
A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies
_Choi.png)
 ,
,  ,
, 
Abstract
:1. Introduction
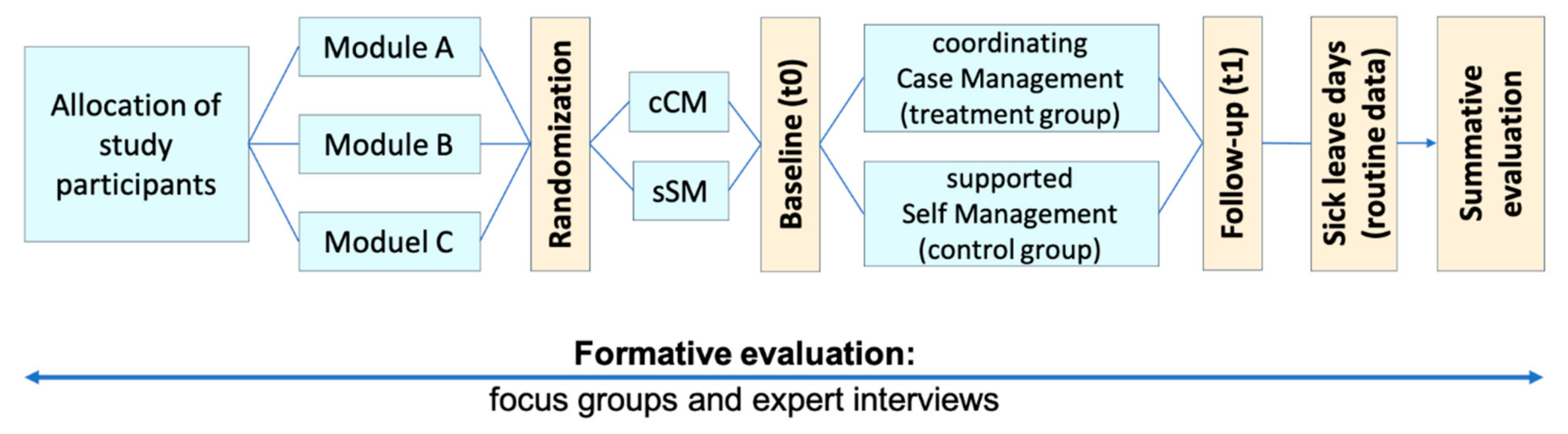
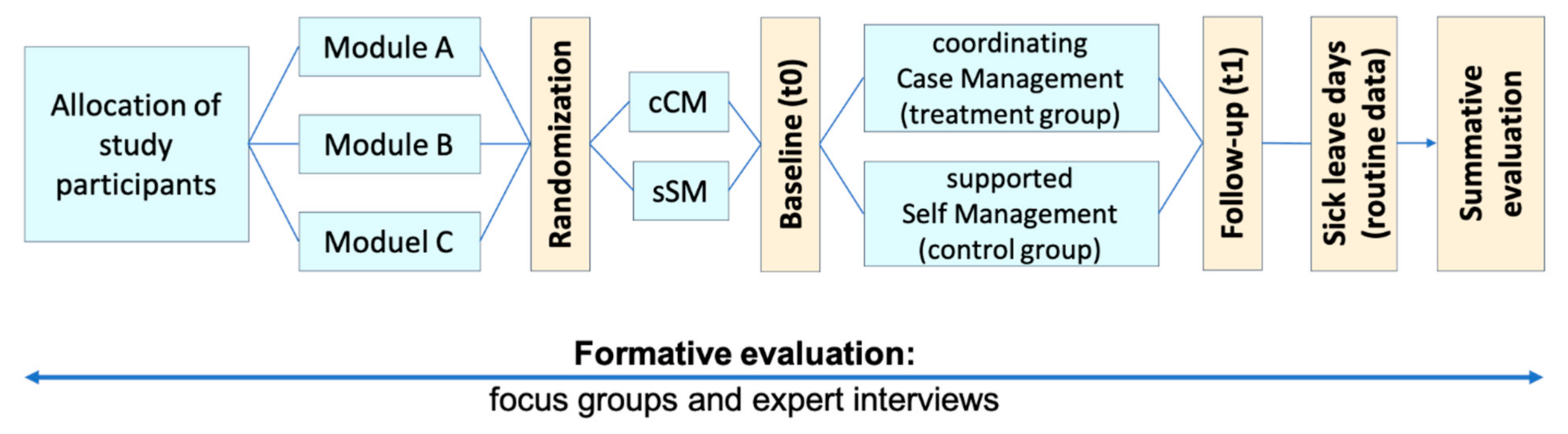
2. Materials and Methods
2.1. Summative/Result Evaluation
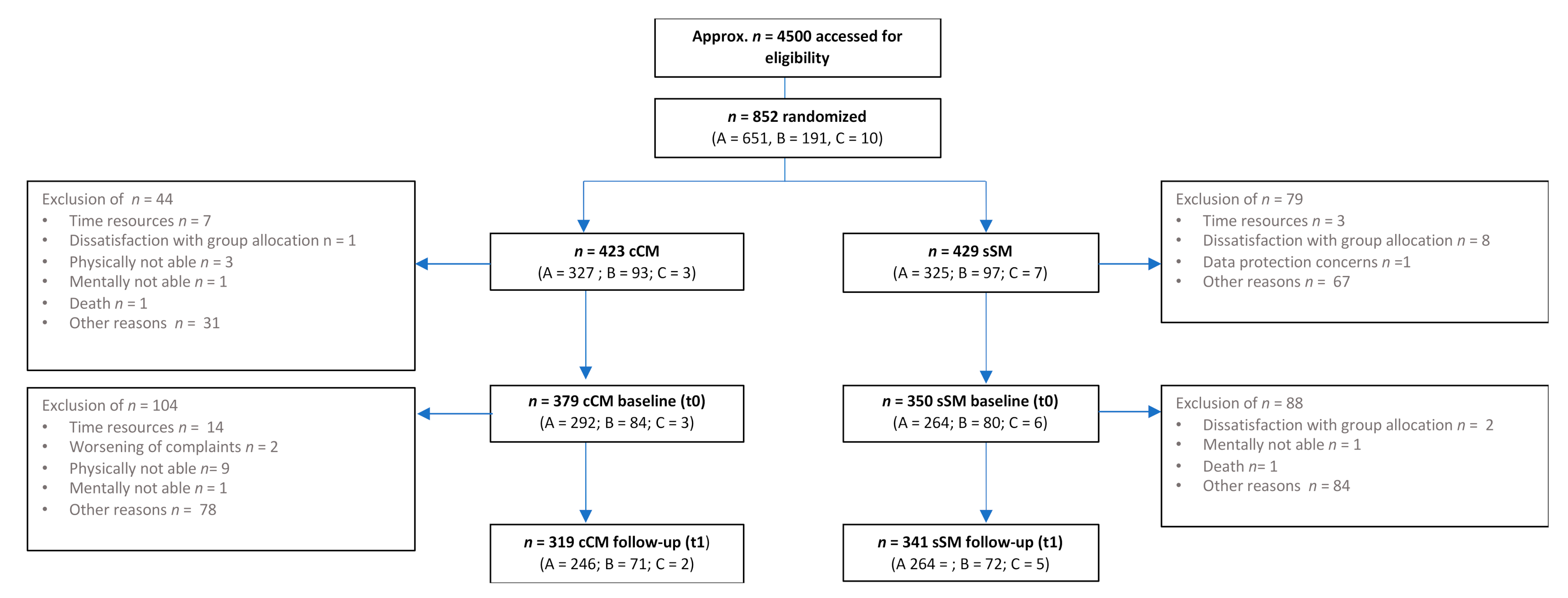
2.1.1. Accessing the Sample
2.1.2. Setting Procedure and Data Collection
2.1.3. Primary and Secondary Outcomes
2.1.4. Data Analysis
2.2. Formative/Process Evaluation
2.2.1. Accessing the Sample
2.2.2. Setting Procedure and Data Collection
2.2.3. Data Analysis
3. Results
3.1. Summative/Result Evaluation
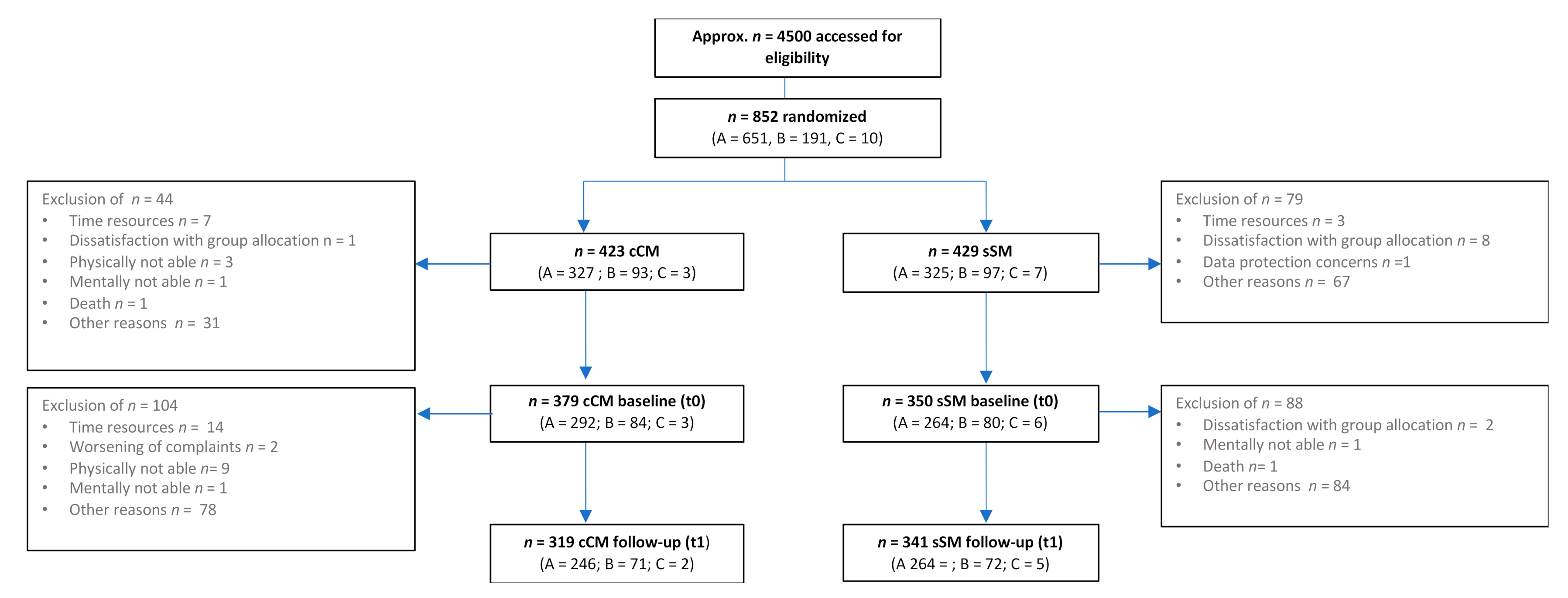
3.1.1. Sample
3.1.2. Overall
3.1.3. Module A
Primary and Secondary Outcomes
EFL, BMI, Pain VAS, PACT
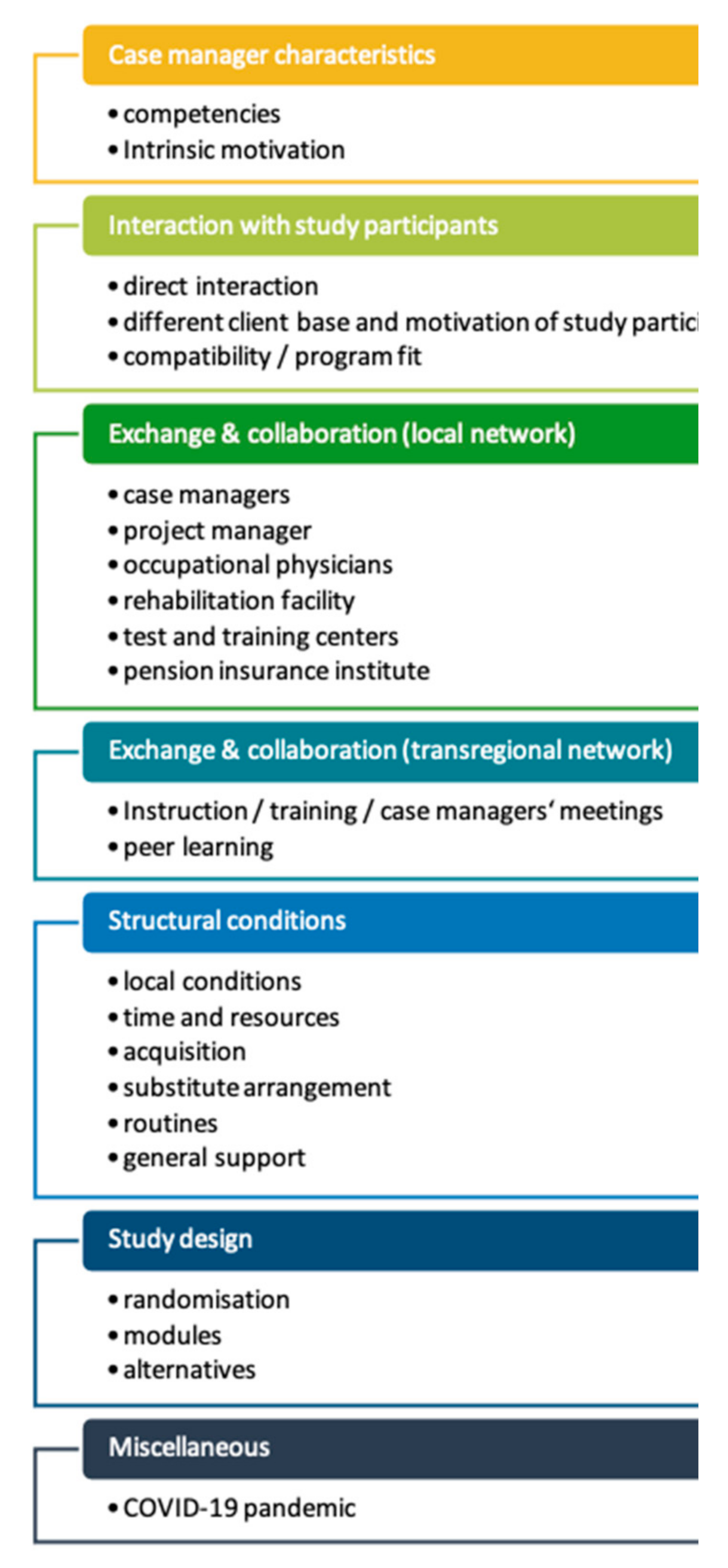
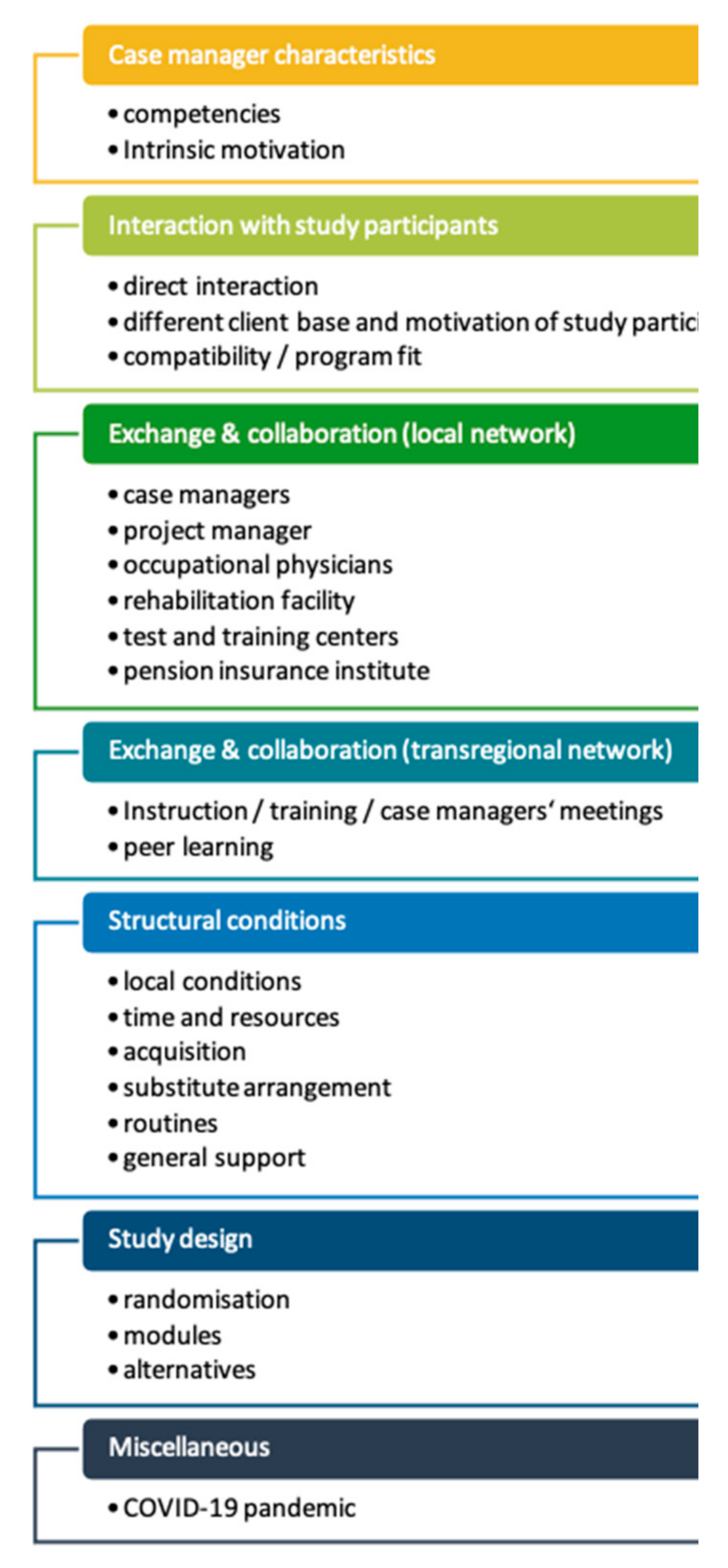
3.2. Formative/Process Evaluation
“Well, good communication skills are essential, proper empathy… to connect with others in their specific circumstances, not only concerning their diseases, but sometimes also their social environment. And you should a good time management—that’s really important”.(focus group with case managers)
