prospective analysis among older adolescents. Int. J. Occup. Med. Environ. Health 2021, 34, 151–163. [Google Scholar] [CrossRef]
- Ricardo, C.Z.; Azeredo, C.M.; De Rezende, L.F.M.; Levy, R.B. Co-occurrence and clustering of the four major non-communicable disease risk factors in Brazilian adolescents: Analysis of a national school-based survey. PLoS ONE 2019, 14, e0219370. [Google Scholar] [CrossRef]
- Pawlowska, A.; Lipowska, K.; Krokosz, D. Too masculine for healthcare, too feminine for intense sports: Correlation between gender conformity and pro-health behaviours. Balt. J. Health Phys. Act. 2021, 13, 29–41. [Google Scholar] [CrossRef]
- Modric, T.; Zenic, N.; Sekulic, D. Substance Use and Misuse Among 17- to 18-Year-Old Croatian Adolescents: Correlation with Scholastic Variables and Sport Factors. Subst. Use Misuse 2011, 46, 1328–1334. [Google Scholar] [CrossRef]
- O’Brien, K.S.; Ali, A.; Cotter, J.D.; O’Shea, R.P.; Stannard, S. Hazardous drinking in New Zealand sportspeople: Level of sporting participation and drinking motives. Alcohol. Alcohol. 2007, 42, 376–382. [Google Scholar] [CrossRef]
- Rodek, J.; Sekulic, D.; Pasalic, E. Can we consider religiousness as a protective factor against doping behavior in sport? J. Relig. Health 2009, 48, 445. [Google Scholar] [CrossRef]
- Boyes, R.; O’Sullivan, D.E.; Linden, B.; McIsaac, M.; Pickett, W. Gender-specific associations between involvement in team sport culture and canadian adolescents’ substance-use behavior. SSM Popul. Health 2017, 3, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; de Bruijn, A.; Angus, K.; Gordon, R.; Hastings, G. Impact of Alcohol Advertising and Media Exposure on Adolescent Alcohol Use: A Systematic Review of Longitudinal Studies. Alcohol Alcohol. 2009, 44, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Lipowski, M.; Lipowska, M.; Jochimek, M.; Krokosz, D. Resiliency as a factor protecting youths from risky behaviour: Moderating effects of gender and sport. Eur. J. Sport Sci. 2016, 16, 246–255. [Google Scholar] [CrossRef]
- Lisha, N.E.; Sussman, S. Relationship of high school and college sports participation with alcohol, tobacco, and illicit drug use: A review. Addict. Behav. 2010, 35, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Wichstrøm, T.; Wichstrøm, L. Does sports participation during adolescence prevent later alcohol, tobacco and cannabis use? Addiction 2009, 104, 138–149. [Google Scholar] [CrossRef]
- Madden, P.A.; Grube, J. The frequency and nature of alcohol and tobacco advertising in televised sports, 1990 through 1992. Am. J. Public Health 1994, 84, 297–299. [Google Scholar] [CrossRef][Green Version]
- Turner, J.C.; Oakes, P.J. The significance of the social identity concept for social psychology with reference to individualism, interactionism and social influence. Br. J. Soc. Psychol. 1986, 25, 237–252. [Google Scholar] [CrossRef]
- Newman, B.M.; Lohman, B.J.; Newman, P.R. Peer group membership and a sense of belonging: Their relationship to adolescent behavior problems. Adolescence 2007, 42, 241–263. [Google Scholar] [PubMed]
- Connell, C.M.; Gilreath, T.D.; Aklin, W.M.; Brex, R.A. Social-Ecological Influences on Patterns of Substance Use among Non-Metropolitan High School Students. Am. J. Community Psychol. 2010, 45, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Hope, A. ‘Lead Us Not into Temptation’: Adolescence and Alcohol Policy in Europe. Alcohol Alcohol. 2014, 49, 126–127. [Google Scholar] [CrossRef]
- Wickel, E.E.; Eisenmann, J.C. Contribution of Youth Sport to Total Daily Physical Activity among 6- to 12-yr-old Boys. Med. Sci. Sports Exerc. 2007, 39, 1493–1500. [Google Scholar] [CrossRef]
- Machado-Rodrigues, A.M.; Silva, M.J.C.E.; Mota, J.; Santos, R.M.; Cumming, S.P.; Malina, R.M. Physical Activity and Energy Expenditure in Adolescent Male Sport Participants and Nonparticipants Aged 13 to 16 Years. J. Phys. Act. Health 2012, 9, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Crane, J.; Temple, V. A systematic review of dropout from organized sport among children and youth. Eur. Phys. Educ. Rev. 2014, 21, 114–131. [Google Scholar] [CrossRef]
