
The 2019 Conference on Health and Active Transportation: Research Needs and Opportunities

 ,
,  , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. The Conference on Health and Active Transportation (CHAT) and Its Context
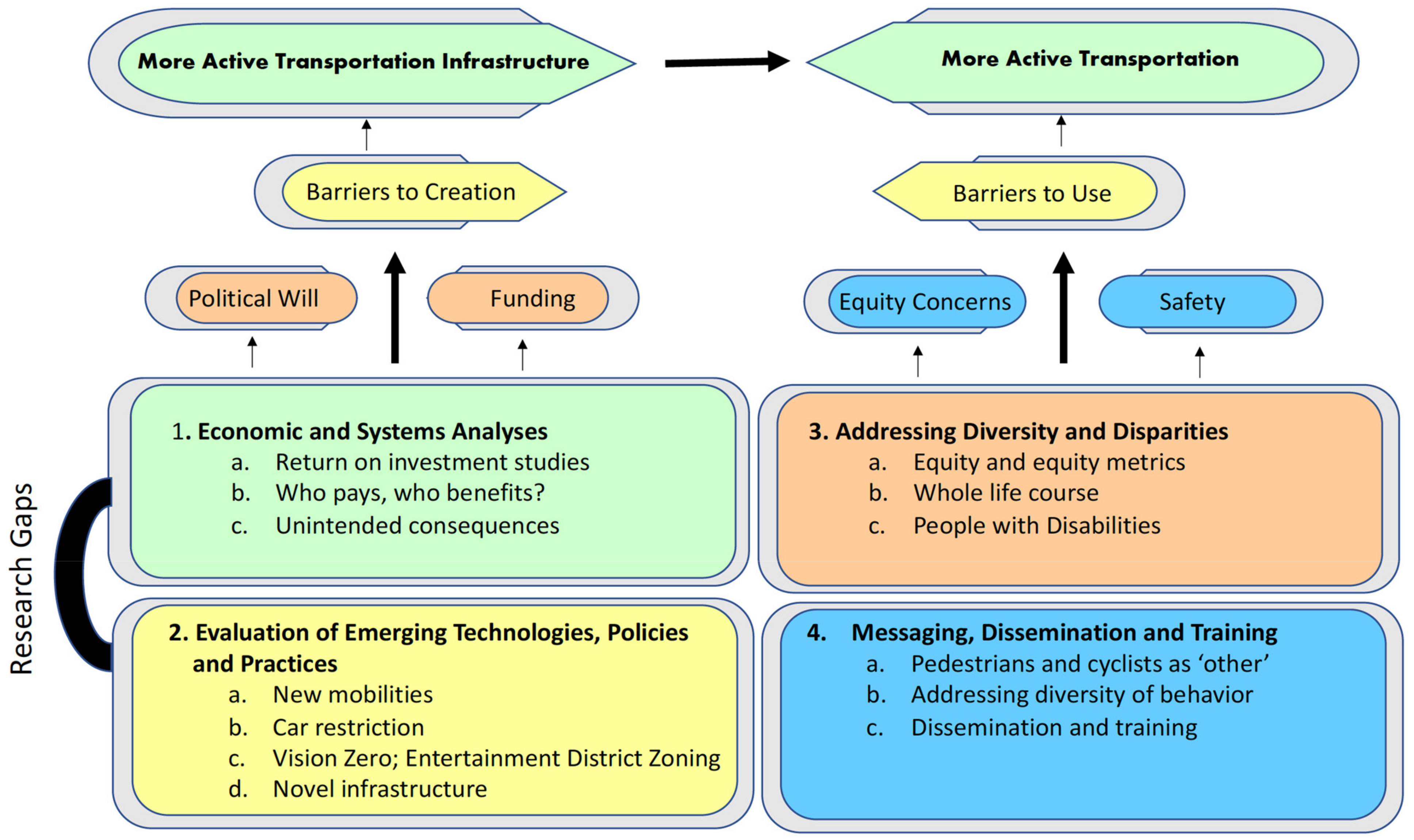
3. The CHAT Program and Research Gaps in Active Transportation
4. Innovative Practices, Building Strategic Institutional Relationships, and Cross-Cutting Needs
5. Active Transportation, Transit Equity and the COVID-19 Pandemic
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Sallis, J.F.; Frank, L.D.; Saelens, B.E.; Kraft, M.K. Active transportation and physical activity: Opportunities for collaboration on transportation and public health research. Transp. Res. Part A Policy Pract. 2004, 38, 249–268. [Google Scholar] [CrossRef]
- Berrigan, D.; Troiano, R.P.; McNeel, T.; Disogra, C.; Ballard-Barbash, R. Active transportation increases adherence to activity recommendations. Am. J. Prev. Med. 2006, 31, 210–216. [Google Scholar] [CrossRef] [PubMed]
- US Department of Transportation. Transportation and Health Tool. Available online: https://www.transportation.gov/transportation-health-tool (accessed on 9 November 2021).