“Within the last two months, I’ve been on my own for four weeks. The work load is too high. (…) If someone who is interested in the study approaches me, then okay… we can meet and talk, but apart from that (…) I’ll leave it”.(focus group with case managers)
“I sometimes almost feel personally related to our employees and I know a lot of them by name… I think, in this company, that’s a big advantage for me. They have a high level of trust in me”.(focus group with case managers)
“I can probably get office people to do something for their health two times a week faster than people working on the assembly line for nine hours, who are really tired in the evening […]. But there are also motivated people on the assembly line who say: ‘Nah, that is important to me and that is why I invest the time’ ”.(telephone interview with occupational physician)
“Well, it’s difficult, since most of the employees cannot complete the full training program because of regular business trips“.(focus group with case managers)
“Learning by doing and feedback—that’s always helpful!”.(focus group with case managers)
“Yes, I had contact to other occupational physicians of the project. Everything works fine, also with the other network partners: the test and training center, for example,… they have an important interface function for us”.(telephone interview with occupational physician)
“Missed meetings are a big issue. Our occupational physician did not attend the regional training. That caused a strange feeling“.(focus group with case managers)
“We have so many other early prevention courses, gymnastics and so on… that means they can choose whatever from a huge range—no matter, if there’re in the self-management group”.(focus group with case managers)
“It was off to a slow start, … advertisement could have been better, but now we’ve informed all employees and that made it a lot better”.(focus group with case managers)