- MacArthur, G.J.; Smith, M.C.; Melotti, R.; Heron, J.; Macleod, J.; Hickman, M.; Kipping, R.R.; Campbell, R.; Lewis, G. Patterns of alcohol use and multiple risk behaviour by gender during early and late adolescence: The ALSPAC cohort. J. Public Health 2012, 34 (Suppl. 1), i20–i30. [Google Scholar] [CrossRef]
- Wang, M.; Zhong, J.-M.; Wang, H.; Zhao, M.; Gong, W.-W.; Pan, J.; Fei, F.-R.; Wu, H.-B.; Yu, M. Breakfast Consumption and Its Associations with Health-Related Behaviors among School-Aged Adolescents: A Cross-Sectional Study in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2016, 13, 761. [Google Scholar] [CrossRef]
- Ostojic, S. Maturational advantage of early maturers in youth sport. Med. Sport Riv. Fisiopatol. Sport 2017, 70, 186–190. [Google Scholar] [CrossRef]
- Kaltiala-Heino, R.; Koivisto, A.-M.; Marttunen, M.; Fröjd, S. Pubertal Timing and Substance Use in Middle Adolescence: A 2-Year Follow-up Study. J. Youth Adolesc. 2011, 40, 1288–1301. [Google Scholar] [CrossRef]
- Costello, E.J.; Sung, M.; Worthman, C.M.; Angold, A. Pubertal maturation and the development of alcohol use and abuse. Drug Alcohol Depend. 2007, 88 (Suppl. 1), S50–S59. [Google Scholar] [CrossRef] [PubMed]
- Vest, A.E.; Simpkins, S.D. When Is Sport Participation Risky or Protective for Alcohol Use? The Role of Teammates, Friendships, and Popularity. New Dir. Child Adolesc. Dev. 2013, 2013, 37–55. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | PAL Baseline | PAL Follow-Up | ||||
|---|---|---|---|---|---|---|
| Insufficiency | Sufficiency | χ2 | Insufficiency | Sufficiency | χ2 | |
| F (%) | F (%) | (p) | F (%) | F (%) | (p) | |
| Gender | ||||||
| Boys | 208 (62.65) | 124 (37.35) | 8.7 | 229 (69) | 262 (77.7) | 6.58 |
| Girls | 247 (73.3) | 90 (26.7) | (0.01) | 103 (31) | 75 (22.3) | (0.02) |
| Sport participation | ||||||
| No | 389 (75.6) | 125 (24.3) | 59.97 | 413 (80.35) | 101 (19.64) | 54.98 |
| Yes | 66 (42.6) | 89 (57.4) | (0.001) | 78 (50.3) | 77 (49.67) | (0.001) |
| High Risk Group | Medium Risk Group | Low Risk Group | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Univariate regression | |||
| AUDIT score | 1.32 (1.11–1.54) | 1.01 (0.87–1.15) | REF |
| Male gender | 1.05 (0.35–2.89) | 0.49 (0.14–1.75) | REF |
| Socio-economic status | 1.00 (0.51–1.54) | 1.03 (0.61–1.45) | REF |
| Sport participation | 1.16 (0.87–1.42) | 1.36 (1.06–1.74) | REF |
| Age | 1.16 (0.74–1.83) | 1.02 (0.65–1.59) | REF |
| Multivariate regression | |||
| AUDIT | 1.25 (1.03–1.57) | 1.00 (0.90–1.11) | REF |
| Male gender | 1.30 (0.91–1.72) | 1.01 (0.62–1.40) | |
| Socio-economic status | 0.99 (0.41–1.60) | 1.03 (0.56–1.56) | |
| Sport participation | 1.08 (0.84–1.39) | 1.36 (1.04–1.75) | |
| Age | 1.14 (0.72–1.81) | 0.98 (0.62–1.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zenic, N.; Lipowska, M.; Maric, D.; Versic, S.; Vlahovic, H.; Gilic, B. Exploring the Association between Alcohol Drinking and Physical Activity in Adolescence; Two-Year Prospective Study in Younger Adolescents from Bosnia and Herzegovina. Int. J. Environ. Res. Public Health 2021, 18, 11899. https://doi.org/10.3390/ijerph182211899
Zenic N, Lipowska M, Maric D, Versic S, Vlahovic H, Gilic B. Exploring the Association between Alcohol Drinking and Physical Activity in Adolescence; Two-Year Prospective Study in Younger Adolescents from Bosnia and Herzegovina. International Journal of Environmental Research and Public Health. 2021; 18(22):11899. https://doi.org/10.3390/ijerph182211899
Chicago/Turabian StyleZenic, Natasa, Małgorzata Lipowska, Dora Maric, Sime Versic, Hrvoje Vlahovic, and Barbara Gilic. 2021. "Exploring the Association between Alcohol Drinking and Physical Activity in Adolescence; Two-Year Prospective Study in Younger Adolescents from Bosnia and Herzegovina" International Journal of Environmental Research and Public Health 18, no. 22: 11899. https://doi.org/10.3390/ijerph182211899
APA StyleZenic, N., Lipowska, M., Maric, D., Versic, S., Vlahovic, H., & Gilic, B. (2021). Exploring the Association between Alcohol Drinking and Physical Activity in Adolescence; Two-Year Prospective Study in Younger Adolescents from Bosnia and Herzegovina. International Journal of Environmental Research and Public Health, 18(22), 11899. https://doi.org/10.3390/ijerph182211899