- Carlson, S.A.; Whitfield, G.P.; Peterson, E.L.; Ussery, E.N.; Watson, K.B.; Berrigan, D.; Fulton, J.E. Geographic and Urban-Rural Differences in Walking for Leisure and Transportation. Am. J. Prev. Med. 2018, 55, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Watson, K.B.; Whitfield, G.P.; Thomas, J.V.; Berrigan, D.; Fulton, J.E.; Carlson, S.A. Associations between the National Walkability Index and walking among US Adults—National Health Interview Survey, 2015. Prev. Med. 2020, 137, 106122. [Google Scholar] [CrossRef]
- Langford, B.C.; Cherry, C.R.; Bassett, D.R.; Fitzhugh, E.C.; Dhakal, N. Comparing physical activity of pedal-assist electric bikes with walking and conventional bicycles. J. Transp. Health 2017, 6, 463–473. [Google Scholar] [CrossRef]
- Ussery, E.N.; Carlson, S.A.; Whitfield, G.P.; Watson, K.B.; Berrigan, D.; Fulton, J.E. Walking for Transportation or Leisure Among, U.S. Women and Men—National Health Interview Survey, 2005–2015. MMWR Morb. Mortal Wkly. Rep. 2017, 66, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Tribby, C.P.; Graubard, B.I.; Berrigan, D. National and metropolitan trends in public transit use, transit-related walking, and ridesharing between 2009 and 2017. J. Transport. Health 2020, 19, 100918. [Google Scholar] [CrossRef]
- Le, V.T.; Dannenberg, A.L. Moving Toward Physical Activity Targets by Walking to Transit: National Household Transportation Survey, 2001–2017. Am. J. Prev. Med. 2020, 59, e115–e123. [Google Scholar] [CrossRef]
- Buehler, R.; Pucher, J. The growing gap in pedestrian and cyclist fatality rates between the United States and the United Kingdom, Germany, Denmark, and The Netherlands, 1990–2018. Transport. Rev. 2020, 41, 48–72. [Google Scholar] [CrossRef]
- Khan, M.A.B.; Grivna, M.; Nauman, J.; Soteriades, E.S.; Cevik, A.A.; Hashim, M.J.; Govender, R.; Al Azeezi, S.R. Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. Int. J. Environ. Res. Public Health 2020, 17, 2135. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, A. Right of Way; Island Press: Washington, DC, USA, 2020; p. 248. [Google Scholar]
- MMWR. QuickStats: Age-Adjusted Pedestrian* Death Rates, (†) by Race/Ethnicity—National Vital Statistics System, United States, 2009 and 2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1434. [Google Scholar] [CrossRef]
- Goddard, T.; Kahn, K.B.; Adkins, A. Racial Bias in Driver Yielding Behavior at Crosswalks; Transportation Research and Education Center (TREC): Portland, OR, USA, 2014. [Google Scholar]
- Goddard, T.; Kahn, K.B.; Adkins, A. Racial Discrimination at the Crosswalks; Transportation Research and Education Center (TREC): Portland, OR, USA, 2015. [Google Scholar]
- Coughenour, C.; Clark, S.; Singh, A.; Claw, E.; Abelar, J.; Huebner, J. Examining racial bias as a potential factor in pedestrian crashes. Accid. Anal. Prev. 2017, 98, 96–100. [Google Scholar] [CrossRef]
- Buehler, R.; Pucher, J. COVID-19 Impacts on Cycling, 2019–2020. Transport. Rev. 2021, 41, 393–400. [Google Scholar] [CrossRef]
- ADA Information and Technical Assistance on the Americans with Disabilities Act. Available online: https://www.ada.gov (accessed on 1 November 2021).