“I had the support of our occupational physician, also from the personnel department. (…) But since the appearance of the pandemic, it’s all over. Most of them work from home… and we have short-time work now—it is a ghost town”.(focus group with case managers)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BeReKo | “Betriebliches Rehabilitationsprojekt” (observational pilot study) |
| BMI | Body mass index |
| EFL | “Evaluation funktioneller Leistungsfähigkeit” (evaluation of functional capacity) |
| GPI | German pain index |
| MSD | Musculoskeletal disorder(s) |
| PACT | Performance Assessment and Capacity Training |
| RCT | Randomized controlled trial |
| VAS | Visual analogue scale |
References
- Organisation for Economic Co-Operation and Development. Sickness, Disablity and Work: Breaking the Barriers: A Synthesis of Findings across OECD Countries; OECD Publishing: Paris, France, 2010. [Google Scholar]
- Henderson, M.; Glozier, N.; Holland Elliott, K. Long term sickness absence. BMJ 2005, 330, 802–803. [Google Scholar] [CrossRef] [PubMed]
- Leiss, H.; Hucke, M.; Becede, M.; Machold-Fabrizii, V.; Smolen, J.S.; Machold, K.P. Effects of a brief workplace-centered consultation for employees with musculoskeletal pain on health outcomes: A prospective cohort study. Sci. Rep. 2019, 9, 5867. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubin, K.; Schlomann, L.; Lindert, L.; Pfaff, H.; Choi, K.E. Occupational Physicians’ Perspectives on Determinants of Employee Participation in a Randomized Controlled Musculoskeletal Health Promotion Measure: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 7445. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.A.; Lindert, L.; Ohlmeier, S.; Schlomann, L.; Pfaff, H.; Choi, K.E. “And Then He Got into the Wrong Group”: A Qualitative Study Exploring the Effects of Randomization in Recruitment to a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuomi, K.; Huuhtanen, P.; Nykyri, E.; Ilmarinen, J. Promotion of work ability, the quality of work and retirement. Occup. Med. 2001, 51, 318–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deutsche Schmerzgesellschaft. Deutscher Schmerzfragebogen. 2012. Available online: http://www.dgss.org/deutscher-schmerzfragebogen (accessed on 10 November 2021).