- Roberts, J.D.; Dickinson, K.L.; Koebele, E.; Neuberger, L.; Banacos, N.; Blanch-Hartigan, D.; Welton-Mitchell, C.; Birkland, T.A. Clinicians, cooks, and cashiers: Examining health equity and the COVID-19 risks to essential workers. Toxicol. Ind. Health 2020, 36, 689–702. [Google Scholar] [CrossRef]
- Hu, M.; Roberts, J.D.; Azevedo, G.P.; Milner, D. The role of built and social environmental factors in Covid-19 transmission: A look at America’s capital city. Sustain. Cities Soc. 2021, 65, 102580. [Google Scholar] [CrossRef]
- Rodgers, K. Conference on Health and Active Transportation; Transportation Research Board: Washington DC, USA, 2020; Volume E-C264. [Google Scholar]
- Hunter, R.F.; Garcia, L.; Herick de SA, T.; Zapata-Diomedi, B.; Millet, C.; Woodcock, J.; Pentland, A.; Moro, E. Effect of COVID-19 response policies on walking behavior in US cities. Nat. Commun. 2021, 12, 3652. [Google Scholar] [CrossRef]
- Dunton, G.F.; Wang, S.D.; Do, B.; Courtney, J. Early effects of the COVID-19 pandemic on physical activity locations and behaviors in adults living in the United States. Prev. Med. Rep. 2020, 20, 101241. [Google Scholar] [CrossRef]
- Liu, L.; Miller, H.J.; Scheff, J. The impacts of COVID-19 pandemic on public transit demand in the United States. PLoS ONE 2020, 15, e0242476. [Google Scholar] [CrossRef]
- Moovit COVID-19 Impact on Public Transit Usage. Available online: https://moovitapp.com/insights/en/Moovit_Insights_Public_Transit_Index-countries (accessed on 28 April 2021).
- Steedly, A.T.; Lane, L.B.; Huston, B.; Danley, C. Connecting Transportation & Health: A Guide to Communication & Collaboration NCHRP Project 25-25, Task 105, National Cooperative Highway Research Program; National Academy of Sciences: Washington, DC, USA, 2019. [Google Scholar]
- Rojas-Rueda, D.; de Nazelle, A.; Andersen, Z.J.; Braun-Fahrländer, C.; Bruha, J.; Bruhova-Foltynova, H.; Desqueyroux, H.; Praznoczy, C.; Ragettli, M.S.; Tainio, M.; et al. Health Impacts of Active Transportation in Europe. PLoS ONE 2016, 11, e0149990. [Google Scholar] [CrossRef]
- Kahlmeier, S.; Boig, E.A.; Fernandez, A.C.; Smeds, E.; Benvenuti, F.; Eriksson, U.; Iacorossi, F.; Nieuwenhuijsen, M.J.; Int Panis, L.; Rojas-Rueda, D.; et al. Assessing the Policy Environment for Active Mobility in Cities-Development and Feasibility of the PASTA Cycling and Walking Policy Environment Score. Int. J. Environ. Res. Public Health 2021, 18, 986. [Google Scholar] [CrossRef]
- Habinger, J.G.; Chávez, J.L.; Matsudo, S.M.; Kovalskys, I.; Gómez, G.; Rigotti, A.; Sanabria, L.Y.C.; García, M.C.Y.; Pareja, R.G.; Herrera-Cuenca, M.; et al. Active Transportation and Obesity Indicators in Adults from Latin America: ELANS Multi-Country Study. Int. J. Environ. Res. Public Health 2020, 17, 6974. [Google Scholar] [CrossRef]
- Day, K. Built environmental correlates of physical activity in China: A review. Prev. Med. Rep. 2016, 3, 303–316. [Google Scholar] [CrossRef] [Green Version]
- Guan, C.H.; Srinivasan, S.; Zhang, B.; Da, L.J.; Liu, J.L.; Nielsen, C. The influence of neighborhood types on active transport in China’s growing cities. Transport. Res. D-Tr E 2020, 80, 102273. [Google Scholar] [CrossRef] [Green Version]
- Schneider, R.; Raynault, E.; Buehler, R. Assessing active transportation and health: Conference highlights innovative practices and research. TR News 2015, 299, 47–49. [Google Scholar]
- Bowles, R.; Anderson, G.S.; Vaughan, C. Building resilient communities: A facilitated discussion. J. Emerg. Manag. 2016, 14, 233–243. [Google Scholar] [CrossRef]
- AHRQ Digital Health Care Research: Multivoting. Available online: https://digital.ahrq.gov/health-it-tools-and-resources/evaluation-resources/workflow-assessment-health-it-toolkit/all-workflow-tools/multivoting (accessed on 18 January 2021).
- NASEM TRB Standing Committee on Transportation and Public Health. Available online: https://www.nationalacademies.org/event/07-29-2020/trb-standing-committee-on-transportation-and-public-health-mid-year-meeting (accessed on 18 January 2021).
- McAndrews, C.; Pollack, K.M.; Berrigan, D.; Dannenberg, A.L.; Christopher, E.J. Understanding and Improving Arterial Roads to Support Public Health and Transportation Goals. Am. J. Public Health 2017, 107, 1278–1282. [Google Scholar] [CrossRef] [PubMed]
- Transportation Research Board. Arterial Roadways Research needs and Concerns; Transportation Research Board: Washington, DC, USA, 2018; Volume E-C239. [Google Scholar]
- Christopher, E.; McAndrews, C. Improving Arterial Roads to Support Public Health: How Can We Do This? ITE J. 2018, 88, 13–16. [Google Scholar]
- National Academies of Sciences, Engineering, and Medicine. Implementing Strategies to Enhance Public Health Surveillance of Physical Activity in the United States; National Academies of Sciences, Engineering, and Medicine: Washington, DC, USA, 2019. [Google Scholar]
- Dunton, G.F.; Berrigan, D.; Young, D.R.; Pfeiffer, K.A.; Lee, S.M.; Slater, S.J.; Pate, R.R. Strategies to Improve Physical Activity Surveillance among Youth in the United States. J. Pediatr. 2019, 210, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Berrigan, D.; Christopher, E.; Dannenberg, A.; McAndrews, C.; Porter, K.P.; Sener, I.N.; Kochtitzky, C.; Rose, K. Public Health and Transportation Centennial Paper. Available online: http://onlinepubs.trb.org/onlinepubs/centennial/papers/ADD55TandADD50(1).pdf (accessed on 9 November 2021).
- Transportation Research Board. Research Roadmap for Transportation and Public Health; Research Report 932; Transportation Research Board: Washington, DC, USA, 2019. [Google Scholar]
- Dannenberg, A.L.; Rodriguez, D.A.; Sandt, L.S. Advancing Research in Transportation and Public Health: A Selection of Twenty Project Ideas from a U.S. Research Roadmap. J. Transport. Health 2021, 21, 1–10. [Google Scholar] [CrossRef]
- TRNEWS Number 299. Available online: http://onlinepubs.trb.org/onlinepubs/trnews/trnews299.pdf (accessed on 9 November 2021).
- Litman, T. Transportation and public health. Annu. Rev. Public Health 2013, 34, 217–233. [Google Scholar] [CrossRef] [Green Version]
- Frank, L.D.; Hong, A.; Ngo, V.D. Causal evaluation of urban greenway retrofit: A longitudinal study on physical activity and sedentary behavior. Prev. Med. 2019, 123, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Renalds, A.; Smith, T.H.; Hale, P.J. A systematic review of built environment and health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Peng, B.; Erdogan, S.; Nasri, A.N.; Zou, Z. Towards a health-conscious transportation planning: A framework for estimating health impacts of active transportation at local level. J. Transport. Health 2021, 22, 101231. [Google Scholar] [CrossRef]
- Sallis, J.F.; Floyd, M.F.; Rodríguez, D.A.; Saelens, B.E. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 2012, 125, 729–737. [Google Scholar] [CrossRef]
- Litman, T. Evaluating Active Transport Benefits and Costs: Guide to Valuing Walking and Cycling Improvements and Encouragement Programs; Victoria Transport Policy Institute: Victoria, BC, Canada, 2021. [Google Scholar]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Int Panis, L.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Culyer, A.J.; Chalkidou, K. Economic Evaluation for Health Investments En Route to Universal Health Coverage: Cost-Benefit Analysis or Cost-Effectiveness Analysis? Value Health 2019, 22, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.; Viney, R. Quality adjusted life years in the time of COVID-19. Aust. Health Rev. 2021, 45, 12–13. [Google Scholar] [CrossRef]
- Frank, L.D.; Iroz-Elardo, N.; MacLeod, K.E.; Hong, A. Pathways from built environment to health: A conceptual framework linking behavior and exposure-based impacts. J. Transport. Health 2019, 12, 319–335. [Google Scholar] [CrossRef]