- Schwarzer, R.J.M. Skalen zur Erfassung von Lehrer- und Schülermerkmalen. Dokumentation der psychometrischen Verfahren im Rahmen der Wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen; Schwarzer, R.J.M., Ed.; Freie Universität Berlin: Berlin, Germany, 1999. [Google Scholar]
- Isernhagen, S. Evaluation Funktioneller Leistungsfähigkeit (EFL), Isernhagen Work Systems; EFL-Akademie: Braunschweig, Germany, 2012. [Google Scholar]
- Matheson, L.N.; Matheson, M.L. Schweizerische Arbeitsgemeinschaft für Rehabilitation SAR Arbeitsgruppe “Ergonomie”: Selbsteinschätzung der Körperlichen Leistungsfähigkeiten. Spinal Function Sort. Rating of Perceived Capacity. Test Booklet and Examiners Manual. Performance Assessment and Capacity Testing PACT, 1989/91. Available online: https://www.congress-compact.de/grip/pdf/teil5.pdf (accessed on 28 September 2021).
- Kirk, M.A.; Kelley, C.; Yankey, N.; Birken, S.A.; Abadie, B.; Damschroder, L. A systematic review of the use of the Consolidated Framework for Implementation Research. Implement. Sci. 2016, 11, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Vilsteren, M.; van Oostrom, S.H.; de Vet, H.C.; Franche, R.L.; Boot, C.R.; Anema, J.R. Workplace interventions to prevent work disability in workers on sick leave. Cochrane Database Syst. Rev. 2015, 10, CD006955. [Google Scholar] [CrossRef] [PubMed]
- Vogel, N.; Schandelmaier, S.; Zumbrunn, T.; Ebrahim, S.; de Boer, W.E.; Busse, J.W.; Kunz, R. Return-to-work coordination programmes for improving return to work in workers on sick leave. Cochrane Database Syst. Rev. 2017, 3, CD011618. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of Workplace Interventions in Return-to-Work for Musculoskeletal, Pain-Related and Mental Health Conditions: An Update of the Evidence and Messages for Practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, K.J.; Doucet, S.; Luke, A. Exploring the roles, functions, and background of patient navigators and case managers: A scoping review. Int. J. Nurs. Stud. 2019, 98, 27–47. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Meanc cCM/sSM | Percentiles | n cCM/sSM | p-Value | r-Value | |||
|---|---|---|---|---|---|---|---|
| 25. cCM/sSM | 50. (Median) cCM/sSM | 75. cCM/sSM | |||||
| t0 disability days | 2/2 | 0.00/0.00 | 2.00/2.00 | 3.00/3.00 | 363/335 | 0.955 | 0.0022 |
| t1 disability days | 1/1 | 0.00/0.00 | 0.00/1.00 | 2.00/2.00 | 256/248 | 0.041 * | 0.091 |
| t0 disability score | 47.89/46.67 | 30.00/26.67 | 50.00/46.67 | 66.67/66.67 | 379/347 | 0.498 | 0.0252 |
| t1 disability score | 31.17/36.15 | 10.00/10.00 | 20.00/33.33 | 50.00/56.67 | 268/262 | 0.030 * | 0.0942 |
| t0 pain intensity | 54.56/54.13 | 43.33/40.00 | 56.67/56.67 | 70.00/70.00 | 378/350 | 0.931 | 0.0032 |
| t1 pain intensity | 40.40/46.19 | 23.33/23.33 | 40.00/46.67 | 56.67/66.67 | 264/259 | 0.005 ** | 0.1233 |
| t0 self-efficacy | 29.92/30.06 | 28.00/28.00 | 30.00/30.00 | 32.00/32.00 | 375/339 | 0.923 | 0.0036 |
| t1 self-efficacy | 30.14/29.89 | 28.00/28.00 | 30.00/30.00 | 32.00/32.00 | 265/255 | 0.146 | 0.0637 |
| t0 work ability | 24.29/24.42 | 20.00/21.00 | 24.00/24.50 | 29.00/29.25 | 375/345 | 0.679 | 0.0154 |
| t1 work ability | 26.73/25.75 | 22.00/22.00 | 27.50/26.50 | 32.00/31.00 | 266/254 | 0.088 | 0.0748 |
| t0 sick leave days (MSD specific) | 29/28 | 3.00/4.25 | 12.00/14.00 | 33.00/33.75 | 163/200 | 0.804 | 0.013 |
| t1 sick leave days (MSD specific) | 18/13 | 0.00/0.00 | 2.00/0.00 | 19.00/16.75 | 163/200 | 0.376 | 0.0465 |
| Over All Modules | Mean t0/t1 | Percentiles | n | p-Value | r-Value | |||
|---|---|---|---|---|---|---|---|---|
| 25. t0/t1 | 50. (Median) t0/t1 | 75. t0/t1 | ||||||
| Case Management | disability days | 2/1 | 0.00/0.00 | 2.00/0.00 | 3.00/2.00 | 243 | 0.000 *** | 0.4806 |
| disability score | 45.20/30.75 | 26.67/10.00 | 46.67/30.00 | 63.33/47.50 | 262 | 0.000 *** | 0.547 | |
| pain intensity | 53.00/40.15 | 40.00/23.33 | 53.33/40.00 | 66.67/56.67 | 259 | 0.000 *** | 0.5673 | |
| sick leave days (MSD-specific) | 29/18 | 3.00/0.00 | 12.00/2.00 | 33.00/19.00 | 163 | 0.000 *** | 0.2953 | |
| self-efficacy | 29.88/30.17 | 28.00/29.00 | 30.00/30.00 | 32.00/32.00 | 256 | 0.191 | 0.0818 | |
| work ability | 24.78/26.83 | 20.88/22.38 | 25.00/27.50 | 29.63/32.00 | 258 | 0.000 *** | 0.3917 | |
| Self Management | disability days | 2/1 | 0.00/0.00 | 2.00/1.00 | 3.00/2.00 | 230 | 0.000 *** | 0.3809 |
| disability score | 46.85/35.88 | 26.67/10.00 | 46.67/33.33 | 70.00/56.67 | 249 | 0.000 *** | 0.4136 | |
| pain intensity | 54.00/45.93 | 40.00/23.33 | 56.67/46.67 | 70.00/66.67 | 249 | 0.000 *** | 0.3913 | |
| sick leave days (MSD-specific) | 28/13 | 4.25/0.00 | 14.00/0.00 | 33.75/16.75 | 200 | 0.000 *** | 0.3971 | |
| self-efficacy | 30.29/29.95 | 29.00/28.00 | 30.00/30.00 | 32.00/32.00 | 241 | 0.148 | 0.0933 | |
| work ability | 24.69/25.79 | 21.00/22.00 | 25.00/26.50 | 29.50/31.00 | 240 | 0.000 *** | 0.2299 | |
| Mean cCM/sSM | Percentiles | n cCM/sSM | p-Value | r-Value | |||
|---|---|---|---|---|---|---|---|
| 25. cCM/sSM | 50. (Median) cCM/sSM | 75. cCM/sSM | |||||
| t0 disability days | 1/1 | 0.00/0.00 | 2.00/2.00 | 3.00/3.00 | 284/253 | 0.898 | 0.0055 |
| t1 disability days | 1/1 | 0.00/0.00 | 0.00/0.00 | 1.00/2.00 | 200/191 | 0.003 ** | 0.1507 |
| t0 disability score | 43.38/42.50 | 26.67/20.83 | 43.33/40.00 | 60.00/63.33 | 293/260 | 0.602 | 0.0222 |
| t1 disability score | 26.36/32.99 | 8.33/10.00 | 20.00/30.00 | 43.33/53.33 | 209/203 | 0.012 * | 0.1241 |
| t0 pain intensity | 51.60/50.52 | 40.00/36.67 | 53.33/53.33 | 65.00/66.67 | 293/263 | 0.759 | 0.013 |
| t1 pain intensity | 36.72/43.50 | 20.00/23.33 | 36.67/43.33 | 50.00/63.33 | 206/201 | 0.004 ** | 0.1447 |
| t0 self-efficacy | 30.16/30.09 | 28.00/28.00 | 30.00/30.00 | 33.00/32.00 | 291/256 | 0.503 | 0.0286 |
| t1 self-efficacy | 30.52/30.06 | 29.00/28.00 | 31.00/30.00 | 33.00/32.75 | 208/200 | 0.049 * | 0.0976 |
| t0 work ability | 25.60/25.64 | 22.00/22.0 | 26.00/26.00 | 30.00/30.00 | 291/259 | 0.888 | 0.006 |
| t1 work ability | 27.93/26.57 | 24.00/22.50 | 28.50/27.50 | 32.00/32.00 | 208/197 | 0.035 * | 0.105 |