- Zapata-Diomedi, B.; Herrera, A.M.; Veerman, J.L. The effects of built environment attributes on physical activity-related health and health care costs outcomes in Australia. Health Place 2016, 42, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Roux, L.; Pratt, M.; Tengs, T.O.; Yore, M.M.; Yanagawa, T.L.; van den Bos, J.; Rutt, C.; Brownson, R.C.; Powell, K.E.; Heath, G.; et al. Cost effectiveness of community-based physical activity interventions. Am. J. Prev. Med. 2008, 35, 578–588. [Google Scholar] [CrossRef]
- Pringle, A.; Cooke, C.; Gilson, N.; Marsh, K.; McKenna, J. Cost-effectiveness of interventions to improve moderate physical activity: A study in nine UK sites. Health Educ. J. 2010, 69, 211–224. [Google Scholar] [CrossRef] [Green Version]
- Toole, J. The History of the Three E’s. Available online: https://tooledesign.com/the-history-of-the-3-es/ (accessed on 28 April 2021).
- Plant, K.; McIllroy, R.C.; Stanton, N.A. Taking a ‘7 E’s’ Approach to Road Safety in the UK and Beyond. In Contemporary Ergonomics and Human Factors; Charles, R., Wilkinson, J., Eds.; CIEHF: Wootton Park, UK, 2018; pp. 1–8. [Google Scholar]
- Emmons, K.M.; Chambers, D.A. Policy Implementation Science—An Unexplored Strategy to Address Social Determinants of Health. Ethn. Dis. 2021, 31, 133–138. [Google Scholar] [CrossRef]
- Brown, A.; Manville, M.; Weber, A. Can mobility on demand bridge the first-last mile transit gap? Equity implications of Los Angeles’ pilot program. Transp. Res. Interdiscip. Perspect. 2021, 10, 100396. [Google Scholar] [CrossRef]
- Cochran, A.L.; Chatman, D.G. Use of app-based ridehailing services and conventional taxicabs by adults with disabilities. Travel Behav. Soc. 2021, 24, 124–131. [Google Scholar] [CrossRef]
- Alessio, H.M.; Reiman, T.; Kemper, B.; Carlowitz, W.; Bailer, A.J.; Timmerman, K.L. Metabolic and Cardiovascular Responses to a Simulated Commute on an E-Bike. Transl. J. ACSM 2021, 6, 1–6. [Google Scholar] [CrossRef]
- Bourne, J.E.; Sauchelli, S.; Perry, R.; Page, A.; Leary, S.; England, C.; Cooper, A.R. Health benefits of electrically-assisted cycling: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 116. [Google Scholar] [CrossRef]
- Fowler, S.L.; Berrigan, D.; Pollack, K.M. Perceived barriers to bicycling in an urban U.S. environment. J. Transport. Health 2016, 6, 474–480. [Google Scholar] [CrossRef]
- Ogilvie, D.; Adams, J.; Bauman, A.; Gregg, E.W.; Panter, J.; Siegel, K.R.; Wareham, N.J.; White, M. Using natural experimental studies to guide public health action: Turning the evidence-based medicine paradigm on its head. J. Epidemiol. Community Health 2020, 74, 203–208. [Google Scholar] [CrossRef] [Green Version]
- Carlson, J.A.; Hipp, J.A.; Kerr, J.; Horowitz, T.S.; Berrigan, D. Unique Views on Obesity-Related Behaviors and Environments: Research Using Still and Video Images. J. Meas. Phys. Behav. 2018, 1, 143–154. [Google Scholar] [CrossRef]
- Patterson, R.F.; Harley, R.A. Effects of Freeway Rerouting and Boulevard Replacement on Air Pollution Exposure and Neighborhood Attributes. Int. J. Environ. Res. Public Health 2019, 16, 4072. [Google Scholar] [CrossRef] [Green Version]
- Booth, L.; Norman, R.; Pettigrew, S. The potential implications of autonomous vehicles for active transport. J. Transport. Health 2019, 15, 1–9. [Google Scholar] [CrossRef]
- Pettigrew, S. The potential effects of autonomous vehicles on walking. Glob. Health Promot. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Khreis, H.; Frumkin, H. Autonomous Vehicles and Public Health. Annu. Rev. Public Health 2020, 41, 329–345. [Google Scholar] [CrossRef] [Green Version]
- Sohrabi, S.; Khreis, H.; Lord, D. Impacts of Autonomous Vehicles on Public Health: A Conceptual Model and Policy Recommendations. Sustain. Cities Soc. 2020, 63, 102457. [Google Scholar] [CrossRef]
- Spence, J.C.; Kim, Y.B.; Lamboglia, C.G.; Lindeman, C.; Mangan, A.J.; McCurdy, A.P.; Stearns, J.A.; Wohlers, B.; Sivak, A.; Clark, M.I. Potential Impact of Autonomous Vehicles on Movement Behavior: A Scoping Review. Am. J. Prev. Med. 2020, 58, e191–e199. [Google Scholar] [CrossRef]