| t0 sick leave days (MSD specific) | 24/22 | 3.00/1.75 | 9.00/12.00 | 22.50/22.25 | 105/138 | 0.641 | 0.03 |
| t1 sick leave days (MSD specific) | 11/12 | 0.00/0.00 | 0.00/0.00 | 15.00/13.00 | 105/138 | 0.786 | 0.0174 |
| Mean t0/t1 | Percentiles | n | p-Value | r-Value | ||||
|---|---|---|---|---|---|---|---|---|
| 25. t0/t1 | 50. (Median) t0/t1 | 75. t0/t1 | ||||||
| Case management | disability days | 1/1 | 0.00/0.00 | 1.00/0.00 | 2.00/1.00 | 192 | 0.000 *** | 0.4858 |
| disability score | 40.67/26.11 | 20.00/6.67 | 40.00/20.00 | 56.67/41.67 | 205 | 0.000 *** | 0.6151 | |
| pain intensity (NRS) | 50.02/36.65 | 36.67/20.00 | 50.00/36.67 | 63.33/50.00 | 203 | 0.000 *** | 0.5665 | |
| sick leave days (MSD-specific) | 24/11 | 3.00/0.00 | 9.00/0.00 | 22.50/15.00 | 105 | 0.000 *** | 0.385 | |
| self-efficacy | 30.05/30.55 | 28.00/29.00 | 30.00/31.00 | 33.00/33.00 | 203 | 0.033 * | 0.1499 | |
| work ability | 26.13/27.95 | 22.50/24.00 | 26.50/28.50 | 30.00/32.00 | 203 | 0.000 *** | 0.3644 | |
| BMI | 27.41/27.06 | 24.25/23.80 | 26.80/26.10 | 29.30/29.53 | 133 | 0.009 ** | 0.2255 | |
| pain (VAS) | 3.59/2.12 | 2.00/0.00 | 3.00/2.00 | 5.00/3.00 | 134 | 0.000 *** | 0.6164 | |
| PACT | 154.07/166.21 | 138.00/154.00 | 156.00/171.00 | 178.00/188.00 | 133 | 0.000 *** | 0.5186 | |
| Self management | disability days | 2/1 | 0.00/0.00 | 2.00/1.00 | 3.00/2.00 | 179 | 0.000 *** | 0.3351 |
| disability score | 42.65/32.97 | 20.00/10.00 | 40.00/30.00 | 63.33/53.33 | 195 | 0.000 *** | 0.3593 | |
| pain intensity | 50.39/43.47 | 36.67/23.33 | 53.33/43.33 | 66.67/63.33 | 196 | 0.000 *** | 0.3418 | |
| sick leave days (MSD-specific) | 22/12 | 1.75/0.00 | 12.00/0.00 | 22.25/13.00 | 138 | 0.000 *** | 0.3333 | |
| self-efficacy | 30.22/30.09 | 29.00/28.00 | 30.00/30.00 | 32.00/33.00 | 191 | 0.717 | 0.0262 | |
| work ability | 25.93/26.55 | 22.00/22.50 | 26.00/27.25 | 30.00/31.88 | 188 | 0.032 * | 0.1561 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, K.-E.; Lindert, L.; Schlomann, L.; Samel, C.; Hellmich, M.; Pfaff, H. A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies. Int. J. Environ. Res. Public Health 2021, 18, 11844. https://doi.org/10.3390/ijerph182211844
Choi K-E, Lindert L, Schlomann L, Samel C, Hellmich M, Pfaff H. A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies. International Journal of Environmental Research and Public Health. 2021; 18(22):11844. https://doi.org/10.3390/ijerph182211844
Chicago/Turabian StyleChoi, Kyung-Eun (Anna), Lara Lindert, Lara Schlomann, Christina Samel, Martin Hellmich, and Holger Pfaff. 2021. "A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies" International Journal of Environmental Research and Public Health 18, no. 22: 11844. https://doi.org/10.3390/ijerph182211844
APA StyleChoi, K.-E., Lindert, L., Schlomann, L., Samel, C., Hellmich, M., & Pfaff, H. (2021). A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies. International Journal of Environmental Research and Public Health, 18(22), 11844. https://doi.org/10.3390/ijerph182211844