- Botello, B.; Buehler, R.; Hankey, S.; Mondschein, A.; Jiang, Z. Planning for walking and cycling in an autonomous-vehicle future. Transp. Res. Interdiscip. Perspect. 2019, 1, 100012. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Wali, B.; Frank, L.D. Neighborhood-level COVID-19 hospitalizations and mortality relationships with built environment, active and sedentary travel. Health Place 2021, 71, 102659. [Google Scholar] [CrossRef] [PubMed]
- TransitCenter. Available online: https://transitcenter.org/2-8-million-u-s-essential-workers-ride-transit-to-their-jobs/ (accessed on 21 June 2021).
- Kinder, M.; Stateler, L. Essential Workers Comprise about Half of All Workers in Low-Paid Occupations. They Deserve a $15 Minimum Wage. Available online: https://www.brookings.edu/blog/the-avenue/2021/02/05/essential-workers-deserve-minimum-wage-increase/ (accessed on 21 June 2021).
- Car Access: Everyone Needs Reliable Transportation Access and in Most American Communities that Means a Car. Available online: https://nationalequityatlas.org/indicators/Car_access#/ (accessed on 21 June 2021).
- Frederick, C. America’s Addiction to Automobiles: Why Cities Need to Kick the Habit and How; Praeger: Westport, CT, USA, 2017. [Google Scholar]
- Combs, T.S.; Pardo, C.F. Shifting streets COVID-19 mobility data: Findings from a global dataset and a research agenda for transport planning and policy. Transp. Res. Interdiscip. Perspect. 2021, 9, 100322. [Google Scholar] [CrossRef]
- COVID-19 Transportation Resources. Available online: https://www.nationalacademies.org/topics/transportation-covid-19-resources (accessed on 7 May 2021).
- Zwald, M.L.; Fakhouri, T.H.I.; Fryar, C.D.; Whitfield, G.; Akinbami, L.J. Trends in active transportation and associations with cardiovascular disease risk factors among U.S. adults, 2007–2016. Prev. Med. 2018, 116, 150–156. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Activity | Scope | Citations |
|---|---|---|
| Transportation Research Board Moving Active Transportation to Higher Ground: Opportunities for Accelerating the Assessment of Health Impacts | “The main themes of the conference were policy and planning initiatives to increase active transportation, health impact assessments (HIAs), data collection and data analysis to quantify active transportation, and methods to forecast active transportation and its effects on health.” | Schneider et al. 2015 [32] |
| Arterial Roadways Research Needs and Concerns: Informing the Planning, Design, and Operation of Arterial Roadways Considering Public Health. Transportation Research Circular E-C239 | “The purpose of the Task Force was to inform the planning, design, and operation of arterials considering public health.” | McAndrews et al. 2017 [36] TRB E-C239, 2018 [37] Christopher and McAndrews, 2018 [38] |
| Implementing Strategies to Enhance Public Health Surveillance of Physical Activity in the United States (2019) | “An ad hoc committee will be convened to develop strategies that support the implementation of recommended actions to improve national physical activity surveillance. Specifically, the committee will: convene a group of experts who will examine and build on existing recommended actions in four topical areas (children and youth, community supports for active transportation, health care, and workplaces) to identify specific strategies for implementing those recommended actions; … “ | National Academies 2019 [39] Dunton et al. 2019 [40] |
| A Guidebook for Communications between Transportation and Public Health Communities | “The purpose of this study is to produce a user-friendly guidebook for state and local transportation professionals that identifies the challenges and best practices for successful communication and collaboration between transportation and public health professionals.” | Steedly et al. 2019 [26] |
| TRB Health and Transportation Subcommittee Centennial Paper | “The TRB Joint Subcommittee on Health and Transportation was created in 2011 to identify, advance and publish research and information to expand and improve current understanding and evaluation of the health impacts of federal, state, regional and local transportation policies, procedures and actions.” | Berrigan et al. 2019 [41] |
| National Cooperative Highway Research Program Research Report 932, “A Research Roadmap for Transportation and Public Health”. | “NCHRP Research Report 932 provides state departments of transportation, their transportation partners, and the public health community with a broad overview of highly relevant research needs at the intersection of transportation and public health in the United States.” | National Academies, 2019 [42] Dannenberg et al. 2021 [43] |
| Transportation Research Board 2019 Conference on Health and Active Transportation | “The purpose of this conference is to explore and collaborate on identifying impacts of the health effects of transportation policies, planning, and infrastructure, and to develop an understanding of the institutional opportunities and barriers for considering health within transportation field.” | Rodgers 2020 [21] This paper |
| Themes and Elements | Research Needs/Approaches | Key Collaborators |
|---|---|---|
| ||
| Community-based research Combine approaches from transportation metrics and health disparities tools Develop Health equity performance metrics | Partners from under-resourced communities Researchers from geriatrics, active transport to school, disability and health disparities arenas. |
| ||
| ||
| ||
| ||
| Greater multi-disciplinary collaboration Development, validation and dissemination of tools and methods Creative thinking about methods to address unintended consequences Development of joint transportation and health funding models | Transportation, health and ecological economists Systems modelers Social epidemiologists |
| ||
| ||
| ||
| ||
| Broad dissemination of experiences and results Evaluation of these “natural experiments” | Data scientists Policy researchers Dissemination and implementation research community |
| ||
| ||
| ||
| ||
| ||
| ||
| Explorations of the social psychology of transportation Risk perception and fatalism research Development and support for short- and long-term interdisciplinary training in transportation and health | Communications researchers Public opinion researchers Behavioral psychologists Educators Transportation and public health programs and courses at colleges and universities Planners at transportation agencies and transit agencies Transportation Demand Management planning and engagement staff Community engagement staff |
| ||
| ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berrigan, D.; Dannenberg, A.L.; Lee, M.; Rodgers, K.; Wojcik, J.R.; Wali, B.; Tribby, C.P.; Buehler, R.; Sallis, J.F.; Roberts, J.D.; et al. The 2019 Conference on Health and Active Transportation: Research Needs and Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 11842. https://doi.org/10.3390/ijerph182211842
Berrigan D, Dannenberg AL, Lee M, Rodgers K, Wojcik JR, Wali B, Tribby CP, Buehler R, Sallis JF, Roberts JD, et al. The 2019 Conference on Health and Active Transportation: Research Needs and Opportunities. International Journal of Environmental Research and Public Health. 2021; 18(22):11842. https://doi.org/10.3390/ijerph182211842
Chicago/Turabian StyleBerrigan, David, Andrew L. Dannenberg, Michelle Lee, Kelly Rodgers, Janet R. Wojcik, Behram Wali, Calvin P. Tribby, Ralph Buehler, James F. Sallis, Jennifer D. Roberts, and et al. 2021. "The 2019 Conference on Health and Active Transportation: Research Needs and Opportunities" International Journal of Environmental Research and Public Health 18, no. 22: 11842. https://doi.org/10.3390/ijerph182211842
APA StyleBerrigan, D., Dannenberg, A. L., Lee, M., Rodgers, K., Wojcik, J. R., Wali, B., Tribby, C. P., Buehler, R., Sallis, J. F., Roberts, J. D., Steedly, A., Peng, B., Eisenberg, Y., & Rodriguez, D. A. (2021). The 2019 Conference on Health and Active Transportation: Research Needs and Opportunities. International Journal of Environmental Research and Public Health, 18(22), 11842. https://doi.org/10.3390/ijerph182211842